
Gait Assessment Using Wearable Sensor-Based Devices in People Living with Dementia: A Systematic Review






Abstract
:1. Introduction
2. Methods
2.1. Search Strategy for Identification of Studies
2.2. Study Selection
- Original research articles in peer reviewed journals in the English language;
- Studies including human individuals over 60 years old, with existing dementia;
- Studies that focused on gait assessment using body-worn, sensor-based tools in a clinical or community-based setting or in a “real life” environment;
- Wearable devices would be small and easy to use and unobtrusive for the desired gait analysis.
2.3. Data Extraction
2.4. Methodological Quality
3. Results
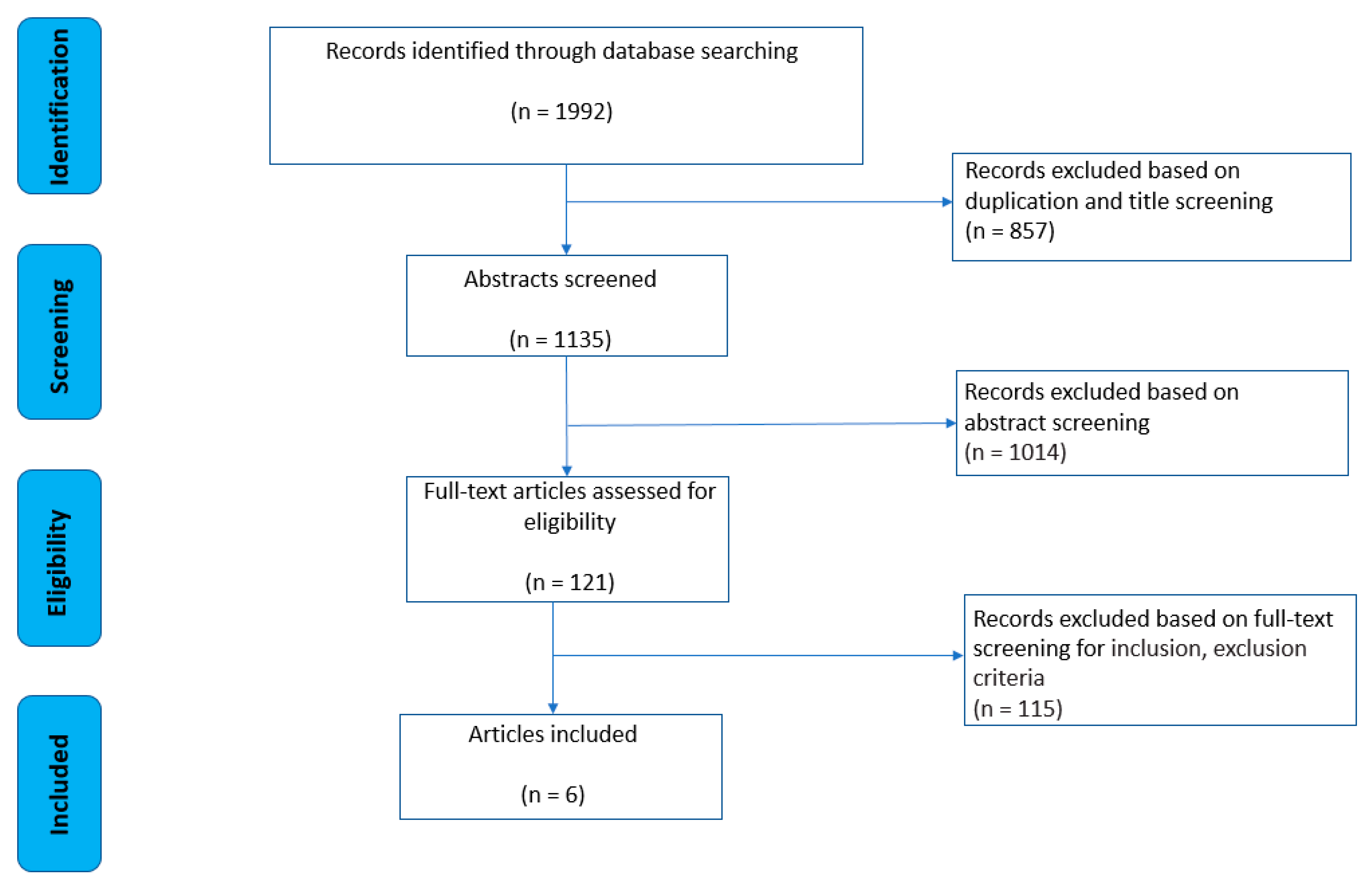
3.1. Search Results
3.2. Study Characteristics
3.3. Study Parameters and Outcome Measures
3.3.1. Sensor Type and Body Location
3.3.2. Gait Assessment Protocol
3.3.3. Calculated Parameters
3.4. Methodological Quality

{kind=link}
| Author [ref’] | Country | Aim | Population Type | Selection Criteria of Dementia Participants | Participants Characteristics |
|---|---|---|---|---|---|
| Ardle et al., 2020 | UK | To assess whether a single accelerometer-based wearable could differentiate dementia disease subtypes through gait analysis | (1) Alzheimer’s disease dementia (ADD), (2) dementia Lewy bodies (DLB), (3) Parkinson’s disease dementia (PDD). | Inclusion: (1) over 60 years old, (2) able to walk for two minutes, as ascertained by self-report. Exclusion: (1) had drug-induced or vascular parkinsonism, (2) any co-existing neurological conditions or movement disorders other than AD, DLB or PD, (3) severe mental illness (major depression, bipolar disorder, schizophrenia), (4) evidence of stroke affecting motor function, or (5) poor command of the English language. | N: 32 (ADD); Gender: M/F: 15/17; Age: 77 ± 6; N: 28 (DLB); Gender: M/F: 22/6; Age: 76 ± 6; N: 14 (PDD); Gender: M/F: 13/1; Age: 76 ± 6 |
| Gietzelt et al., 2014 | Germany | To make a fall prognosis in a cohort of older people with dementia in short-term (2 month), mid-term (4 month), and long-term (8 month) Intervals using accelerometry during the subjects’ everyday life. | adults with dementia | Inclusion: (1) over 65 years, (2) can do TUG > 15 s, (3) Mini Mental State Examination (MMSE) 524 points, (4) recurrent falls, (5) signed written informed consent by the subjects’ legal guardians. Exclusion: (1) not able to walk independently. | N: 40 Gender: M/F: 20/20 Age: 76.0 ± 8.3 |
| Williams et al., 2018 | UK | To explore relationships between the instrumented Timed Up and Go test (iTUG) and the following risk factors for falls: cognitive functioning, fear of falling (FoF), and quality of life (QoL) in people with dementia. | adults with dementia | Inclusion: (1) living at home, (2) have a diagnosis of a dementia, (3) able and willing to complete weekly standing Tai Chi without physical assistance. Exclusion: (1) living in a care home or in receipt of palliative care, (2) severe dementia (>9 on M-ACE scale), (3) a Lewy body dementia or dementia with Parkinson’s disease, (4) severe sensory impairment, (5) or lacking mental capacity to provide informed consent. | N: 83 Gender: M/F: 50/33 Age: 78.00 ± 7.96 |
| Schwenk et al., 2014 | Germany | To explore the validity of sensor derived physical activity (PA) parameters for predicting future falls in people with dementia (24 h). To compare sensor-based fall risk assessment with conventional fall risk measures. | adults with dementia (fallers and non-fallers) | Inclusion: (1) over 65 years old, (2) cognitive impairment (Mini-Mental State Examination), a dementia diagnosis was confirmed according to international standards, 3) informed consent, approval by the legal guardian (if appointed), and (4) no uncontrolled or terminal neurological, cardiovascular, metabolic, or psychiatric disorder. Exclusion: n/a | N: 28 (fallers); Gender: M/F: 6/22; Age: 82.0 ± 7.1; N:49 (non-fallers); Gender: M/F: 17/32; Age: 81.8 ± 6.3 |
| Ijmker et al., 2012 | Netherlands | To investigate differences in the relationship between executive function and gait variability and stability during single-task and dual-task walking in persons with and without dementia. | (1) dementia group (2) cognitively intact elderly group (3) cognitively intact younger elderly group | Inclusion: (1) diagnosis of (pre)senile dementia (Alzheimer’s disease or FrontoTemporal dementia), (2) an MMSE-score 16. Exclusion: (1) unable to walk indoors without assistance for at least three minutes, (2) had neurological disorders, (3) orthopaedic surgery within the last two years, (4) history of stroke, (5) psychiatric disorders, and h) were unable to understand the instructions. | N: 15 (dementia); Gender: M/F: 13/2; Age: 81.7 ± 6.3 N:14 (healthy elderly); Gender: M/F: 12/2; Age: 76.9 ± 4.1 N:12 (younger elderly); Age: 64.3 ± 2.8; Gender: M/F: 9/3 |
| Ardle et al., 2021 | UK | To investigate how different environments (lab, real world) impact gait. | (1) dementia Lewy bodies, (2) CI Alzheimer’s disease dementia, (3) control group | Inclusion: (1) aged over 60 years, (2) able to walk for two minutes, as ascertained by self-report. Exclusion: (1) drug-induced or vascular parkinsonism, (2) any coexisting neurological conditions or movement disorders, (3) severe mental illness, (4) evidence of stroke affecting motor function, or g) poor command of the English language | N: 28 (DLB); Gender: M/F: 22/6; Age: 76 ± 6 N: 32 (ADD): Gender: M/F: 15/17; Age: 77 ± 6; N:25 (control); Gender: M/F: 11/14; Age: 74 ± 9 |
| Author [Ref’] | Sensor Type | Location on the Body | Calculated Gait Parameter | Gait Assessment Protocol | Environment | Main Findings |
|---|---|---|---|---|---|---|
| Ardle et al., 2020 | IMU: AX3, Axivity; sampling at 100 Hz | above the fifth lumbar vertebra (L5) | (1) pace, (2) variability, (3) rhythm, (4) asymmetry, (5) postural control | 6 × 10 m; comfortable paste | controlled environment | - the wearable device differentiated dementia disease subtypes (p ≤ 0.05). |
| Gietzelt et al., 2014 | IMUs: SHIMMER; and MMA7260QT; sampling rate was not reported | trunk | (1) anterior-posterior acceleration, (2) average kinetic energy, (3) compensation movements, (4) step frequency, (5) number of dominant peaks | (1) TUG, (2) 4 × one-week sensor-based measurement (every 2 months) | everyday life (nursing home) | - evaluation of the models showed a rate of correctly classified gait episodes of 88.4% (short-term), 74.8% (midterm), and 88.5% (long-term) monitoring. - geriatric assessment tests were unable to distinguish between the groups (AUC < 0.6). |
| Williams et al., 2018 | IMU: THETAmetrix; sampling at 30 Hz | middle of the lower back | linear accelerations and rotational velocities | instrumented Timed Up and Go Test (iTUG) | controlled environment | - cognition was related to duration of walking sub-phases and total time to complete iTUG (r = 0.25–0.28) suggesting that gait speed was related to cognition. - FoF was most strongly related to turning velocity (r = 0.39–0.44), but also to sit-to-stand, gait sub-phases and total time to complete iTUG. - Sub-phases explained 27% of the variance in FoF and there were no correlations between iTUG and QoL. |
| Schwenk et al., 2014 | IMU: Physilog, BioAGM; sampling at 40 Hz | chest | (1) walking during 24 h, (2) walking bout average duration, (3) longest walking bout duration, (4) walking bout duration variability, (5) standing during 24 h, (6) standing bout average duration, (7) sitting during 24 h, (8) sitting bout average duration, and (9) lying during 24 h | (1) Timed Up and Go Test, (2) 5-Chair Stand, (3) 24-h period, (4) follow up after 3 months (no sensor) | real world (everyday life) | - fallers and non-fallers did not differ on any conventional assessment (p = 0.069–0.991), except for ‘previous faller’ (p = 0.006). - several PA parameters discriminated between the groups. |
| Ijmker et al., 2012 | IMU: DynaPort1 MiniMod, McRoberts BV; sampling at 100 Hz | trunk | anterior-posterior and medio-lateral accelerations time-series | 3 min at comfortable pace (10 m long course); (1) once under single and (2) once under dual task condition | controlled environment | - patients with dementia exhibited a significantly (p < 0.05) less variable but more irregular trunk acceleration pattern than cognitively intact elderly on single and dual-task walking. - the walking pattern during dual tasking for the whole group became increasingly unstable. - moderate to high correlations (r > 0.51) were found between executive tasks and gait parameters. |
| Ardle et al., 2021 | IMU: AX3, Axivity; sampling at 20 Hz | (1) above the fifth lumbar vertebra (L5); (2) 7 days—lower backs | (1) pace, (2) variability, (3) rhythm, (4) asymmetry, (5) postural control | (1) controlled environment (lab): 6 × 10 m at comfortable pace; (2) 7 days—real world (everyday life) | (1) controlled environment; (2) real world (everyday life) | - in the lab, DLB group showed greater step length variability (p = 0.008) compared to AD. Both subtypes demonstrated significant gait impairments (p < 0.01) compared to controls. - in the real world, only very short walking bouts (<10 s) demonstrated different gait impairments between subtypes. The context where walking occurs impacts signatures of gait impairment in dementia subtypes. |
| Question | Ardle et al., 2020 | Gietzelt et al., 2014 | Williams et al., 2018 | Schwenk et al., 2014 | Ijmker et al., 2012 | Ardle et al., 2021 |
|---|---|---|---|---|---|---|
| Q1. Is the hypothesis/aim/objective of the study clearly described? | Y | Y | Y | Y | Y | Y |
| Q2. Are the main outcomes clearly described in the Introduction or Methods? | Y | Y | Y | Y | Y | Y |
| Q3. Are the characteristics of the participants clearly described (including age, sex, and status as healthy/injured/pathological)? | Y | Y | Y | N | Y | Y |
| Q4. Are the inclusion/exclusion criteria described and appropriate? | Y | Y | Y | N | Y | Y |
| Q5. Are the main findings of the study clearly described? | Y | Y | Y | Y | Y | Y |
| Q6. Are estimates of the random variability in the data for the main outcomes provided? | Y | N | Y | Y | Y | Y |
| Q7. Have actual probability values been reported for the main outcomes? | Y | N | Y | Y | Y | Y |
| Q8. Are the participants representative of the entire population from which they were recruited? | Y | Y | Y | Y | Y | Y |
| Q9. Are the setting and conditions typical for the population represented by the participants? | Y | Y | Y | Y | Y | Y |
| Q10. Are the statistical tests used to assess the main outcomes appropriate? | Y | Y | Y | Y | Y | Y |
| Q11. Are the main outcome measures used accurate (valid and reliable)? | Y | Y | Y | Y | Y | Y |
| Q12. Is a sample size justification, power description, or variance and effect estimates provided? | N | N | N | N | N | N |
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Alexander, N.B. Gait disorders in older adults. J. Am. Geriatr. Soc. 1996, 44, 434–451. [Google Scholar] [CrossRef] [Green Version]
- Nutt, J.G.; Marsden, C.D.; Thompson, P.D. Human walking and higher-level gait disorders, particularly in the elderly. Neurology 1993, 43, 268. [Google Scholar] [CrossRef]
- Wilson, R.S.; Schneider, J.A.; Beckett, L.A.; Evans, D.A.; Bennett, D.A. Progression of gait disorder and rigidity and risk of death in older persons. Neurology 2002, 58, 1815–1819. [Google Scholar] [CrossRef]
- Jørstad, E.C.; Hauer, K.; Becker, C.; Lamb, S.E.; ProFaNE Group. Measuring the psychological outcomes of falling: A systematic review. J. Am. Geriatr. Soc. 2005, 53, 501–510. [Google Scholar] [CrossRef] [PubMed]
- Snijders, A.H.; van de Warrenburg, B.P.; Giladi, N.; Bloem, B.R. Neurological gait disorders in elderly people: Clinical approach and classification. Lancet Neurol. 2007, 6, 63–74. [Google Scholar] [CrossRef]
- Podsiadlo, D.; Richardson, S. The timed “Up & Go”: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar]
- Guralnik, J.M.; Simonsick, E.M.; Ferrucci, L.; Glynn, R.J.; Berkman, L.F.; Blazer, D.G.; Scherr, P.A.; Wallace, R.B. A short physical performance battery assessing lower extremity function: Association with self-reported disability and prediction of mortality and nursing home admission. J. Gerontol. 1994, 49, M85–M94. [Google Scholar] [CrossRef] [PubMed]
- Muro-De-La-Herran, A.; Garcia-Zapirain, B.; Mendez-Zorrilla, A. Gait analysis methods: An overview of wearable and non-wearable systems, highlighting clinical applications. Sensors 2014, 14, 3362–3394. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aminian, K.; Najafi, B. Capturing human motion using body-fixed sensors: Outdoor measurement and clinical applications. Comput. Animat. Virtual Worlds 2004, 15, 79–94. [Google Scholar] [CrossRef]
- Weizman, Y.; Tan, A.M.; Fuss, F.K. Use of wearable technology to enhance response to the Coronavirus (COVID-19) pandemic. Public Health 2020, 185, 221. [Google Scholar] [CrossRef]
- González, R.C.; López, A.M.; Rodriguez-Uría, J.; Álvarez, D.; Alvarez, J.C.A. Real-time gait event detection for normal subjects from lower trunk accelerations. Gait Posture 2010, 31, 322–325. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.C.; Kim, J.Y.; Lee, H.N.; Lee, H.H.; Kwon, J.H.; Kim, N.B.; Kim, M.J.; Hwang, J.H.; Han, G.C. A quantitative analysis of gait patterns in vestibular neuritis patients using gyroscope sensor and a continuous walking protocol. J. Neuroeng. Rehabil. 2014, 11, 58. [Google Scholar] [CrossRef] [Green Version]
- Mobbs, R.J.; Phan, K.; Maharaj, M.; Rao, P.J. Physical activity measured with accelerometer and self-rated disability in lumbar spine surgery: A prospective study. Glob. Spine J. 2016, 6, 459–464. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mueller, M.J.; Strube, M.J. Generalizability of in-shoe peak pressure measures using the F-scan system. Clin. Biomech. 1996, 11, 159–164. [Google Scholar] [CrossRef]
- Lane, T.J.; Landorf, K.B.; Bonanno, D.R.; Raspovic, A.; Menz, H.B. Effects of shoe sole hardness on plantar pressure and comfort in older people with forefoot pain. Gait Posture 2014, 39, 247–251. [Google Scholar] [CrossRef]
- Godi, M.; Turcato, A.M.; Schieppati, M.; Nardone, A. Test-retest reliability of an insole plantar pressure system to assess gait along linear and curved trajectories. J. Neuroeng. Rehabil. 2014, 11, 95. [Google Scholar] [CrossRef] [Green Version]
- Tan, A.M.; Fuss, F.K.; Weizman, Y.; Woudstra, Y.; Troynikov, O. Design of low cost smart insole for real time measurement of plantar pressure. Procedia Technol. 2015, 20, 117–122. [Google Scholar] [CrossRef] [Green Version]
- Weizman, Y.; Tan, A.M.; Fuss, F.K. Benchmarking study of the forces and centre of pressure derived from a novel smart-insole against an existing pressure measuring insole and force plate. Measurement 2019, 142, 48–59. [Google Scholar] [CrossRef]
- Brognara, L.; Palumbo, P.; Grimm, B.; Palmerini, L. Assessing gait in Parkinson’s disease using wearable motion sensors: A systematic review. Diseases 2019, 7, 18. [Google Scholar] [CrossRef] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The Prisma statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, N.; Phillips, M. Rayyan for systematic reviews. J. Electron. Resour. Libr. 2018, 30, 46–48. [Google Scholar] [CrossRef] [Green Version]
- Benson, L.C.; Clermont, C.A.; Bošnjak, E.; Ferber, R. The use of wearable devices for walking and running gait analysis outside of the lab: A systematic review. Gait Posture 2018, 63, 124–138. [Google Scholar] [CrossRef]
- Campos, S.; Doxey, J.; Hammond, D. Nutrition labels on pre-packaged foods: A systematic review. Public Health Nutr. 2011, 14, 1496–1506. [Google Scholar] [CrossRef] [Green Version]
- Downs, S.H.; Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J. Epidemiol. Community Health 1998, 52, 377–384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mc Ardle, R.; Del Din, S.; Galna, B.; Thomas, A.; Rochester, L. Differentiating dementia disease subtypes with gait analysis: Feasibility of wearable sensors? Gait Posture 2020, 76, 372–376. [Google Scholar] [CrossRef]
- Gietzelt, M.; Feldwieser, F.; Govercin, M.; Steinhagen-Thiessen, E.; Marschollek, M. A prospective field study for sensor-based identification of fall risk in older people with dementia. Inform. Health Soc. Care 2014, 39, 249–261. [Google Scholar] [CrossRef] [PubMed]
- Williams, J.M.; Nyman, S.R. Association between the instrumented timed up and go test and cognitive function, fear of falling and quality of life in community dwelling people with dementia. J. Frailty Sarcopenia Falls 2018, 3, 185–193. [Google Scholar] [CrossRef] [Green Version]
- Schwenk, M.; Hauer, K.; Zieschang, T.; Englert, S.; Mohler, J.; Najafi, B. Sensor-derived physical activity parameters can predict future falls in people with dementia. Gerontology 2014, 60, 483–492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ijmker, T.; Lamoth, C.J.C. Gait and cognition: The relationship between gait stability and variability with executive function in persons with and without dementia. Gait Posture 2012, 35, 126–130. [Google Scholar] [CrossRef]
- Mc Ardle, R.; Del Din, S.; Donaghy, P.; Galna, B.; Thomas, A.J.; Rochester, L. The impact of environment on gait assessment: Considerations from real-world gait analysis in dementia subtypes. Sensors 2021, 21, 813. [Google Scholar] [CrossRef] [PubMed]
- Dolatabadi, E.; van Ooteghem, K.; Taati, B.; Iaboni, A. Quantitative mobility assessment for fall risk prediction in dementia: A systematic review. Dement. Geriatr. Cogn. Disord. 2018, 45, 353–367. [Google Scholar] [CrossRef] [PubMed]
- Beauchet, O.; Annweiler, C.; Lecordroch, Y.; Allali, G.; Dubost, V.; Herrmann, F.R.; Kressig, R.W. Walking speed-related changes in stride time variability: Effects of decreased speed. J. Neuroeng. Rehabil. 2009, 6, 32. [Google Scholar] [CrossRef] [PubMed]
- Waldemar, G.; Phung, K.T.T.; Burns, A.; Georges, J.; Hansen, F.R.; Iliffe, S.; Marking, C.; Rikkert, M.O.; Selmes, J.; Stoppe, G. Access to diagnostic evaluation and treatment for dementia in Europe. Int. J. Geriatr. Psychiatry 2007, 22, 47–54. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Weizman, Y.; Tirosh, O.; Beh, J.; Fuss, F.K.; Pedell, S. Gait Assessment Using Wearable Sensor-Based Devices in People Living with Dementia: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 12735. https://doi.org/10.3390/ijerph182312735
Weizman Y, Tirosh O, Beh J, Fuss FK, Pedell S. Gait Assessment Using Wearable Sensor-Based Devices in People Living with Dementia: A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(23):12735. https://doi.org/10.3390/ijerph182312735
Chicago/Turabian StyleWeizman, Yehuda, Oren Tirosh, Jeanie Beh, Franz Konstantin Fuss, and Sonja Pedell. 2021. "Gait Assessment Using Wearable Sensor-Based Devices in People Living with Dementia: A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 23: 12735. https://doi.org/10.3390/ijerph182312735
APA StyleWeizman, Y., Tirosh, O., Beh, J., Fuss, F. K., & Pedell, S. (2021). Gait Assessment Using Wearable Sensor-Based Devices in People Living with Dementia: A Systematic Review. International Journal of Environmental Research and Public Health, 18(23), 12735. https://doi.org/10.3390/ijerph182312735