
Differences in Coping Strategies and Help-Seeking Behaviours among Australian Junior and Senior Doctors during the COVID-19 Pandemic

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Sample
2.2. Data Collection
2.3. Statistical Methods and Data Analysis
3. Results
3.1. Prevalence of Mental Health Issues
3.2. Utilisation of Coping Strategies and Help-Seeking Behaviour
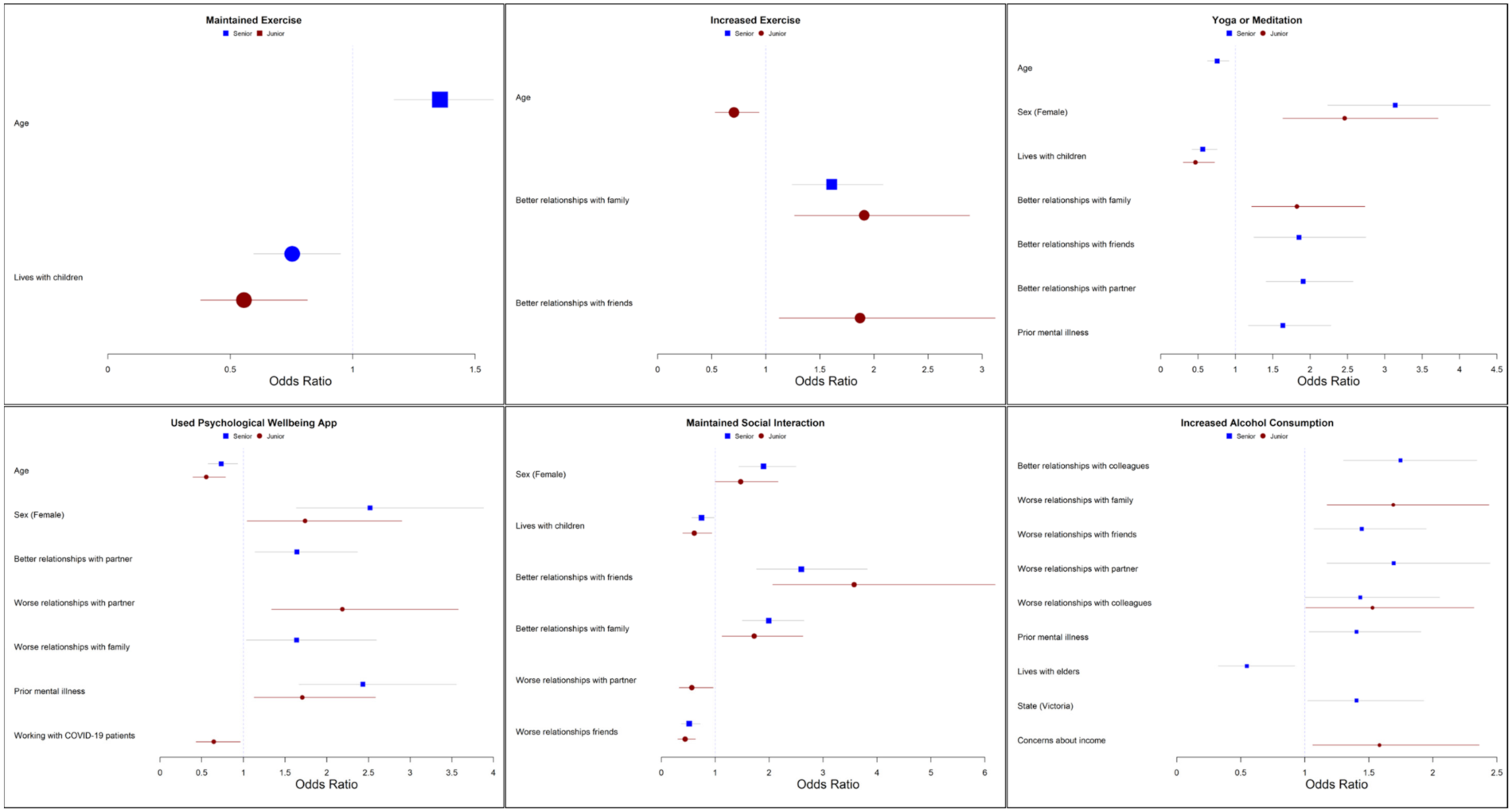
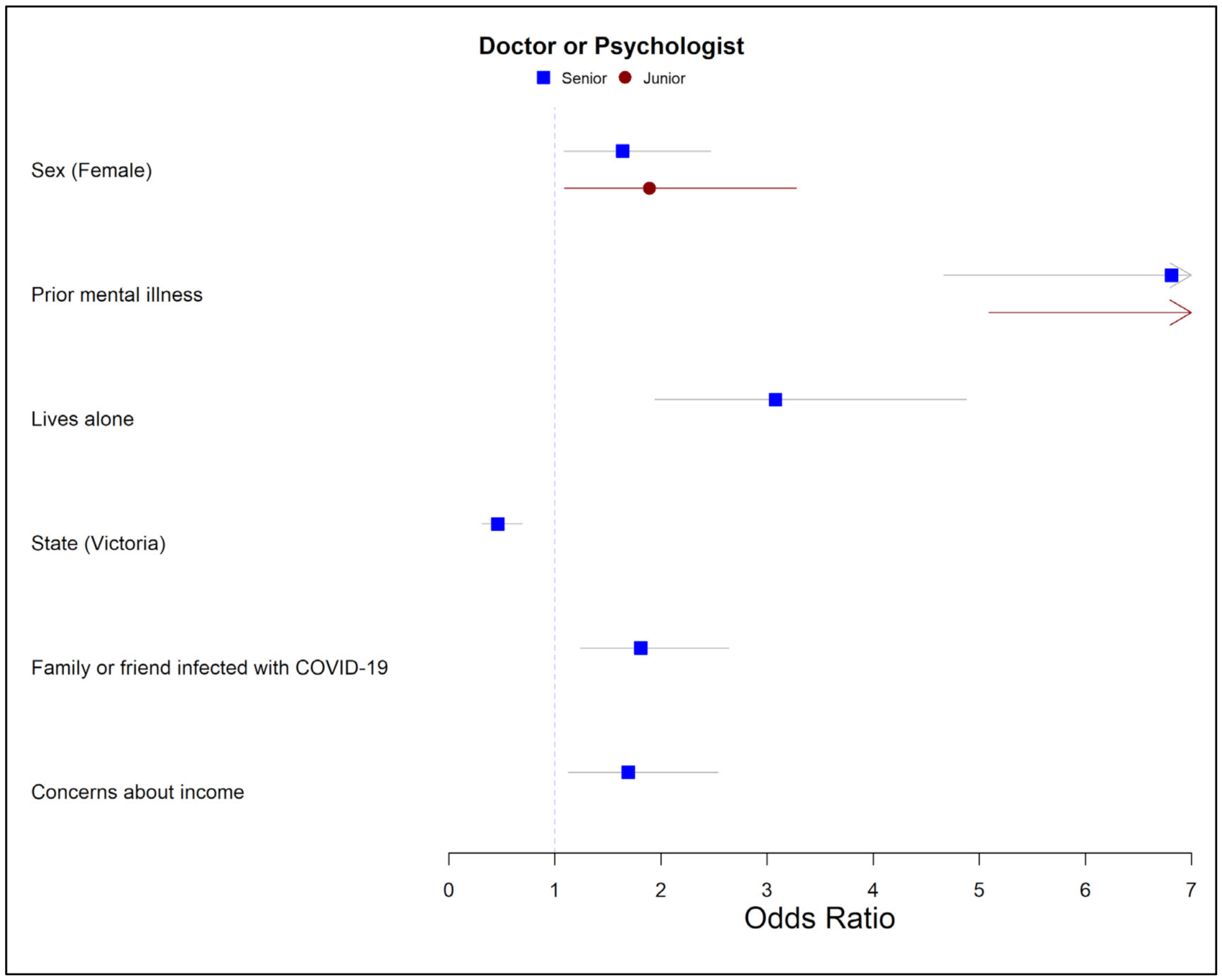
3.3. Predictors of Coping Strategies and Help-Seeking Behaviour
3.4. Coping Strategies, Help-Seeking Behaviour and Mental Health Symptoms
4. Discussion
4.1. Coping Strategies Varied by Seniority
4.2. Low Levels of Engagement with Professional Support Services
4.3. Increased Alcohol Consumption Associated with Symptoms of Mental Illness
4.4. Implications
4.5. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rimmer, A. Over 80% of doctors work unpaid overtime, NHS survey shows. BMJ 2015, 350, h1086. [Google Scholar] [CrossRef]
- Soares, D.S.; Chan, L. Stress and wellbeing of junior doctors in Australia: A comparison with American doctors and population norms. BMC Med. Educ. 2016, 16, 183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basso, A.; Serra, R.; Drago, I.; Soleo, L.; Lovreglio, P. Biological accidents at work among resident physicians in specialist training at Bari University Hospital, Italy. Am. J. Infect. Control. 2016, 44, e265–e267. [Google Scholar] [CrossRef] [PubMed]
- Sime, W.; Quick, J.; Saleh, K.; Martin, W. Critical Decisions, Trauma, and Burnout in Medicine: A Stress Management Challenge to Physician Well-Being. Biofeedback 2007, 35, 95–100. [Google Scholar]
- Kumar, S. Burnout and Doctors: Prevalence, Prevention and Intervention. Healthcare 2016, 4, 37. [Google Scholar] [CrossRef] [Green Version]
- Smallwood, N.; Karimi, L.; Bismark, M.; Putland, M.; Johnson, D.; Dharmage, S.C.; Barson, E.; Atkin, N.; Long, C.; Ng, I.; et al. High levels of psychosocial distress among Australian frontline healthcare workers during the COVID-19 pandemic: A cross-sectional survey. Gen. Psychiatry 2021, 34, e100577. [Google Scholar] [CrossRef]
- Smallwood, N.; Pascoe, A.; Karimi, L.; Bismark, M.; Willis, K. Occupational Disruptions during the COVID-19 Pandemic and Their Association with Healthcare Workers’ Mental Health. Int. J. Environ. Res. Public Health 2021, 18, 9263. [Google Scholar] [CrossRef]
- Holton, S.; Wynter, K.; Trueman, M.; Bruce, S.; Sweeney, S.; Crowe, S.; Dabscheck, A.; Eleftheriou, P.; Booth, S.; Hitch, D.; et al. Psychological well-being of Australian hospital clinical staff during the COVID-19 pandemic. Aust. Health Rev. 2020, 45, 297–305. [Google Scholar] [CrossRef]
- Smallwood, N.; Pascoe, A.; Karimi, L.; Willis, K. Moral Distress and Perceived Community Views Are Associated with Mental Health Symptoms in Frontline Health Workers during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 8723. [Google Scholar] [CrossRef]
- Smallwood, N.; Karimi, L.; Pascoe, A.; Bismark, M.; Putland, M.; Johnson, D.; Dharmage, S.C.; Barson, E.; Atkin, N.; Long, C.; et al. Coping strategies adopted by Australian frontline health workers to address psychological distress during the COVID-19 pandemic. Gen. Hosp. Psychiatry 2021, 72, 124–130. [Google Scholar] [CrossRef]
- Vizheh, M.; Qorbani, M.; Arzaghi, S.M.; Muhidin, S.; Javanmard, Z.; Esmaeili, M. The mental health of healthcare workers in the COVID-19 pandemic: A systematic review. J. Diabetes Metab. Disord. 2020, 19, 1967–1978. [Google Scholar] [CrossRef]
- Uphoff, E.P.; Lombardo, C.; Johnston, G.; Weeks, L.; Rodgers, M.; Dawson, S.; Seymour, C.; Kousoulis, A.A.; Churchill, R. Mental health among healthcare workers and other vulnerable groups during the COVID-19 pandemic and other coronavirus outbreaks: A rapid systematic review. PLoS ONE 2021, 16, e0254821. [Google Scholar] [CrossRef]
- Wu, P.; Liu, X.; Fang, Y.; Fan, B.; Fuller, C.J.; Guan, Z.; Yao, Z.; Kong, J.; Lu, J.; Litvak, I.J. Alcohol abuse/dependence symptoms among hospital employees exposed to a SARS outbreak. Alcohol Alcohol. 2008, 43, 706–712. [Google Scholar] [CrossRef]
- Hugelius, K.; Adolfsson, A.; Örtenwall, P.; Gifford, M. Being Both Helpers and Victims: Health Professionals’ Experiences of Working During a Natural Disaster. Prehosp. Disaster Med. 2017, 32, 117–123. [Google Scholar] [CrossRef]
- Man, M.A.; Toma, C.; Motoc, N.S.; Necrelescu, O.L.; Bondor, C.I.; Chis, A.F.; Lesan, A.; Pop, C.M.; Todea, D.A.; Dantes, E.; et al. Disease Perception and Coping with Emotional Distress During COVID-19 Pandemic: A Survey Among Medical Staff. Int. J. Environ. Res. Public Health 2020, 17, 4899. [Google Scholar] [CrossRef]
- Shechter, A.; Diaz, F.; Moise, N.; Anstey, D.; Ye, S.; Agarwal, S.; Birk, J.L.; Brodie, D.; Cannone, D.E.; Chang, B.; et al. Psychological distress, coping behaviors, and preferences for support among New York healthcare workers during the COVID-19 pandemic. Gen. Hosp. Psychiatry 2020, 66, 1–8. [Google Scholar] [CrossRef]
- Zhu, W.; Wei, Y.; Meng, X.; Li, J. The mediation effects of coping style on the relationship between social support and anxiety in Chinese medical staff during COVID-19. BMC Health Serv. Res. 2020, 20, 1007. [Google Scholar] [CrossRef]
- Babore, A.; Lombardi, L.; Viceconti, M.L.; Pignataro, S.; Marino, V.; Crudele, M.; Candelori, C.; Bramanti, S.M.; Trumello, C. Psychological effects of the COVID-2019 pandemic: Perceived stress and coping strategies among healthcare professionals. Psychiatry Res. 2020, 293, 113366. [Google Scholar] [CrossRef]
- Colville, G.A.; Smith, J.; Brierley, J.; Citron, K.; Nguru, N.M.; Shaunak, P.D.; Tam, O.; Perkins-Porras, L. Coping With Staff Burnout and Work-Related Posttraumatic Stress in Intensive Care. Pediatr. Crit. Care Med. 2017, 18, e267–e273. [Google Scholar] [CrossRef]
- Beyondblue Doctors’ Mental Health Program. National Mental Health Survey of Doctors and Medical Students. Available online: https://medicine.uq.edu.au/files/42088/Beyondblue%20Doctors%20Mental%20health.pdf (accessed on 23 April 2021).
- Hayes, B.; Prihodova, L.; Walsh, G.; Doyle, F.; Doherty, S. What’s up doc? A national cross-sectional study of psychological wellbeing of hospital doctors in Ireland. BMJ Open 2017, 7, e018023. [Google Scholar] [CrossRef] [Green Version]
- Petrie, K.; Crawford, J.; Lamontagne, A.D.; Milner, A.; Dean, J.; Veness, B.G.; Christensen, H.; Harvey, S.B. Working hours, common mental disorder and suicidal ideation among junior doctors in Australia: A cross-sectional survey. BMJ Open 2020, 10, e033525. [Google Scholar] [CrossRef] [Green Version]
- Fitzpatrick, O.; Biesma, R.; Conroy, R.M.; McGarvey, A. Prevalence and relationship between burnout and depression in our future doctors: A cross-sectional study in a cohort of preclinical and clinical medical students in Ireland. BMJ Open 2019, 9, e023297. [Google Scholar] [CrossRef] [Green Version]
- Forbes, M.P.; Iyengar, S.; Kay, M. Barriers to the psychological well-being of Australian junior doctors: A qualitative analysis. BMJ Open 2019, 9, e027558. [Google Scholar] [CrossRef] [Green Version]
- Torjesen, I. COVID-19: Doctors need proper mental health support, says BMA. BMJ 2020, 369, m2192. [Google Scholar] [CrossRef]
- Royal College of Physicians. More Than 1 in 4 Doctors Have Sought Mental Health Support during the Pandemic. Available online: https://www.rcplondon.ac.uk/news/more-1-4-doctors-have-sought-mental-health-support-during-pandemic (accessed on 23 September 2021).
- Tsirtsakis, A. ‘We Can Only Soak up so Much before It Starts to Affect Us’. A New E-Mental Health Hub Will Connect Frontline Healthcare Workers with Services to Cope with the Stress of the Ongoing Pandemic. Available online: https://www1.racgp.org.au/newsgp/professional/we-can-only-soak-up-so-much-before-it-starts-to-af (accessed on 27 September 2021).
- Australian Government Department of Health. Coronavirus (COVID-19) at a Glance—23 October 2020. Available online: https://www.health.gov.au/resources/publications/coronavirus-covid-19-at-a-glance-23-october-2020 (accessed on 2 June 2021).
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [Green Version]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [Green Version]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Thoresen, S.; Tambs, K.; Hussain, A.; Heir, T.; Johansen, V.; Bisson, J. Brief measure of posttraumatic stress reactions: Impact of Event Scale-6. Soc. Psychiatry Psychiatr. Epidemiol. 2009, 45, 405–412. [Google Scholar] [CrossRef]
- Vaishnavi, S.; Connor, K.; Davidson, J.R. An abbreviated version of the Connor-Davidson Resilience Scale (CD-RISC), the CD-RISC2: Psychometric properties and applications in psychopharmacological trials. Psychiatry Res. 2007, 152, 293–297. [Google Scholar] [CrossRef] [Green Version]
- Murray-Atfield, Y.; Dunstan, J. Melbourne Placed under Stage 4 Lockdown, 8pm Curfew, Regional Victoria Moved to Stage 3 Restrictions; Australian Broadcasting Corporation: Sydney, Australia, 2020; 8p. [Google Scholar]
- El-Osta, A.; Alaa, A.; Webber, I.; Sasco, E.R.; Bagkeris, E.; Millar, H.; Vidal-Hall, C.; Majeed, A. How is the COVID-19 lockdown impacting the mental health of parents of school-age children in the UK? A cross-sectional online survey. BMJ Open 2021, 11, e043397. [Google Scholar] [CrossRef]
- Penman, S.; Stevens, P.; Cohen, M.; Jackson, S. Yoga in Australia: Results of a national survey. Int. J. Yoga 2012, 5, 92–101. [Google Scholar] [CrossRef] [PubMed]
- Daly, N.; Robb, K. Junior Doctors to Launch New Class Action Claiming Unrostered, Unpaid Overtime. Available online: https://www.abc.net.au/news/2021-05-19/junior-doctors-new-class-action-claiming-unpaid-overtime/100147606 (accessed on 11 June 2021).
- Lopez, A.M.; Lam, K.; Thota, R. Barriers and Facilitators to Telemedicine: Can You Hear Me Now? Am. Soc. Clin. Oncol. Educ. Book 2021, 41, 25–36. [Google Scholar] [CrossRef] [PubMed]
- Upton, E.; Clare, P.J.; Aiken, A.; Boland, V.C.; De Torres, C.; Bruno, R.; Hutchinson, D.; Kypri, K.; Mattick, R.; McBride, N.; et al. Changes in mental health and help-seeking among young Australian adults during the COVID-19 pandemic: A prospective cohort study. Psychol. Med. 2021, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Terhaag, S.; Quinn, B.; Swami, N.; Daraganova, G. Mental Health of Australian Males: Depression, Suicidality and Loneliness. Available online: https://tentomen.org.au/sites/default/files/publication-documents/2020_ttm_insights_report_chapter_1.pdf (accessed on 14 April 2021).
- Australian Institute of Health and Welfare. National Drug Strategy Household Survey 2016: Detailed Findings. Available online: https://www.aihw.gov.au/reports/illicit-use-of-drugs/2016-ndshs-detailed/summary (accessed on 15 September 2021).
- Nash, L.M.; Daly, M.; Kelly, P.J.; Van Ekert, E.H.; Walter, G.; Walton, M.; Willcock, S.M.; Tennant, C.C. Factors associated with psychiatric morbidity and hazardous alcohol use in Australian doctors. Med. J. Aust. 2010, 193, 161–166. [Google Scholar] [CrossRef]
- Tran, T.D.; Hammarberg, K.; Kirkman, M.; Nguyen, H.T.M.; Fisher, J. Alcohol use and mental health status during the first months of COVID-19 pandemic in Australia. J. Affect. Disord. 2020, 277, 810–813. [Google Scholar] [CrossRef]
- Medisauskaite, A.; Kamau, C. Does occupational distress raise the risk of alcohol use, binge-eating, ill health and sleep problems among medical doctors? A UK cross-sectional study. BMJ Open 2019, 9, e027362. [Google Scholar] [CrossRef] [Green Version]
- Alcohol and Drug Foundation. Break the Habit Campaign. Available online: https://www.littlehabit.com.au/about/break-the-habit-campaign/ (accessed on 14 April 2021).
- Australian Bureau of Statistics. Household Impacts of COVID-19 Survey. Coronavirus (COVID-19) Impacts on Jobs, Lifestyle, Stressors, Wellbeing, Moving, Health Precautions and Use of Health Services. Available online: https://www.abs.gov.au/statistics/people/people-and-communities/household-impacts-covid-19-survey/24-29-june-2020 (accessed on 22 September 2021).
- Medical Board of Australia, Registration Data Table—December 2020. Available online: https://www.medicalboard.gov.au/news/statistics.aspx (accessed on 28 April 2021).
- Medical Board of Australia. Medical Board of Australia and Ahpra Medical Training Survey 2020 Annual Report. Available online: https://www.medicaltrainingsurvey.gov.au/Download/2020/2020%20MTS%20Report%20for%20ACD.pdf (accessed on 28 April 2021).



{kind=link}
{kind=link}
| Characteristic | Senior (n = 1221) | Junior (n = 745) | ||
|---|---|---|---|---|
| n | % | n | % | |
| Age (years) | ||||
| 20–30 | 3 | 0.2 | 361 | 48.5 |
| 31–40 | 325 | 26.6 | 339 | 45.5 |
| 41–50 | 483 | 39.6 | 38 | 5.1 |
| 50+ | 410 | 33.6 | 7 | 0.9 |
| Sex | ||||
| Male | 498 | 40.8 | 203 | 27.2 |
| Female | 715 | 58.6 | 536 | 71.9 |
| Non-binary | 5 | 0.4 | 1 | 0.1 |
| Prefer not to say | 3 | 0.2 | 5 | 0.7 |
| State | ||||
| Victoria | 932 | 76.3 | 613 | 82.3 |
| Other states | 289 | 23.6 | 132 | 17.8 |
| Location of practice | ||||
| Metropolitan | 1068 | 87.5 | 661 | 88.7 |
| Regional or Remote | 153 | 12.5 | 84 | 11.2 |
| Health organisation type # | ||||
| Public | 1118 | 91.6 | 735 | 98.7 |
| Community | 277 | 22.7 | 33 | 4.4 |
| Private | 470 | 38.5 | 54 | 7.2 |
| Other | 58 | 4.8 | 9 | 1.2 |
| Frontline area | ||||
| Emergency Department | 173 | 14.2 | 159 | 21.3 |
| ICU | 92 | 7.5 | 94 | 12.7 |
| Anaesthetics/peri-op/surgical | 261 | 21.4 | 74 | 9.9 |
| Medical specialty areas * | 642 | 52.6 | 391 | 52.5 |
| Other ** | 26 | 2.1 | 15 | 2.0 |
| Community *** | 27 | 2.2 | 12 | 1.6 |
| Current Employment Status | ||||
| Full time | 657 | 53.8 | 656 | 88.1 |
| Part time | 528 | 43.2 | 63 | 8.5 |
| Casual/other | 36 | 2.9 | 26 | 3.5 |
| Number of people in the household | ||||
| Lives alone | 145 | 11.9 | 133 | 17.9 |
| Children < 16 years at home | 684 | 56.0 | 164 | 22.0 |
| Person aged ≥ 65 at home | 109 | 8.9 | 38 | 5.1 |
| Categories | Senior (n = 1221) | Junior (n = 745) | Chi-Square | ||
|---|---|---|---|---|---|
| n | % | n | % | p | |
| Pre-existing mental health condition diagnosed before the pandemic | <0.001 | ||||
| No or prefer not to say | 973 | 79.7 | 539 | 72.3 | |
| Yes | 248 | 20.3 | 206 | 27.7 | |
| Activities to manage possible mental health issues since the pandemic started * | |||||
| Maintained exercise | 579 | 47.4 | 275 | 36.9 | <0.001 |
| Increased exercise | 334 | 27.4 | 179 | 24.0 | 0.103 |
| Yoga, meditation or similar | 269 | 22.0 | 219 | 29.4 | <0.001 |
| Maintained or increased social interaction with family and friends | 352 | 28.8 | 243 | 32.6 | 0.076 |
| Used a psychological wellbeing App (e.g., Smiling Mind, Headspace or other) | 149 | 12.2 | 129 | 17.3 | 0.002 |
| Increased alcohol use | 341 | 27.9 | 188 | 25.2 | 0.191 |
| Other strategy | 168 | 13.8 | 94 | 12.6 | 0.47 |
| None of the above | 145 | 11.9 | 112 | 15.0 | 0.044 |
| Sought help for stress or mental health issues from other sources * | |||||
| Doctor or psychologist | 162 | 13.3 | 134 | 18.0 | 0.005 |
| Employee support program at place of work | 39 | 3.2 | 20 | 2.7 | 0.521 |
| Professional support program outside of work | 23 | 1.9 | 17 | 2.3 | 0.544 |
| Other | 29 | 2.4 | 30 | 4.0 | 0.037 |
| None of the above | 997 | 81.7 | 569 | 76.4 | 0.005 |
| Mental Health Symptom | Maintained Exercise | Increased Exercise | Yoga or Meditation | Maintained Social Interactions | Used Psychological Wellbeing App | Increased Alcohol | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No | Yes | No | Yes | No | Yes | No | Yes | No | Yes | No | Yes | ||
| Junior | |||||||||||||
| Anxiety | None-mild | 61.9% | 38.1% | 76.6% | 23.4% | 71.7% | 28.3% | 64.7% | 35.3% | 83.8% | 16.2% | 79.6% | 20.4% |
| Mod-severe | 66.0% | 34.0% | 74.4% | 25.6% | 67.9% | 32.1% | 74.0% | 26.0% | 80.0% | 20.0% | 62.8% | 37.2% | |
| p | 0.286 | 0.527 | 0.303 | 0.015 | 0.217 | <0.001 | |||||||
| Depression | None-mild | 62.3% | 37.7% | 75.6% | 24.4% | 70.8% | 29.2% | 66.6% | 33.4% | 83.0% | 17.0% | 77.3% | 22.7% |
| Mod-severe | 66.2% | 33.8% | 77.2% | 22.8% | 70.3% | 29.7% | 71.0% | 29.0% | 81.4% | 18.6% | 64.1% | 35.9% | |
| p | 0.378 | 0.683 | 0.917 | 0.308 | 0.65 | 0.001 | |||||||
| PTSD | None-mild | 63.0% | 37.0% | 77.8% | 22.2% | 74.9% | 25.1% | 65.9% | 34.1% | 87.4% | 12.6% | 79.7% | 20.3% |
| Mod-severe | 62.8% | 37.2% | 73.8% | 26.2% | 65.2% | 34.8% | 69.8% | 30.2% | 76.8% | 23.2% | 68.6% | 31.4% | |
| p | 0.947 | 0.205 | 0.004 | 0.262 | <0.001 | 0.001 | |||||||
| MBI DP | None-low | 60.4% | 39.6% | 74.8% | 25.2% | 69.2% | 30.8% | 63.6% | 36.4% | 84.1% | 15.9% | 81.6% | 18.4% |
| Mod-high | 65.5% | 34.5% | 77.2% | 22.8% | 72.1% | 27.9% | 70.6% | 29.4% | 81.6% | 18.4% | 69.7% | 30.3% | |
| p | 0.155 | 0.446 | 0.387 | 0.042 | 0.364 | <0.001 | |||||||
| MBI EE | None-low | 57.3% | 42.7% | 79.8% | 20.2% | 72.5% | 27.5% | 58.4% | 41.6% | 86.0% | 14.0% | 87.1% | 12.9% |
| Mod-high | 65.2% | 34.8% | 75.0% | 25.0% | 70.3% | 29.7% | 70.5% | 29.5% | 81.6% | 18.4% | 71.0% | 29.0% | |
| p | 0.056 | 0.189 | 0.574 | 0.003 | 0.184 | <0.001 | |||||||
| MBI PA | None-low | 63.6% | 36.4% | 80.4% | 19.6% | 72.0% | 28.0% | 73.8% | 26.2% | 83.6% | 16.4% | 70.7% | 29.3% |
| Mod-high | 63.2% | 36.8% | 74.2% | 25.8% | 70.3% | 29.7% | 64.8% | 35.2% | 82.3% | 17.7% | 76.8% | 23.2% | |
| p | 0.924 | 0.068 | 0.636 | 0.016 | 0.675 | 0.079 | |||||||
| Senior | |||||||||||||
| Anxiety | None-mild | 51.0% | 49.0% | 71.1% | 28.9% | 78.0% | 22.0% | 69.5% | 30.5% | 89.1% | 10.9% | 74.9% | 25.1% |
| Mod-severe | 59.5% | 40.5% | 79.3% | 20.7% | 78.0% | 22.0% | 78.4% | 21.6% | 81.9% | 18.1% | 59.5% | 40.5% | |
| p | 0.021 | 0.013 | 0.998 | 0.008 | 0.003 | <0.001 | |||||||
| Depression | None-mild | 51.3% | 48.7% | 71.8% | 28.2% | 78.6% | 21.4% | 70.2% | 29.8% | 88.9% | 11.1% | 74.7% | 25.3% |
| Mod-severe | 59.9% | 40.1% | 77.3% | 22.7% | 74.4% | 25.6% | 76.7% | 23.3% | 81.4% | 18.6% | 57.0% | 43.0% | |
| p | 0.036 | 0.134 | 0.219 | 0.079 | 0.005 | <0.001 | |||||||
| PTSD | None-mild | 49.9% | 50.1% | 72.8% | 27.2% | 78.9% | 21.1% | 69.5% | 30.5% | 89.4% | 10.6% | 77.5% | 22.5% |
| Mod-severe | 57.8% | 42.2% | 71.9% | 28.1% | 76.1% | 23.9% | 74.8% | 25.2% | 84.4% | 15.6% | 60.7% | 39.3% | |
| p | 0.011 | 0.734 | 0.279 | 0.059 | 0.013 | <0.001 | |||||||
| MBI DP | None-low | 50.6% | 49.4% | 72.2% | 27.8% | 79.0% | 21.0% | 68.90% | 31.1% | 89.8% | 10.2% | 77.6% | 22.4% |
| Mod-high | 55.7% | 44.3% | 72.7% | 27.3% | 76.2% | 23.8% | 75.3% | 24.7% | 84.3% | 15.7% | 62.4% | 37.6% | |
| p | 0.094 | 0.849 | 0.253 | 0.019 | 0.005 | <0.001 | |||||||
| MBI EE | None-low | 52.2% | 47.8% | 68.5% | 31.5% | 81.6% | 18.4% | 67.5% | 32.5% | 92.3% | 7.7% | 80.5% | 19.5% |
| Mod-high | 52.6% | 47.4% | 74.9% | 25.1% | 75.8% | 24.2% | 73.5% | 26.5% | 85.1% | 14.9% | 66.9% | 33.1% | |
| p | 0.918 | 0.016 | 0.018 | 0.023 | <0.001 | <0.001 | |||||||
| MBI PA | None-low | 58.3% | 41.7% | 75.2% | 24.8% | 77.9% | 22.1% | 76.2% | 23.8% | 90.2% | 9.8% | 73.3% | 26.7% |
| Mod-high | 50.5% | 49.5% | 71.5% | 28.5% | 78.1% | 21.9% | 69.4% | 30.6% | 87.0% | 13.0% | 71.8% | 28.2% | |
| p | 0.018 | 0.209 | 0.935 | 0.023 | 0.140 | 0.606 | |||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pascoe, A.; Paul, E.; Johnson, D.; Putland, M.; Willis, K.; Smallwood, N. Differences in Coping Strategies and Help-Seeking Behaviours among Australian Junior and Senior Doctors during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 13275. https://doi.org/10.3390/ijerph182413275
Pascoe A, Paul E, Johnson D, Putland M, Willis K, Smallwood N. Differences in Coping Strategies and Help-Seeking Behaviours among Australian Junior and Senior Doctors during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2021; 18(24):13275. https://doi.org/10.3390/ijerph182413275
Chicago/Turabian StylePascoe, Amy, Eldho Paul, Douglas Johnson, Mark Putland, Karen Willis, and Natasha Smallwood. 2021. "Differences in Coping Strategies and Help-Seeking Behaviours among Australian Junior and Senior Doctors during the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 18, no. 24: 13275. https://doi.org/10.3390/ijerph182413275
APA StylePascoe, A., Paul, E., Johnson, D., Putland, M., Willis, K., & Smallwood, N. (2021). Differences in Coping Strategies and Help-Seeking Behaviours among Australian Junior and Senior Doctors during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health, 18(24), 13275. https://doi.org/10.3390/ijerph182413275