
Effects of the COVID-19 Pandemic on Physical Activity in Chronic Diseases: A Systematic Review and Meta-Analysis


 ,
,  ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Search Strategy and Data Resources
2.3. Study Selection: Inclusion and Exclusion Criteria
2.4. Reviewing Procedure and Data Extraction
2.5. Methodological Quality of Studies
2.6. Statistical Analysis
3. Results
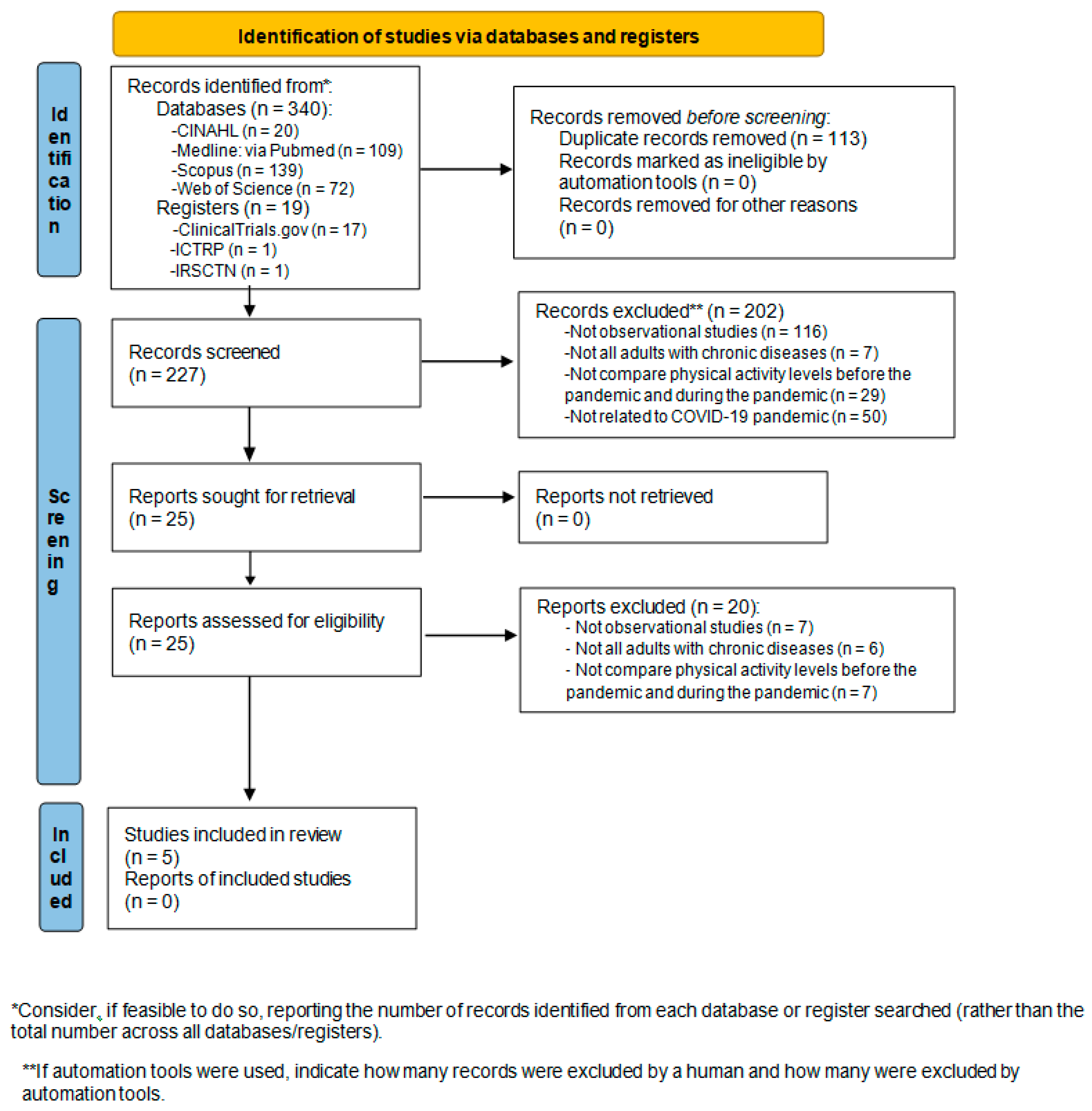
3.1. Results of the Search
3.2. Characteristics of the Included Studies and the Participants
3.3. Outcome Measures of Included Studies and Main Results
3.3.1. Objective Measures of PA
3.3.2. Subjective Measures of PA
3.3.3. Main Results on PA
Differences in PA Levels by Gender
Differences in PA Levels by Age
Other Outcome Measures
3.4. Methodological Quality of Studies
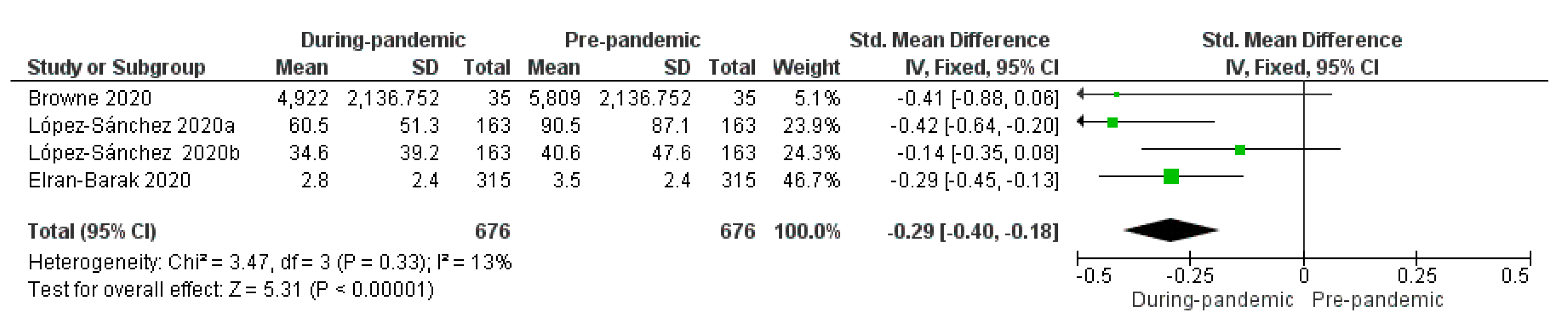
3.5. Meta-Analysis
4. Discussion
4.1. Clinical Implications for Practice
4.2. Strength and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Search Strategy
| DATABASE | CINAHL |
| DATE | 14/01/2021 |
| STRATEGY | #1 AND #2 AND #3 |
| #1 | AB (Exercise* OR “Physical Activit*” OR “Physical Exercise*” OR “Acute Exercise*” OR “Isometric Exercise*” OR “Aerobic Exercise*” OR “Exercise Training*” OR “Activity level*” OR “Physical fitness”) |
| #2 | AB (Pandemic* OR “Involuntary Commitment*” OR “COVID-19” OR “2019 novel coronavirus disease” OR “COVID19” OR “COVID-19 pandemic” OR “SARS-CoV-2 infection” OR “COVID-19 virus disease” OR “2019 novel coronavirus infection” OR “2019-nCoV infection” OR “coronavirus disease 2019” OR “coronavirus disease-19” OR “2019-nCoV disease” OR “COVID-19 virus infection” OR “Coronavirus Infection*”) |
| #3 | AB (“Chronic Disease*” OR “Chronic Illness*” OR “Chronically Ill” OR “chronic condition*”) |
| DATABASE | Medline (via Pubmed) |
| DATE | 14/01/2021 |
| STRATEGY | #1 AND #2 AND #3 |
| #1 | (“Exercise”[Mesh] OR Exercise* OR “Physical Activit*” OR “Physical Exercise*” OR “Acute Exercise*” OR “Isometric Exercise*” OR “Aerobic Exercise*” OR “Exercise Training*” OR “Activity level*” OR “Physical fitness”) |
| #2 | (“Pandemics”[Mesh] OR Pandemic* OR “Involuntary Commitment”[Mesh] OR “Involuntary Commitment*” OR “COVID-19”[Mesh] OR “COVID-19” OR “2019 novel coronavirus disease” OR “COVID19” OR “COVID-19 pandemic” OR “SARS-CoV-2 infection” OR “COVID-19 virus disease” OR “2019 novel coronavirus infection” OR “2019-nCoV infection” OR “coronavirus disease 2019” OR “coronavirus disease-19” OR “2019-nCoV disease” OR “COVID-19 virus infection” OR “Coronavirus Infections”[Mesh] OR “Coronavirus Infection*”) |
| #3 | (“Chronic Disease”[Mesh] OR “Chronic Disease*” OR “Chronic Illness*” OR “Chronically Ill” OR “chronic condition*”) |
| DATABASE | Scopus |
| DATE | 14/01/2021 |
| STRATEGY | #1 AND #2 AND #3 |
| #1 | TITLE-ABS-KEY (Exercise* OR “Physical Activit*” OR “Physical Exercise*” OR “Acute Exercise*” OR “Isometric Exercise*” OR “Aerobic Exercise*” OR “Exercise Training*” OR “Activity level*” OR “Physical fitness”) |
| #2 | TITLE-ABS-KEY (Pandemic* OR “Involuntary Commitment*” OR “COVID-19” OR “2019 novel coronavirus disease” OR “COVID19” OR “COVID-19 pandemic” OR “SARS-CoV-2 infection” OR “COVID-19 virus disease” OR “2019 novel coronavirus infection” OR “2019-nCoV infection” OR “coronavirus disease 2019” OR “coronavirus disease-19” OR “2019-nCoV disease” OR “COVID-19 virus infection” OR “Coronavirus Infection*”) |
| #3 | TITLE-ABS-KEY (“Chronic Disease*” OR “Chronic Illness*” OR “Chronically Ill” OR “chronic condition*”) |
| DATABASE | Web Of Science |
| DATE | 14/01/2021 |
| STRATEGY | #1 AND #2 AND #3 |
| #1 | TS = (“Exercise”[Mesh] OR Exercise* OR “Physical Activit*” OR “Physical Exercise*” OR “Acute Exercise*” OR “Isometric Exercise*” OR “Aerobic Exercise*” OR “Exercise Training*” OR “Activity level*” OR “Physical fitness”) |
| #2 | TS = (“Pandemics”[Mesh] OR Pandemic* OR “Involuntary Commitment”[Mesh] OR “Involuntary Commitment*” OR “COVID-19”[Mesh] OR “COVID-19” OR “2019 novel coronavirus disease” OR “COVID19” OR “COVID-19 pandemic” OR “SARS-CoV-2 infection” OR “COVID-19 virus disease” OR “2019 novel coronavirus infection” OR “2019-nCoV infection” OR “coronavirus disease 2019” OR “coronavirus disease-19” OR “2019-nCoV disease” OR “COVID-19 virus infection” OR “Coronavirus Infections”[Mesh] OR “Coronavirus Infection*”) |
| #3 | TS = (“Chronic Disease”[Mesh] OR “Chronic Disease*” OR “Chronic Illness*” OR “Chronically Ill” OR “chronic condition*”) |
Appendix B. Excluded Studies in the Last Screening (n = 20)
Appendix C. STROBE Checklist
| Title and Abstract | Introduction | Methods | Results | Other Analysis | Discussion | Other Information | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Autor (Year) [Ref] | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | 21 | 22 | TOTAL | % |
| Al Fagih, A. et al. (2020) [29] | V | V | V | V | V | V | V | V | X | X | V | V | V | V | V | V | V | V | V | V | X | X | 18 | 82 |
| Browne, R. et al. (2020) [30] | V | V | X | V | V | V | V | V | X | X | V | V | V | V | V | V | V | V | V | V | V | V | 19 | 86 |
| Elran-Barak, R. et al. (2020) [1] | V | V | V | X | V | V | V | V | X | X | V | V | X | X | V | V | V | V | V | V | V | V | 17 | 77 |
| López-Sánchez, G.F. et al. (2020) [17] | V | V | V | V | V | V | V | V | X | X | V | V | V | V | V | V | V | V | V | V | X | X | 18 | 82 |
| Zorcec, T. et al. (2020) [31] | V | V | V | X | V | V | X | X | X | X | X | X | X | V | V | X | V | V | X | V | X | X | 10 | 45 |
| Letter code: V: Reported on the article; X: Not reported on the article. | ||||||||||||||||||||||||
References
- Elran-Barak, R.; Mozeikov, M. One Month into the Reinforcement of Social Distancing due to the COVID-19 Outbreak: Subjective Health, Health Behaviors, and Loneliness among People with Chronic Medical Conditions. Int. J. Environ. Res. Public Health 2020, 17, 5403. [Google Scholar] [CrossRef] [PubMed]
- Bhutani, S.; Cooper, J.A. COVID-19-Related Home Confinement in Adults: Weight Gain Risks and Opportunities. Obesity 2020, 28, 1576–1577. [Google Scholar] [CrossRef]
- Ammar, A.; Brach, M.; Trabelsi, K.; Chtourou, H.; Boukhris, O.; Masmoudi, L.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M.; et al. Effects of COVID-19 Home Confinement on Eating Behaviour and Physical Activity: Results of the ECLB-COVID19 International Online Survey. Nutrients 2020, 12, 1583. [Google Scholar] [CrossRef] [PubMed]
- Bernell, S.; Howard, S.W. Use Your Words Carefully: What Is a Chronic Disease? Front. Public Health 2016, 4, 159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geleta, T.A.; Deriba, B.S.; Beyane, R.S.; Mohammed, A.; Birhanu, T.; Jemal, K. COVID-19 Pandemic Preparedness and Response of Chronic Disease Patients in Public Health Facilities. Int. J. Gen. Med. 2020, 13, 1011–1023. [Google Scholar] [CrossRef] [PubMed]
- Prasad, S.S.; Duncanson, K.; Keely, S.; Talley, N.J.; Kairuz, T.; Holtmann, G.J.; Shah, A.; Walker, M.M. A Role for Primary Care Pharmacists in the Management of Inflammatory Bowel Disease? Lessons from Chronic Disease: A Systematic Review. Pharmacy 2020, 8, 204. [Google Scholar] [CrossRef]
- Bachmann, M.C.; Bellalta, S.; Basoalto, R.; Gómez-Valenzuela, F.; Jalil, Y.; Lépez, M.; Matamoros, A.; Von Bernhardi, R. The Challenge by Multiple Environmental and Biological Factors Induce Inflammation in Aging: Their Role in the Promotion of Chronic Disease. Front. Immunol. 2020, 11, 570083. [Google Scholar] [CrossRef]
- Vera-Remartínez, E.J.; Borraz-Fernández, J.R.; Domínguez-Zamorano, J.A.; Mora-Parra, L.M.; Casado-Hoces, S.V.; González-Gómez, J.A.; Blanco-Quiroga, A.; Armenteros-López, B.; Garcés-Pina, E. Prevalencia de patologías crónicas y factores de riesgo en población penitenciaria española [Prevalence of chronic diseases and risk factors among the Spanish prison population]. Rev. Esp. Sanid. Penit. 2014, 16, 38–47. [Google Scholar] [CrossRef] [Green Version]
- Unwin, N.; Alberti, K.G. Chronic non-communicable diseases. Ann. Trop. Med. Parasitol. 2006, 100, 455–464. [Google Scholar] [CrossRef]
- Lacombe, J.; Armstrong, M.E.; Wright, F.L.; Foster, C. The impact of physical activity and an additional behavioural risk factor on cardiovascular disease, cancer and all-cause mortality: A systematic review. BMC Public Health 2019, 19, 900. [Google Scholar] [CrossRef] [Green Version]
- Desveaux, L.; Lee, A.; Goldstein, R.; Brooks, D. Yoga in the Management of Chronic Disease: A Systematic Review and Meta-analysis. Med. Care 2015, 53, 653–661. [Google Scholar] [CrossRef]
- Warburton, D.E.; Bredin, S.S. Health benefits of physical activity: A systematic review of current systematic reviews. Curr. Opin. Cardiol. 2017, 32, 541–556. [Google Scholar] [CrossRef]
- Bullard, T.; Ji, M.; An, R.; Trinh, L.; Mackenzie, M.; Mullen, S.P. A systematic review and meta-analysis of adherence to physical activity interventions among three chronic conditions: Cancer, cardiovascular disease, and diabetes. BMC Public Health 2019, 19, 636. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thornton, J.S.; Frémont, P.; Khan, K.; Poirier, P.; Fowles, J.; Wells, G.D.; Frankovich, R.J. Physical activity prescription: A critical opportunity to address a modifiable risk factor for the prevention and management of chronic disease: A position statement by the Canadian Academy of Sport and Exercise Medicine. Br. J. Sports Med. 2016, 50, 1109–1114. [Google Scholar] [CrossRef]
- West, S.L.; Banks, L.; Schneiderman, J.E.; Stephens, S.; White, G.; Dogra, S.; Greg, D. Physical activity for children with chronic disease; a narrative review and practical applications. BMC Pediatr. 2019, 19, 12. [Google Scholar] [CrossRef] [Green Version]
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.M.; Nieman, D.C.; Swain, D.P. American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Med. Sci. Sports Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef] [PubMed]
- Gerritsen, J.; Vincent, A. Exercise improves quality of life in patients with cancer: A systematic review and meta-analysis of randomised controlled trials. Br. J. Sports Med. 2015, 796–803. [Google Scholar] [CrossRef]
- Hu, G.; Jousilahti, P.; Barengo, N.; Qiao, Q.; Lakka, T.; Tuomilehto, J. Physical activity, cardiovascular risk factors, and mortality among Finnish adults with diabetes. Diabetes Care 2005, 28, 799–805. [Google Scholar] [CrossRef] [Green Version]
- López-Sánchez, G.F.; López-Bueno, R.; Gil-Salmerón, A.; Zauder, R.; Skalska, M.; Jastrzębska, J.; Jastrzębski, Z.; Schuch, F.B.; Grabovac, I.; Tully, M.A.; et al. Comparison of physical activity levels in Spanish adults with chronic conditions before and during COVID-19 quarantine. Eur. J. Public Health 2021, 31, 161–166. [Google Scholar] [CrossRef] [PubMed]
- González, K.; Fuentes, J.; Márquez, J.L. Physical Inactivity, Sedentary Behavior and Chronic Diseases. Korean J. Fam. Med. 2017, 38, 111–115. [Google Scholar] [CrossRef] [Green Version]
- Paudel, S.; Owen, A.J.; Owusu-Addo, E.; Smith, B.J. Physical activity participation and the risk of chronic diseases among South Asian adults: A systematic review and meta-analysis. Sci. Rep. 2019, 9, 9771. [Google Scholar] [CrossRef] [PubMed]
- Fallon, K. Exercise in the time of COVID-19. Aust. J. Gen. Pract. 2020, 49, 1–2. [Google Scholar] [CrossRef]
- Fletcher, G.F.; Landolfo, C.; Niebauer, J.; Ozemek, C.; Arena, R.; Lavie, C.J. Promoting Physical Activity and Exercise: JACC Health Promotion Series. J. Am. Coll. Cardiol. 2018, 72, 1622–1639. [Google Scholar] [CrossRef]
- Beller, E.M.; Glasziou, P.P.; Altman, D.G.; Hopewell, S.; Bastian, H.; Chalmers, I. PRISMA for Abstracts: Reporting systematic reviews in journal and conference abstracts. PLoS Med. 2013, 10, e1001419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef] [PubMed]
- Hutton, B.; Catalá-López, F.; Moher, D. La extensión de la declaración PRISMA para revisiones sistemáticas que incorporan metaanálisis en red: PRISMA-NMA. Med. Clin. 2016, 147, 262–266. [Google Scholar] [CrossRef] [PubMed]
- Vandenbroucke, J.P.; Von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): Explanation and elaboration. Epidemiology 2007, 18, 805–835. [Google Scholar] [CrossRef] [Green Version]
- Moreno-Rabié, C.; Torres, A.; Lambrechts, P.; Jacobs, R. Clinical applications, accuracy and limitations of guided endodontics: A systematic review. Int. Endod. J. 2020, 53, 214–231. [Google Scholar] [CrossRef] [Green Version]
- St-Onge, M.; Dubé, P.A.; Gosselin, S.; Guimont, C.; Godwin, J.; Archambault, P.M.; Chauny, J.M.; Frenette, A.J.; Darveau, M.; Le Sage, N.; et al. Treatment for calcium channel blocker poisoning: A systematic review. Clin. Toxicol. 2014, 52, 926–944. [Google Scholar] [CrossRef] [Green Version]
- Cortegoso, P.; Skonieczna-Żydecka, K.; Pennazio, M.; Rondonotti, E.; Marlicz, W.; Toth, E.; Koulaouzidis, A. Capsule endoscopy transit-related indicators in choosing the insertion route for double-balloon enteroscopy: A systematic review. Endosc. Int. Open 2021, 9, E163–E170. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analysis. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Al Fagih, A.; Al Onazi, M.; Al Basiri, S.; Al-Kaf, F.; Dagriri, K.; Al Hebaishi, Y.; Samargandy, S.; Al Shengeiti, L. Remotely monitored inactivity due to COVID-19 lockdowns. Potential hazard for heart failure patients. Saudi Med. J. 2020, 41, 1211–1216. [Google Scholar] [CrossRef]
- Browne, R.; Macêdo, G.; Cabral, L.; Oliveira, G.; Vivas, A.; Fontes, E.B.; Elsangedy, H.M.; Costa, E.C. Initial impact of the COVID-19 pandemic on physical activity and sedentary behavior in hypertensive older adults: An accelerometer-based analysis. Exp. Gerontol. 2020, 142, 111121. [Google Scholar] [CrossRef] [PubMed]
- Zorcec, T.; Jakovska, T.; Micevska, V.; Boskovska, K.; Cholakovska, V.C. Pandemic with COVID-19 and Families with Children with Chronic Respiratory Diseases. Prilozi 2020, 41, 95–101. [Google Scholar] [CrossRef]
- Prieto, M.Á.; March, J.C.; Martín, A.; Escudero, M.; López, M.; Luque, N. Repercusiones del confinamiento por COVID-19 en pacientes crónicos de Andalucía [Consequences of the COVID-19 lockdown in patients with chronic diseases in Andalusia]. Gac. Sanit. 2020. [Google Scholar] [CrossRef]
- Altena, E.; Baglioni, C.; Espie, C.A.; Ellis, J.; Gavriloff, D.; Holzinger, B.; Schlarb, A.; Frase, L.; Jernelöv, S.; Riemann, D. Dealing with sleep problems during home confinement due to the COVID-19 outbreak: Practical recommendations from a task force of the European CBT-I Academy. J. Sleep Res. 2020, 29, e13052. [Google Scholar] [CrossRef] [PubMed]
- Pietrobelli, A.; Pecoraro, L.; Ferruzzi, A.; Heo, M.; Faith, M.; Zoller, T.; Antoniazzi, F.; Piacentini, G.; Fearnbach, S.N.; Heymsfield, S.B. Effects of COVID-19 Lockdown on Lifestyle Behaviors in Children with Obesity Living in Verona, Italy: A Longitudinal Study. Obesity 2020, 28, 1382–1385. [Google Scholar] [CrossRef]
- Chevance, A.; Gourion, D.; Hoertel, N.; Llorca, P.M.; Thomas, P.; Bocher, R.; Moro, M.R.; Laprévote, V.; Benyamina, A.; Fossati, P.; et al. Ensuring mental health care during the SARS-CoV-2 epidemic in France: A narrative review. Encephale 2020, 46, 193–201. [Google Scholar] [CrossRef]
- Narici, M.; De Vito, G.; Franchi, M.; Paoli, A.; Moro, T.; Marcolin, G.; Grassi, B.; Baldassarre, G.; Zuccarelli, L.; Biolo, G.; et al. Impact of sedentarism due to the COVID-19 home confinement on neuromuscular, cardiovascular and metabolic health: Physiological and pathophysiological implications and recommendations for physical and nutritional countermeasures. Eur. J. Sport Sci. 2020, 21, 614–635. [Google Scholar] [CrossRef]
- Marçal, I.R.; Fernandes, B.; Viana, A.A.; Ciolac, E.G. The Urgent Need for Recommending Physical Activity for the Management of Diabetes During and Beyond COVID-19 Outbreak. Front. Endocrinol. 2020, 11, 584–642. [Google Scholar] [CrossRef]
- Stavridou, A.; Stergiopoulou, A.A.; Panagouli, E.; Mesiris, G.; Thirios, A.; Mougiakos, T.; Troupis, T.; Psaltopoulou, T.; Tsolia, M.; Sergentanis, T.N.; et al. Psychosocial consequences of COVID-19 in children, adolescents and young adults: A systematic review. Psychiatry Clin. Neurosci. 2020, 74, 615–616. [Google Scholar] [CrossRef] [PubMed]
- Bentlage, E.; Ammar, A.; How, D.; Ahmed, M.; Trabelsi, K.; Chtourou, H.; Brach, M. Practical Recommendations for Maintaining Active Lifestyle during the COVID-19 Pandemic: A Systematic Literature Review. Int. J. Environ. Res. Public Health 2020, 17, 6265. [Google Scholar] [CrossRef] [PubMed]
- Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. Available online: www.handbook.cochrane.org (accessed on 19 October 2021).
- Ndwiga, D.; MacMillan, F.; McBride, K.; Simmons, D. Lifestyle Interventions for People with, and at Risk of Type 2 Diabetes in Polynesian Communities: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2018, 15, 882. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hedlund, C.; Rapoport, A.; Dodick, D.; Goadsby, P. Zolmitriptan nasal spray in the acute treatment of cluster headache: A meta-analysis of two studies. Headache J. Head Face Pain 2009, 49, 1315–1323. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Author (Year) [Ref] | Study Place | Design of the Study | Sample Size (n = ) | Chronic Disease (%) | Age | Gender (% Males) | Study Period |
|---|---|---|---|---|---|---|---|
| Al Fagih, A. et al. (2020) [32] | Riyadh, Kingdom of Saudi Arabia | Longitudinal retrospective | 82 | Heart failure (100) | Median (25th, 75th percentile) 65 (58, 72) | 64.6 | 2 February to 19 April 2020 |
| Browne, R. et al. (2020) [33] | Natal, Brazil | Longitudinal prospective | 35 | Hypertension (100) | Mean ± SD 65.6 ± 3.8 | 34.3 | January to March and June 2020 |
| Elran-Barak, R. et al. (2020) [1] | Israel | Cross-sectional | 315 | Mental health (11.7); Metabolic (27); Cardiovascular (17.3); Cancer and autoimmune (20.8); Orthopedic/pain (17.6); Other (5.5) | % (n)18–45: 19.2 (60) % (n) 46–55: 13.8 (43) % (n) 56–65: 22.1 (69) % (n): 66–75: 34.3 (107) % (n) >76: 10.6 (33) | 40.5 | 20–22 April 2020 |
| López- Sánchez, G.F. et al. (2020) [19] | Spain | Cross-sectional | 163 | Depression (14.1); Anxiety (7.9); Other psychiatric disorders (6.7); Obesity (15.3); Hypertension (10.4); Varicose veins of lower extremities (12.3); Osteoarthritis (2.5); chronic neck pain (8.6); Chronic low back pain (11.0); Chronic allergy excluding asthma (13.5); Asthma including allergic asthma (15.3); Chronic bronchitis (3.1); Diabetes type 2 (1.8); Cataracts (2.5); Peptic ulcer disease (1.2); Urinary incontinence or urine control problems (0.6); Hypercholesterolemia (15.3); Chronic skin disease (12.9); Chronic constipation (4.3); Chronic migraine and other frequent chronic headaches (19.0); Hemorrhoids (12.9); Cancer (1.2); Osteoporosis (3.7); Thyroid disease (7.4); Renal disease (6.7); Injury (4.9) | (N = x) 18–24 (n = 59) 25–34 (n = 52) 45–54 (n = 11) 55–64 (n = 10) | 28.8 | 1 April to 1 May 2020 |
| Zorcec, T. et al. (2020) [34] | Republic of Macedonia | Cross-sectional | 72 | Chronic respiratory diseases (Cystic Fibrosis, Asthma, Tuberculosis and Allergic Rhinitis) (100) | Mean ± SD 7.3 ± 2.89 | Not reported | May, June, and the first week of July 2020. |
| Author (Year) [Ref] | Method of PA Assessment | PA Measuring Instrument | Description of PA Measuring Instrument | Measured Variable | Main Results | Other Outcome Measures | Measuring Instrument for Other Outcome Measures |
|---|---|---|---|---|---|---|---|
| Al Fagih, A. et al. (2020) [32] | Objective | Medtronic ICD/CRT accelerometer | Mode of use: Patients wear the accelerometer all day. | PA | PA: –0.6 h/day (p = 0.000010) Reduction of PA of 27.1% | Age; Gender; Weight; Medications; Residence; Comorbidities; Implanted device type; Palpitation; Dizziness; Syncope; Adjusted use of diuretics; Unplanned hospitalization; Daily activity and exercise. | Online questionnaire |
| Optivol fluid index; Thoracic impedance of patients (ohms). | Medtronic CareLink | ||||||
| Browne, R. et al. (2020) [33] | Objective | Actigraph GT3X accelerometer Complement: a diary | Mode of use: Accelerometer: 7 consecutive days including awake and asleep periods. Diary: Registry of time the accelerometer is removed during the vigil, time to go to sleep and time to wake up. | PA Light PA Moderate–vigorous PA SB | PA: –886 step/day (p = 0.018) Light PA: –26.6 min/day (p = 0.053) Moderate–vigorous PA: –2.8 min/day (p = 0.018) SB: +29.6 min/day (p = 0.032) The magnitude of changes was greater on the weekend, mainly for steps/day and SB. | Age; Gender; Married; Living alone; Post-secondary education; BMI; Resting SBP; Resting DBP; Resting HR; Hypertension diagnosis; Risk factors; Medication. | - |
| Elran- Barak, R. et al. (2020) [1] | Subjective | Online questionnaire | Question: PA: “On average, how many times a week do you participate in any exercise/sports activity for half an hour or longer?” | PA | PA: –0.7 (times/week) (p < 0.001) | Age; Gender; Marital status; Education; Work status before and during COVID-19; Economic status; Religiosity; Nº people in the household; Crowed housing conditions; Main medical condition; Duration and Medical care for condition; Medical visit frequency; BMI | Online questionnaire |
| Health behaviors | 1 item based on SF-36; 2 based on Serving Fruits and Vegetables Scale | ||||||
| Disease management | Based on disease-specific self-efficacy measures and Challenges to Illness Management Scale | ||||||
| Time spent on social media | 2 items adopted from the Technology Use Questionnaire | ||||||
| Self-rated health | 5 items based on SF-36 | ||||||
| Loneliness | 3 items based on version of the Revised UCLA Loneliness Scale | ||||||
| López- Sánchez, G.F. et al. (2020) [19] | Subjective | Online questionnaire | Questions: (1) “How much time on an average day did you usually spend in moderate activity before quarantine?” (2) “How much time on an average day do you spend in moderate activity during quarantine?” (3) “How much time on an average day did you usually spend in vigorous activity before quarantine?” (4) “How much time on an average day do you spend in vigorous activity during quarantine?” | Moderate PA Vigorous PA | Moderate PA General: −30 min/day (p < 0.001) Males: −22.1 min/day (p = 0.006) Females: −33.2 min/day (p < 0.001) Aged 18–44 and 55–64: (p < 0.05) Multimorbidity: −30.1 min/day (p < 0.001) Asthma: −26.2 min/day (p = 0.026) Hypercholesterolemia: −39 min/day (p = 0.011) Chronic skin disease: −44.3 min/day (p = 0.004) Hemorrhoids: −50.1 min/day (p = 0.009) Vigorous PA Males: −15.5 min/day (p = 0.025) Multimorbidity: −11.4 min/day (p = 0.045) | Age; Gender; Chronic condition | Online questionnaire |
| Zorcec, T. et al. (2020) [34] | Subjective | Online questionnaire | Questions: (1) PA one month before the pandemic. (2) PA during the pandemic. | PA | PA more than 2 h: −32% (p = 0.0001) PA few hours per week: +18.8% (p = 0.0056) Statistically significant number of children deteriorated in their PA from more than 2 h per day to few hours per week. | Family demographic characteristics; Employment status during pandemic related to fathers and mothers; Medication; Checkups during pandemic; Mental health of children before and during pandemic; Physical health of children before and during pandemic; Children’s routines during pandemic | Online questionnaire |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pérez-Gisbert, L.; Torres-Sánchez, I.; Ortiz-Rubio, A.; Calvache-Mateo, A.; López-López, L.; Cabrera-Martos, I.; Valenza, M.C. Effects of the COVID-19 Pandemic on Physical Activity in Chronic Diseases: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 12278. https://doi.org/10.3390/ijerph182312278
Pérez-Gisbert L, Torres-Sánchez I, Ortiz-Rubio A, Calvache-Mateo A, López-López L, Cabrera-Martos I, Valenza MC. Effects of the COVID-19 Pandemic on Physical Activity in Chronic Diseases: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2021; 18(23):12278. https://doi.org/10.3390/ijerph182312278
Chicago/Turabian StylePérez-Gisbert, Laura, Irene Torres-Sánchez, Araceli Ortiz-Rubio, Andrés Calvache-Mateo, Laura López-López, Irene Cabrera-Martos, and Marie Carmen Valenza. 2021. "Effects of the COVID-19 Pandemic on Physical Activity in Chronic Diseases: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 18, no. 23: 12278. https://doi.org/10.3390/ijerph182312278
APA StylePérez-Gisbert, L., Torres-Sánchez, I., Ortiz-Rubio, A., Calvache-Mateo, A., López-López, L., Cabrera-Martos, I., & Valenza, M. C. (2021). Effects of the COVID-19 Pandemic on Physical Activity in Chronic Diseases: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 18(23), 12278. https://doi.org/10.3390/ijerph182312278