
Why It Is Difficult for Military Personnel to Quit Smoking: From the Perspective of Compensatory Health Beliefs



Abstract
:1. Introduction
2. Literature Review
2.1. Why Is It More Challenging for Taiwanese Soldiers to Quit Smoking?
2.2. What Factors Can Affect the Formation of CHBs?
3. Methods
3.1. Study Design
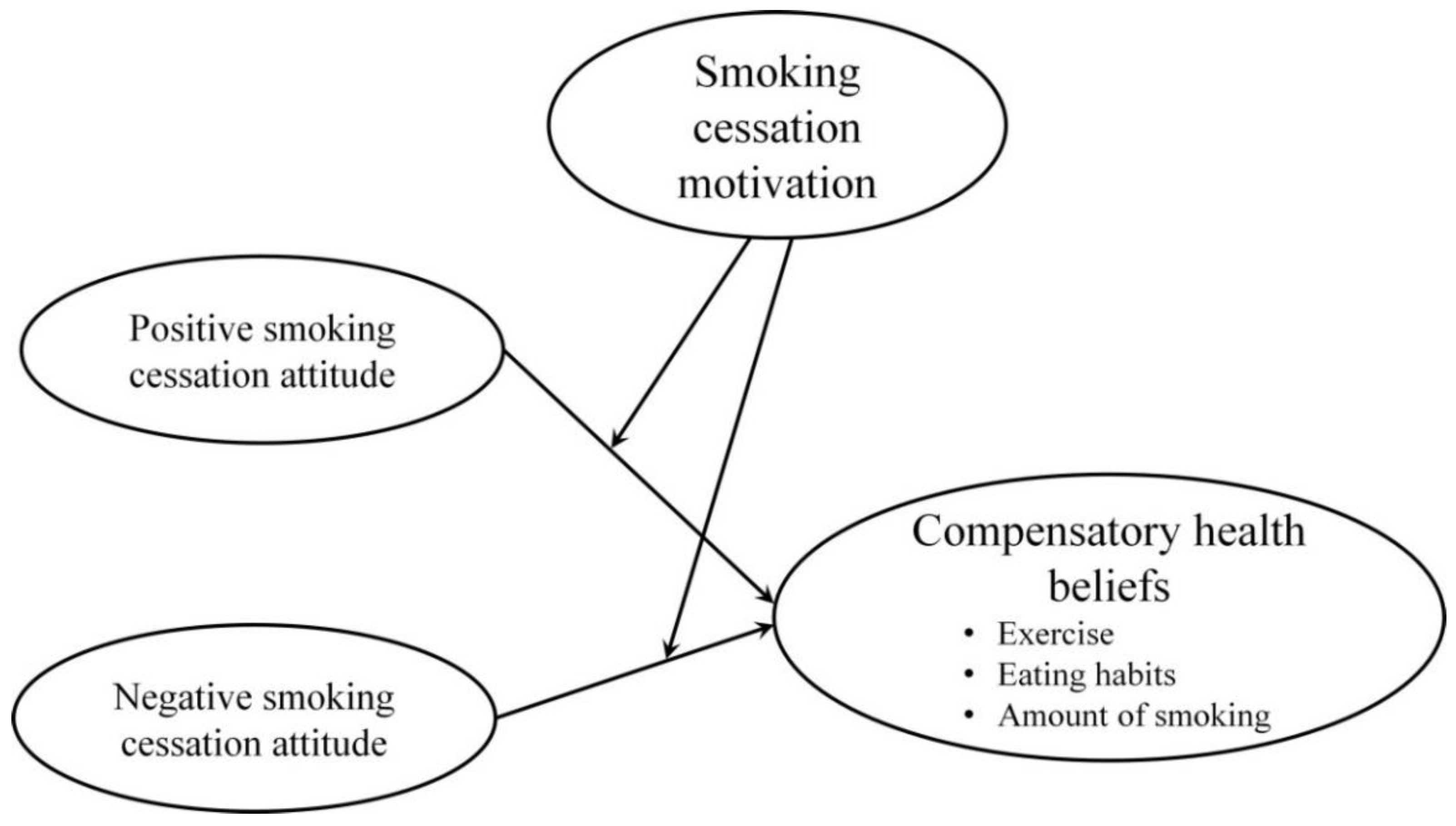
- 1.
- PAs towards smoking cessation have a negative effect on CHBs.
- 2.
- NAs towards smoking cessation have a positive effect on CHBs.
- 3.
- The intensity of the MO for smoking cessation is a PA, which has a negative moderating effect on CHBs.
- 4.
- The intensity of the MO for smoking cessation is an NA, which has a positive moderating effect on CHBs.
3.2. Participants
3.3. Questionnaire Design
3.4. Statistical Method
4. Results
4.1. Measurement Model
4.2. Structural Model
5. Discussion
5.1. Predicting the Influence of Attitudes towards Smoking Cessation on CHB
5.2. The Moderating Role of Smoking Cessation MO
5.3. Research Implications
6. Conclusions
6.1. Practical Recommendations
6.2. Limitations
6.3. Future Research
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Appendix A. Questionnaire Design

{kind=link}
| Items | Source | |
|---|---|---|
| Positive attitudes towards smoking cessation | [30] | |
| PA1: I think long-term smoking poses a threat to health. | ||
| PA2: I find that smoking is destroying my own health. | ||
| PA3: Smoking makes my mouth smell bad. | ||
| PA4: Smoking makes me feel bad breath. | ||
| PA5: In order to buy cigarettes, it cost me a lot of money. | ||
| PA6: The smell of smoking is unpleasant, which also bothers others. | ||
| PA7: Smoking will affect the surrounding relatives and friends due to second-hand smoke. | ||
| PA8: Smoking is harmful to your skin. | ||
| PA9: Too much dependence on cigarettes will trouble my life. | ||
| PA10: I think that when I quit smoking, I will have more energy to do other things. | ||
| Negative attitudes towards smoking cessation | [30] | |
| NA1: When I am under stress, cigarettes can calm my mood. | ||
| NA2: When I am unhappy, cigarettes can calm me down. | ||
| NA3: Smoking can help me cope with difficult situations. | ||
| NA4: When I’m feeling down, smoking can help me concentrate. | ||
| NA5: I like the motions of smoking. | ||
| NA6: It feels so good to smoke. | ||
| NA7: I love smoking. | ||
| NA8: I like to communicate with colleagues by smoking. | ||
| Compensatory health beliefs | [15] | |
| Exercise |
| |
| ||
| ||
| Food and drink |
| |
| ||
| ||
| ||
| Amount of smoking |
| |
| ||
| ||
| Motivation for smoking cessation | [31] | |
| MO1: I believe that quitting smoking is the best thing for my health. | ||
| MO2: Quitting smoking has an important impact on many aspects of my life. | ||
| MO3: Quitting smoking is an important choice. | ||
| MO4: Quitting smoking is very important for me to maintain my health. | ||
| MO5: I feel guilty if I smoke. | ||
| MO6: If I smoke, other people will be upset. | ||
| MO7: Would feel bad about myself if I smoked. | ||
| MO8: I hope others will approve of my decision to quit smoking. | ||
References
- Doll, R.; Peto, R.; Boreham, J.; Sutherland, I. Mortality in relation to smoking: 50 years’ observations on male British doctors. Br. Med. J. 2004, 328, 1519. [Google Scholar] [CrossRef] [Green Version]
- Lin, Y.S.; Wu, D.M.; Lai, H.R.; Shi, Z.P.; Chu, N.F. Influence of knowledge and attitudes on smoking habits among young military conscripts in Taiwan. J. Chin. Med. Assoc. 2010, 73, 411–418. [Google Scholar] [CrossRef] [Green Version]
- Lehto, R.H. Patient views on smoking, lung cancer, and stigma: A focus group perspective. Eur. J. Oncol. Nurs. 2014, 18, 316–322. [Google Scholar] [CrossRef]
- Nakata, A.; Ikeda, T.; Takahashi, M.; Haratani, T.; Hojou, M.; Fujioka, Y.; Araki, S. Non-fatal occupational injury among active and passive smokers in small-and medium-scale manufacturing enterprises in Japan. Soc. Sci. Med. 2006, 63, 2452–2463. [Google Scholar] [CrossRef]
- Suwazono, Y.; Okubo, Y.; Kobayashi, E.; Kido, T.; Nogawa, K. A follow-up study on the association of working conditions and lifestyles with the development of (perceived) mental symptoms in workers of a telecommunication enterprise. Occup. Med. 2003, 53, 436–442. [Google Scholar] [CrossRef]
- Suwa, K.; Flores, N.M.; Yoshikawa, R.; Goto, R.; Vietri, J.; Igarashi, A. Examining the association of smoking with work productivity and associated costs in Japan. J. Med. Econ. 2017, 20, 938–944. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- London, A.S.; Herd, P.; Miech, R.A.; Wilmoth, J.M. The influence of men’s military service on smoking across the life course. J. Drug Issues 2017, 47, 562–586. [Google Scholar] [CrossRef]
- Storm, V.; Reinwand, D.; Wienert, J.; Kuhlmann, T.; de Vries, H.; Lippke, S. Brief report: Compensatory health beliefs are negatively associated with intentions for regular fruit and vegetable consumption when self-efficacy is low. J. Health Psychol. 2017, 22, 1094–1100. [Google Scholar] [CrossRef] [Green Version]
- Amrein, M.A.; Scholz, U.; Inauen, J. Compensatory health beliefs and unhealthy snack consumption in daily life. Appetite 2021, 157, 104996. [Google Scholar] [CrossRef]
- Radtke, T.; Inauen, J.; Rennie, L.; Orbell, S.; Scholz, U. Trait versus state effects of dispositional and situational Compensatory Health Beliefs on high-calorie snack consumption. Zeitschr. Gesundheitspsychol. 2014, 22, 156–164. [Google Scholar] [CrossRef]
- Rabia, M.; Knäuper, B.; Miquelon, P. The eternal quest for optimal balance between maximizing pleasure and minimizing harm: The compensatory health beliefs model. Brit. J. Health Psych. 2006, 11, 139–153. [Google Scholar] [CrossRef]
- Su, F.Y.; Wang, S.H.; Lu, H.H.S.; Lin, G.M. Association of tobacco smoking with physical fitness of military males in taiwan: The CHIEF study. Can. Respir. J. 2020, 2020, 1–6. [Google Scholar] [CrossRef]
- Fuentes, J.P.O.; Almagiá, E.B. Creencias compensatorias de salud: Implicaciones para la salud y la adherencia al tratamiento. Psicología y Salud 2017, 27, 207–211. [Google Scholar]
- Matley, F.A.I.; Davies, E.L. Resisting temptation: Alcohol specific self-efficacy mediates the impacts of compensatory health beliefs and behaviours on alcohol consumption. Psychol. Health Med. 2017, 8506, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Radtke, T.; Scholz, U.; Keller, R.; Knäuper, B.; Hornung, R. Smoking-specific compensatory health beliefs and the readiness to stop smoking in adolescents. Br. J. Health Psychol. 2011, 16, 610–625. [Google Scholar] [CrossRef] [PubMed]
- Amrein, M.A.; Lüscher, J.; Berli, C.; Radtke, T.; Scholz, U. Do daily compensatory health beliefs predict intention to quit and smoking behavior? A daily diary study during smoking cessation. Int. J. Environ. Res. Public Health 2020, 17, 6419. [Google Scholar] [CrossRef]
- Bergman, H.E.; Chan, P.K.; Cooper, A.A.; Shirley, E.; Goto, T.; Fine, T.; Cohen, G.H.; Sampson, L.; Ganocy, S.; Tamburrino, M.; et al. Examining the relationship between PTSD symptomatology and cigarette smoking among Ohio army national guard soldiers. Mil. Behav. Health 2019, 7, 46–56. [Google Scholar] [CrossRef]
- Feldner, M.T.; Babson, K.A.; Zvolensky, M.J. Smoking, traumatic event exposure, and post-traumatic stress: A critical review of the empirical literature. Clin. Psychol. Rev. 2007, 27, 14–45. [Google Scholar] [CrossRef] [Green Version]
- Widome, R.; Joseph, A.M.; Polusny, M.A.; Chlebeck, B.; Brock, B.; Gulden, A.; Fu, S.S. Talking to Iraq and Afghanistan war veterans about tobacco use. Nicotine Tob. Res. 2011, 13, 623–626. [Google Scholar] [CrossRef] [PubMed]
- Jamal, A.; King, B.A.; Neff, L.J.; Whitmill, J.; Babb, S.D.; Graffunder, C.M. Current cigarette smoking among adults—United States 2005–2015. Morb. Mortal. Wkly. Rep. 2016, 65, 12051211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poston, W.S.; Taylor, J.E.; Hoffman, K.M.; Peterson, A.L.; Lando, H.A.; Shelton, S.; Haddock, C.K. Smoking and deployment: Perspectives of junior-enlisted US Air Force and US Army personnel and their supervisors. Mil. Med. 2008, 173, 441–447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lucchiari, C.; Masiero, M.; Pravettoni, G. Psychological and behavioral correlates of readiness to stop smoking. J. Adv. Nurs. 2020, 31, 194–202. [Google Scholar] [CrossRef] [PubMed]
- GBD 2015 Tobacco Collaborators. Smoking prevalence and attributable disease burden in 195 countries and territories, 1990–2015: A systematic analysis from the global burden of disease study 2015. Lancet 2017, 389, 1885–1906. [Google Scholar] [CrossRef] [Green Version]
- Chu, N.F.; Wu, D.M.; Shen, M.H.; Lin, Y.S. Prevalence of adverse behaviors among young military conscripts in Taiwan. Mil. Med. 2006, 171, 301–305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chu, N.F.; Lin, F.H.; Wu, Y.C. Prevalence and trends of cigarette smoking among military personnel in Taiwan: Results of 10-year anti-smoking health promotion programs in military. Mil. Med. 2017, 182, 1933–1937. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thongworn, S.; Sirisuk, V. Weight control specific compensatory health beliefs: Hypothetical testing and model extension. Kasetsart J. Soc. Sci. 2018, 39, 312–319. [Google Scholar] [CrossRef]
- Monnot, M.J. The effect of incentives on intrinsic motivation and employee attitudes: A multilevel study across nations and cultural clusters. Thunderbird Int. Bus. Rev. 2018, 60, 675–689. [Google Scholar] [CrossRef]
- Sugano, S.G.C.; Mamolo, L.A. The effects of teaching methodologies on students’ attitude and motivation: A meta-analysis. Int. J. Instr. 2021, 14, 827–846. [Google Scholar] [CrossRef]
- Radtke, T.; Rackow, P. Autonomous motivation is not enough: The role of compensatory health beliefs for the readiness to change stair and elevator use. Int. J. Environ. Res. Public Health 2014, 11, 12412–12428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Etter, J.F.; Humair, J.P.; Bergman, M.M.; Perneger, T.V. Development and validation of the attitudes towards smoking scale (ATS-18). Addiction 2000, 95, 613–625. [Google Scholar] [CrossRef]
- Cupertino, A.P.; Berg, C.; Gajewski, B.; Hui, S.K.A.; Richter, K.; Catley, D.; Ellerbeck, E.F. Change in self-efficacy, autonomous and controlled motivation predicting smoking. J. Health Psychol. 2012, 17, 640–652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hair, J.F., Jr.; Hult, G.T.M.; Ringle, C.M.; Sarstedt, M. A Primer on Partial Least Squares Structural Equation Modeling (PLS-SEM); Sage Publications: Thousand Oaks, CA, USA, 2021. [Google Scholar]
- Ringle, C.M.; Sarstedt, M.; Straub, D.W. Editor’s comments: A critical look at the use of PLS-SEM in MIS Quarterly. MIS Q. 2012, 36, iii–xiv. [Google Scholar] [CrossRef] [Green Version]
- Chin, W.W. How to write up and report PLS analyses. In Handbook of Partial Least Squares: Concepts, Methods and Applications in Marketing and Related Fields; Vinzi, V.E., Chin, W.W., Henseler, J., Wang, H., Eds.; Springer: Heidelberg, Germany, 2010; pp. 655–690. [Google Scholar]
- George, D.; Mallery, P. IBM SPSS Statistics 26 Step by Step: A Simple Guide and Reference, 6th ed.; Routledge: New York, NY, USA, 2008. [Google Scholar]
- Hair, J.F., Jr.; Black, W.C.; Babin, B.J.; Anderson, R.E.; Tatham, R.L. Multivariate Data Analysis, 7th ed.; Pearson: London, UK, 2017. [Google Scholar]
- Kline, R.B. Principles and Practice of Structural Equation Modeling, 4th ed.; Guilford Publications: New York, NY, USA, 2015. [Google Scholar]
- Martínez, Ú.; Brandon, T.H.; Sutton, S.K.; Simmons, V.N. Associations between the smoking-relatedness of a cancer type, cessation attitudes and beliefs, and future abstinence among recent quitters. Psychooncology 2018, 27, 2104–2110. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Liu, L.; Sharma, M.; Zhao, Y. Smoking-related knowledge, attitudes, behaviors, smoking cessation idea and education level among young adult male smokers in Chongqing, China. Int. J. Environ. Res. Public Health 2015, 12, 2135–2149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Premananto, G.C.; Muhammad, F.M.; Aisyah, R.A. Influence of picture health warnings on the attitudes and intention to quit smoking in middle school students. Int. J. Innov. Creat. Chang. 2020, 11, 269–279. [Google Scholar]
- Tohidi, H.; Jabbari, M.M. The effects of motivation in education. Proced. Soc. Behav. Sci. 2012, 31, 820–824. [Google Scholar] [CrossRef] [Green Version]
- Miquelon, P.; Knäuper, B.; Vallerand, R.J. Motivation and goal attainment. The role of compensatory beliefs. Appetite 2012, 58, 608–615. [Google Scholar] [CrossRef] [PubMed]
- Sheldon, K.M.; Elliot, A.J. Not all personal goals are personal: Comparing autonomous and controlled reasons for goals as predictors of effort and attainment. Pers. Soc. Psychol. Bull. 1998, 24, 546–557. [Google Scholar] [CrossRef]
- Beckham, J.C.; Wiley, M.T.; Miller, S.C.; Dennis, M.F.; Wilson, S.M.; McClernon, F.J.; Calhoun, P.S. Ad lib smoking in post-traumatic stress disorder: An electronic diary study. Nicotine Tob. Res. 2008, 10, 1149–1157. [Google Scholar] [CrossRef]
- Ulanday, K.T.; Jeffery, D.D.; Nebeling, L.; Srinivasan, S. Perceived deterrence of cigarette use and smoking status among active duty military personnel. Mil. Med. 2017, 182, e1733–e1741. [Google Scholar] [CrossRef] [Green Version]

| Categories | Variables | n | % |
|---|---|---|---|
| Gender | Male | 346 | 92.02 |
| Female | 30 | 7.98 | |
| Age | Under 20 | 43 | 11.44 |
| 21–25 | 233 | 61.97 | |
| 26–30 | 64 | 17.02 | |
| 31–35 | 30 | 7.98 | |
| 36–40 | 3 | 0.80 | |
| 46 and over | 3 | 0.80 | |
| Education level | High school education or lower | 128 | 34.04 |
| College degrees | 49 | 13.03 | |
| University degrees | 167 | 44.41 | |
| Postgraduate and over | 32 | 8.51 | |
| Smoking history | Under 5 years | 170 | 45.21 |
| 6–10 years | 165 | 43.88 | |
| 11–20 years | 37 | 9.84 | |
| 21 years and over | 4 | 1.06 | |
| Military time | Under six months | 181 | 48.14 |
| 1 year | 31 | 8.24 | |
| 1–2 year(s) | 54 | 14.36 | |
| 3–5 years | 44 | 11.70 | |
| 6–10 years | 44 | 11.70 | |
| 11–15 years | 20 | 5.32 | |
| 16 years or over | 2 | 0.53 | |
| Rank | Soldiers | 275 | 73.14 |
| Sergeant | 80 | 21.28 | |
| Officer | 21 | 5.59 | |
| Had thought about quitting smoking | Yes | 247 | 65.69 |
| No | 129 | 34.31 |
| Constructs | Items | Loading | CR | AVE |
|---|---|---|---|---|
| Attitude | ||||
| Positive | PA1 | 0.783 | 0.959 | 0.703 |
| PA2 | 0.842 | |||
| PA3 | 0.869 | |||
| PA4 | 0.824 | |||
| PA5 | 0.809 | |||
| PA6 | 0.878 | |||
| PA7 | 0.845 | |||
| PA8 | 0.866 | |||
| PA9 | 0.845 | |||
| PA10 | 0.818 | |||
| Negative | NA1 | 0.786 | 0.957 | 0.738 |
| NA2 | 0.873 | |||
| NA3 | 0.863 | |||
| NA4 | 0.887 | |||
| NA5 | 0.821 | |||
| NA6 | 0.911 | |||
| NA7 | 0.872 | |||
| NA8 | 0.853 | |||
| CHB | ||||
| CE | CE1 | 0.946 | 0.954 | 0.874 |
| CE2 | 0.938 | |||
| CE3 | 0.919 | |||
| EH | EH1 | 0.834 | 0.917 | 0.733 |
| EH2 | 0.889 | |||
| EH3 | 0.864 | |||
| EH4 | 0.837 | |||
| AS | AS1 | 0.883 | 0.924 | 0.802 |
| AS2 | 0.896 | |||
| AS3 | 0.907 | |||
| Smoking cessation MO | MO1 | 0.826 | 0.960 | 0.751 |
| MO2 | 0.840 | |||
| MO3 | 0.857 | |||
| MO4 | 0.854 | |||
| MO5 | 0.904 | |||
| MO6 | 0.880 | |||
| MO7 | 0.880 | |||
| MO8 | 0.889 | |||
| Constructs | PA | NA | CE | EH | AS | MO |
|---|---|---|---|---|---|---|
| PA | 0.838 | |||||
| NA | −0.031 | 0.859 | ||||
| CE | −0.097 | 0.213 | 0.935 | |||
| EH | −0.080 | 0.443 | 0.355 | 0.856 | ||
| AS | −0.160 | 0.376 | 0.300 | 0.390 | 0.895 | |
| MO | 0.731 | −0.167 | −0.026 | −0.053 | −0.152 | 0.867 |
| Hypothesis | Coefficient | t | p | Supported |
|---|---|---|---|---|
| 1. PA → CHB | ||||
| H1: PA → CE | −0.193 | 2.140 | 0.032 | Y |
| H2: PA → EH | −0.176 | 2.169 | 0.030 | Y |
| H3: PA → AS | −0.144 | 1.992 | 0.046 | Y |
| 2. NA → CHB | ||||
| H4: NA → CE | 0.188 | 3.110 | 0.002 | Y |
| H5: NA → EH | 0.449 | 7.666 | <0.001 | Y |
| H6: NA → AS | 0.305 | 5.910 | <0.001 | Y |
| 3. Moderating effect of MO between PAs and CHBs | ||||
| H7: MO × PA → CE | −0.223 | 3.929 | <0.001 | Y |
| H8: MO × PA → EH | −0.184 | 3.455 | 0.001 | Y |
| H9: MO × PA → AS | −0.232 | 4.769 | <0.001 | Y |
| 4. Moderating effect of MO between NAs and CHBs | ||||
| H10: MO × NA → CE | 0.017 | 0.331 | 0.740 | N |
| H11: MO × NA → EH | 0.020 | 0.407 | 0.684 | N |
| H12: MO × NA → AS | 0.052 | 1.186 | 0.236 | N |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Au-Yeung, C.-S.; Chao, R.-F.; Hsu, L.-Y. Why It Is Difficult for Military Personnel to Quit Smoking: From the Perspective of Compensatory Health Beliefs. Int. J. Environ. Res. Public Health 2021, 18, 12261. https://doi.org/10.3390/ijerph182212261
Au-Yeung C-S, Chao R-F, Hsu L-Y. Why It Is Difficult for Military Personnel to Quit Smoking: From the Perspective of Compensatory Health Beliefs. International Journal of Environmental Research and Public Health. 2021; 18(22):12261. https://doi.org/10.3390/ijerph182212261
Chicago/Turabian StyleAu-Yeung, Chor-Sum, Ren-Fang Chao, and Li-Yun Hsu. 2021. "Why It Is Difficult for Military Personnel to Quit Smoking: From the Perspective of Compensatory Health Beliefs" International Journal of Environmental Research and Public Health 18, no. 22: 12261. https://doi.org/10.3390/ijerph182212261
APA StyleAu-Yeung, C. -S., Chao, R. -F., & Hsu, L. -Y. (2021). Why It Is Difficult for Military Personnel to Quit Smoking: From the Perspective of Compensatory Health Beliefs. International Journal of Environmental Research and Public Health, 18(22), 12261. https://doi.org/10.3390/ijerph182212261