
Prevalence, Awareness, Treatment, and Control of Hypertension in the United Arab Emirates: A Systematic Review and Meta-Analysis



Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection
2.2.1. Inclusion Criteria
- Population-based prospective observational studies, conducted among apparently healthy adult subjects living in the UAE and that defined hypertension using the guidelines-recommended BP cut-off ≥130/80 mmHg or ≥140/90 mmHg, were considered.
- Studies provided estimates of the prevalence of hypertension and investigated the level of awareness, treatment, and control of hypertension among the general population.
- Multi-country studies were included if data on the prevalence, awareness, treatment, and control of hypertension in the UAE could be distinctly extracted.
- Only peer-reviewed full-length research articles were considered.
2.2.2. Exclusion Criteria
- Studies conducted on diseased populations, children, and pregnant women were excluded.
- Studies that did not provide the estimates in numbers or percentages were excluded.
- Conference proceedings, abstracts, reviews, non-human studies, correspondences, and editorials were excluded.
- Studies with unrelated outcome measures and articles with missing or insufficient data were excluded.
2.3. Operational Definitions
- Prevalence of hypertension is defined as mean SBP ≥ 140 mmHg and/or diastolic BP (DBP) ≥ 90 mmHg and/or using antihypertensive medication if hypertension was known.
- Awareness of hypertension is defined as the proportion of subjects with hypertension who reported either having been diagnosed with hypertension by a clinician or reported taking antihypertensive medications.
- Hypertension treatment was defined as the proportion of adults with hypertension who reported taking any medication for hypertension.
- Hypertension control was defined as the proportion of adults taking antihypertensive medications but who had not reached the guidelines-recommended BP targets of <130/80 mmHg or <140/90 mmHg.
2.4. Data Extraction
2.5. Quality Assessment
2.6. Statistical Analysis
3. Results
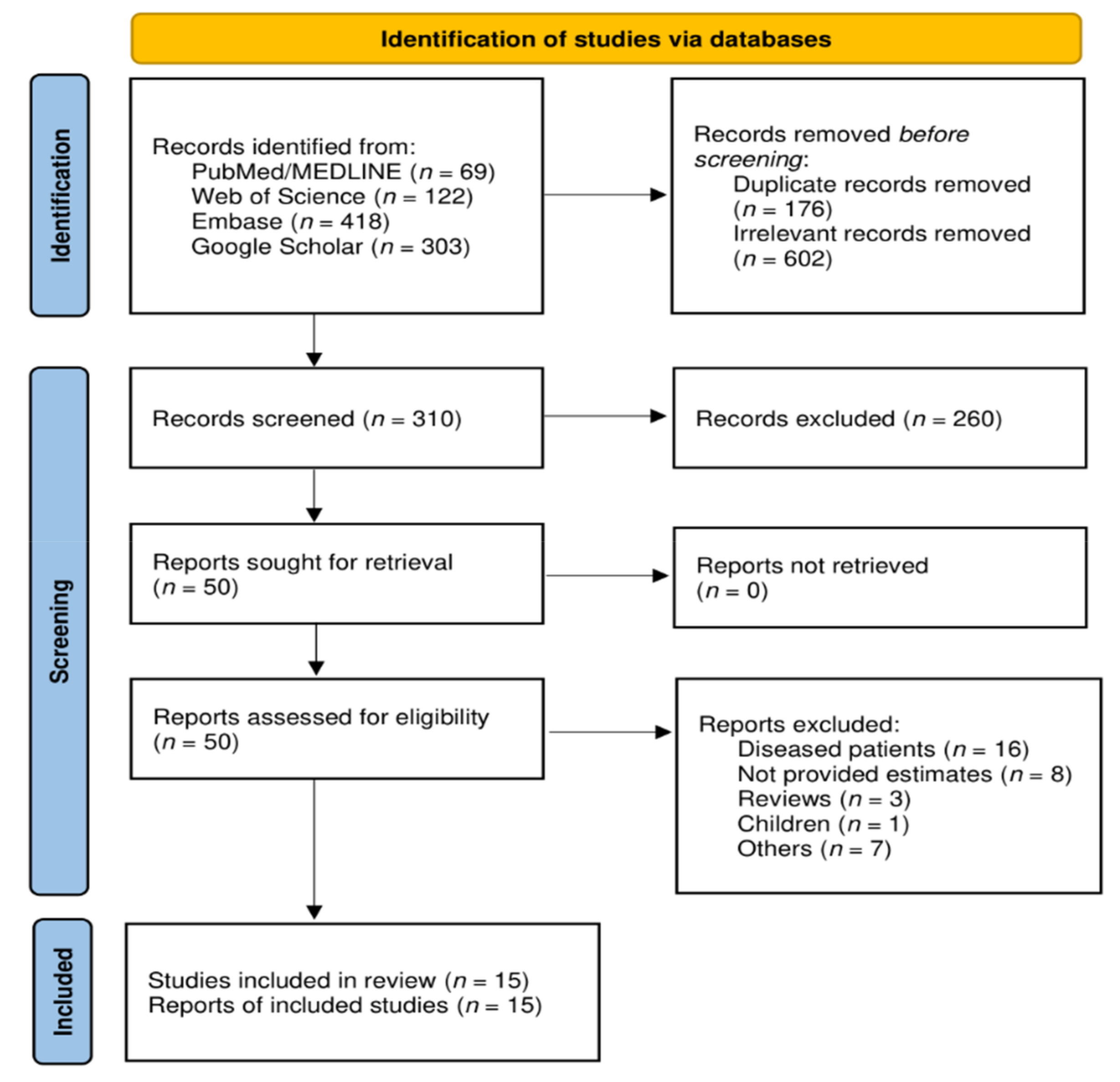
3.1. Study Selection
3.2. Characteristics of the Included Studies
3.3. Quality of Included Studies
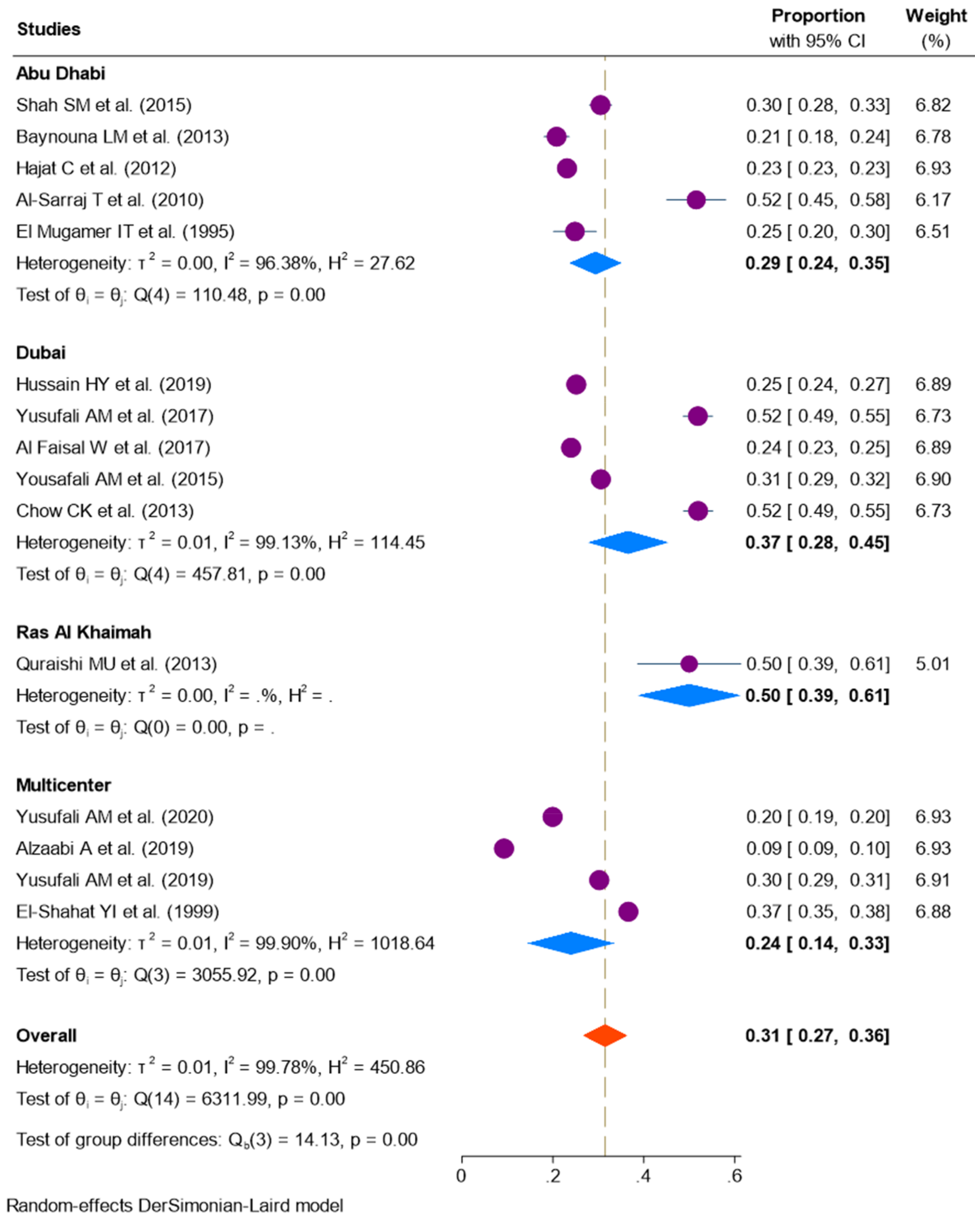
3.4. Prevalence of Hypertension
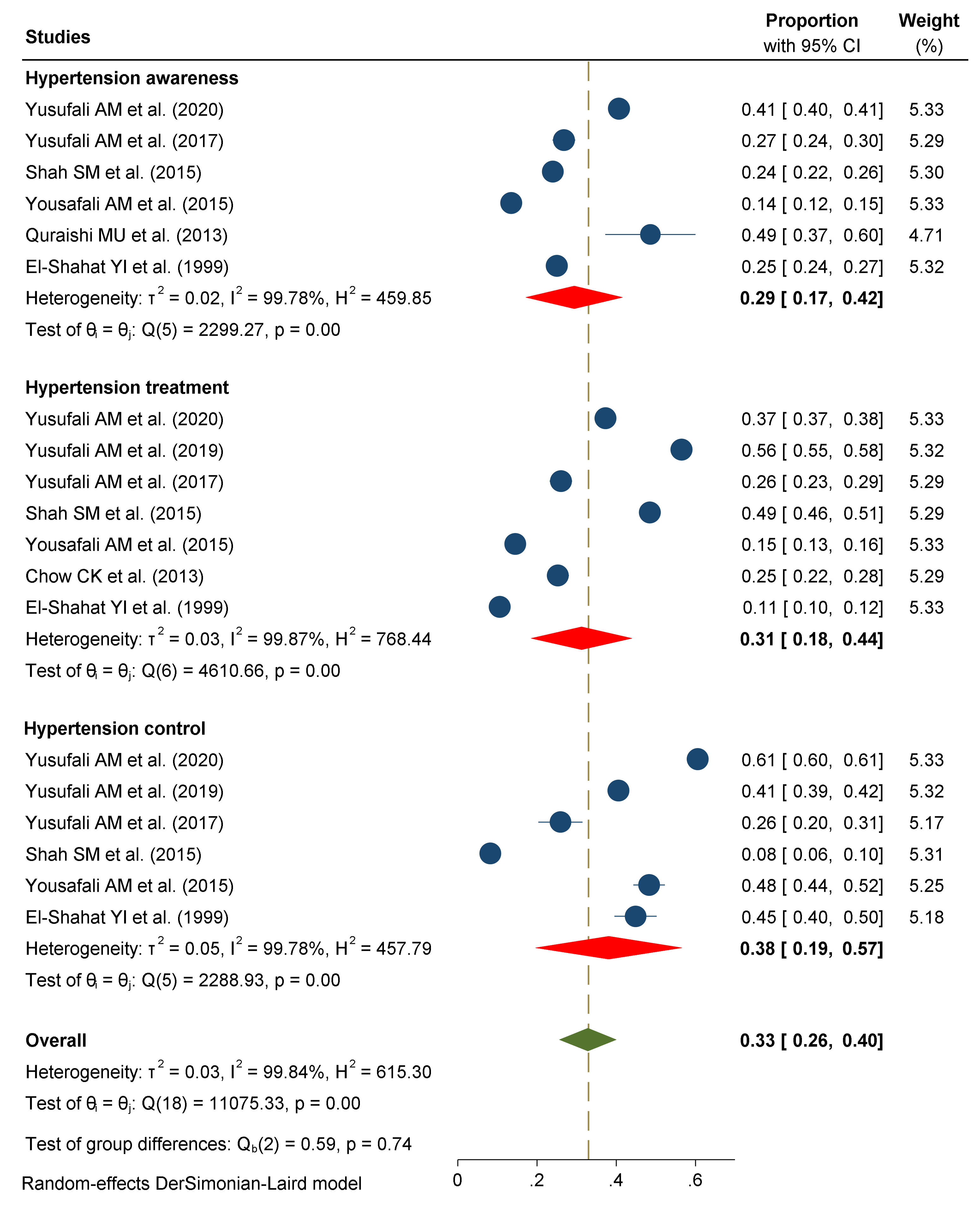
3.5. Awareness, Treatment, and Control of Hypertension
3.6. Stratified Analysis
3.7. Subgroup Analysis
3.8. Publication Bias
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Forouzanfar, M.H.; Liu, P.; Roth, G.A.; Ng, M.; Biryukov, S.; Marczak, L.; Alexander, L.; Estep, K.; Hassen Abate, K.; Akinyemiju, T.F.; et al. Global Burden of Hypertension and Systolic Blood Pressure of at Least 110 to 115 mm Hg, 1990–2015. JAMA 2017, 317, 165–182. [Google Scholar] [CrossRef] [Green Version]
- Kontis, V.; Mathers, C.D.; Rehm, J.; Stevens, G.A.; Shield, K.D.; Bonita, R.; Riley, L.M.; Poznyak, V.; Beaglehole, R.; Ezzati, M. Contribution of six risk factors to achieving the 25×25 non-communicable disease mortality reduction target: A modelling study. Lancet 2014, 384, 427–437. [Google Scholar] [CrossRef]
- Lewington, S.; Clarke, R.; Qizilbash, N.; Peto, R.; Collins, R.; Prospective Studies Collaboration. Age-specific relevance of usual blood pressure to vascular mortality: A meta-analysis of individual data for one million adults in 61 prospective studies. Lancet 2002, 360, 1903–1913. [Google Scholar] [CrossRef] [PubMed]
- Singh, G.M.; Danaei, G.; Farzadfar, F.; Stevens, G.A.; Woodward, M.; Wormser, D.; Kaptoge, S.; Whitlock, G.; Qiao, Q.; Lewington, S.; et al. The age-specific quantitative effects of metabolic risk factors on cardiovascular diseases and diabetes: A pooled analysis. PLoS ONE 2013, 8, e65174. [Google Scholar] [CrossRef] [PubMed]
- NCD Risk Factor Collaboration (NCD-RisC). Long-term and recent trends in hypertension awareness, treatment, and control in 12 high-income countries: An analysis of 123 nationally representative surveys. Lancet 2019, 394, 639–651. [Google Scholar] [CrossRef] [Green Version]
- O’Donnell, M.; Hankey, G.J.; Rangarajan, S.; Chin, S.L.; Rao-Melacini, P.; Ferguson, J.; Xavier, D.; Lisheng, L.; Zhang, H.; Pais, P.; et al. Variations in knowledge, awareness and treatment of hypertension and stroke risk by country income level. Heart 2020, 107, 282–289. [Google Scholar] [CrossRef]
- Chow, C.K.; Teo, K.K.; Rangarajan, S.; Islam, S.; Gupta, R.; Avezum, A.; Bahonar, A.; Chifamba, J.; Dagenais, G.; Diaz, R.; et al. PURE (Prospective Urban Rural Epidemiology) Study investigators. Prevalence, awareness, treatment, and control of hypertension in rural and urban communities in high-, middle-, and low-income countries. JAMA 2013, 310, 959–968. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yusufali, A.M.; Khatib, R.; Islam, S.; Alhabib, K.F.; Bahonar, A.; Swidan, H.M.; Khammash, U.; Alshamiri, M.Q.; Rangarajan, S. Prevalence, awareness, treatment and control of hypertension in four Middle East countries. J. Hypertens. 2017, 35, 1457–1464. [Google Scholar] [CrossRef]
- Saka, M.; Shabu, S.; Shabila, N. Prevalence of hypertension and associated risk factors in older adults in Kurdistan, Iraq. East. Mediterr. Health J. 2020, 26, 268–275. [Google Scholar] [CrossRef]
- Yusufali, A.; Bazargani, N.; Agrawal, A.; Muhammed, K.; Obaid, H.; Gabroun, A.; Albadwawi, M.; Albawab, A.; Musa, A.; Alraeesi, F.; et al. May Measurement Month 2017: An analysis of blood pressure screening results from the United Arab Emirates-Northern Africa and Middle East. Eur. Heart J. Suppl. 2019, 21 (Suppl. D), D118–D120. [Google Scholar] [CrossRef]
- Arnaout, M.S.; Almahmeed, W.; Ibrahim, M.; Ker, J.; Khalil, M.T.; Van Wyk, C.T.; Mancia, G.; Al Mousa, E. Hypertension and its management in countries in Africa and the Middle East, with special reference to the place of β-blockade. Curr. Med. Res. Opin. 2011, 27, 1223–1236. [Google Scholar] [CrossRef]
- Motlagh, B.; O’Donnell, M.; Yusuf, S. Prevalence of cardiovascular risk factors in the Middle East: A systematic review. Eur. J. Cardiovasc. Prev. Rehabil. 2009, 16, 268–280. [Google Scholar] [CrossRef] [PubMed]
- Hajat, C.; Harrison, O.; Al Siksek, Z. Weqaya: A population-wide cardiovascular screening program in Abu Dhabi, United Arab Emirates. Am. J. Public Health 2012, 102, 909–914. [Google Scholar] [CrossRef]
- Yusufali, A.; Bazargani, N.; Bin Belaila, B.A.; Suhail, A.M.; Shuri, H.H.; Agrawal, A.; Muhammed, K.; Gabroun, A.; Albawab, A.; Vazir, Z.; et al. May Measurement Month 2018: An analysis of blood pressure screening results from United Arab Emirates. Eur. Heart J. Suppl. 2020, 22 (Suppl. H), H128–H131. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.M.; Loney, T.; Sheek-Hussein, M.; El Sadig, M.; Al Dhaheri, S.; El Barazi, I.; Al Marzouqi, L.; Aw, T.C.; Ali, R. Hypertension prevalence, awareness, treatment, and control, in male South Asian immigrants in the United Arab Emirates: A cross-sectional study. BMC Cardiovasc. Disord. 2015, 15, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khan, S.; Ali, S.A. Exploratory study into awareness of heart disease and health care seeking behavior among Emirati women (UAE)—Cross sectional descriptive study. BMC Womens Health 2017, 17, 88. [Google Scholar] [CrossRef]
- Akl, C.; Akik, C.; Ghattas, H.; Obermeyer, C.M. The cascade of care in managing hypertension in the Arab world: A systematic assessment of the evidence on awareness, treatment and control. BMC Public Health 2020, 20, 835. [Google Scholar] [CrossRef]
- Bhagavathula, A.S.; Shehab, A.; Ullah, A.; Rahmani, J. The Burden of Cardiovascular Disease Risk Factors in the Middle East: A Systematic Review and Meta-Analysis Focusing on Primary Prevention. Curr. Vasc. Pharmacol. 2021, 19, 379–389. [Google Scholar] [CrossRef]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef]
- Hussain, H.Y.; Salim, N.A.; Tuffaha, M.G.; Ayoub, A.Y. Systolic and diastolic hypertension among Dubai population, utilizing household survey data, risk approach analysis, 2019. Int. J. Biomed. Clin. Sci. 2019, 4, 115–120. [Google Scholar]
- Alzaabi, A.; Al-Kaabi, J.; Al-Maskari, F.; Farhood, A.F.; Ahmed, L.A. Prevalence of diabetes and cardio-metabolic risk factors in young men in the United Arab Emirates: A cross-sectional national survey. Endocrinol. Diab. Metabol. 2019, 2, e00081. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al Faisal, W.; Hussein, H. Hypertension: Discrepancy between Enquiry and Measurement, Understanding Blood Pressure Readings. Front. Biomed. Sci. 2017, 2, 18–22. [Google Scholar]
- Yusufali, A.; Bazargani, N.; Muhammed, K.; Gabroun, A.; AlMazrooei, A.; Agrawal, A.; Al-Mulla, A.; Hajat, C.; Baslaib, F.; Philip, J.; et al. Opportunistic Screening for CVD Risk Factors: The Dubai Shopping for Cardiovascular Risk Study (DISCOVERY). Glob. Heart. 2015, 10, 265–272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quraishi, M.U.; Begum, S.; AnshooAgarwal, S.C.; UmmulbaneenShamji, A.N.; Al Akeel, N.; Noori, M.A.; Arya, S. A Study to Know the Prevalence and Awareness of Hypertension in Market Population of Ras Al Khaimah, UAE. J. Basic Appl. Sci. Res. 2013, 3, 458–462. [Google Scholar]
- Baynouna, L.M.; Revel, A.D.; Nagelkerke, N.J.; Jaber, T.M.; Omar, A.O.; Ahmed, N.M.; Naziruldeen, M.K.; Al-Sayed, M.F.; & Nour, F.A. High prevalence of the cardiovascular risk factors in Al-Ain, United Arab Emirates. An emerging health care priority. Saudi Med. J. 2008, 29, 1173–1178. [Google Scholar]
- Al-Sarraj, T.; Saadi, H.; Volek, J.S.; Fernandez, M.L. Metabolic syndrome prevalence, dietary intake, and cardiovascular risk profile among overweight and obese adults 18–50 years old from the United Arab Emirates. Metab. Syndr. Relat. Disord. 2010, 8, 39–46. [Google Scholar] [CrossRef]
- El-Shahat, Y.I.; Bakir, S.Z.; Farjou, N.; Hashim, T.; Bohaliga, A.; Al-Hossani, H.; Jaffar, A.R. Hypertension in UAE Citizens—Preliminary Results of a Prospective Study. Saudi J. Kidney Dis. Transpl. 1999, 10, 376–381. [Google Scholar]
- el Mugamer, I.T.; Ali Zayat, A.S.; Hossain, M.M.; Pugh, R.N. Diabetes, obesity and hypertension in urban and rural people of bedouin origin in the United Arab Emirates. J. Trop. Med. Hyg. 1995, 98, 407–415. [Google Scholar]
- Zhou, B.; Perel, P.; Mensah, G.A.; Ezzati, M. Global epidemiology, health burden and effective interventions for elevated blood pressure and hypertension. Nat. Rev. Cardiol. 2021, 18, 1–18. [Google Scholar] [CrossRef]
- NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: A pooled analysis of 1201 population-representative studies with 104 million participants. Lancet 2021, 398, 957–980. [Google Scholar] [CrossRef]
- NCD Countdown 2030 collaborators. NCD Countdown 2030: Pathways to achieving Sustainable Development Goal target 3.4. Lancet 2020, 396, 918–934. [Google Scholar] [CrossRef]
- Kazim, M.N.; AbouMoussa, T.H.; AL-Hammadi, F.A.; Al Ali, A.; Abedini, F.M.; Ahmad, F.S.M.; Abdulrahman, M. Population Awareness of Cardiovascular Disease Risk factors and Health Care Seeking Behavior in the UAE. Am. J. Prev. Cardiol. 2021, 8, 100255. [Google Scholar] [CrossRef] [PubMed]
- Khawaja, A.H.; Qassim, S.; Hassan, N.A.; Arafa, E.A. Added sugar: Nutritional knowledge and consumption pattern of a principal driver of obesity and diabetes among undergraduates in UAE. Diabetes Metab. Syndr. 2019, 13, 2579–2584. [Google Scholar] [CrossRef]
- Bairapareddy, K.C.; Kamcheh, M.M.S.; Itani, R.J.; Mohamed, M.; Abdellatif Zahran, H.A.E.; Alaparthi, G.K.; Tamim, M.; Anche, P.; Chandrashekaran, B. Low Physical Activity Levels Are Linked to Early Hypertension Risk in College-Going Young Adults. Healthcare 2021, 9, 1258. [Google Scholar] [CrossRef] [PubMed]
- Sulaiman, N.; Elbadawi, S.; Hussein, A.; Abusnana, S.; Madani, A.; Mairghani, M.; Peeters, A. Prevalence of overweight and obesity in United Arab Emirates Expatriates: The UAE National Diabetes and Lifestyle Study. Diabetol. Metab. Syndr. 2017, 9, 88. [Google Scholar] [CrossRef] [Green Version]
- Shin, S.; Jee, H. Prevalence of metabolic syndrome in the Gulf Cooperation Council countries: Meta-analysis of cross-sectional studies. J. Exerc. Rehabil. 2020, 16, 27–35. [Google Scholar] [CrossRef] [Green Version]
- Radaideh, G.; Tzemos, N.; Ali, T.M.; Eldershaby, Y.; Joury, J.; Abreu, P. Cardiovascular Risk Factor Burden in the United Arab Emirates (UAE): The Africa Middle East (AfME) Cardiovascular Epidemiological (ACE) Study Sub-analysis. Int. Cardiovasc. Forum. J. 2017, 11, 6–12. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Author, Year | Study Characteristics | BP Device | Evaluation Criteria | Prevalence (%) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Location | Study Design | Setting | Population | Screened Population | Mean Age | Hypertension | Awareness | Treatment | Control | |||
| Yusufali A. et al. (2020) [14] | Seven emirates | CS | Health centers | General public | 31,316 | 36.8 (11.4) | Automated /Manual | ≥140/90 mmHg | 19.9 | 40.7 | 37.3 | 60.6 |
| Hussain H.Y. et al. (2019) [20] | Dubai | CS | Household | General public | 3289 | Manual | >130/80 mmHg | 25.1 | - | - | - | |
| Alzaabi A. et al. (2019) [21] | Abu Dhabi, Al Ain, Sharjah | CS | Medical examination centers | Men | 33,327 | 21.6 | Manual | ≥140/90 mmHg | 9.2 | - | - | - |
| Yusufali A. et al. (2019) [10] | Seven emirates | CS | Community | General public | 6193 | 38.2 (13.1) | Automated | ≥140/90 mmHg | 30.2 | - | 56.5 | 40.6 |
| Yusufali A.M. et al. (2017) [8] | Dubai | CS | Community | General public | 917 | 49.5 (10.3) | Automated | ≥140/90 mmHg | 51.9 | 26.8 | 26.1 | 25.9 |
| Al Faisal W. et al. (2017) [22] | Dubai | CS | Community | General public | 3716 | Manual | ≥140/90 mmHg | 24.0 | - | - | - | |
| Shah S.M. et al. (2015) [15] | Al Ain | CS | Community | South Asian Immigrants | 1375 | 34 | Automated | ≥140/90 mmHg | 30.5 | 24.0 | 48.5 | 8.2 |
| Yusufali A.M. et al. (2015) [23] | Dubai | CS | Community, hospital | General public | 4128 | 38.4 (11.4) | Automated | ≥140/90 mmHg | 30.5 | 13.5 | 14.5 | 48.3 |
| Quraishi M.U. et al. (2013) [24] | Ras Al Khaimah | CS | Kerala market | General public | 74 | Manual | ≥140/90 mmHg | 50.0 | 48.6 | - | - | |
| Baynouna L.M. et al. (2013) [25] | Al Ain | CS | Community | General public | 817 | Manual | ≥140/90 mmHg | 20.8 | - | - | - | |
| Chow C.K. et al. (2013) [7] | Dubai | CS | Community | General public | 918 | 49.1 (10.2) | Automated | ≥140/90 mmHg | 52.0 | - | 25.3 | - |
| Hajat C. et al. (2012) [13] | Abu Dhabi | CS | Community | General public | 50,138 | 36.8 (14.3) | Automated | ≥140/90 mmHg | 23.1 | - | - | - |
| Al-Sarraj T. et al. (2010) [26] | Al Ain | CS | Hospital | UAE citizens | 227 | 31.2 (8.9) | Automated | ≥135/85 mmHg | 51.5 | - | - | - |
| El-Shahat Y.I. et al. (1999) [27] | Abu Dhabi, Al Ain, Sharjah | CS | Community | General public | 3150 | Manual | ≥140/90 mmHg | 36.6 | 25.0 | 10.6 | 44.9 | |
| el Mugamer I.T. et al. (1995) [28] | Abu Dhabi | CS | Community | General public | 322 | Manual | ≥140/90 mmHg | 25.2 | 40.7 | 37.3 | 60.6 | |
| Characteristics | Number of Studies | Pooled Prevalence in Percentage (95% CI) | p for Interaction † | I2 (%) | Z | Heterogeneity between Groups | ||
|---|---|---|---|---|---|---|---|---|
| Q | df | p | ||||||
| Year | 0.096 | 2.80 | 1 | 0.09 | ||||
| 1995–2015 | 9 | 35 (2941) | 98.9 | 11.5 | ||||
| 2016–2020 | 6 | 27 (1934) | 99.8 | 6.84 | ||||
| Screened population | 0.001 | 4.54 | 1 | 0.03 | ||||
| ≤1000 | 6 | 42 (28–55) | 98.5 | 5.92 | ||||
| >1000 | 9 | 25 (20–31) | 99.8 | 8.72 | ||||
| Type of population | 0.008 | |||||||
| General public | 13 | 33 (29–36) | 99.1 | 18.8 | ||||
| Men only | 2 | 10 (9–10) | - | 60.9 | ||||
| Percent of female | 0.083 | 3.25 | 1 | 0.07 | ||||
| <50% | 6 | 39 (29–50) | 99.4 | 7.22 | ||||
| ≥50% | 3 | 27 (19–35) | 99.5 | 6.51 | ||||
| Type of setting | 0.387 | 2.15 | 2 | 0.34 | ||||
| Community | 11 | 33 (28–37) | 98.9 | 14.1 | ||||
| Hospital | 3 | 26 (16–35) | - | 5.50 | ||||
| Both | 1 | 31 (29–32) | - | 42.60 | ||||
| Type of device | 0.006 | 7.50 | 1 | 0.01 | ||||
| Manual | 8 | 25 (19–32) | 99.7 | 7.85 | ||||
| Automated | 7 | 38 (32–45) | 99.3 | 11.38 | ||||
| Sub-population | ||||||||
| Age ≤ 40 years | 5 | 23 (16–30) | - | 99.7 | 6.33 | 7.38 | 1 | 0.01 |
| Arab descents | 5 | 26 (22–29) | - | 99.1 | 15.37 | 2.63 | 1 | 0.10 |
| Emirati | 8 | 27 (20–35) | - | 98.8 | 7.36 | 2.95 | 1 | 0.09 |
| South Asian | 7 | 27 (24–31) | 98.8 | 17.61 | 0.96 | 1 | 0.33 | |
| Quality of studies | 0.738 | 0.06 | 1 | 0.81 | ||||
| High (> 7 score) | 6 | 33 (25–38) | 99.5 | 7.13 | ||||
| Low (≤ 7 score) | 9 | 31 (23–38) | 99.9 | 12.43 | ||||
| Subgroup | No. of Studies | Proportion (95% CI) | Test for Heterogeneity | Between Subgroup Differences | ||||
|---|---|---|---|---|---|---|---|---|
| Tau2 | I2 | Q | df | p | ||||
| Hypertension Awareness | ||||||||
| Geographic region | Abu Dhabi | 1 | 24 (22–26) | - | - | 18.8 | 3 | 0.001 |
| Dubai | 2 | 20 (7–33) | 0.01 | 98.6 | ||||
| Ras Al Khaimah | 1 | 49 (37–60) | - | - | ||||
| Multicenter | 2 | 33 (18–48) | 0.01 | 99.7 | ||||
| Study setting | Community | 4 | 27 (23–31) | 0.00 | 83.9 | 2069.9 | 2 | 0.001 |
| Healthcare | 1 | 41 (40–41) | - | - | ||||
| Both | 1 | 14 (12–15) | - | - | ||||
| Type of BP device | Manual | 2 | 25 (24–27) | 0.03 | 93.8 | 0.17 | 1 | 0.68 |
| Automated | 4 | 29 (12–46) | 0.03 | 99.8 | ||||
| Study population | General public | 5 | 31 (16–45) | 0.03 | 99.8 | 0.80 | 1 | 0.37 |
| Immigrant men | 1 | 24 (22–26) | - | - | ||||
| Population characteristics | Age ≤ 40 years | 2 | 43 (36–49) | 0.00 | 46.4 | 1.87 | 1 | 0.17 |
| Nationals | 2 | 19 (8–31) | 0.01 | 99.3 | - | - | - | |
| Expatriates | 4 | 31 (14–49) | 0.03 | 99.8 | 2142.6 | 3 | 0.001 | |
| Hypertension Treatment | ||||||||
| Geographic region | Abu Dhabi | 1 | 49 (46–51) | - | - | 45.0 | 2 | 0.001 |
| Dubai | 3 | 22 (14–29) | 0.00 | 97.0 | ||||
| Multicenter | 3 | 35 (9–61) | 0.05 | 99.9 | ||||
| Study setting | Community | 5 | 33 (17–50) | 0.04 | 99.7 | 1379.8 | 2 | 0.001 |
| Healthcare | 1 | 37 (37–38) | - | - | ||||
| Both | 1 | 15 (13–16) | - | - | ||||
| Type of device | Manual | 1 | 11 (10–12) | 0.00 | - | 15.78 | 1 | 0.001 |
| Automated | 6 | 36 (24–49) | 0.03 | 99.8 | ||||
| Study population | General public | 6 | 28 (15–42) | 0.03 | 99.8 | 8.36 | 1 | 0.001 |
| Immigrant men | 1 | 49 (46–51) | - | - | ||||
| Population characteristics | Age ≤ 40 years | 1 | 37 (37–38) | - | - | |||
| Nationals | 2 | 13 (9–16) | 0.00 | 96.1 | 25.6 | 1 | 0.001 | |
| Expatriates | 4 | 39 (21–57) | 0.03 | 99.9 | 2697.6 | 3 | 0.001 | |
| Hypertension control | ||||||||
| Geographic region | Abu Dhabi | 1 | 8 (6–10) | - | - | 47.9 | 2 | 0.001 |
| Dubai | 2 | 37 (15–59) | 0.02 | 97.5 | ||||
| Multicenter | 3 | 49 (37–61) | 0.01 | 99.2 | ||||
| Study setting | Community | 4 | 30 (14–46) | 0.03 | 99.2 | 47.4 | 2 | 0.001 |
| Healthcare | 1 | 61 (60–61) | - | - | ||||
| Both | 1 | 48 (44–52) | - | - | ||||
| Type of device | Manual | 1 | 45 (40–50) | - | - | 0.55 | 1 | 0.46 |
| Automated | 5 | 37 (16–58) | 0.06 | 99.8 | ||||
| Study population | General public | 5 | 44 (33–55) | 0.02 | 99.1 | 39.6 | 1 | 0.001 |
| Immigrant men | 1 | 8 (6–10) | - | - | ||||
| Population characteristics | Age ≤ 40 years | 1 | 61 (60–61) | - | - | |||
| Nationals | 2 | 47 (44–50) | 0.00 | 1.27 | 1.01 | 1 | 0.31 | |
| Expatriates | 4 | 39 (17–61) | 0.05 | 99.8 | 2214.3 | 3 | 0.001 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bhagavathula, A.S.; Shah, S.M.; Aburawi, E.H. Prevalence, Awareness, Treatment, and Control of Hypertension in the United Arab Emirates: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 12693. https://doi.org/10.3390/ijerph182312693
Bhagavathula AS, Shah SM, Aburawi EH. Prevalence, Awareness, Treatment, and Control of Hypertension in the United Arab Emirates: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2021; 18(23):12693. https://doi.org/10.3390/ijerph182312693
Chicago/Turabian StyleBhagavathula, Akshaya Srikanth, Syed Mahboob Shah, and Elhadi Husein Aburawi. 2021. "Prevalence, Awareness, Treatment, and Control of Hypertension in the United Arab Emirates: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 18, no. 23: 12693. https://doi.org/10.3390/ijerph182312693
APA StyleBhagavathula, A. S., Shah, S. M., & Aburawi, E. H. (2021). Prevalence, Awareness, Treatment, and Control of Hypertension in the United Arab Emirates: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 18(23), 12693. https://doi.org/10.3390/ijerph182312693