
An Association between Lower Extremity Function and Cognitive Frailty: A Sample Population from the KFACS Study

 , ,
, ,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
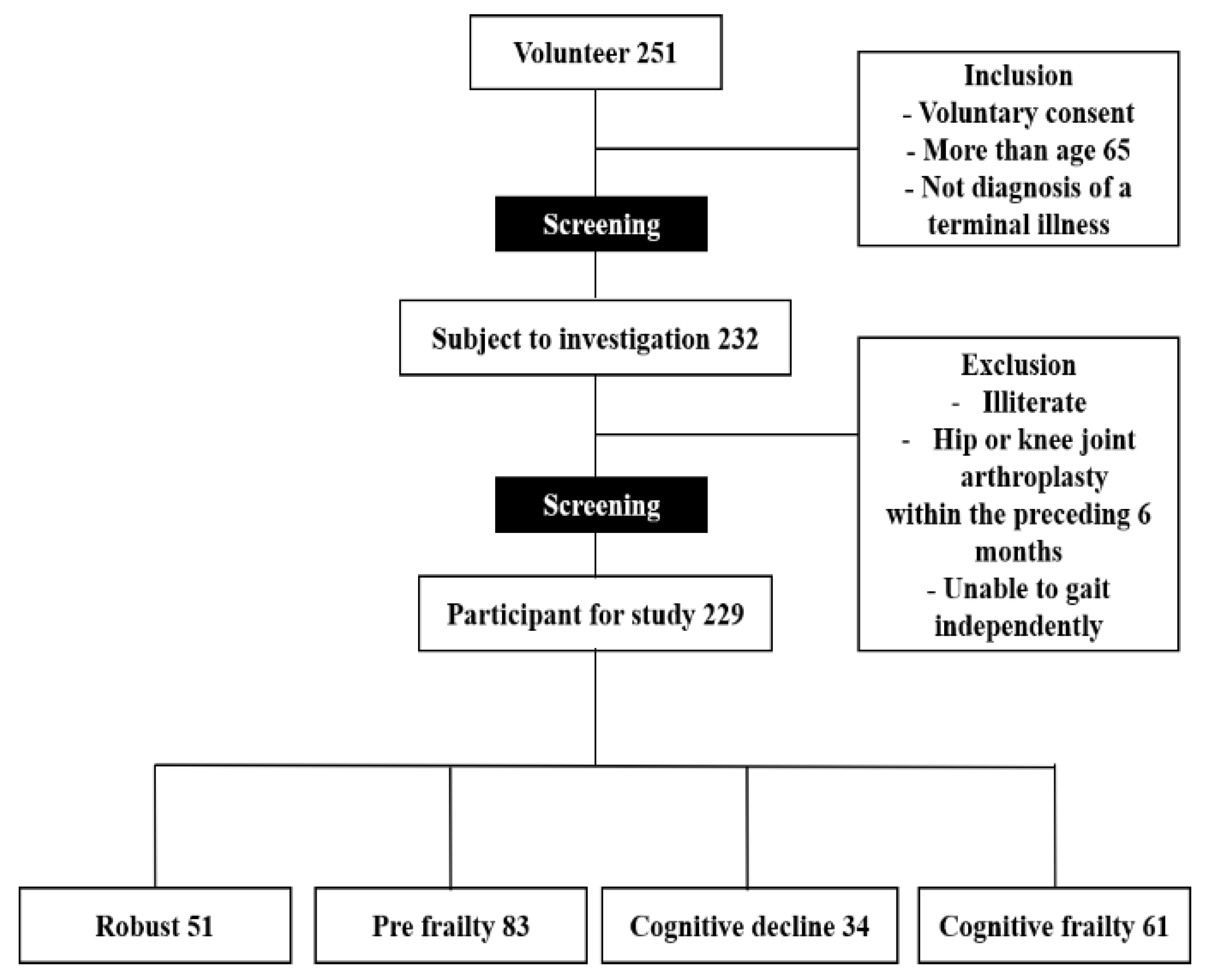
2.1. Participants
2.2. Cognitive Function
2.3. Defined Cognitive Frailty
2.4. Body Composition
2.5. Blood Pressure and Blood Test
2.6. Physical Function
2.7. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Participants
3.2. Comparisons of Physical Function and Blood Biomarkers Using ANOVA Followed by Pairwise Comparisons Using the Bonferroni Test.
3.3. For Multi-Nominal Logistic Regression Models Predicting Cognitive Frailty from Physical Function
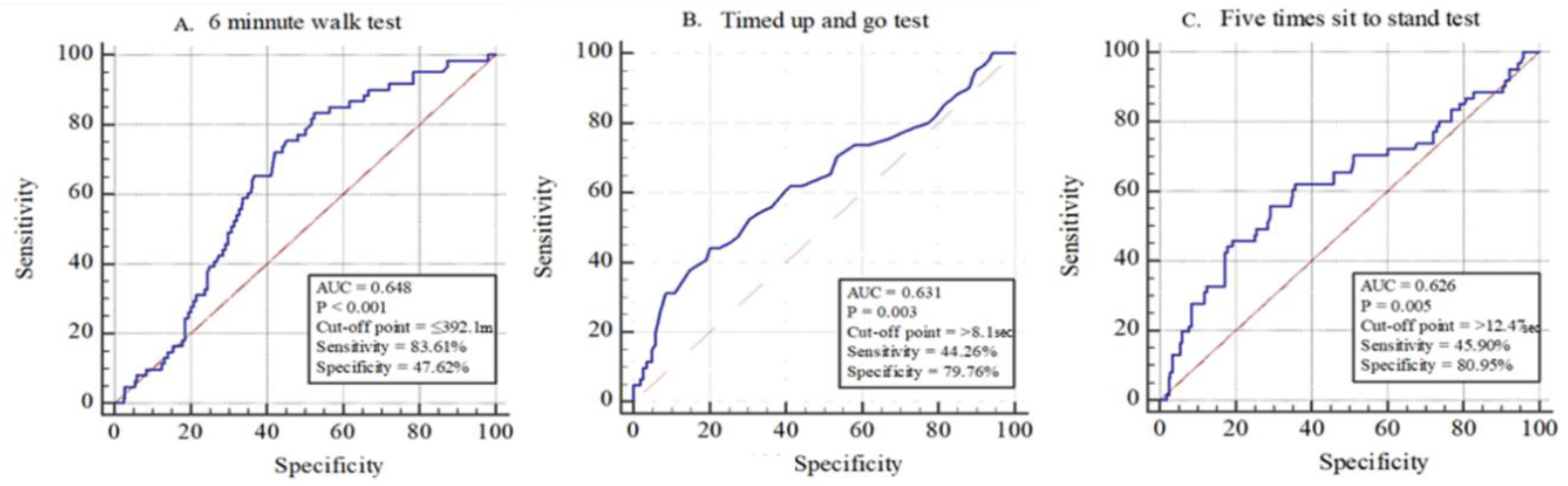
3.4. ROC Curves of 6MWT, TUG Test, and FTSS Test in the Cognitive Frailty Groups
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Morley, J.E.; Vellas, B.; Van Kan, G.A.; Anker, S.D.; Bauer, J.M.; Bernabei, R.; Cesari, M.; Chumlea, W.; Doehner, W.; Evans, J.; et al. Frailty Consensus: A Call to Action. J. Am. Med Dir. Assoc. 2013, 14, 392–397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clegg, A.; Barber, S.; Young, J.; Iliffe, S.; Forster, A. The Home-based Older People’s Exercise (HOPE) trial: A pilot randomised controlled trial of a home-based exercise intervention for older people with frailty. Age Ageing 2014, 43, 687–695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dorner, T.E.; Lackinger, C.; Haider, S.; Luger, E.; Kapan, A.; Luger, M.; Schindler, K.E. Nutritional interven-tion and physical training in malnourished frail community-dwelling elderly persons carried out by trained lay “buddies”: Study protocol of a randomized controlled trial. BMC Public Health 2013, 13, 1232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tavassoli, N.; Guyonnet, S.; Abellan Van Kan, G.; Sourdet, S.; Krams, T.; Soto, M.E.; Subra, J.; Chicoulaa, B.; Ghisolfi, A.; Balardy, L.; et al. Description of 1,108 older patients referred by their physician to the “Geriatric Frailty Clinic (G.F.C) for assessment of frailty and prevention of disability” at the gerontopole. J. Nutr. Health Aging 2014, 18, 457–464. [Google Scholar] [CrossRef] [PubMed]
- Aubertin-Leheudre, M.; Woods, A.J.; Anton, S.; Cohen, R.; Pahor, M. Frailty clinical phenotype: A physical and cognitive point of view. Nestle Nutr. Inst. Workshop Ser. 2015, 83, 55–64. [Google Scholar] [CrossRef] [Green Version]
- Kelaiditi, E.; Cesari, M.; Canevelli, M.; Van Kan, G.A.; Ousset, P.-J.; Gillette-Guyonnet, S.; Ritz, P.; Duveau, F.; Soto, M.E.; Provencher, V.; et al. Cognitive frailty: Rational and definition from an (I.A.N.A./I.A.G.G.) International Consensus Group. J. Nutr. Health Aging 2013, 17, 726–734. [Google Scholar] [CrossRef]
- Sargent, L.; Brown, R. Assessing the current state of cognitive frailty: Measurement properties. J. Nutr. Health Aging 2016, 21, 152–160. [Google Scholar] [CrossRef]
- Ruan, Q.; Yu, Z.; Chen, M.; Bao, Z.; Li, J.; He, W. Cognitive frailty, a novel target for the prevention of elderly dependency. Ageing Res. Rev. 2015, 20, 1–10. [Google Scholar] [CrossRef]
- Roppolo, M.; Mulasso, A.; Rabaglietti, E. Cognitive frailty in Italian community-dwelling older adults: Prevalence rate and its association with disability. J. Nutr. Health Aging 2016, 21, 631–636. [Google Scholar] [CrossRef]
- Shimada, H.; Makizako, H.; Lee, S.; Doi, T.; Tsutsumimoto, K.; Harada, K.; Hotta, R.; Bae, S.; Nakakubo, S.; Suzuki, T. Impact of cognitive frailty on daily activities in older persons. J. Nutr. Health Aging 2016, 20, 729–735. [Google Scholar] [CrossRef]
- Rietman, M.L.; van der A, D.L.; van Oostrom, S.H.; Picavet, H.S.J.; Dollé, M.E.T.; van Steeg, H.; Verschuren, W.M.M.; Spijkerman, A.M.W. The Association between BMI and Different Frailty Domains: A U-Shaped Curve? J. Nutr. Health Aging 2016, 22, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Meuleman, J.R.; Brechue, W.F.; Kubilis, P.S.; Lowenthal, D.T. Exercise training in the debilitated aged: Strength and functional outcomes. Arch. Phys. Med. Rehabil. 2000, 81, 312–318. [Google Scholar] [CrossRef]
- Aggarwal, N.T.; Wilson, R.S.; Beck, T.L.; Bienias, J.L.; Bennett, D.A. Motor Dysfunction in Mild Cognitive Impairment and the Risk of Incident Alzheimer Disease. Arch. Neurol. 2006, 63, 1763–1769. [Google Scholar] [CrossRef] [PubMed]
- Waite, L.; Grayson, D.; Piguet, O.; Creasey, H.; Bennett, H.; Broe, G. Gait slowing as a predictor of incident dementia: 6-year longitudinal data from the Sydney Older Persons Study. J. Neurol. Sci. 2005, 229, 89–93. [Google Scholar] [CrossRef] [PubMed]
- Tabue-Teguo, M.; Simo, N.; Harmand, M.G.-C.; Cesari, M.; Avila-Funes, J.A.; Féart, C.; Amiéva, H.; Dartigues, J.-F. Frailty in elderly: A brief review. Gériatrie Psychologie Neuropsychiatrie Viellissement 2017, 15, 127–137. [Google Scholar] [CrossRef] [PubMed]
- Clouston, S.A.; Brewster, P.; Kuh, D.; Richards, M.; Cooper, R.; Hardy, R.; Rubin, M.S.; Hofer, S.M. The dynamic relationship between physical function and cognition in longitudinal aging cohorts. Epidemiol. Rev. 2013, 35, 33–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mossello, E.; Boncinelli, M. Mini-Mental State Examination: A 30-year story. Aging Clin. Exp. Res. 2006, 18, 271–273. [Google Scholar] [CrossRef]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in Older Adults: Evidence for a Phenotype. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef]
- Pinheiro, P.A.; Passos, T.D.-R.O.; Coqueiro, R.D.S.; Fernandes, M.H.; Barbosa, A.R. [Motor performance of the elderly in northeast Brazil: Differences with age and sex]. Rev. Esc. Enferm. USP 2013, 47, 128–136. [Google Scholar] [CrossRef] [Green Version]
- Burr, J.F.; Bredin, S.S.D.; Faktor, M.D.; Warburton, D.E.R. The 6-Minute Walk Test as a Predictor of Objectively Measured Aerobic Fitness in Healthy Working-Aged Adults. Physician Sportsmed. 2011, 39, 133–139. [Google Scholar] [CrossRef]
- Morley, J.E. Developing novel therapeutic approaches to frailty. Curr. Pharm. Des. 2009, 15, 3384–3395. [Google Scholar] [CrossRef] [PubMed]
- Landi, F.; Russo, A.; Pahor, M.; Capoluongo, E.; Liperoti, R.; Cesari, M.; Bernabei, R.; Onder, G. Serum High-Density Lipoprotein Cholesterol Levels and Mortality in Frail, Community-Living Elderly. Gerontology 2008, 54, 71–78. [Google Scholar] [CrossRef]
- Kim, T.H.; Jhoo, J.H.; Park, J.H.; Kim, J.L.; Ryu, S.H.; Moon, S.W.; Choo, I.H.; Lee, D.W.; Yoon, J.C.; Do, Y.J.; et al. Korean Version of Mini Mental Status Examination for Dementia Screening and Its’ Short Form. Psychiatry Investig. 2010, 7, 102–108. [Google Scholar] [CrossRef] [PubMed]
- Ehrari, H.; Larsen, R.T.; Langberg, H.; Andersen, H.B. Effects of Playful Exercise of Older Adults on Balance and Physical Activity: A Randomized Controlled Trial. J. Popul. Ageing 2020, 13, 207–222. [Google Scholar] [CrossRef] [Green Version]
- Makizako, H.; Shimada, H.; Doi, T.; Tsutsumimoto, K.; Nakakubo, S.; Hotta, R.; Suzuki, T. Predictive Cutoff Values of the Five-Times Sit-to-Stand Test and the Timed “Up & Go” Test for Disability Incidence in Older People Dwelling in the Community. Phys. Ther. 2017, 97, 417–424. [Google Scholar] [CrossRef]
- Park, H.; Na, H.R.; Hiroyuki, S.; Kim, W.K.; Jung, M.K. Combined Intervention of Physical Activity, Aerobic Exercise, and Cognitive Exercise Intervention to Prevent Cognitive Decline for Patients with Mild Cognitive Impairment: A Randomized Controlled Clinical Study. J. Clin. Med. 2019, 8, 940. [Google Scholar] [CrossRef] [Green Version]
- Kadikar, A.; Maurer, J.; Kesten, S. The six-minute walk test: A guide to assessment for lung transplantation. J. Heart Lung Transplant. 1997, 16, 313–319. [Google Scholar] [PubMed]
- Hayashida, I.; Tanimoto, Y.; Takahashi, Y.; Kusabiraki, T.; Tamaki, J. Correlation between Muscle Strength and Muscle Mass, and Their Association with Walking Speed, in Community-Dwelling Elderly Japanese Individuals. PLoS ONE 2014, 9, e111810. [Google Scholar] [CrossRef]
- Lear, S.A.; James, P.T.; Ko, G.T.; Kumanyika, S. Appropriateness of waist circumference and waist-to-hip ratio cutoffs for different ethnic groups. Eur. J. Clin. Nutr. 2009, 64, 42–61. [Google Scholar] [CrossRef] [Green Version]
- Katzmarzyk, P.T.; Bray, G.A.; Greenway, F.L.; Johnson, W.D.; Newton Jr, R.L.; Ravussin, E.; Ryan, D.H.; Bouchard, C. Ethnic-specific BMI and waist circumference thresholds. Obesity (Silver Spring). 2011, 19, 1272–1278. [Google Scholar] [CrossRef] [Green Version]
- Krall, J.R.; Carlson, M.C.; Fried, L.P.; Xue, Q.L. Examining the dynamic, bidirectional associations be-tween cognitive and physical functioning in older adults. Am. J. Epidemiol. 2014, 180, 838–846. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Panza, F.; Lozupone, M.; Solfrizzi, V.; Sardone, R.; Dibello, V.; Di Lena, L.; D’Urso, F.; Stallone, R.; Petruzzi, M.; Giannelli, G. Different cognitive frailty models and health-and cognitive-related outcomes in older age: From epidemiology to prevention. J. Alzheimer’s Dis. 2018, 62, 993–1012. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Canevelli, M.; Cesari, M. Cognitive frailty: What is still missing? J. Nutr. Health Aging 2015, 19, 273–275. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Basic Factor | |
|---|---|
| Female (no, %) | 184 (80.3) |
| Age (year) | 76.76 ± 3.72 |
| Body mass index (kg/m2) | 24.83 ± 3.15 |
| Appendicular skeletal muscle (kg) | 15.40 ± 3.15 |
| Waist-hip ratio (%) | 0.93 ± 0.07 |
| Systolic blood pressure (mmHg) | 138.81 ± 18.00 |
| Diastolic blood pressure (mmHg) | 74.18 ± 11.22 |
| Cognitive function | |
| Mini mental state examination (point) | 24.74 ± 3.54 |
| Physical function | |
| 6 minute walk test (m) | 378.11 ± 63.25 |
| Five times sit to stand test (s) | 10.96 ± 3.60 |
| Timed up and go test (s) | 7.33 ± 1.52 |
| Grip strength (kg) | 22.03 ± 5.74 |
| Gait speed (m/s) | 1.14 ± 0.18 |
| Bio-marker | |
| Total cholesterol (mmol/L) | 4.76 ± 4.76 |
| Triglycerides (mmol/L) | 1.45 ± 0.64 |
| Low density lipoprotein cholesterol (mmol/L) | 3.07 ± 0.91 |
| High density lipoprotein cholesterol (mmol/L) | 1.40 ± 0.35 |
| Glucose (mmol/L) | 2.55 ± 0.46 |
| Insulin (mmol/L) | 8.41 ± 6.01 |
| Creatinine kinase (μkat/L) | 1.74 ± 2.24 |
| Data represent mean ± SD and number, % | |
| Physical Function | A 1 (51) | A 2 (83) | A 3 (34) | A 4 (61) | p | Post-Hoc |
|---|---|---|---|---|---|---|
| 6 min walk test (m) | 397.27 ± 65.11 | 381.77 ± 74.94 | 372.65 ± 47.61 | 360.16 ± 45.52 | 0.02 | A 1 > A 4 |
| Five times sit to stand test(s) | 9.69 ± 2.41 | 10.60 ± 3.63 | 11.84 ± 3.79 | 12.01 ± 3.92 | 0.00 | A 1 < A 3, A 4 |
| Timed up and go test (s) | 6.74 ± 1.10 | 7.10 ± 1.37 | 7.74 ± 1.45 | 7.92 ± 1.80 | 0.00 | A 1 < A 3, A 4; A 2 < A 4 |
| Grip strength (kg) | 22.70 ± 4.59 | 22.68 ± 6.03 | 20.97 ± 4.96 | 21.18 ± 6.49 | 0.24 | - |
| Gait speed (m/s) | 0.87 ± 0.12 | 0.92 ± 0.19 | 0.89 ± 0.11 | 0.91 ± 0.13 | 0.21 | - |
| Biomarker | ||||||
| Total cholesterol (mmol/L) | 4.77 ± 0.99 | 4.75 ± 0.94 | 4.93 ± 1.00 | 4.68 ± 0.86 | 0.63 | - |
| Triglycerides (mmol/L) | 1.37 ± 0.59 | 1.48 ± 63.90 | 1.54 ± 0.62 | 1.43 ± 0.56 | 0.67 | - |
| Low density lipoprotein cholesterol (mmol/L) | 3.07 ± 0.95 | 3.05 ± 0.93 | 3.23 ± 0.98 | 3.01 ± 0.83 | 0.75 | - |
| High density lipoprotein cholesterol (mmol/L) | 1.44 ± 0.33 | 1.39 ± 0.36 | 1.37 ± 0.38 | 1.38 ± 0.36 | 0.77 | - |
| Glucose (mmol/L) | 5.33 ± 0.90 | 5.62 ± 1.10 | 5.60 ± 0.86 | 5.32 ± 0.92 | 0.18 | - |
| Insulin (mmol/L) | 8.10 ± 5.03 | 7.61 ± 5.47 | 10.56 ± 8.02 | 8.56 ± 6.04 | 0.11 | - |
| Creatinine kinase (μkat/L) | 2.23 ± 3.11 | 1.84 ± 2.67 | 1.55 ± 0.96 | 1.31 ± 0.62 | 0.16 | - |
| Robust Model | Adjust Model | |
|---|---|---|
| Timed up and go | odds ratio (CI 95%) | odds ratio (CI 95%) |
| < 6.31 | Ref. | Ref. |
| 6.31–7.10 | 0.748 (0.295–1.897) | 0.772 (0.302–1.972) |
| 7.11–8.20 | 1.080 (0.458–2.546) | 1.120 (0.464–2.703) |
| ≥ 8.21 | 2.790 (1.266–6.151) | 2.897 (1.283–6.541) |
| FTSS | odds ratio (CI 95%) | odds ratio (CI 95%) |
| < 8.69 | Ref. | Ref. |
| 8.69–10.37 | 0.736 (0.293–1.848) | 0.743 (0.296–1.870) |
| 10.38–12.53 | 0.828 (0.336–2.040) | 0.856 (0.345–2.122) |
| ≥ 12.54 | 3.115 (1.390–6.982) | 3.337 (1.451–7.673) |
| 6MWT | odds ratio (CI 95%) | odds ratio (CI 95%) |
| < 340.01 | Ref. | Ref. |
| 340.01–377.80 | 1.604 (0.752–3.422) | 1.587 (0.739–3.410) |
| 377.81–420.00 | 0.491 (0.208–1.156) | 0.450 (0.187–1.080) |
| ≥ 420.01 | 0.241 (0.088–0.662) | 0.204 (0.070–0.591) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, G.-M.; Kim, B.-K.; Kim, D.-R.; Liao, Y.; Park, J.-H.; Park, H. An Association between Lower Extremity Function and Cognitive Frailty: A Sample Population from the KFACS Study. Int. J. Environ. Res. Public Health 2021, 18, 1007. https://doi.org/10.3390/ijerph18031007
Kim G-M, Kim B-K, Kim D-R, Liao Y, Park J-H, Park H. An Association between Lower Extremity Function and Cognitive Frailty: A Sample Population from the KFACS Study. International Journal of Environmental Research and Public Health. 2021; 18(3):1007. https://doi.org/10.3390/ijerph18031007
Chicago/Turabian StyleKim, Gwon-Min, Bo-Kun Kim, Du-Ri Kim, Yung Liao, Jong-Hwan Park, and Hyuntae Park. 2021. "An Association between Lower Extremity Function and Cognitive Frailty: A Sample Population from the KFACS Study" International Journal of Environmental Research and Public Health 18, no. 3: 1007. https://doi.org/10.3390/ijerph18031007
APA StyleKim, G. -M., Kim, B. -K., Kim, D. -R., Liao, Y., Park, J. -H., & Park, H. (2021). An Association between Lower Extremity Function and Cognitive Frailty: A Sample Population from the KFACS Study. International Journal of Environmental Research and Public Health, 18(3), 1007. https://doi.org/10.3390/ijerph18031007