
Factors Associated with the Patient’s Decision to Avoid Healthcare during the COVID-19 Pandemic

 , , ,
, , , 


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Variables
2.3. Statistical Analysis
3. Results
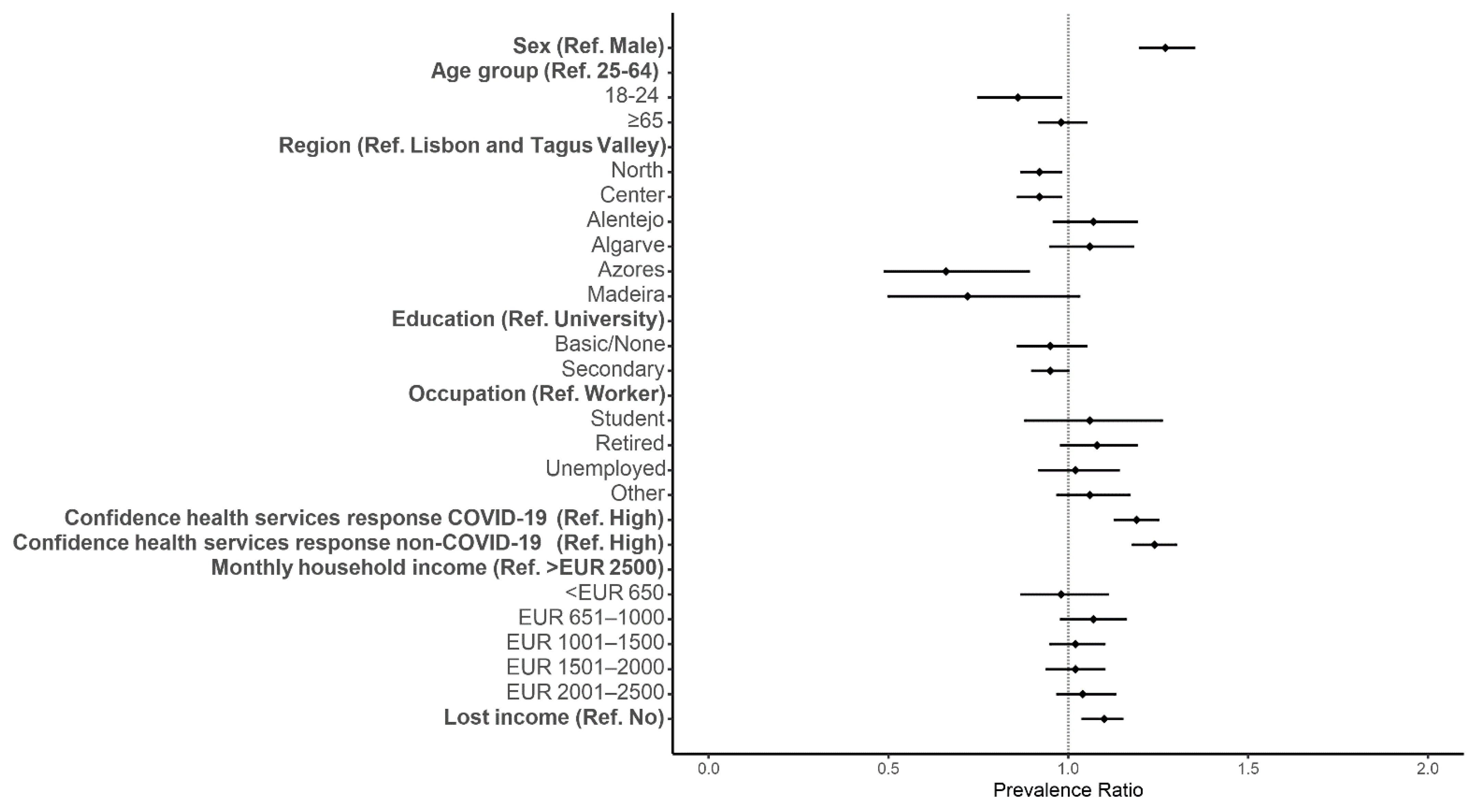
3.1. Predisposing Factors
3.2. Enabling Factors
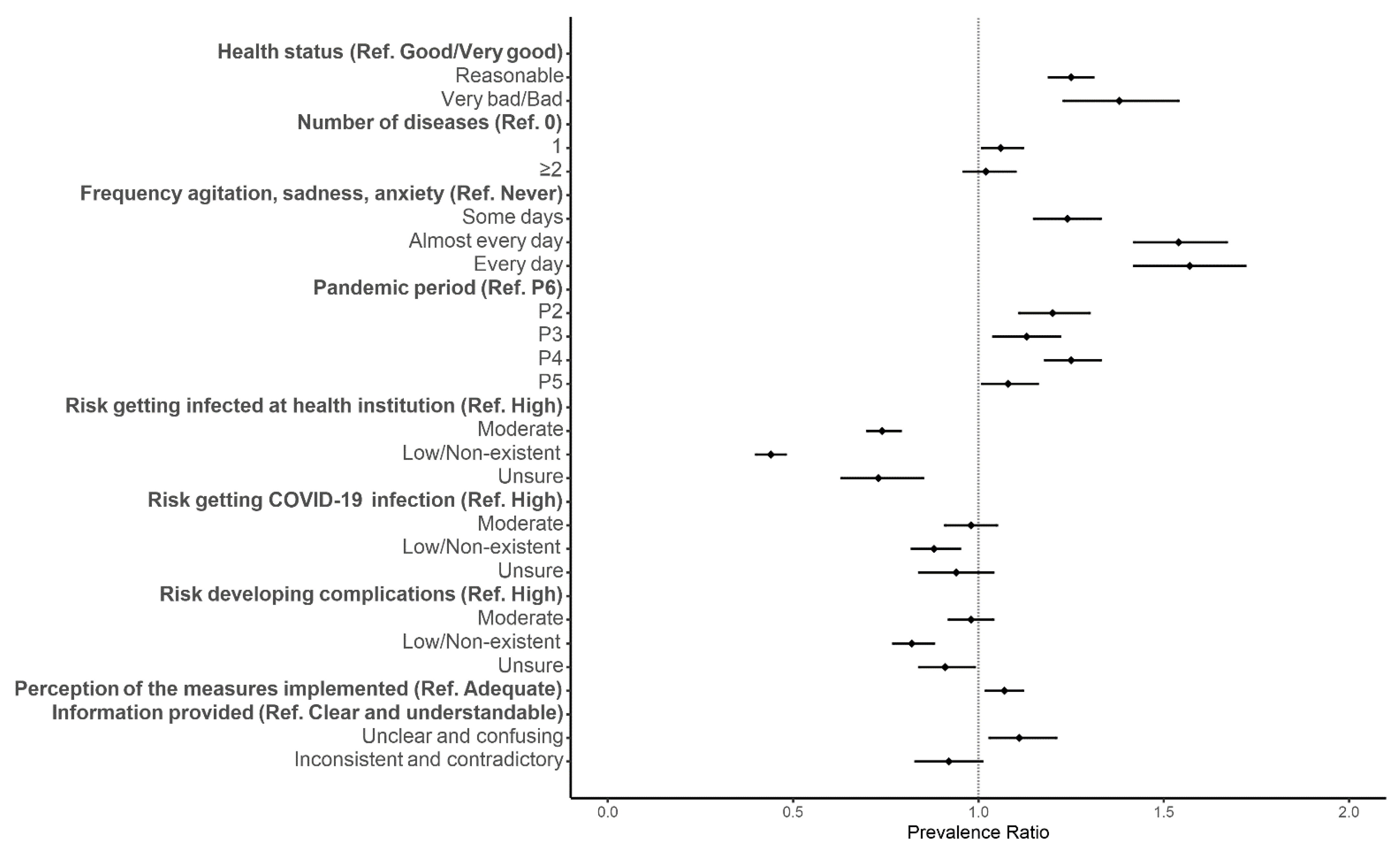
3.3. Need for Care
3.4. COVID-19-Specific Factors
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19—11 March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 7 July 2021).
- Ishaque Saah, F.; Amu, H.; Seidu, A.-A.; Bain, L.E. Health Knowledge and Care Seeking Behaviour in Resource-Limited Settings amidst the COVID-19 Pandemic: A Qualitative Study in Ghana. PLoS ONE 2021, 16, e0250940. [Google Scholar] [CrossRef]
- Roy, C.M.; Bollman, E.B.; Carson, L.M.; Northrop, A.J.; Jackson, E.F.; Moresky, R.T. Assessing the Indirect Effects of COVID-19 on Healthcare Delivery, Utilization and Health Outcomes: A Scoping Review. Eur. J. Public Health 2020, 31, 634–640. [Google Scholar] [CrossRef] [PubMed]
- Mira, J.J.; Lorenzo, S. Collateral Damage for Failing to Do in the Times of COVID-19. J. Healthc. Qual. Res. 2021, 36, 125–127. [Google Scholar] [CrossRef]
- Iacobucci, G. COVID-19: All Non-Urgent Elective Surgery Is Suspended for at Least Three Months in England. BMJ 2020, 1106, 18–19. [Google Scholar] [CrossRef] [Green Version]
- Sharon, K. Byrne. Healthcare Avoidance: A Critical Review. Holist. Nurs. Pract. 2008, 22, 280–292. [Google Scholar] [CrossRef]
- Singh, D.R.; Sunuwar, D.R.; Shah, S.K.; Karki, K.; Sah, L.K.; Adhikari, B.; Sah, R.K. Impact of COVID-19 on Health Services Utilization in Province-2 of Nepal: A Qualitative Study among Community Members and Stakeholders. BMC Health Serv. Res. 2021, 21, 174. [Google Scholar] [CrossRef]
- Lee, M.; You, M. Avoidance of Healthcare Utilization in South Korea during the Coronavirus Disease 2019 (COVID-19) Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 4363. [Google Scholar] [CrossRef]
- Andersen, R.M. Revisiting the Behavioral Model and Access to Medical Care: Does It Matter? J. Health Soc. Behav. 1995, 36, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Findling, M.G.; Blendon, R.J.; Benson, J.M. Delayed Care with Harmful Health Consequences—Reported Experiences from National Surveys During Coronavirus Disease 2019. JAMA Health Forum 2020, 1, e201463. [Google Scholar] [CrossRef]
- Czeisler, M.É.; Kennedy, J.L.; Wiley, J.F.; Facer-Childs, E.R.; Robbins, R.; Barger, L.K.; Czeisler, C.A.; Rajaratnam, S.M.W.; Howard, M.E. Delay or Avoidance of Routine, Urgent and Emergency Medical Care Due to Concerns about COVID-19 in a Region with Low COVID-19 Prevalence: Victoria, Australia. Respirol. Case Rep. 2021, 26, 701–712. [Google Scholar] [CrossRef]
- Czeisler, M.É.; Marynak, K.; Clarke, K.E.N.; Salah, Z.; Shakya, I.; Thierry, J.M.; Ali, N.; McMillan, H.; Wiley, J.F.; Weaver, M.D.; et al. Delay or Avoidance of Medical Care Because of COVID-19—Related Concerns—United States, June 2020. Available online: https://www.cdc.gov/mmwr/volumes/69/wr/mm6936a4.htm (accessed on 1 November 2021).
- Vieira, A.; Peixoto, V.R.; Aguiar, P.; Sousa, P.; Abrantes, A. Excess Non-COVID-19 Mortality in Portugal: Seven Months after the First Death. Port. J. Public Health 2021, 38 (Suppl. 1), 51–57. [Google Scholar] [CrossRef]
- Kondilis, E.; Tarantilis, F.; Benos, A. Essential Public Healthcare Services Utilization and Excess Non-COVID-19 Mortality in Greece. Public Health 2021, 198, 85–88. [Google Scholar] [CrossRef]
- Cronin, C.J.; Evans, W.N. Excess Mortality from COVID and Non-COVID Causes in Minority Populations. Proc. Natl. Acad. Sci. USA 2021, 118, e2101386118. [Google Scholar] [CrossRef]
- Dryhurst, S.; Schneider, C.R.; Kerr, J.; Freeman, A.L.J.; Recchia, G.; Van Der Bles, A.M.; Spiegelhalter, D.; Van Der Linden, S. Risk Perceptions of COVID-19 around the World. J. Risk Res. 2020, 23, 994–1006. [Google Scholar] [CrossRef]
- Darker, C.; Whittaker, A.C. Risk Perception. In Encyclopedia of Behavioral Medicine; Gellman, M., Ed.; Springer: New York, NY, USA, 2018; pp. 1–3. [Google Scholar] [CrossRef]
- Santana, R.; Sousa, J.S.; Soares, P.; Lopes, S.; Boto, P.; Rocha, J.V. The Demand for Hospital Emergency Services: Trends during the First Month of COVID-19 Response. Port. J. Public Health 2020, 38, 30–36. [Google Scholar] [CrossRef]
- Rocha, J.; Soares, P.; Filipe, C.; Lopes, S.; Teixeira, M.; Fonseca, I.; Sousa, J.; Marquês, D.; Mestre, R.; Duarte, A.; et al. Inpatient Hospitalizations during the First Wave of COVID-19 in Portugal. Port. J. Public Health 2021, 38, 11–17. [Google Scholar] [CrossRef]
- Parpia, A.S.; Ndeffo-mbah, M.L.; Wenzel, N.S.; Galvani, A.P. Effects of Response to 2014–2015 Ebola Outbreak on Deaths from Malaria, HIV / AIDS, and Tuberculosis, West Africa. Emerg. Infect. Dis. 2016, 22, 433–441. [Google Scholar] [CrossRef] [PubMed]
- Wagenaar, B.H.; Augusto, O.; Beste, J.; Toomay, S.J.; Wickett, E.; Dunbar, N.; Bawo, L.; Wesseh, C.S. The 2014–2015 Ebola Virus Disease Outbreak and Primary Healthcare Delivery in Liberia: Time-Series Analyses for 2010–2016. PLoS Med. 2018, 15, e1002508. [Google Scholar] [CrossRef] [Green Version]
- Delamou, A.; El Ayadi, A.M.; Sidibe, S.; Delvaux, T.; Camara, B.S.; Sandouno, S.D.; Beavogui, A.H.; Rutherford, G.W.; Okumura, J.; Zhang, W.-H.; et al. Effect of Ebola Virus Disease on Maternal and Child Health Services in Guinea: A Retrospective Observational Cohort Study. Lancet Glob. Health 2017, 5, e448–e457. [Google Scholar] [CrossRef] [Green Version]
- Laires, P.A.; Dias, S.; Gama, A.; Moniz, A.M.; Pedro, A.R.; Soares, P.; Aguiar, P.; Nunes, C. The Association of Chronic Diseases with COVID-19 Outcomes and Its Role on Risk Perception: Nationwide COVID-19 Database & Online Community-Based Survey (Preprint). JMIR Public Health Surveill. 2020, 7, e22794. [Google Scholar] [CrossRef]
- Pedro, A.R.; Gama, A.; Soares, P.; Moniz, M.; Laires, P.A.; Dias, S. COVID-19 Barometer: Social Opinion—What Do the Portuguese Think in This Time of COVID-19 ? Port. J. Public Health 2021, 38 (Suppl. 1), 42–50. [Google Scholar] [CrossRef]
- Babitsch, B.; Gohl, D.; von Lengerke, T. Re-Revisiting Andersen’s Behavioral Model of Health Services Use: A Systematic Review of Studies from 1998–2011. GMS Psycho-Soc.-Med. 2012, 9, 1–15. [Google Scholar]
- Zou, G. A Modified Poisson Regression Approach to Prospective Studies with Binary Data. Am. J. Epidemiol. 2004, 159, 702–706. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020. [Google Scholar]
- Lu, P.; Kong, D.; Shelley, M. Risk Perception, Preventive Behavior, and Medical Care Avoidance among American Older Adults During the COVID-19 Pandemic. J. Ageing Health 2021, 33, 577–584. [Google Scholar] [CrossRef]
- Ganson, K.T.; Weiser, S.D.; Tsai, A.C.; Nagata, J.M. Associations between Anxiety and Depression Symptoms and Medical Care Avoidance during COVID-19. J. Gen. Intern. Med. 2020, 35, 3406–3408. [Google Scholar] [CrossRef]
- Gil-Lacruz, M.; Gil-Lacruz, A.I. Health Perception and Health Care Access: Sex Differences in Behaviors and Attitudes. Am. J. Econ. Sociol. 2010, 69, 783–801. [Google Scholar] [CrossRef]
- Bertakis, K.D.; Azari, R.; Helms, L.J.; Callahan, E.; Robbins, J.A. Gender Differences in the Utilization of Health Care Services. J. Fam. Pract. 2000, 49, 147–152. [Google Scholar] [PubMed]
- Siegrist, M.; Luchsinger, L.; Bearth, A. The Impact of Trust and Risk Perception on the Acceptance of Measures to Reduce COVID-19 Cases. Risk Anal. 2021, 41, 787–800. [Google Scholar] [CrossRef]
- Instituto Nacional de Estatística. Inquérito Nacional de Saúde. 2014. Available online: https://www.ine.pt/xurl/pub/263714091 (accessed on 25 January 2021).
- Hengen, K.M.; Alpers, G.W. What’s the Risk? Fearful Individuals Generally Overestimate Negative Outcomes and They Dread Outcomes of Specific Events. Front. Psychol. 2019, 10, 1676. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Dimensions Considered | Variables |
|---|---|
| Predisposing | Sex |
| Age group | |
| Region | |
| Education | |
| Occupation | |
| Confidence in the capacity of health services to respond to COVID-19 | |
| Confidence in the capacity of health services to respond to non-COVID-19 | |
| Enabling | Monthly household income |
| Partial or total income loss during the pandemic | |
| Need for care | Perception of the health status |
| Number of diseases | |
| Frequency of agitation, sadness or anxiety due to the physical distancing measures | |
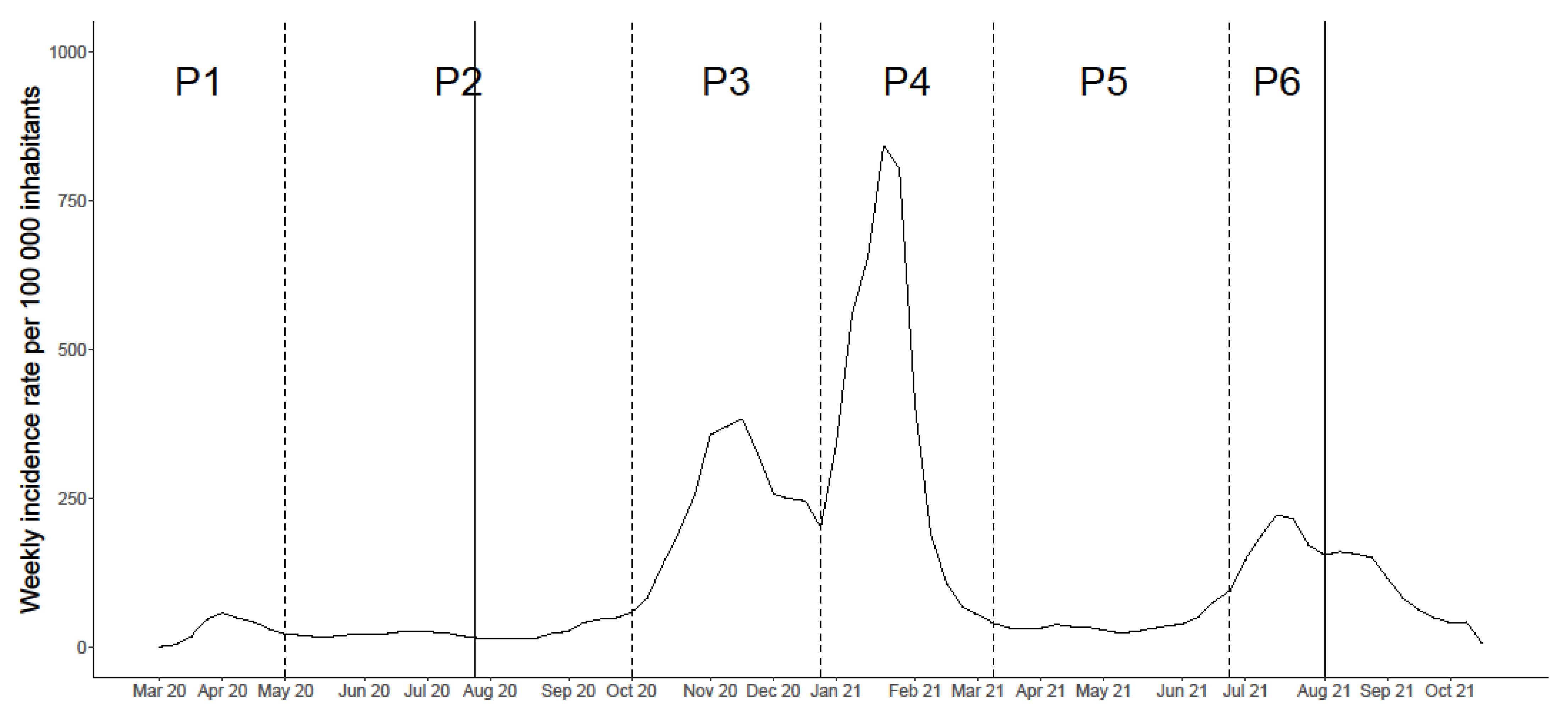
| Period of the pandemic | |
| COVID-19 specific | Self-perceived risk of getting COVID-19 |
| Self-perceived risk of developing severe disease following SARS-CoV-2 infection | |
| Self-perceived risk of getting infected in a health institution | |
| Perception of the level of adequacy of measures implemented by the Government | |
| Perception of the information provided by health authorities |
| Total Sample (N = 9660) | Healthcare Avoidance (N = 4216, 43.6%) | Did Not Avoid and/or Delay Healthcare (N = 5444, 56.4%) | |
|---|---|---|---|
| N (%) | N (%) | N (%) | |
| Predisposing | |||
| Sex (N = 9626) | |||
| Male | 2494 (25.9%) | 911 (21.7%) | 1583 (29.2%) |
| Female | 7132 (74.1%) | 3289 (78.3%) | 3843 (70.8%) |
| Age (N = 9660) | |||
| 18–24 years | 384 (4.0%) | 146 (3.5%) | 238 (4.4%) |
| 25–64 years | 7752 (80.2%) | 3416 (81.0%) | 4336 (79.6%) |
| ≥65 years | 1524 (15.8%) | 654 (15.5%) | 870 (16.0%) |
| Region (N = 9660) | |||
| North | 1942 (20.1%) | 806 (19.1%) | 1136 (20.9%) |
| Center | 1406 (14.6%) | 583 (13.8%) | 823 (15.1%) |
| Lisbon and Tagus Valley | 5354 (55.4%) | 2399 (56.9%) | 2955 (54.3%) |
| Alentejo | 417 (4.32%) | 198 (4.70%) | 219 (4.02%) |
| Algarve | 381 (3.94%) | 181 (4.29%) | 200 (3.67%) |
| Azores | 100 (1.04%) | 30 (0.71%) | 70 (1.29%) |
| Madeira | 60 (0.62%) | 19 (0.45%) | 41 (0.75%) |
| Education (N = 9615) | |||
| No education/Basic education | 573 (5.96%) | 241 (5.75%) | 332 (6.12%) |
| Secondary | 2166 (22.5%) | 914 (21.8%) | 1252 (23.1%) |
| University | 6876 (71.5%) | 3038 (72.5%) | 3838 (70.8%) |
| Occupation (N = 9660) | |||
| Worker | 6849 (70.9%) | 2971 (70.5%) | 3878 (71.2%) |
| Student | 339 (3.51%) | 137 (3.25%) | 202 (3.71%) |
| Retired | 1434 (14.8%) | 635 (15.1%) | 799 (14.7%) |
| Unemployed | 451 (4.67%) | 198 (4.70%) | 253 (4.65%) |
| Other | 587 (6.08%) | 275 (6.52%) | 312 (5.73%) |
| Confidence in the capacity of health services to respond to COVID-19 (N = 9585) | |||
| High | 7361 (76.8%) | 3068 (73.3%) | 4293 (79.5%) |
| Low | 2224 (23.2%) | 1118 (26.7%) | 1106 (20.5%) |
| Confidence in the capacity of health services to respond to non-COVID-19 (N = 9593) | |||
| High | 4423 (46.1%) | 1688 (40.4%) | 2735 (50.5%) |
| Low | 5170 (53.9%) | 2490 (59.6%) | 2680 (49.5%) |
| Enabling | |||
| Monthly household income (N = 8644) | |||
| <EUR 650 | 508 (5.88%) | 211 (5.61%) | 297 (6.08%) |
| EUR 651–1000 | 1222 (14.1%) | 553 (14.7%) | 669 (13.7%) |
| EUR 1001–1500 | 1878 (21.7%) | 830 (22.1%) | 1048 (21.4%) |
| EUR 1501–2000 | 1587 (18.4%) | 680 (18.1%) | 907 (18.6%) |
| EUR 2001–2500 | 1352 (15.6%) | 607 (16.2%) | 745 (15.2%) |
| >EUR 2501 | 2097 (24.3%) | 877 (23.3%) | 1220 (25.0%) |
| Loss of income due to the pandemic (N = 9446) | |||
| No | 6778 (71.8%) | 2870 (69.9%) | 3908 (73.2%) |
| Partial/Total | 2668 (28.2%) | 1237 (30.1%) | 1431 (26.8%) |
| Need for care | |||
| Perception of the health status (N = 9625) | |||
| Very good/Good | 5418 (56.3%) | 2121 (50.4%) | 3297 (60.8%) |
| Reasonable | 3889 (40.4%) | 1914 (45.5%) | 1975 (36.4%) |
| Bad/Very bad | 318 (3.30%) | 170 (4.04%) | 148 (2.73%) |
| Number of diseases (N = 9413) | |||
| 0 | 5018 (53.3%) | 2084 (50.6%) | 2934 (55.5%) |
| 1 | 2853 (30.3%) | 1326 (32.2%) | 1527 (28.9%) |
| ≥2 | 1537 (16.3%) | 709 (17.2%) | 828 (15.7%) |
| Frequency of agitation, sadness or anxiety due to the physical distance measures (N = 9624) | |||
| Never | 1901 (19.8%) | 612 (14.6%) | 1289 (23.8%) |
| Some days | 5588 (58.1%) | 2402 (57.1%) | 3186 (58.8%) |
| Almost every day | 1411 (14.7%) | 777 (18.5%) | 634 (11.7%) |
| Every day | 724 (7.52%) | 412 (9.80%) | 312 (5.76%) |
| Pandemic period (N = 9660) | |||
| P2 | 1071 (11.1%) | 499 (11.8%) | 572 (10.5%) |
| P3 | 1121 (11.6%) | 486 (11.5%) | 635 (11.7%) |
| P4 | 2284 (23.6%) | 1116 (26.5%) | 1168 (21.5%) |
| P5 | 1757 (18.2%) | 757 (18.0%) | 1000 (18.4%) |
| P6 | 3427 (35.5%) | 1358 (32.2%) | 2069 (38.0%) |
| COVID-19 specific | |||
| Self-perceived risk of getting COVID-19 (N = 9635) | |||
| High | 1091 (11.3%) | 533 (12.7%) | 558 (10.3%) |
| Moderate | 4004 (41.6%) | 1836 (43.6%) | 2168 (39.9%) |
| Low/No risk | 3885 (40.3%) | 1546 (36.7%) | 2339 (43.1%) |
| Unsure | 655 (6.80%) | 292 (6.94%) | 363 (6.69%) |
| Self-perceived risk to develop severe disease following SARS-CoV-2 infection (N = 9627) | |||
| High | 1699 (17.6%) | 864 (20.5%) | 835 (15.4%) |
| Moderate | 2948 (30.6%) | 1384 (32.9%) | 1564 (28.8%) |
| Low/No risk | 3639 (37.8%) | 1369 (32.6%) | 2270 (41.9%) |
| Unsure | 1341 (13.9%) | 588 (14.0%) | 753 (13.9%) |
| Self-perceived risk to get infected in a health institution (N = 5399) | |||
| High | 822 (15.2%) | 566 (22.6%) | 256 (8.84%) |
| Moderate | 2429 (45.0%) | 1247 (49.8%) | 1182 (40.8%) |
| Low/No risk | 1978 (36.6%) | 604 (24.1%) | 1374 (47.4%) |
| Unsure | 170 (3.15%) | 86 (3.44%) | 84 (2.90%) |
| Perception of the level of adequacy of the measures implemented by the Government (N = 9423) | |||
| Adequate | 5886 (62.5%) | 2509 (61.1%) | 3377 (63.5%) |
| Inadequate | 3537 (37.5%) | 1597 (38.9%) | 1940 (36.5%) |
| View on the information provided by the health authorities (N = 3926) | |||
| Clear and understandable | 2398 (61.1%) | 1118 (61.1%) | 1280 (61.1%) |
| Unclear and confusing | 730 (18.6%) | 380 (20.8%) | 350 (16.7%) |
| Inconsistent and contradictory | 798 (20.3%) | 333 (18.2%) | 465 (22.2%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Soares, P.; Leite, A.; Esteves, S.; Gama, A.; Laires, P.A.; Moniz, M.; Pedro, A.R.; Santos, C.M.; Goes, A.R.; Nunes, C.; et al. Factors Associated with the Patient’s Decision to Avoid Healthcare during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 13239. https://doi.org/10.3390/ijerph182413239
Soares P, Leite A, Esteves S, Gama A, Laires PA, Moniz M, Pedro AR, Santos CM, Goes AR, Nunes C, et al. Factors Associated with the Patient’s Decision to Avoid Healthcare during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2021; 18(24):13239. https://doi.org/10.3390/ijerph182413239
Chicago/Turabian StyleSoares, Patrícia, Andreia Leite, Sara Esteves, Ana Gama, Pedro Almeida Laires, Marta Moniz, Ana Rita Pedro, Cristina Mendes Santos, Ana Rita Goes, Carla Nunes, and et al. 2021. "Factors Associated with the Patient’s Decision to Avoid Healthcare during the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 18, no. 24: 13239. https://doi.org/10.3390/ijerph182413239
APA StyleSoares, P., Leite, A., Esteves, S., Gama, A., Laires, P. A., Moniz, M., Pedro, A. R., Santos, C. M., Goes, A. R., Nunes, C., & Dias, S. (2021). Factors Associated with the Patient’s Decision to Avoid Healthcare during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health, 18(24), 13239. https://doi.org/10.3390/ijerph182413239