
Examining the Drivers of Racial/Ethnic Disparities in Non-Adherence to Antihypertensive Medications and Mortality Due to Heart Disease and Stroke: A County-Level Analysis

 ,
,  ,
,  , , , and
, , , and 
Abstract
:1. Background
2. Methods
2.1. Data Sources
2.2. Measurement of Determinants of Health Factors
2.3. Measurement of County-Level Non-Adherence to AHM
2.4. Measurement of Outcomes
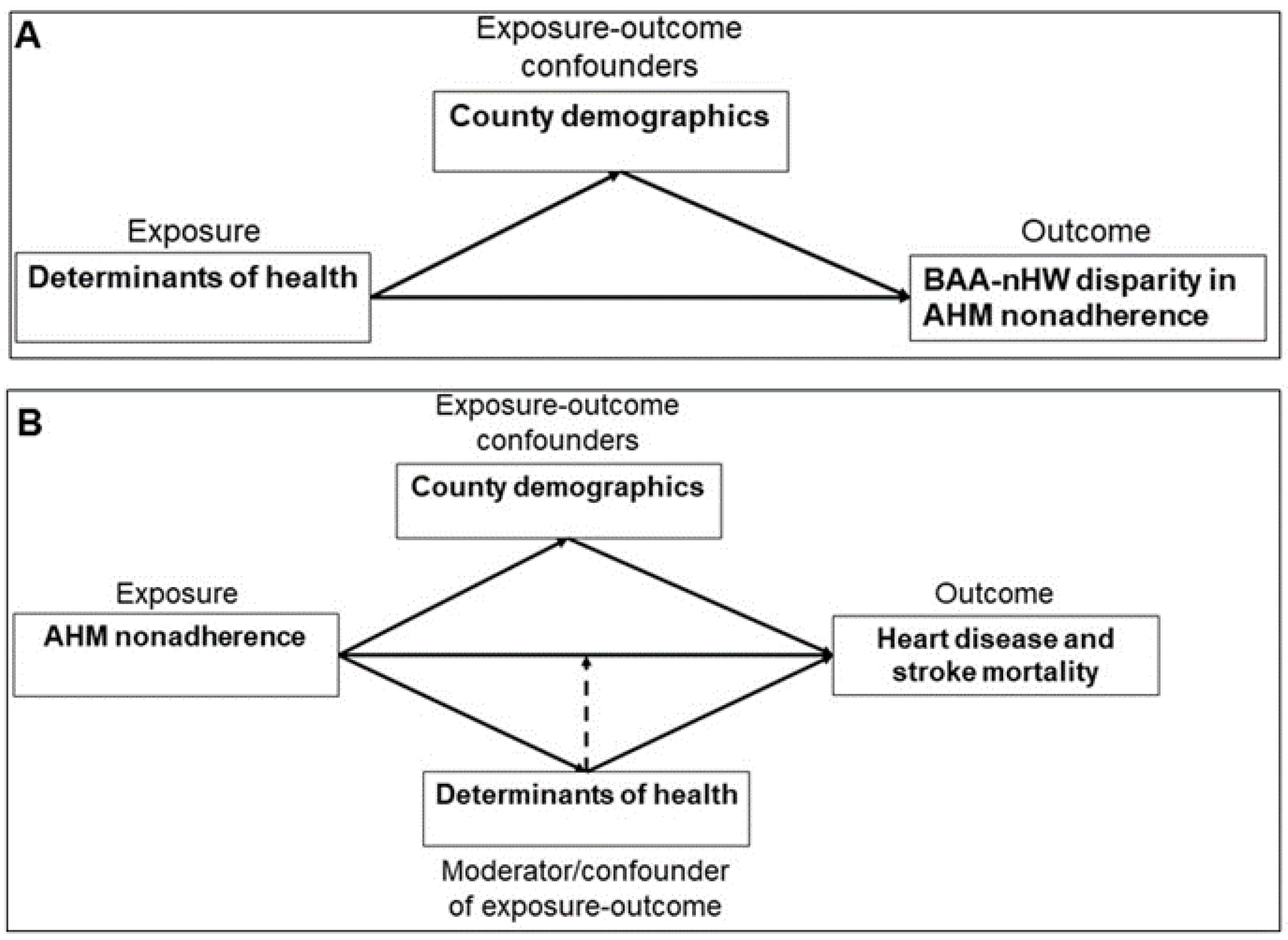
- Quantification of racial disparities in AHM non-adherence (Objective 1): We used the prevalence rate ratio (PRR), a widely used measure of racial disparities, to define the BAA–nHW disparity in AHM non-adherence [35]. For each county that presented measures of prevalence of AHM non-adherence for both BAAs and nHWs, the prevalence among BAAs was divided by that among nHWs to generate county-level PRRs.
- Assessment of heart disease and stroke mortality (Objective 2): In the CDC Atlas dataset, heart disease mortality was defined as deaths due to diseases of the circulatory system (ICD-10 codes: I00-I99, I11, I13, I20-I51). All deaths for which stroke was identified as the underlying cause were defined as stroke mortality.
2.5. Statistical Analysis
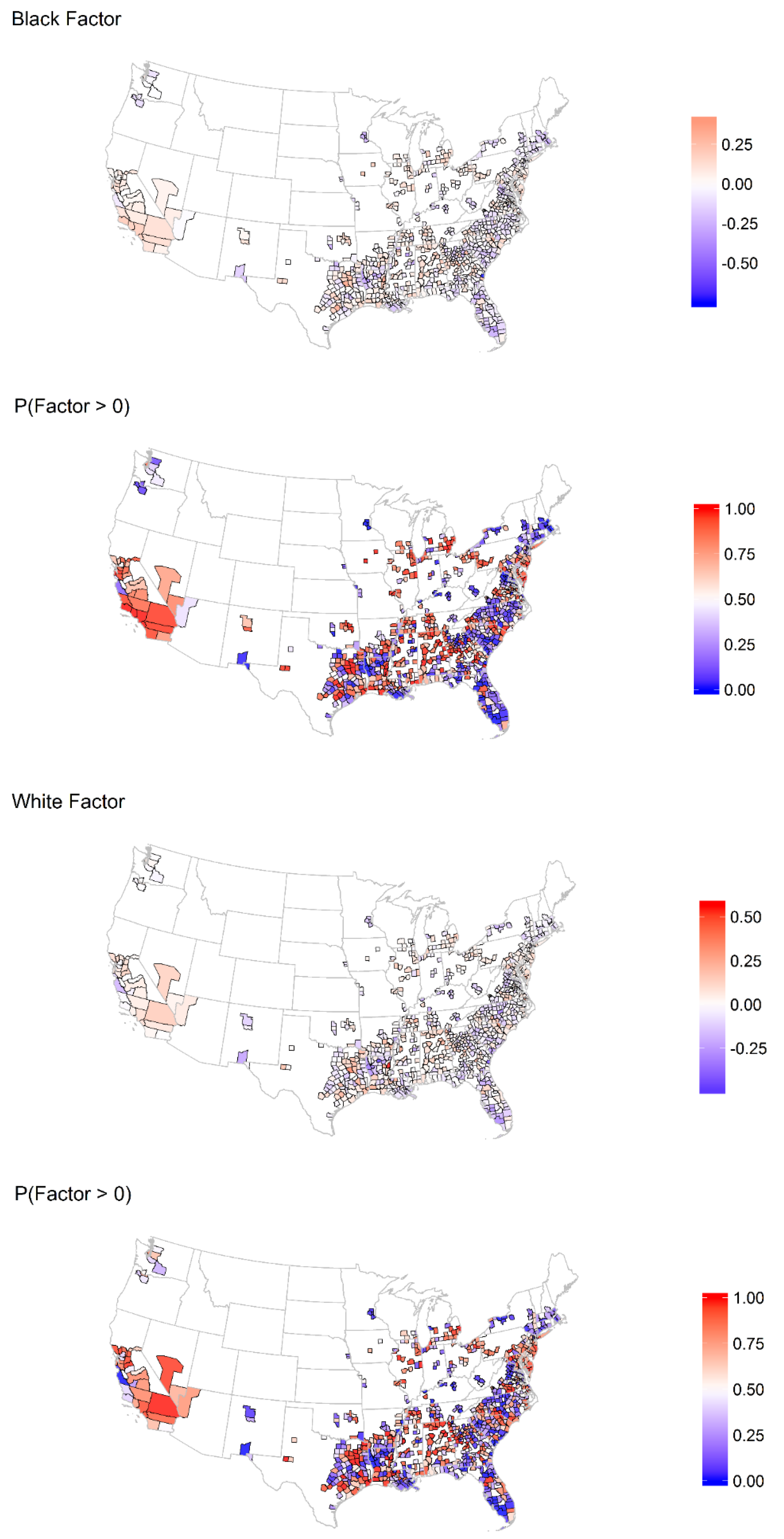
- Because not all measures of areal risk are easily measured, there are likely to be unmeasured factors that contribute to the risk of mortality from heart disease and stroke. These unmeasured factors may also differ by race/ethnicity, as racial groups may experience a common areal environment differently. To capture this variation, we included a county-level, shared racial factor in all models which accounts for correlation across outcomes within a racial group due to unmeasured factors.
- To account for correlations between races within a county, we allowed the BAA and nHW unmeasured factors within a county to be correlated.
- In addition, counties within a state were correlated because they share several health determinants, whereas states may differ with respect to these factors. To account for this, we included a state factor that is shared across all the outcomes in a state.
3. Results
3.1. The Role of County-Level Constructs of Determinants of Health in BAA–nHW Disparities in AHM Non-Adherence
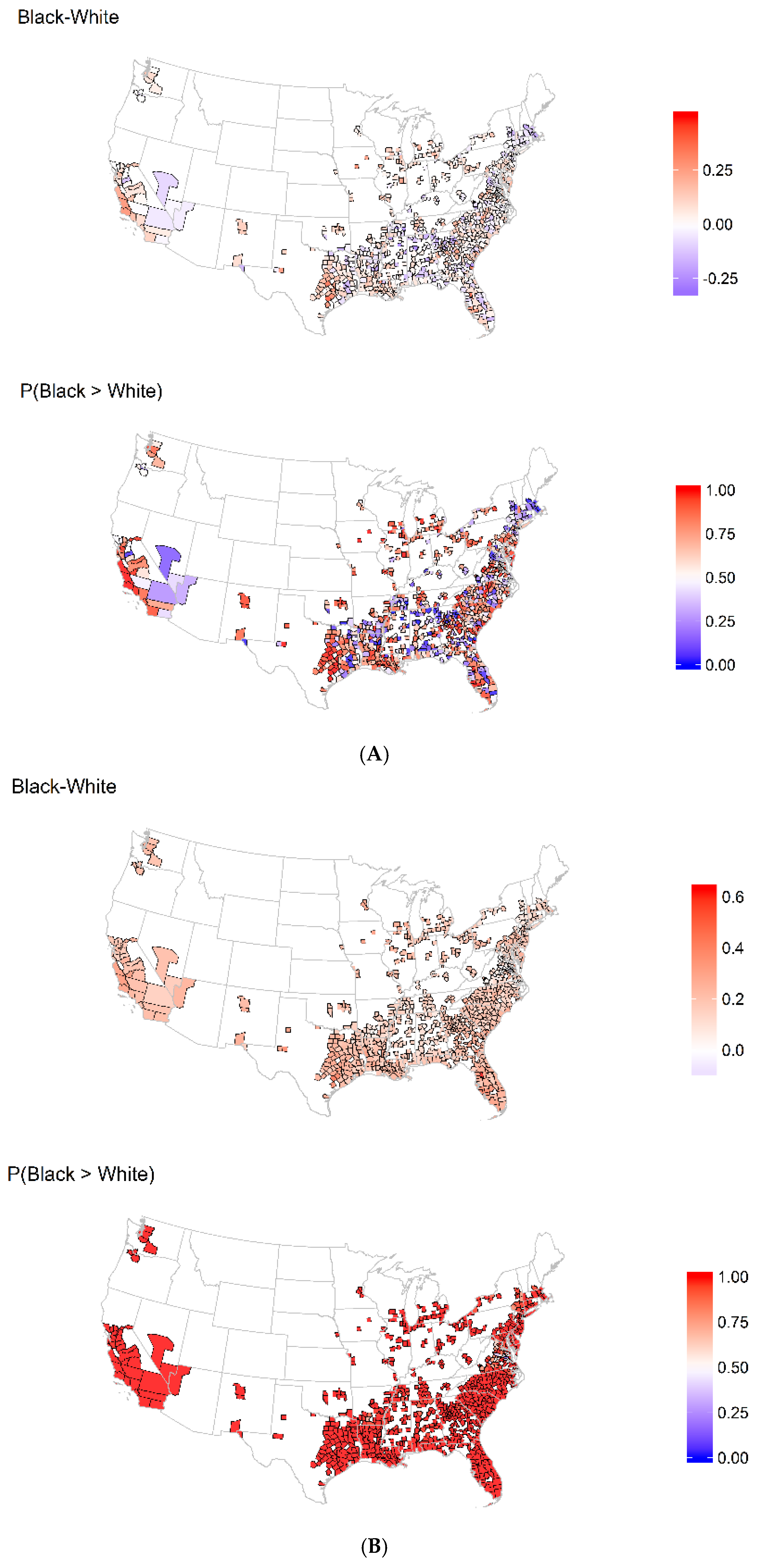
3.2. Spatial Distribution in Heart Disease and Stroke Mortality
3.3. Associations between AHM Non-Adherence and Heart Disease and Stroke Mortality by Race/Ethnicity
3.4. The Impact of Determinants of Health on the Effects of AHM Non-Adherence on Heart Disease and Stroke Mortality by Race/Ethnicity
4. Discussion
5. Limitations
6. Strengths
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Howard, G.; Prineas, R.; Moy, C.; Cushman, M.; Kellum, M.; Temple, E.; Graham, A.; Howard, V. Racial and geographic differences in awareness, treatment, and control of hypertension: The REasons for Geographic And Racial Differences in Stroke study. Stroke 2006, 37, 1171–1178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Redmond, N.; Baer, H.J.; Hicks, L.S. Health behaviors and racial disparity in blood pressure control in the national health and nutrition examination survey. Hypertension 2011, 57, 383–389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; Das, S.R.; de Ferranti, S.; Despres, J.P.; Fullerton, H.J.; et al. Heart Disease and Stroke Statistics-2016 Update: A Report From the American Heart Association. Circulation 2016, 133, e38–e360. [Google Scholar] [CrossRef]
- Chowdhury, R.; Khan, H.; Heydon, E.; Shroufi, A.; Fahimi, S.; Moore, C.; Stricker, B.; Mendis, S.; Hofman, A.; Mant, J.; et al. Adherence to cardiovascular therapy: A meta-analysis of prevalence and clinical consequences. Eur. Heart J. 2013, 34, 2940–2948. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ho, P.M.; Bryson, C.L.; Rumsfeld, J.S. Medication adherence: Its importance in cardiovascular outcomes. Circulation 2009, 119, 3028–3035. [Google Scholar] [CrossRef]
- Choudhry, N.K.; Avorn, J.; Glynn, R.J.; Antman, E.M.; Schneeweiss, S.; Toscano, M.; Reisman, L.; Fernandes, J.; Spettell, C.; Lee, J.L.; et al. Full coverage for preventive medications after myocardial infarction. N. Engl. J. Med. 2011, 365, 2088–2097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charles, H.; Good, C.B.; Hanusa, B.H.; Chang, C.C.; Whittle, J. Racial differences in adherence to cardiac medications. J. Natl. Med Assoc. 2003, 95, 17–27. [Google Scholar] [PubMed]
- Holmes, H.M.; Luo, R.; Hanlon, J.T.; Elting, L.S.; Suarez-Almazor, M.; Goodwin, J.S. Ethnic disparities in adherence to antihypertensive medications of medicare part D beneficiaries. J. Am. Geriatr. Soc. 2012, 60, 1298–1303. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Baik, S.H. Race/Ethnicity, disability, and medication adherence among medicare beneficiaries with heart failure. J. Gen. Intern. Med. 2014, 29, 602–607. [Google Scholar] [CrossRef] [Green Version]
- Cummings, D.M.; Wu, J.R.; Cene, C.; Halladay, J.; Donahue, K.E.; Hinderliter, A.; Miller, C.; Garcia, B.; Penn, D.; Tillman, J.; et al. Perceived Social Standing, Medication Nonadherence, and Systolic Blood Pressure in the Rural South. J. Rural Health 2016, 32, 156–163. [Google Scholar] [CrossRef] [Green Version]
- Rolnick, S.J.; Pawloski, P.A.; Hedblom, B.D.; Asche, S.E.; Bruzek, R.J. Patient characteristics associated with medication adherence. Clin. Med. Res. 2013, 11, 54–65. [Google Scholar] [CrossRef] [Green Version]
- Steiner, J.F.; Ho, P.M.; Beaty, B.L.; Dickinson, L.M.; Hanratty, R.; Zeng, C.; Tavel, H.M.; Havranek, E.P.; Davidson, A.J.; Magid, D.J.; et al. Sociodemographic and Clinical Characteristics Are Not Clinically Useful Predictors of Refill Adherence in Patients With Hypertension. Circ. Cardiovasc. Qual. Outcomes 2009, 2, 451–457. [Google Scholar] [CrossRef] [Green Version]
- Bosworth, H.B.; Dudley, T.; Olsen, M.K.; Voils, C.I.; Powers, B.; Goldstein, M.K.; Oddone, E.Z. Racial differences in blood pressure control: Potential explanatory factors. Am. J. Med. 2006, 119, 70-e9. [Google Scholar] [CrossRef] [Green Version]
- Butler, M.J.; Tanner, R.M.; Muntner, P.; Shimbo, D.; Bress, A.P.; Shallcross, A.J.; Sims, M.; Ogedegbe, G.; Spruill, T.M. Adherence to antihypertensive medications and associations with blood pressure among African Americans with hypertension in the Jackson Heart Study. J. Am. Soc. Hypertens. 2017, 11, 581–588. [Google Scholar] [CrossRef] [PubMed]
- Howard, G.; Lackland, D.T.; Kleindorfer, D.O.; Kissela, B.M.; Moy, C.S.; Judd, S.E.; Safford, M.M.; Cushman, M.; Glasser, S.P.; Howard, V.J. Racial differences in the impact of elevated systolic blood pressure on stroke risk. JAMA Intern. Med. 2013, 173, 46–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- James, P.A.; Oparil, S.; Carter, B.L.; Cushman, W.C.; Dennison-Himmelfarb, C.; Handler, J.; Lackland, D.T.; LeFevre, M.L.; MacKenzie, T.D.; Ogedegbe, O.; et al. 2014 evidence-based guideline for the management of high blood pressure in adults: Report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA 2014, 311, 507–520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hillemeier, M.M.; Lynch, J.; Harper, S.; Casper, M. Measuring contextual characteristics for community health. Health Serv. Res. 2003, 38, 1645–1717. [Google Scholar] [CrossRef] [Green Version]
- Havranek, E.P.; Mujahid, M.S.; Barr, D.A.; Blair, I.V.; Cohen, M.S.; Cruz-Flores, S.; Davey-Smith, G.; Dennison-Himmelfarb, C.R.; Lauer, M.S.; Lockwood, D.W.; et al. Social Determinants of Risk and Outcomes for Cardiovascular Disease: A Scientific Statement From the American Heart Association. Circulation 2015, 132, 873–898. [Google Scholar] [CrossRef] [Green Version]
- Marmot, M.; Friel, S. Global health equity: Evidence for action on the social determinants of health. J. Epidemiol. Community Health 2008, 62, 1095–1097. [Google Scholar] [CrossRef] [PubMed]
- Morenoff, J.D.; House, J.S.; Hansen, B.B.; Williams, D.R.; Kaplan, G.A.; Hunte, H.E. Understanding social disparities in hypertension prevalence, awareness, treatment, and control: The role of neighborhood context. Soc. Sci. Med. 2007, 65, 1853–1866. [Google Scholar] [CrossRef]
- Billimek, J.; Sorkin, D.H. Self-reported neighborhood safety and nonadherence to treatment regimens among patients with type 2 diabetes. J. Gen. Intern. Med. 2012, 27, 292–296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mujahid, M.S.; Diez Roux, A.V.; Morenoff, J.D.; Raghunathan, T.E.; Cooper, R.S.; Ni, H.; Shea, S. Neighborhood characteristics and hypertension. Epidemiology 2008, 19, 590–598. [Google Scholar] [CrossRef]
- Kershaw, K.N.; Osypuk, T.L.; Do, D.P.; De Chavez, P.J.; Diez Roux, A.V. Neighborhood-level racial/ethnic residential segregation and incident cardiovascular disease: The multi-ethnic study of atherosclerosis. Circulation 2015, 131, 141–148. [Google Scholar] [CrossRef] [Green Version]
- Liu, L.; Nunez, A.E.; Yu, X.; Yin, X.; Eisen, H.J.; Urban Health Research, G. Multilevel and spatial-time trend analyses of the prevalence of hypertension in a large urban city in the USA. J. Urban. Health 2013, 90, 1053–1063. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shin, J.; Choi, Y.; Kim, S.W.; Lee, S.G.; Park, E.C. Cross-level interaction between individual socioeconomic status and regional deprivation on overall survival after onset of ischemic stroke: National health insurance cohort sample data from 2002 to 2013. J. Epidemiol. 2017, 27, 381–388. [Google Scholar] [CrossRef] [PubMed]
- Xu, H. Comparing Spatial and Multilevel Regression Models for Binary Outcomes in Neighborhood Studies. Sociol. Methodol. 2014, 44, 229–272. [Google Scholar] [CrossRef]
- Acevedo-Garcia, D.; Diez-Roux, A.V.; Geiger, J.; Godsil, R.D.; James, S.; Krieger, N.; Randall, V.R.; Smith, D.B.; Williams, D.R. Unequal Health Outcomes in the United States: Racial and Ethnic Disparities in Health Care Treatment and Access, the Role of Social and Environmental Determinants of Health, and the Responsibility of the State; PRRAC: Washington, DC, USA, 2008. [Google Scholar]
- Diez-Roux, A.V. Bringing context back into epidemiology: Variables and fallacies in multilevel analysis. Am. J. Public Health 1998, 88, 216–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Freccero, C.; Sundquist, K.; Sundquist, J.; Ji, J. Primary adherence to antidepressant prescriptions in primary health care: A population-based study in Sweden. Scand. J. Prim. Health Care 2016, 34, 83–88. [Google Scholar] [CrossRef] [Green Version]
- van Geffen, E.C.; Gardarsdottir, H.; van Hulten, R.; van Dijk, L.; Egberts, A.C.; Heerdink, E.R. Initiation of antidepressant therapy: Do patients follow the GP’s prescription? Br. J. Gen. Pract. 2009, 59, 81–87. [Google Scholar] [CrossRef]
- Remington, P.L.; Catlin, B.B.; Gennuso, K.P. The County Health Rankings: Rationale and methods. Popul. Health Metr. 2015, 13, 11. [Google Scholar] [CrossRef] [Green Version]
- Steiner, J.F.; Koepsell, T.D.; Fihn, S.D.; Inui, T.S. A general method of compliance assessment using centralized pharmacy records. Description and validation. Med. Care 1988, 26, 814–823. [Google Scholar] [CrossRef]
- Steiner, J.F.; Prochazka, A.V. The assessment of refill compliance using pharmacy records: Methods, validity, and applications. J. Clin. Epidemiol. 1997, 50, 105–116. [Google Scholar] [CrossRef]
- Osterberg, L.; Blaschke, T. Adherence to medication. N. Engl. J. Med. 2005, 353, 487–497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keppel, K.; Pamuk, E.; Lynch, J.; Carter-Pokras, O.; Kim, I.; Mays, V.; Pearcy, J.; Schoenbach, V.; Weissman, J.S. Methodological issues in measuring health disparities. Vital. Health Stat. 2005, 2, 1–16. [Google Scholar]
- Singer, J.D.; Willett, J.B. Applied Longitudinal Data Analysis: Modeling Change and Event Occurrence; Oxford University Press: New York, NY, USA, 2003. [Google Scholar]
- Knorr-Held, L.; Best, N.G. A shared component model for detecting joint and selective clustering of two diseases. J. R. Stat. Soc. Ser. 2001, 164, 73–85. [Google Scholar] [CrossRef]
- SKRONDAL, A.; RABE-HESKETH, S. Latent Variable Modelling: A Survey. Scand. J. Stat. 2007, 34, 712–745. [Google Scholar] [CrossRef] [Green Version]
- Muthen, B.; Asparouhov, T. Bayesian structural equation modeling: A more flexible representation of substantive theory. Psychol. Methods 2012, 17, 313–335. [Google Scholar] [CrossRef]
- de Valpine, P.; Turek, D.; Paciorek, C.J.; Anderson-Bergman, C.; Lang, D.T.; Bodik, R. Programming With Models: Writing Statistical Algorithms for General Model Structures With NIMBLE. J. Comput. Graph. Stat. 2017, 26, 403–413. [Google Scholar] [CrossRef] [Green Version]
- Dahlof, B.; Devereux, R.B.; Kjeldsen, S.E.; Julius, S.; Beevers, G.; de Faire, U.; Fyhrquist, F.; Ibsen, H.; Kristiansson, K.; Lederballe-Pedersen, O.; et al. Cardiovascular morbidity and mortality in the Losartan Intervention For Endpoint reduction in hypertension study (LIFE): A randomised trial against atenolol. Lancet 2002, 359, 995–1003. [Google Scholar] [CrossRef]
- Furberg, C.D.; Wright, J.T.; Davis, B.R.; Cutler, J.A.; Alderman, M.; Black, H.; Cushman, W.; Grimm, R.; Leenen, F.; Pelosi, J. Major outcomes in high-risk hypertensive patients randomized to angiotensin-converting enzyme inhibitor or calcium channel blocker vs diuretic: The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT). J. Am. Med Assoc. 2002, 288, 2981–2997. [Google Scholar]
- Park, I.U.; Taylor, A.L. Race and ethnicity in trials of antihypertensive therapy to prevent cardiovascular outcomes: A systematic review. Ann. Fam. Med. 2007, 5, 444–452. [Google Scholar] [CrossRef]
- Chen, J.; Hoek, G. Long-term exposure to PM and all-cause and cause-specific mortality: A systematic review and meta-analysis. Environ. Int 2020, 143, 105974. [Google Scholar] [CrossRef] [PubMed]
- Juarez, P.D.; Tabatabai, M.; Valdez, R.B.; Hood, D.B.; Im, W.; Mouton, C.; Colen, C.; Al-Hamdan, M.Z.; Matthews-Juarez, P.; Lichtveld, M.Y.; et al. The Effects of Social, Personal, and Behavioral Risk Factors and PM2.5 on Cardio-Metabolic Disparities in a Cohort of Community Health Center Patients. Int. J. Environ. Res. Public Health 2020, 17, 3561. [Google Scholar] [CrossRef]
- Lee, Y.M.; Kim, R.B.; Lee, H.J.; Kim, K.; Shin, M.H.; Park, H.K.; Ahn, S.K.; Kim, S.Y.; Lee, Y.H.; Kim, B.G.; et al. Relationships among medication adherence, lifestyle modification, and health-related quality of life in patients with acute myocardial infarction: A cross-sectional study. Health Qual. Life Outcomes 2018, 16, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Shani, M.; Schonmann, Y.; Comaneshter, D.; Lustman, A. The Relationship Between Patient Medication Adherence and Following Preventive Medicine Recommendation. J. Am. Board Fam Med. 2021, 34, 1157–1162. [Google Scholar] [CrossRef] [PubMed]
- Schisterman, E.F.; Cole, S.R.; Platt, R.W. Overadjustment bias and unnecessary adjustment in epidemiologic studies. Epidemiology 2009, 20, 488–495. [Google Scholar] [CrossRef] [Green Version]
- Pampel, F.C.; Krueger, P.M.; Denney, J.T. Socioeconomic Disparities in Health Behaviors. Annu. Rev. Sociol. 2010, 36, 349–370. [Google Scholar] [CrossRef] [Green Version]
- Giles-Corti, B.; Donovan, R.J. Socioeconomic status differences in recreational physical activity levels and real and perceived access to a supportive physical environment. Prev. Med. 2002, 35, 601–611. [Google Scholar] [CrossRef] [PubMed]
- Sugiyama, T.; Howard, N.J.; Paquet, C.; Coffee, N.T.; Taylor, A.W.; Daniel, M. Do relationships between environmental attributes and recreational walking vary according to area-level socioeconomic status? J. Urban. Health 2015, 92, 253–264. [Google Scholar] [CrossRef] [Green Version]
- Saint Onge, J.M.; Krueger, P.M. Health Lifestyle Behaviors among U.S. Adults. SSM Popul. Health 2017, 3, 89–98. [Google Scholar] [CrossRef]
- Matthews, K.A.; Croft, J.B.; Liu, Y.; Lu, H.; Kanny, D.; Wheaton, A.G.; Cunningham, T.J.; Khan, L.K.; Caraballo, R.S.; Holt, J.B.; et al. Health-Related Behaviors by Urban-Rural County Classification-United States, 2013. MMWR Surveill. Summ. 2017, 66, 1. [Google Scholar] [CrossRef] [PubMed]
- Akbarpour, S.; Khalili, D.; Zeraati, H.; Mansournia, M.A.; Ramezankhani, A.; Fotouhi, A. Healthy lifestyle behaviors and control of hypertension among adult hypertensive patients. Sci. Rep. 2018, 8, 1–9. [Google Scholar] [CrossRef]
- Naci, H.; Ioannidis, J.P. Comparative effectiveness of exercise and drug interventions on mortality outcomes: Metaepidemiological study. BMJ 2013, 347, f5577. [Google Scholar] [CrossRef] [Green Version]
- Delgado-Rodriguez, M.; Llorca, J. Bias. J. Epidemiol. Community Health 2004, 58, 635–641. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, T.J.; Bridges, J.F.P.; Bynum, M.; Jackson, J.W.; Joseph, J.J.; Fischer, M.A.; Lu, B.; Donneyong, M.M. Association Between Patient-Clinician Relationships and Adherence to Antihypertensive Medications Among Black Adults: An Observational Study Design. J. Am. Heart Assoc. 2021, 10, e019943. [Google Scholar] [CrossRef]
- Schoenthaler, A.; Montague, E.; Baier Manwell, L.; Brown, R.; Schwartz, M.D.; Linzer, M. Patient-physician racial/ethnic concordance and blood pressure control: The role of trust and medication adherence. Ethn. Health 2014, 19, 565–578. [Google Scholar] [CrossRef] [Green Version]
- Kindig, D.; Stoddart, G. What is population health? Am. J. Public Health 2003, 93, 380–383. [Google Scholar] [CrossRef] [PubMed]
- Zullig, L.L.; Blalock, D.V.; Dougherty, S.; Henderson, R.; Ha, C.C.; Oakes, M.M.; Bosworth, H.B. The new landscape of medication adherence improvement: Where population health science meets precision medicine. Patient Prefer. Adherence 2018, 12, 1225–1230. [Google Scholar] [CrossRef] [Green Version]
- Krumme, A.A.; Glynn, R.J.; Schneeweiss, S.; Gagne, J.J.; Dougherty, J.S.; Brill, G.; Choudhry, N.K. Medication Synchronization Programs Improve Adherence To Cardiovascular Medications And Health Care Use. Health Aff. 2018, 37, 125–133. [Google Scholar] [CrossRef]
- Seabury, S.A.; Dougherty, J.S.; Sullivan, J. Medication adherence as a measure of the quality of care provided by physicians. Am. J. Manag. Care 2019, 25, 78–83. [Google Scholar] [CrossRef] [PubMed]
- Centers for Medicare & Medicaid Services. Part. C & D Star Ratings Technical Notes. 2019. Available online: https://www.cms.gov/Medicare/Prescription-Drug-Coverage/PrescriptionDrugCovGenIn/Downloads/2019-Technical-Notes.pdf (accessed on 28 October 2021).




{kind=link}
{kind=link}
{kind=link}
| Means Scores (Standard Deviation) | |||||
|---|---|---|---|---|---|
| Variable | Overall | Midwest | Northeast | South | West |
| Measures of non-adherence | |||||
| BAA AHM non-adherence (%) | 34.6 (3.4) | 32.1 (1.8) | 31.9 (2.2) | 35.5 (3.2) | 31.8 (2.8) |
| White AHM non-adherence (%) | 25.5 (3.4) | 21.2 (2.0) | 21.5 (2.0) | 26.7 (2.8) | 23.8 (2.3) |
| Determinants of health scores | |||||
| Health Behavior | 0.06 (0.68) | −0.07 (0.48) | −0.65 (0.47) | 0.23 (0.63) | −0.83 (0.50) |
| Clinical Care | 0.02 (0.56) | −0.43 (0.37) | −0.53 (0.39) | 0.17 (0.52) | −0.19 (0.40) |
| Physical Environment | 0.18 (0.39) | 0.27 (0.35) | 0.09 (0.23) | 0.21 (0.40) | −0.26 (0.36) |
| Social Economic Factors (%) | 0.21 (0.69) | −0.17 (0.61) | −0.25 (0.57) | 0.33 (0.67) | 0.17 (0.68) |
| Demographic factors | |||||
| Black/African American population (%) | 20.5 (16.0) | 11.4 (8.5) | 9.7 (7.8) | 24.3 (16.2) | 4.1 (3.2) |
| Over Age 65 (%) | 15.9 (4.1) | 14.7 (2.4) | 16.1 (2.7) | 16.2 (4.4) | 13.8 (3.6) |
| Female (%) | 50.7 (1.9) | 51.0 (0.73) | 51.2 (0.75) | 50.7 (2.2) | 50.1 (1.1) |
| Rural (%) | 39.5 (29.1) | 17.7 (15.3) | 17.2 (18.0) | 47.5 (28.3) | 9.9 (8.4) |
| Constructs of Determinants of Health | Regression Coefficients | |||
|---|---|---|---|---|
| Model 1 | Model 2 | Model 3 | Model 4 | |
| Health Behaviors | −0.17 ** | −0.17 ** | 0.05 | 0.11 |
| Clinical Care | −0.31 ** | −0.31 ** | −0.30 ** | −0.21 ** |
| Social and Economic | −0.16 ** | −0.16 ** | −0.06 | −0.11 * |
| Physical Environment | −0.03 | −0.04 | −0.01 | 0.00 |
| Pseudo-R2 | N/A | N/A | 0.24 | 0.25 |
| Predictor | BAA Heart Disease | BAA Stroke | nHW Heart Disease | nHW Stroke | ||||
|---|---|---|---|---|---|---|---|---|
| Posterior Mean Estimate (95% CI) | p (Effect > 0) | Posterior Mean Estimate (95% CI) | p (Effect > 0) | Posterior Mean Estimate (95% CI) | p (Effect > 0) | Posterior Mean Estimate (95% CI) | p (Effect > 0) | |
| BAA AHM Non-adherence | 0.043 (0.027, 0.058) | 1.00 | 0.043 (0.023, 0.065) | 1.00 | n/a | n/a | n/a | n/a |
| nHW AHM Non-adherence | n/a | n/a | n/a | 0.065 (0.047, 0.082) | 1.00 | 0.032 (0.011, 0.052) | 1.00 | |
| BAA Heart Disease | BAA Stroke | White Heart Disease | White Stroke | |||||
|---|---|---|---|---|---|---|---|---|
| Posterior Mean Estimate (95% CI) | p (Effect > 0) | Posterior Mean Estimate (95% CI) | p (Effect > 0) | Posterior Mean Estimate (95% CI) | p (Effect > 0) | Posterior Mean Estimate (95% CI) | p (Effect > 0) | |
| AHM non-adherence interaction with: | ||||||||
| Health Behavior | −0.011 (−0.031, 0.009) | 0.14 | −0.010 (−0.035, 0.015) | 0.21 | −0.009 (−0.028, 0.009) | 0.16 | 0.015 (−0.006, 0.037) | 0.92 |
| Clinical Care | −0.020 (−0.038, −0.002) | 0.02 | 0.006 (−0.018, 0.031) | 0.71 | 0.004 (−0.012, 0.020) | 0.68 | −0.008 (−0.025, 0.011) | 0.20 |
| Physical Environment | −0.018 (−0.031, −0.004) | 0.01 | −0.010 (−0.028, 0.007) | 0.14 | −0.007 (−0.019, 0.005) | 0.13 | −0.009 (−0.023, 0.005) | 0.11 |
| Social and economic Factors | 0.014 (−0.008, 0.035) | 0.89 | −0.018 (−0.046, 0.008) | 0.09 | 0.007 (−0.013, 0.026) | 0.76 | −0.027 (−0.049, −0.005) | 0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Donneyong, M.M.; Fischer, M.A.; Langston, M.A.; Joseph, J.J.; Juarez, P.D.; Zhang, P.; Kline, D.M. Examining the Drivers of Racial/Ethnic Disparities in Non-Adherence to Antihypertensive Medications and Mortality Due to Heart Disease and Stroke: A County-Level Analysis. Int. J. Environ. Res. Public Health 2021, 18, 12702. https://doi.org/10.3390/ijerph182312702
Donneyong MM, Fischer MA, Langston MA, Joseph JJ, Juarez PD, Zhang P, Kline DM. Examining the Drivers of Racial/Ethnic Disparities in Non-Adherence to Antihypertensive Medications and Mortality Due to Heart Disease and Stroke: A County-Level Analysis. International Journal of Environmental Research and Public Health. 2021; 18(23):12702. https://doi.org/10.3390/ijerph182312702
Chicago/Turabian StyleDonneyong, Macarius M., Michael A. Fischer, Michael A. Langston, Joshua J. Joseph, Paul D. Juarez, Ping Zhang, and David M. Kline. 2021. "Examining the Drivers of Racial/Ethnic Disparities in Non-Adherence to Antihypertensive Medications and Mortality Due to Heart Disease and Stroke: A County-Level Analysis" International Journal of Environmental Research and Public Health 18, no. 23: 12702. https://doi.org/10.3390/ijerph182312702
APA StyleDonneyong, M. M., Fischer, M. A., Langston, M. A., Joseph, J. J., Juarez, P. D., Zhang, P., & Kline, D. M. (2021). Examining the Drivers of Racial/Ethnic Disparities in Non-Adherence to Antihypertensive Medications and Mortality Due to Heart Disease and Stroke: A County-Level Analysis. International Journal of Environmental Research and Public Health, 18(23), 12702. https://doi.org/10.3390/ijerph182312702