
Coping Strategies as a Mental Health Protection Factor of Spanish Nurses during COVID-19

 ,
,  ,
, 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Instruments
2.3. Procedure
2.4. Data Analysis
3. Results
3.1. Descriptive Analysis of Sociodemographic Variables and Use of Coping Strategies
3.2. Use of Coping Strategies by Nurses in the Context of COVID-19
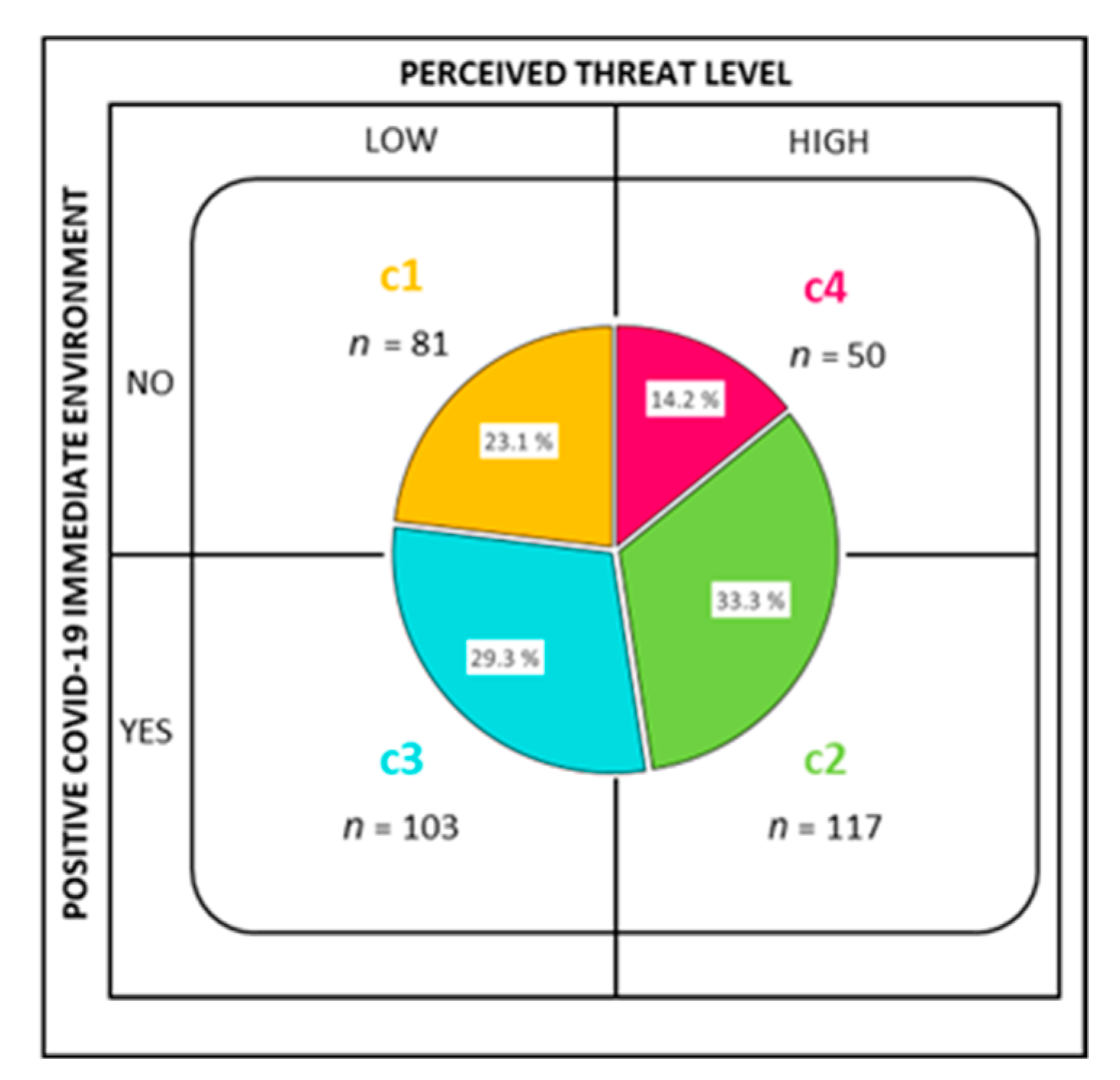
3.3. Profiles by Someone Close COVID-19 Positive and Perceived Threat
3.4. Coping Strategies and Health: Correlations and Cluster Comparison
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Stawicko, S.P.; Jeanmonod, R.; Miller, A.C.; Paladino, L.; Gaieski, D.F.; Yaffee, A.Q.; De Wulf, A.; Grover, J.; Papadimos, T.J.; Bloem, C.; et al. The 2019–2020 Novel Coronavirus (Severe Acute Respiratory Syndrome Coronavirus 2) Pandemic: A Joint American College of Academic International Medicine-World Academic Council of Emergency Medicine Multidisciplinary COVID-19 Working Group Consensus Paper. J. Glob. Infect. Dis. 2020, 12, 47–93. [Google Scholar] [CrossRef]
- Heymann, D.L.; Shindo, N. WHO Scientific and Technical Advisory Group for Infectious Hazards. COVID-19: What is next for public health? Lancet 2020, 395, 542–545. [Google Scholar] [CrossRef] [Green Version]
- Lee, M.C.C.; Thampi, S.; Chan, H.P.; Khoo, D.; Chin, B.; Foo, D.; Lua, C.B.; Lewin, B.; Jacob, R. Psychological distress during the COVID-19 pandemic amongst anaesthesiologists and nurses. Br. J. Anaesth. 2020, 125, 384–386. [Google Scholar] [CrossRef]
- Moreno-Cabas, M.T. Factors related to SARS-CoV-2 infection in healthcare professionals in Spain. The SANICOVI project. Enferm. Clin. 2020, 30, 360–370. [Google Scholar] [CrossRef]
- Blake, H.; Bermingham, F.; Johnson, G.; Tabner, A. Mitigating the Psychological Impact of COVID-19 on Healthcare Workers: A Digital Learning Package. Int. J. Environ. Res. Public Health 2020, 17, 2997. [Google Scholar] [CrossRef]
- Hong, S.; Ai, M.; Xu, X.; Wang, W.; Chen, J.; Zhang, Q.; Wang, L.; Kuang, L. Immediate Psychological Impact on Nurses working at 42 Government-Designated Hospital During COVID-19 Outbreak in China: A cross-sectional study. Nurs. Outlook 2020, 69, 6–12. [Google Scholar] [CrossRef]
- Pérez-Fuentes, M.C.; Molero, M.M.; Gázquez, J.J.; Simón, M.M. Analysis of Burnout Predictors in Nursing: Risk and Protective Psychological Factors. Eur. J. Psychol. Appl. Leg. Context 2019, 11, 33–40. [Google Scholar] [CrossRef] [Green Version]
- Wersabe, H.; Lieb, R.; Meyer, A.H.; Hofer, P.; Gloster, A.T. The link between stress, well-being, and psychological flexibility during an Acceptance and Commitment Therapy self-help intervention. Int. J. Clin. Health Psychol. 2018, 18, 60–68. [Google Scholar] [CrossRef]
- Khubchandani, J.; Kandiah, J.; Saiki, D. The COVID-19 Pandemic, Stress, and Eating Practices in the United States. Eur. J. Investig. Health Psychol. Educ. 2020, 10, 950–956. [Google Scholar] [CrossRef] [PubMed]
- Justo-Alonso, A.; García-Dantas, A.; González-Vázquez, A.I.; Sánchez-Martín, M.; del Río-Casanova, L. How did Different Generations Cope with the COVID-19 Pandemic? Early Stages of the Pandemic in Spain. Psicothema 2020, 32, 490–500. [Google Scholar] [CrossRef]
- Soriano, J.G.; Pérez-Fuentes, M.C.; Molero, M.M.; Tortosa, B.M.; González, A. Benefits of psychological intervention related to stress and anxiety: Systematic review and meta-analysis. Eur. J. Educ. Psychol. 2019, 12, 191–206. [Google Scholar] [CrossRef]
- Tirado, G.; Llorente-Alonso, M.; Topa, G. Desequilibrio esfuerzo-recompensa y quejas subjetivas de salud: Estudio exploratorio entre médicos en España [Effort-reward imbalance and subjective health complaints: An exploratory study among doctors in Spain]. Eur. J. Investig. Health Psychol. Educ. 2019, 9, 59–70. [Google Scholar] [CrossRef] [Green Version]
- Kan, T.; Zhang, J. Factors influencing seasonal influenza vaccination behaviour among elderly people: A systematic review. Public Health 2018, 156, 67–78. [Google Scholar] [CrossRef] [PubMed]
- Chang, B.P. Can hospitalization be hazardous to your health? A nosocomial based stress model for hospitalization. Gen. Hosp. Psychiatry 2019, 60, 83–89. [Google Scholar] [CrossRef]
- Nasaescu, E.; Zych, I.; Ortega-Ruiz, R.; Farrington, D.P.; Llorent, V.J. Longitudinal Patterns of Antisocial Behaviors in Early Adolescence: A Latent Class and Latent Transition Analysis. Eur. J. Psychol. Appl. Leg. Context 2020, 12, 85–92. [Google Scholar] [CrossRef]
- Pérez-Fuentes, M.C.; Molero, M.M.; Martos, Á.; Gázquez, J.J. Threat of COVID-19 and emotional state during quarantine: Positive and negative affect as mediators in a cross-sectional study of the Spanish population. PLoS ONE 2020, 15, e0235305. [Google Scholar] [CrossRef]
- Yang, B.; Wang, Y.; Cui, F.; Huang, T.; Sheng, P.; Shi, T.; Huang, C.; Lan, Y.; Huang, Y.N. Association between insomnia and job stress: A meta-analysis. Sleep Breath. 2018, 22, 1221–1231. [Google Scholar] [CrossRef]
- Molero, M.M.; Herrera-Peco, I.; Pérez-Fuentes, M.C.; Gázquez, J.J. Análisis de la amenaza percibida por la COVID-19 en población española [Analysis of the threat perceived by the COVID-19 in the Spanish population]. Aten. Prim. 2020, 52, 515–516. [Google Scholar] [CrossRef]
- Mazza, C.; Ricci, E.; Biondi, S.; Colasanti, M.; Ferracuti, S.; Napoli, C.; Roma, P. A Nationwide Survey of Psychological Distress among Italian People during the COVID-19 Pandemic: Immediate Psychological Responses and Associated Factors. Int. J. Env. Res. Public Health 2020, 17, 3165. [Google Scholar] [CrossRef] [PubMed]
- Carreno, D.F.; Eisenbeck, N.; Cangas, A.J.; García-Montes, J.M.; Del Vas, L.G.; María, A. Spanish adaptation of the Personal Meaning Profile-Brief: Meaning in life, psychological well-being, and distress. Int. J. Clin. Health Psychol. 2020, 20, 151–162. [Google Scholar] [CrossRef] [PubMed]
- Holgado-Tello, F.P.; Amor, P.J.; Lasa-Aristu, A.; Domínguez-Sánchez, F.J.; Delgado, B. Two new brief versions of the Cognitive Emotion Regulation Questionnaire and its relationships with depression and anxiety. An. Psicol. Spain 2018, 34, 458–464. [Google Scholar] [CrossRef]
- Nie, A.; Su, X.; Zhang, S.; Guan, W.; Li, J. Psychological impact of COVID-19 outbreak on frontline nurses: A cross-sectional survey study. J. Clin. Nurs. 2020, 29, 4217–4226. [Google Scholar] [CrossRef]
- Díaz-Ramiro, E.M.; Rubio-Valdehita, S.; López-Núñez, M.I.; Aparicio-García, M.E. Los hábitos de sueño como predictores de la salud psicológica en profesionales sanitarios. An. Psicol. 2020, 36, 242–246. [Google Scholar] [CrossRef]
- Lazarus, R.S.; Folkman, S. Stress, Appraisal, and Coping; Springer: New York, NY, USA, 1984. [Google Scholar]
- Morales, F. Estrategias de afrontamiento, empatía y tendencia prosocial en universitarios. Eur. J. Educ. Psycho. 2020, 13, 187–200. [Google Scholar] [CrossRef]
- De la Barrera, U.; Villanueva, L.; Prado-Garcó, V. Emotional and personality predictor that influence the appearance of somatic complaints in children and adults. Psicothema 2019, 31, 407–413. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Wang, P. Perceived stress and psychological distress among chinese physicians. Medicine 2019, 98, e15950. [Google Scholar] [CrossRef] [PubMed]
- Araujo, C.; da Silva, E.C.; de Souza, S.; Cardoso, L.; Reisdorfer, E. Estrés laboral y estrategias de afrontamiento entre los profesionales de enfermería hospitalaria [Work stress and coping strategies among hospital nursing professionals]. Enferm. Glob. 2016, 15, 288–320. [Google Scholar] [CrossRef] [Green Version]
- Eslami, R.; Elahi, N.; Mohammadi, E.; Fallahi, M. How Do the Nurses Cope with Job Stress? A Study with Grounded Theory Approach. J. Caring. Sci. 2017, 6, 199–211. [Google Scholar] [CrossRef] [Green Version]
- Jiménez, M.N.; Axpe, I.; Esnaola, I. El rol del apoyo social percibido en la predicción de la inteligencia emocional entre adolescentes de la República Dominicana. Eur. J. Educ. Psycho. 2020, 13, 97–110. [Google Scholar] [CrossRef]
- Melendez, J.C.; Satorres, E.; Delhom, I. Personalidad y afrontamiento. ¿Qué rasgos predicen las estrategias adaptativas? An. Psicol. Spain 2020, 36, 39–45. [Google Scholar] [CrossRef] [Green Version]
- Hernández-Mendoza, E.; Cerezo-Reséndiz, S.; López-Sandoval, M.G. Estrategias de afrontamiento ante el estrés laboral en enfermeras [Coping strategies for work stress in nurses]. Rev. Enferm. IMSS Méx. 2007, 15, 161–166. [Google Scholar]
- Brailovskaia, J.; Margraf, J. Predicting adaptive and maladaptive responses to the Coronavirus (COVID-19) outbreak: A prospective longitudinal study. Int. J. Clin. Health Psychol. 2020, 20, 183–191. [Google Scholar] [CrossRef] [PubMed]
- Carver, C.S.; Scheier, M.F.; Weintraub, J.K. Assessing coping strategies: A theoretically based approach. J. Pers. Soc. Psychol. 1989, 56, 267–283. [Google Scholar] [CrossRef]
- Al Barmawi, M.A.; Subih, M.; Salameh, O.; Sayyah, N.; Shoqirat, N.; Abdel-Azeez, R. Coping strategies as moderating factors to compassion fatigue among critical care nurses. Brain Behav. 2019, 9, e01264. [Google Scholar] [CrossRef] [Green Version]
- Kivimäki, M.; Steptoe, A. Effects of stress on the development and progression of cardiovascular disease. Nat. Rev. Cardiol. 2018, 15, 215–229. [Google Scholar] [CrossRef] [PubMed]
- Dauriz, M.; Mantovani, A.; Bonapace, S.; Verlato, G.; Zoppini, G.; Bonora, E.; Targher, G. Prognostic Impact of Diabetes on Long-term Survival Outcomes in Patients with Heart Failure: A Meta-analysis. Diabetes Care 2017, 40, 1597–1605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dawe, K.; Montgomery, A.; McGee, H.; Panagopoulou, E.; Morgan, K.; Hackshaw, L.; Vedhara, K. The effects of perceived stress on biological parameters in healthcare professionals: A systematic review. J. Health Psychol. 2016, 21, 607–618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zerbini, G.; Ebigbo, A.; Reicherts, P.; Kunz, M.; Messman, H. Psychosocial burden of healthcare professionals in times of COVID-19–A survey conducted at the University Hospital Augsburg. Ger. Med. Sci. 2020, 18, 1–9. [Google Scholar] [CrossRef]
- González-Rivera, J.A.; Pagán-Torres, O.M.; Pérez-Torres, E.M. Depression, Anxiety and Stress Scales (DASS-21): Construct Validity Problem in Hispanics. Eur. J. Investig. Health Psychol. Educ. 2020, 10, 375–389. [Google Scholar] [CrossRef] [Green Version]
- Pérez-Fuentes, M.C.; Gázquez, J.J.; Molero, M.M.; Oropesa, N.F.; Martos, Á. Violence and Job Satisfaction of Nurses: Importance of a Support Network in Healthcare. Eur. J. Psychol. Appl. Leg. Context 2020, 13, 21–28. [Google Scholar] [CrossRef]
- Pérez-Fuentes, M.C.; Molero, M.M.; Oropesa, N.F.; Martos, Á.; Simón, M.; Herrera-Peco, I.; Gázquez, J.J. Questionnaire on Perception of Threat from COVID-19. J. Clin. Med. 2020, 9, 1196. [Google Scholar] [CrossRef]
- Garnefski, N.; Van den Kommer, T.; Kraaij, V.; Teerds, J.; Legerstee, J.; Onstein, E. The relationship between cognitive emotion regulation strategies and emotional problems: Comparison between a clinical and a non-clinical sample. Eur. J. Pers. 2002, 16, 403–420. [Google Scholar] [CrossRef]
- Domínguez-Sánchez, F.J.; Lasa-Aristu, A.; Amor, P.J.; Holgado-Tello, F.P. Psychometric properties of the spanish version of the Cognitive Emotion Regulation Questionnaire. Assessment 2011, 20, 253–261. [Google Scholar] [CrossRef]
- Goldberg, D.; Hillier, V. A scaled version of the General Health Questionnaire. Psychol. Med. 1979, 9, 139–145. [Google Scholar] [CrossRef]
- Lobo, A.; Pérez-Echeverría, M.J.; Artal, J. Validity of the scaled version of the General Health Questionnaire (GHQ-28) in a Spanish population. Psychol. Med. 1986, 16, 135–140. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge: New York, NY, USA, 1988. [Google Scholar] [CrossRef]
- IBM Corp. IBM SPSS Statistics for Windows, Version 24.0; Released; IBM Corp.: Armonk, NY, USA, 2016. [Google Scholar]
- Ventura-León, J.L.; Caycho, T. El coeficiente Omega: Un método alternativo para la estimación de la confiabilidad [The Omega coefficient: An alternative method for estimating reliability]. Rev. Lat. Cienc. Soc. Niñez Juv. 2017, 15, 625–627. [Google Scholar]
- Thanoi, W.; Klainin-Yobas, P. Assessing rumination response style among undergraduate nursing students: A construct validation study. Nurse Educ. Today 2015, 35, 641–646. [Google Scholar] [CrossRef]
- Ruta, F.; Mas, F.D.; Biancuzzi, H.; Ferrara, P.; Monica, A.D. Covid-19 and front-line nurses’ mental health: A literature review. Prof. Inferm. 2021, 74, 41–47. [Google Scholar] [CrossRef]
- Stelnicki, A.M.; Carleton, R.N.; Reichert, C. Nurses’ Mental Health and Well-Being: COVID-19 Impacts. Can. J. Nurs. Res. 2020, 52, 237–239. [Google Scholar] [CrossRef]


{kind=link}
| CERQ | Male | Female | t | p | Mean Dif. | SE Dif. | 95% CI Mean Dif. | Cohen’s d | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | M | SD | N | M | SD | Lower | Upper | ||||||
| SB | 49 | 7.73 | 2.46 | 302 | 7.41 | 2.25 | 0.91 | 0.363 | 0.32 | 0.35 | −0.37 | 1.01 | 0.14 |
| AC | 49 | 14.38 | 3.02 | 302 | 14.09 | 2.58 | 0.72 | 0.471 | 0.29 | 0.40 | −0.50 | 1.09 | 0.11 |
| RU | 49 | 11.83 | 2.89 | 302 | 12.41 | 3.50 | −1.09 | 0.275 | −0.57 | 0.52 | −1.61 | 0.46 | −0.16 |
| PF | 49 | 12.46 | 3.50 | 302 | 13.49 | 3.33 | −1.97 | 0.049 | −1.02 | 0.51 | −2.03 | −0.00 | −0.30 |
| RP | 49 | 14.57 | 2.83 | 302 | 14.75 | 2.88 | −0.40 | 0.684 | −0.18 | 0.44 | −1.05 | 0.69 | −0.06 |
| PR | 49 | 15.14 | 3.17 | 302 | 15.24 | 3.09 | −0.21 | 0.831 | −0.10 | 0.47 | −1.04 | 0.83 | −0.03 |
| PP | 49 | 13.93 | 3.49 | 302 | 14.51 | 2.79 | −1.28 | 0.201 | −0.57 | 0.44 | −1.44 | 0.30 | −0.19 |
| CA | 49 | 7.85 | 2.60 | 302 | 8.22 | 3.00 | −0.81 | 0.418 | −0.36 | 0.45 | −1.26 | 0.52 | −0.12 |
| OB | 49 | 9.83 | 4.08 | 302 | 9.68 | 4.35 | 0.23 | 0.816 | 0.15 | 0.66 | −1.15 | 1.46 | 0.03 |
| CERQ Subscales | SB | AC | RU | PF | RP | PR | PP | CA | OB | |
|---|---|---|---|---|---|---|---|---|---|---|
| Perceived Threat | Pearson’s r | 0.190 | 0.087 | 0.338 | −0.016 | 0.061 | −0.138 | −0.069 | 0.397 | 0.149 |
| p-value | <0.001 | 0.105 | <0.001 | 0.760 | 0.256 | 0.010 | 0.200 | <0.001 | 0.005 | |
| Upper 95% CI | 0.289 | 0.190 | 0.427 | 0.088 | 0.164 | −0.034 | 0.036 | 0.481 | 0.250 | |
| Lower 95% CI | 0.087 | −0.018 | 0.241 | −0.121 | −0.044 | −0.239 | −0.172 | 0.305 | 0.045 | |
| 32.95 (6.27) | M (SD) | 7.45 (2.28) | 14.13 (2.65) | 12.33 (3.42) | 13.34 (3.37) | 14.72 (2.87) | 15.23 (3.10) | 14.43 (2.89) | 8.17 (2.94) | 9.70 (4.31) |
| CERQ Subscales | GHQ-28 | Somatic Symptoms | Anxiety/Insomnia | Social Dysfunction | Depression |
|---|---|---|---|---|---|
| Self-blame | Pearson’s r | 0.183 | 0.226 | 0.084 | 0.207 |
| p-value | <0.001 | <0.001 | 0.116 | <0.001 | |
| Upper 95% CI | 0.282 | 0.323 | 0.187 | 0.305 | |
| Lower 95% CI | 0.080 | 0.124 | −0.021 | 0.105 | |
| Acceptance | Pearson’s r | −0.065 | 0.034 | −0.169 | −0.078 |
| p-value | 0.223 | 0.527 | 0.001 | 0.146 | |
| Upper 95% CI | 0.040 | 0.138 | −0.065 | 0.027 | |
| Lower 95% CI | −0.169 | −0.071 | −0.269 | −0.181 | |
| Rumination | Pearson’s r | 0.333 | 0.406 | 0.090 | 0.190 |
| p-value | <0.001 | <0.001 | 0.093 | <0.001 | |
| Upper 95% CI | 0.423 | 0.490 | 0.193 | 0.289 | |
| Lower 95% CI | 0.237 | 0.315 | −0.015 | 0.087 | |
| Positive refocusing | Pearson’s r | −0.119 | −0.133 | −0.227 | −0.300 |
| p-value | 0.026 | 0.013 | <0.001 | <0.001 | |
| Upper 95% CI | −0.015 | −0.028 | −0.125 | −0.202 | |
| Lower 95% CI | −0.221 | −0.234 | −0.324 | −0.392 | |
| Refocus on planning | Pearson’s r | −0.019 | 0.010 | −0.189 | −0.166 |
| p-value | 0.718 | 0.857 | <0.001 | 0.002 | |
| Upper 95% CI | 0.085 | 0.114 | −0.086 | −0.062 | |
| Lower 95% CI | −0.124 | −0.095 | −0.288 | −0.266 | |
| Positive reappraisal | Pearson’s r | −0.191 | −0.180 | −0.319 | −0.373 |
| p-value | <0.001 | <0.001 | <0.001 | <0.001 | |
| Upper 95% CI | −0.088 | −0.077 | −0.221 | −0.280 | |
| Lower 95% CI | −0.290 | −0.279 | −0.410 | −0.460 | |
| Putting into perspective | Pearson’s r | −0.080 | −0.132 | −0.147 | −0.218 |
| p-value | 0.136 | 0.013 | 0.006 | <0.001 | |
| Upper 95% CI | 0.025 | −0.028 | −0.043 | −0.116 | |
| Lower 95% CI | −0.183 | −0.233 | −0.248 | −0.316 | |
| Catastrophizing | Pearson’s r | 0.336 | 0.457 | 0.203 | 0.301 |
| p-value | <0.001 | <0.001 | <0.001 | <0.001 | |
| Upper 95% CI | 0.426 | 0.536 | 0.301 | 0.393 | |
| Lower 95% CI | 0.240 | 0.370 | 0.100 | 0.202 | |
| Other-blame | Pearson’s r | 0.171 | 0.245 | 0.098 | 0.179 |
| p-value | 0.001 | <0.001 | 0.065 | <0.001 | |
| Upper 95% CI | 0.271 | 0.341 | 0.201 | 0.279 | |
| Lower 95% CI | 0.067 | 0.144 | −0.006 | 0.076 | |
| M (SD) | 9.63 (4.82) | 10.61 (5.00) | 8.01 (3.20) | 2.20 (3.42) |
| CERQ | C1 | C2 | C3 | C4 | |
|---|---|---|---|---|---|
| Self-blame | M | 7.27 | 7.81 | 7.14 | 7.60 |
| SD | 2.49 | 2.14 | 2.15 | 2.44 | |
| Acceptance | M | 14.14 | 14.26 | 14.15 | 13.80 |
| SD | 2.64 | 2.39 | 2.78 | 2.99 | |
| Rumination | M | 11.27 | 13.10 | 12.09 | 12.76 |
| SD | 3.72 | 3.04 | 3.67 | 2.78 | |
| Positive refocusing | M | 13.28 | 13.20 | 13.43 | 13.64 |
| SD | 3.72 | 3.25 | 3.21 | 3.42 | |
| Refocus on planning | M | 14.60 | 14.78 | 14.78 | 14.70 |
| SD | 3.19 | 2.62 | 2.98 | 2.71 | |
| Positive reappraisal | M | 15.79 | 14.84 | 15.38 | 14.94 |
| SD | 2.74 | 3.13 | 3.25 | 3.17 | |
| Putting into perspective | M | 15.07 | 14.32 | 14.23 | 14.06 |
| SD | 3.04 | 2.74 | 2.70 | 3.31 | |
| Catastrophizing | M | 6.99 | 9.09 | 7.32 | 9.72 |
| SD | 2.76 | 2.86 | 2.39 | 3.15 | |
| Other-blame | M | 8.74 | 10.06 | 9.06 | 11.76 |
| SD | 4.18 | 4.31 | 3.86 | 4.69 | |
| GHQ-28 | C1 | C2 | C3 | C4 | |
| Somatic symptoms | M | 7.58 | 11.95 | 7.78 | 11.38 |
| SD | 4.32 | 4.42 | 3.85 | 5.33 | |
| Anxiety/insomnia | M | 7.99 | 12.80 | 9.05 | 12.94 |
| SD | 4.63 | 4.52 | 4.18 | 5.05 | |
| Social dysfunction | M | 7.59 | 8.69 | 7.02 | 9.18 |
| SD | 2.48 | 3.59 | 2.79 | 3.37 | |
| Depression | M | 1.57 | 2.79 | 1.39 | 3.54 |
| SD | 2.77 | 3.55 | 2.29 | 5.03 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Molero-Jurado, M.d.M.; Pérez-Fuentes, M.d.C.; Gázquez-Linares, J.J.; Santillán García, A. Coping Strategies as a Mental Health Protection Factor of Spanish Nurses during COVID-19. Int. J. Environ. Res. Public Health 2021, 18, 12748. https://doi.org/10.3390/ijerph182312748
Molero-Jurado MdM, Pérez-Fuentes MdC, Gázquez-Linares JJ, Santillán García A. Coping Strategies as a Mental Health Protection Factor of Spanish Nurses during COVID-19. International Journal of Environmental Research and Public Health. 2021; 18(23):12748. https://doi.org/10.3390/ijerph182312748
Chicago/Turabian StyleMolero-Jurado, María del Mar, María del Carmen Pérez-Fuentes, José Jesús Gázquez-Linares, and Azucena Santillán García. 2021. "Coping Strategies as a Mental Health Protection Factor of Spanish Nurses during COVID-19" International Journal of Environmental Research and Public Health 18, no. 23: 12748. https://doi.org/10.3390/ijerph182312748
APA StyleMolero-Jurado, M. d. M., Pérez-Fuentes, M. d. C., Gázquez-Linares, J. J., & Santillán García, A. (2021). Coping Strategies as a Mental Health Protection Factor of Spanish Nurses during COVID-19. International Journal of Environmental Research and Public Health, 18(23), 12748. https://doi.org/10.3390/ijerph182312748