Differences in Characteristics, Hospital Care and Outcomes between Acute Critically Ill Emergency Department Patients with Early and Late Do-Not-Resuscitate Orders

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Study Setting
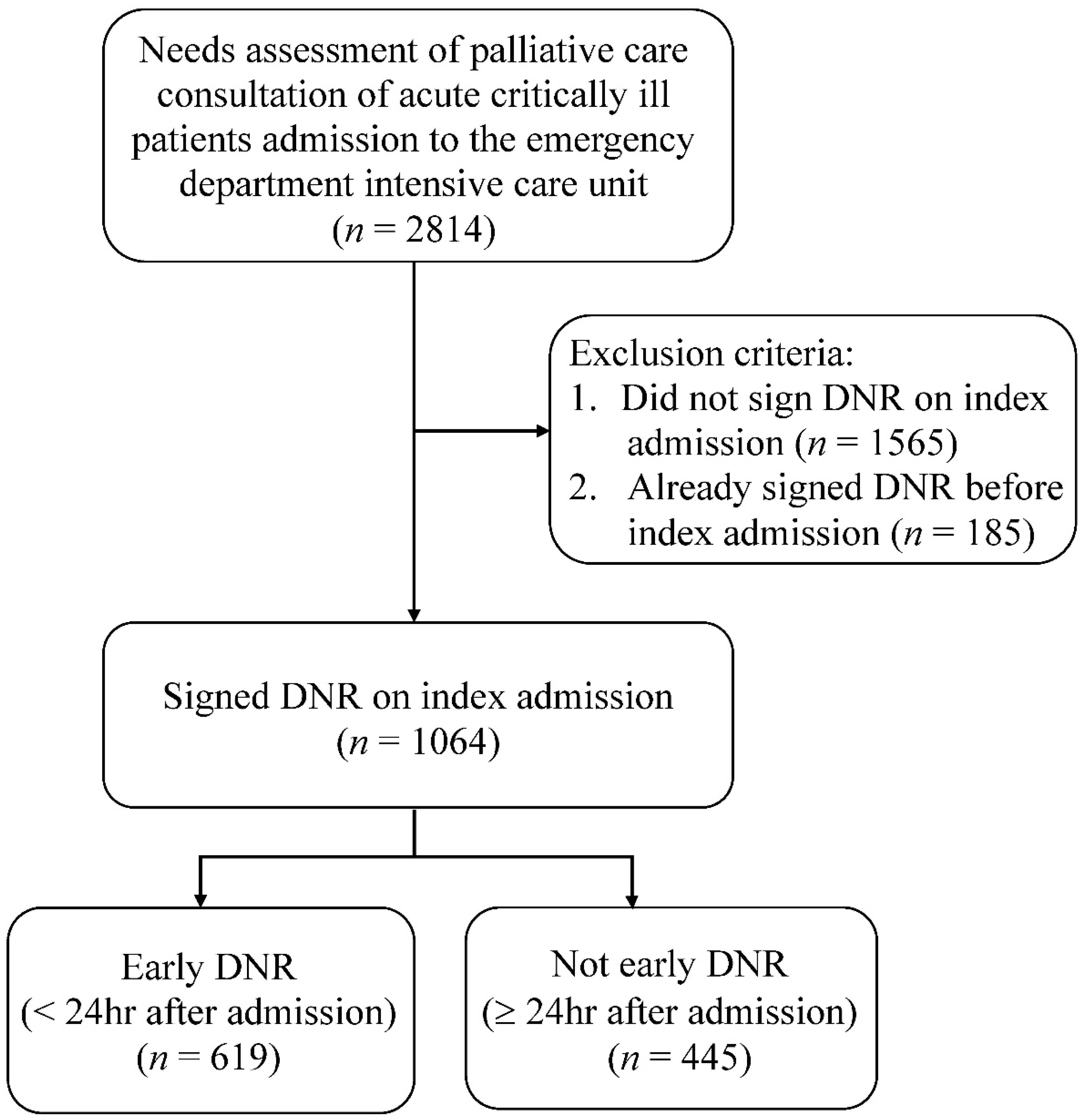
2.3. Patient Population
2.4. Palliative Care Assessment and Data Collection
2.5. Outcome Measures
2.6. Data Analysis
3. Results
4. Discussion
4.1. Characteristics
4.2. Age
4.3. Living in Long-Term Care Facilities
4.4. Advanced Cardiovascular Disease
4.5. Medical Staff Would Not Be Surprised If the Patient Died within 12 Months
4.6. Patients’ Family Requesting Palliative Care
4.7. Hospital Care
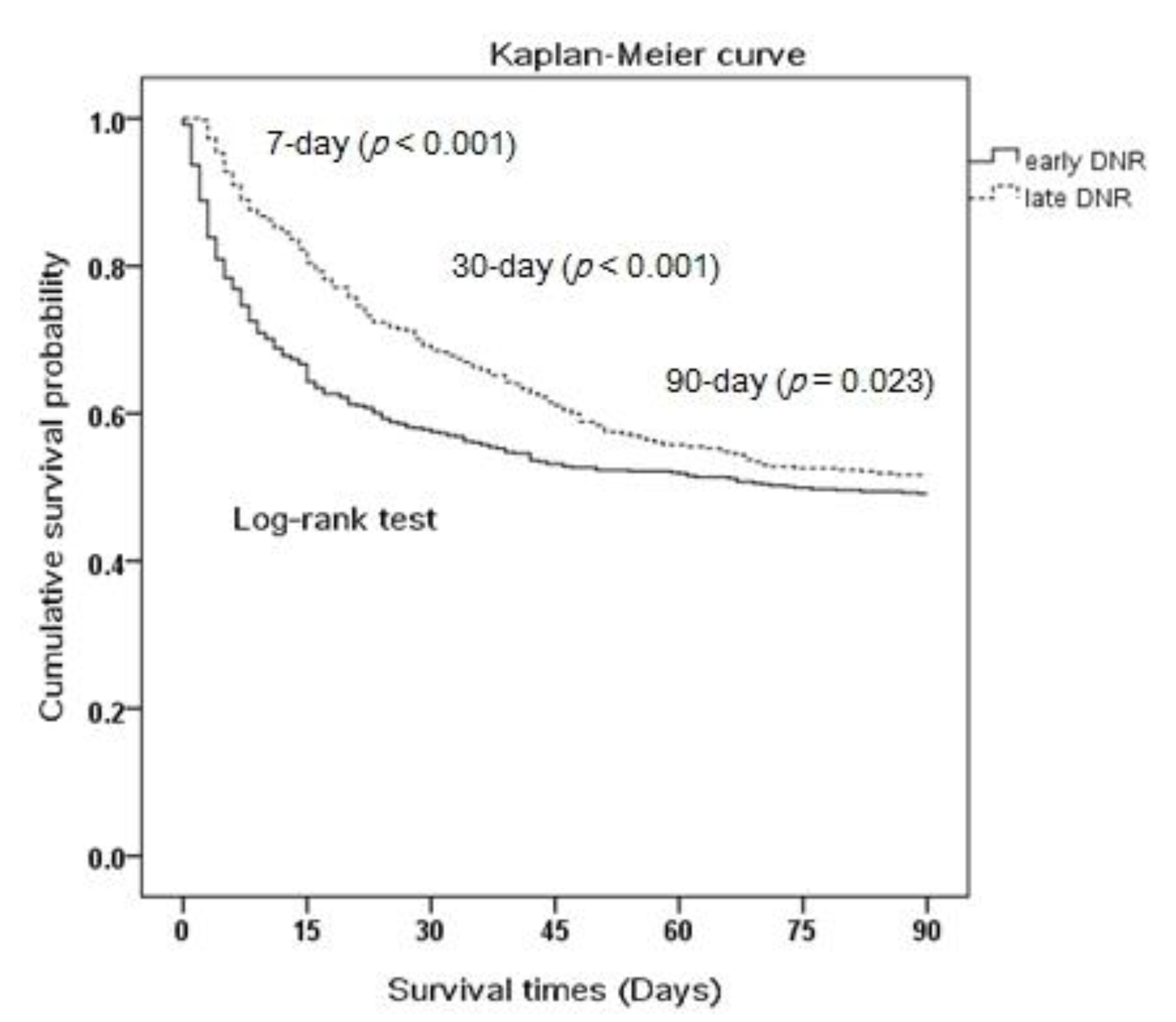
4.8. Survival
4.9. Resource Utilization
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

References
- Rabkin, M.T.; Gillerman, G.; Rice, N.R. Orders not to resuscitate. N. Engl. J. Med. 1976, 295, 364–366. [Google Scholar] [CrossRef] [PubMed]
- Tomlinson, T.; Brody, H. Ethics and communication in do-not-resuscitate orders. N. Engl. J. Med. 1988, 318, 43–46. [Google Scholar] [CrossRef] [PubMed]
- Richardson, D.K.; Zive, D.; Daya, M.; Newgard, C.D. The impact of early do not resuscitate (DNR) orders on patient care and outcomes following resuscitation from out of hospital cardiac arrest. Resuscitation 2013, 84, 483–487. [Google Scholar] [CrossRef] [PubMed]
- Zingmond, D.S.; Wenger, N.S. Regional and institutional variation in the initiation of early do-not-resuscitate orders. Arch. Intern. Med. 2005, 165, 1705–1712. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Auerbach, A.D.; Katz, R.; Pantilat, S.Z.; Bernacki, R.; Schnipper, J.; Kaboli, P.; Wetterneck, T.; Gonzales, D.; Arora, V.; Zhang, J.; et al. Factors associated with discussion of care plans and code status at the time of hospital admission: Results from the multicenter hospitalist study. J. Hosp. Med. 2008, 3, 437–445. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ouyang, D.J.; Lief, L.; Russell, D.; Xu, J.; Berlin, D.A.; Gentzler, E.; Su, A.; Cooper, Z.R.; Senglaub, S.S.; Maciejewski, P.K.; et al. Timing is everything: Early do-not-resuscitate orders in the intensive care unit and patient outcomes. PLoS ONE 2020, 15, e0227971. [Google Scholar] [CrossRef] [Green Version]
- Fuchs, L.; Anstey, M.; Feng, M.; Toledano, R.; Kogan, S.; Howell, M.D.; Clardy, P.; Celi, L.; Talmor, D.; Novack, V. Quantifying the Mortality Impact of Do-Not-Resuscitate Orders in the ICU. Crit. Care Med. 2017, 45, 1019–1027. [Google Scholar] [CrossRef]
- Baldwin, M.R.; Narain, W.R.; Wunsch, H.; Schluger, N.W.; Cooke, J.T.; Maurer, M.S.; Rowe, J.W.; Ledere, D.J.; Bach, P.B. A prognostic model for 6-month mortality in elderly survivors of critical illness. Chest 2013, 143, 910–919. [Google Scholar] [CrossRef] [Green Version]
- Fu, K.H.; Chen, Y.R.; Fan, J.S.; Chen, Y.C.; Huang, H.H.; How, C.K.; Yen, D.H.-T.; Chen, S.-A.; Huang, M.-S. Emergency department critical care unit for critically ill cardiovascular patients: An observation study. J. Chin. Med. Assoc. 2017, 80, 233–244. [Google Scholar] [CrossRef]
- Yang, C.; Yang, T.T.; Tsou, Y.J.; Lin, M.H.; Fan, J.S.; Huang, H.H.; Tsai, M.C.; Yen, D.H. Initiating palliative care consultation for acute critically ill patients in the emergency department intensive care unit. J. Chin. Med. Assoc. 2020, 83, 500–506. [Google Scholar] [CrossRef]
- Chang, Y.C.; Fang, Y.T.; Chen, H.C.; Lin, C.Y.; Chang, Y.P.; Chen, Y.M.; Huang, C.H.; Huang, K.T.; Chang, H.C.; Su, M.C.; et al. Effect of do-not-resuscitate orders on patients with sepsis in the medical intensive care unit: A retrospective, observational and propensity score-matched study in a tertiary referral hospital in Taiwan. BMJ Open 2019, 9, e029041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sinuff, T.; Cook, D.J.; Rocker, G.M.; Griffith, L.E.; Walter, S.D.; Fisher, M.M.; Dodek, P.M.; Sjokvist, P.; McDonald, E.; Marshall, J.C.; et al. Level of Care Study Investigators & the Canadian Critical Care Trials Group. DNR directives are established early in mechanically ventilated intensive care unit patients. Can. J. Anaesth. 2004, 51, 1034–1041. [Google Scholar] [PubMed]
- Cook, D.J.; Guyatt, G.; Rocker, G.; Sjokvist, P.; Weaver, B.; Dodek, P.; Marshall, J.; Leasa, D.; Levy, M.; Varon, J.; et al. Cardiopulmonary resuscitation directives on admission to intensive care unit: An international observational study. Lancet 2001, 358, 1941–1945. [Google Scholar] [CrossRef]
- Al-Dorzi, H.M.; Tamim, H.M.; Mundekkadan, S.; Sohail, M.R.; Arabi, Y.M. Characteristics, management and outcomes of critically ill patients who are 80 years and older: A retrospective comparative cohort study. BMC Anesthesiol. 2014, 14, 126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharp, T.; Moran, E.; Kuhn, I.; Barclay, S. Do the elderly have a voice? Advance care planning discussions with frail and older individuals: A systematic literature review and narrative synthesis. Br. J. Gen. Pract. 2013, 63, e657–e668. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Egelund, G.B.; Jensen, A.V.; Petersen, P.T.; Andersen, S.B.; Lindhardt, B.Ø.; Rohde, G.; Ravn, P.; von Plessen, C. Do-not-resuscitate orders in patients with community-acquired pneumonia: A retrospective study. BMC Pulm. Med. 2020, 20, 201. [Google Scholar] [CrossRef]
- Marrie, T.J.; Fine, M.J.; Kapoor, W.N.; Coley, C.M.; Singer, D.E.; Obrosky, D.S. Community-acquired pneumonia and do not resuscitate orders. J. Am. Geriatr. Soc. 2002, 50, 290–299. [Google Scholar] [CrossRef]
- Lo, Y.T.; Wang, J.J.; Liu, L.F.; Wang, C.N. Prevalence and related factors of do-not-resuscitate directives among nursing home residents in Taiwan. J. Am. Med. Dir. Assoc. 2010, 11, 436–442. [Google Scholar] [CrossRef]
- Abbo, E.D.; Yuen, T.C.; Buhrmester, L.; Geocadin, R.; Volandes, A.E.; Siddique, J.; Edelson, D.P. Cardiopulmonary resuscitation outcomes in hospitalized community-dwelling individuals and nursing home residents based on activities of daily living. J. Am. Geriatr. Soc. 2013, 61, 34–39. [Google Scholar] [CrossRef]
- Dunlay, S.M.; Redfield, M.M.; Weston, S.A.; Therneau, T.M.; Hall Long, K.; Shah, N.D.; Roger, V.L. Hospitalizations after heart failure diagnosis a community perspective. J. Am. Coll. Cardiol. 2009, 54, 1695–1702. [Google Scholar] [CrossRef] [Green Version]
- Allen, L.A.; Stevenson, L.W.; Grady, K.L.; Goldstein, N.E.; Matlock, D.D.; Arnold, R.M.; Cook, N.R.; Felker, G.M.; Francis, G.S.; Hauptman, P.J.; et al. American Heart Association; Council on Quality of Care and Outcomes Research; Council on Cardiovascular Nursing; Council on Clinical Cardiology; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular Surgery and Anesthesia. Decision making in advanced heart failure: A scientific statement from the American Heart Association. Circulation 2012, 125, 1928–1952. [Google Scholar] [PubMed]
- Dunlay, S.M.; Swetz, K.M.; Redfield, M.M.; Mueller, P.S.; Roger, V.L. Resuscitation preferences in community patients with heart failure. Circ. Cardiovasc. Qual. Outcomes 2014, 7, 353–359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allen, L.A.; Yager, J.E.; Funk, M.J.; Levy, W.C.; Tulsky, J.A.; Bowers, M.T.; Dodson, G.C.; O’Connor, C.M.; Felker, G.M. Discordance between patient-predicted and model-predicted life expectancy among ambulatory patients with heart failure. JAMA 2008, 299, 2533–2542. [Google Scholar] [CrossRef] [PubMed]
- Agård, A.; Hermerén, G.; Herlitz, J. Should cardiopulmonary resuscitation be performed on patients with heart failure? The role of the patient in the decision-making process. J. Intern. Med. 2000, 248, 279–286. [Google Scholar] [CrossRef] [Green Version]
- Raymont, V.; Bingley, W.; Buchanan, A.; David, A.S.; Hayward, P.; Wessely, S.; Hotopf, M. Prevalence of mental incapacity in medical inpatients and associated risk factors: Cross-sectional study. Lancet 2004, 364, 1421–1427. [Google Scholar] [CrossRef]
- Levin, T.T.; Li, Y.; Weiner, J.S.; Lewis, F.; Bartell, A.; Piercy, J.; Kissane, D.W. How do-not-resuscitate orders are utilized in cancer patients:Timing relative to death and communication-training implications. Palliat. Support Care 2008, 6, 341–348. [Google Scholar] [CrossRef] [Green Version]
- Fu, P.K.; Yang, M.C.; Wang, C.Y.; Lin, S.P.; Kuo, C.T.; Hsu, C.Y.; Tung, Y.C. Early Do-Not-Resuscitate Directives Decrease Invasive Procedures and Health Care Expenses during the Final Hospitalization of Life of COPD Patients. J. Pain Symptom Manag. 2019, 58, 968–976. [Google Scholar] [CrossRef]
- Loggers, E.T.; Maciejewski, P.K.; Jimenez, R.; Nilsson, M.; Paulk, E.; Stieglitz, H.; Prigerson, H.G. Predictors of intensive end-of-life and hospice care in Latino and white advanced cancer patients. J. Palliat. Med. 2013, 16, 1249–1254. [Google Scholar] [CrossRef] [Green Version]
- Detering, K.M.; Hancock, A.D.; Reade, M.C.; Silvester, W. The impact of advance care planning on end of lifecare in elderly patients: Randomised controlled trial. BMJ 2010, 340, c1345. [Google Scholar] [CrossRef] [Green Version]
- Claude Hemphill, J., III; Newman, J.; Zhao, S.; Johnston, S.C. Hospital usage of early do-not-resuscitate orders and outcome after intracerebral hemorrhage. Stroke 2004, 35, 1130–1134. [Google Scholar] [CrossRef] [Green Version]
- Becker, K.J.; Baxter, A.B.; Cohen, W.A.; Bybee, H.M.; Tirschwell, D.L.; Newell, D.W.; Winn, H.R.; Longstreth, W.T., Jr. Withdrawal of support in intracerebral hemorrhage may lead to selffulfilling prophecies. Neurology 2001, 56, 766–772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Torke, A.M.; Sachs, G.A.; Helft, P.R.; Petronio, S.; Purnell, C.; Hui, S.; Callahan, C.M. Timing of do-not-resuscitate orders for hospitalized older adults who require a surrogate decision-maker. J. Am. Geriatr. Soc. 2011, 59, 1326–1331. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
| Items | Overall n = 1064 (%) | Early DNR n = 619 (%) | Late DNR n = 445 (%) | p-Value |
|---|---|---|---|---|
| A. Acute critical and life-limiting illness | ||||
| 1. Advanced cancer, metastatic or locally aggressive disease | 204 (19.2) | 123 (19.9) | 81 (18.2) | 0.495 |
| 2. Advanced COPD who needs long-term oxygen therapy or respiratory failure requiring assisted ventilation | 11 (1.0) | 7 (1.1) | 4 (0.9) | 0.712 |
| 3. End-stage liver disease, e.g., cirrhosis, that repeatedly appears with jaundice, ascites, peritonitis, hepatic coma, esophageal varices | 20 (1.9) | 14 (2.3) | 6 (1.3) | 0.279 |
| 4. Acute or chronic renal failure, decision of not receiving dialysis | 26 (2.4) | 19 (3.1) | 7 (1.6) | 0.119 |
| 5. Advanced cardiovascular diseases (chronic heart failure NYHA III or IV, chest pain, or dyspnea while in minimal exercise or exertion, or devastating inoperable peripheral vascular diseases) * | 60 (5.6) | 48 (7.8) | 12 (2.7) | <0.001 |
| 6. Advanced central neurological diseases (e.g., stroke, dementia) in long-term bed-bound, combined with repeatedly or severely progressive deterioration or recurrent pneumonia, shortness of breath, or respiratory failure requiring hospital admission * | 295 (27.7) | 202 (32.6) | 93 (20.9) | <0.001 |
| 7. Septic shock, ARDS, multiple organ failure, or impending death (other devastating diseases) * | 343 (32.2) | 231 (37.3) | 112 (25.2) | <0.001 |
| 8. Very severely frail (completely dependent, approaching the end-of-life, CSHA-CFS > scale 8 and 9) * | 61 (5.7) | 49 (7.9) | 12 (2.7) | <0.001 |
| B. The unmet palliative care needs | ||||
| 1. Medical care staffs would not be surprised if the patient died within 12 months of this episode (surprise question) * | 544 (51.1) | 374 (60.4) | 170 (38.2) | <0.001 |
| 2. Appearing progressive functional deterioration with ≥3 ADLs needing for assistance | 363 (34.1) | 226 (36.5) | 137 (30.8) | 0.052 |
| 3. Appearing biopsychosocial discomforts needing hospital admission * | 368 (34.6) | 247 (39.9) | 121 (27.2) | <0.001 |
| 4. Patients with three or more unexpected emergency department visits or hospital admissions within 6 months, with symptoms consistent with a terminal or degenerative chronic medical condition * | 235 (22.1) | 159 (25.7) | 76 (17.1) | 0.001 |
| 5. Patients Weight loss 10% or BMI ≤ 18 within 6 months | 10 (0.9) | 8 (1.3) | 2 (0.4) | 0.160 |
| 6. Bed-bound patients with long-term unhealed bed sore or ulceration * | 54 (5.1) | 39 (6.3) | 15 (3.4) | 0.032 |
| 7. Needing complicated medical care and assistance of medical decisions, including do-not-resuscitate order, ventilator, or nutritional supports * | 632 (59.4) | 424 (68.5) | 208 (46.7) | <0.001 |
| 8. Patient’s family request of palliative care * | 53 (5.0) | 41 (6.6) | 12 (2.7) | 0.004 |
| Variable | Overall | Early DNR | Late DNR | p-Value |
|---|---|---|---|---|
| n = 1064 (%) | n = 619 (%) | n = 445 (%) | ||
| Age, year * | 80.8 ± 14.2 | 83.3 ± 12.8 | 77.3 ± 15.4 | <0.001 |
| <65 | 157 (14.8) | 73 (11.8) | 84 (18.9) | |
| 65–75 | 137 (12.9) | 54 (8.7) | 83 (18.7) | |
| 75–85 | 219 (20.6) | 122 (19.7) | 97 (21.8) | |
| >85 | 551 (51.8) | 370 (59.8) | 181 (40.7) | |
| Female sex | 399 (37.5) | 234 (37.8) | 165 (37.1) | 0.81 |
| Insurance status * | 0.003 | |||
| National health insurance only | 621 (58.4) | 338 (54.6) | 283 (63.6) | |
| With Medicaid | 443 (41.6) | 281 (45.4) | 162 (36.4) | |
| Living conditions * | 0.035 | |||
| With family | 860 (81.0) | 484 (78.2) | 376 (84.9) | |
| Veterans home | 37 (3.5) | 27 (4.4) | 10 (2.3) | |
| Long-term care facilities | 74 (7.0) | 53 (8.6) | 21 (4.7) | |
| Solitary living | 70 (6.6) | 42 (6.8) | 28 (6.3) | |
| Others | 21 (2.0) | 13 (2.1) | 8 (1.8) | |
| Marital status | 0.287 | |||
| Single | 93 (8.8) | 54 (8.7) | 39 (8.8) | |
| Married | 642 (60.6) | 363 (58.7) | 279 (63.3) | |
| Divorced | 37 (3.5) | 20 (3.2) | 17 (3.9) | |
| Widow or widower | 387 (27.1) | 181 (29.3) | 106 (24.0) | |
| Religion | 0.478 | |||
| Taoism | 189 (17.8) | 108 (17.4) | 81 (18.3) | |
| Buddhism | 355 (33.5) | 205 (33.1) | 150 (33.9) | |
| Catholic/Christian | 97 (9.1) | 53 (8.6) | 44 (10.0) | |
| Others | 11 (1.0) | 9 (1.5) | 2 (0.5) | |
| None | 409 (38.5) | 244 (39.4) | 165 (37.3) | |
| Educational level | 0.055 | |||
| Higher than high school | 444 (42.0) | 244 (39.5) | 200 (45.5) | |
| Lower than high school | 613 (58.0) | 373 (60.5) | 240 (54.5) | |
| Current alcohol consumption | 18 (1.7) | 11 (1.8) | 7 (1.6) | 0.796 |
| Current smoker * | 69 (6.5) | 32 (5.2) | 37 (8.3) | 0.041 |
| TTAS * | 0.004 | |||
| Emergent (triage 1) | 404 (38.1) | 258 (41.9) | 146 (32.9) | |
| Urgent (triage 2) | 371 (35.0) | 212 (34.4) | 159 (35.8) | |
| Non-urgent (triage 3, 4) | 285 (26.9) | 146 (23.7) | 139 (31.3) | |
| Glasgow Coma Scale * | 10.8 ± 4.5 | 10.4 ± 4.6 | 11.4 ± 4.2 | <0.001 |
| 13–15 | 536 (50.4) | 291 (47.0) | 245 (55.1) | |
| 5–12 | 366 (34.4) | 214 (34.6) | 152 (34.2) | |
| 3–4 | 162 (15.2) | 114 (18.4) | 48 (10.8) | |
| Mean blood pressure in the emergency department (ED) (mmHg) | 91.1 ± 24.2 | 90.6 ± 24.3 | 91.9 ± 24.0 | 0.369 |
| Charlson Comorbidity Index | 6.7 ± 2.5 | 6.8 ± 2.3 | 6.6 ± 2.7 | 0.414 |
| ≤3 | 59 (5.5) | 20 (3.2) | 39 (8.8) | |
| 4–6 | 496 (46.6) | 298 (48.1) | 198 (44.5) | |
| ≥7 | 509 (47.8) | 301 (48.6) | 208 (46.7) | |
| APACHE II score at admission * | 21.8 ± 8.4 | 22.7 ± 8.4 | 20.6 ± 8.2 | <0.001 |
| 0–14 | 204 (19.2) | 101 (16.3) | 103 (23.1) | |
| 15–24 | 486 (45.7) | 277 (44.7) | 209 (47.0) | |
| >24 | 374 (35.2) | 241 (38.9) | 133 (29.9) | |
| Hospital length of stay (day) * | 23.1 ± 25.6 | 17.8 ± 18.4 | 30.3 ± 31.7 | <0.001 |
| Total hospital expense (point) * | 339,468 ± 384,772 | 246,684 ± 266,447 | 468,532 ± 476,382 | <0.001 |
| Inhospital mortality | 480 (45.1) | 282 (45.6) | 198 (44.5) | 0.731 |
| Variable | Univariate Analysis | Multiple Logistic Regression | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p | AOR | 95% CI | p | |
| Age, year | ||||||
| <65 | 1 | 1 | ||||
| 65–75 | 0.749 | (0.470–1.191) | 0.222 | 0.677 | (0.399–1.151) | 0.15 |
| 75–85 | 1.447 | (0.959–2.184) | 0.078 | 1.201 | (0.725–1.992) | 0.477 |
| >85 | 2.352 | (1.640–3.373) | <0.001 | 1.7 | (1.027–2.814) | 0.039 * |
| Insurance status | ||||||
| National health insurance only | 1 | 1 | 1 | |||
| With Medicaid | 1.452 | (1.131–1.864) | 0.003 | 0.988 | (0.729–1.340) | 0.939 |
| Living conditions | ||||||
| With family | 1 | 1 | 1 | |||
| Veterans home | 2.098 | (1.003–4.108) | 0.046 | 1.707 | (0.753–3.866) | 0.2 |
| Long-term care facilities | 1.961 | (1.162–3.308) | 0.012 | 1.88 | (1.066–3.319) | 0.029 * |
| Solitary living | 1.165 | (0.709–1.915) | 0.546 | 1.544 | (0.896–2.659) | 0.118 |
| Others | 1.262 | (0.518–3.077) | 0.608 | 1.533 | (0.591–3.982) | 0.38 |
| Smoker | ||||||
| No smoking/quit smoking | 1 | 1 | ||||
| Current smoker | 0.602 | (0.369–0.983) | 0.042 | 0.848 | (0.497–1.447) | 0.545 |
| TTAS | ||||||
| Non-urgent | 1 | 1 | ||||
| Urgent | 1.269 | (0.931–1.731) | 0.132 | 1.162 | (0.830–1.628) | 0.382 |
| Emergent | 1.682 | (1.236–2.290) | 0.001 | 1.413 | (1.005–1.985) | 0.046 |
| Glasgow Coma Scale | ||||||
| 13–15 | 1 | 1 | ||||
| 5–12 | 1.185 | (0.906–1.550) | 0.215 | 0.816 | (0.590–1.128) | 0.218 |
| 3–4 | 2 | (1.371–2.917) | <0.001 | 1.434 | (0.924–2.226) | 0.108 |
| Charlson Comorbidity Index | ||||||
| ≤3 | 1 | 1 | ||||
| 4–6 | 2.935 | (1.663–5.180) | <0.001 | 1.53 | (0.780–3.000) | 0.216 |
| ≥7 | 2.822 | (1.600–4.976) | <0.001 | 1.44 | (0.732–2.832) | 0.291 |
| APACHE II score at admission | ||||||
| 0–14 | 1 | 1 | ||||
| 15–24 | 1.352 | (0.974–1.876) | 0.072 | 1.042 | (0.713–1.524) | 0.83 |
| >24 | 1.848 | (1.307–2.613) | 0.001 | 1.167 | (0.758–1.798) | 0.483 |
| palliative care consultation screening items | ||||||
| A5 | 3.033 | (1.592–5.780) | 0.001 | 2.128 | (1.039–4.358) | 0.039 * |
| A6 | 1.833 | (1.381–2.435) | <0.001 | 0.955 | (0.659–1.383) | 0.807 |
| A7 | 1.77 | (1.353–2.317) | <0.001 | 0.956 | (0.673–1.357) | 0.8 |
| A8 | 3.102 | (1.630–5.903) | 0.001 | 1.674 | (0.839–3.342) | 0.144 |
| B1 | 2.469 | (1.923–3.171) | <0.001 | 1.725 | (1.193–2.496) | 0.004 * |
| B3 | 1.778 | (1.366–2.314) | <0.001 | 1.181 | (0.844–1.652) | 0.331 |
| B4 | 1.678 | (1.236–2.278) | 0.001 | 1.127 | (0.791–1.606) | 0.508 |
| B6 | 1.928 | (1.049–3.542) | 0.035 | 1.194 | (0.615–2.317) | 0.601 |
| B7 | 2.478 | (1.926–3.187) | <0.001 | 1.279 | (0.815–2.007) | 0.284 |
| B8 | 2.56 | (1.329–4.929) | 0.005 | 2.42 | (1.187–4.935) | 0.015 * |
| Variable | Early DNR Patients with Mortality | Late DNR Patients with Mortality | p |
|---|---|---|---|
| n = 282 (%) | n = 198 (%) | ||
| Place of death | 0.446 | ||
| Intensive care unit | 109 (38.7) | 73 (36.9) | |
| Wards | 108 (38.3) | 89 (44.9) | |
| Hospice unit | 31 (11.0) | 17 (8.6) | |
| Critical against advice discharge | 34 (12.1) | 19 (9.6) | |
| End-of-life care | |||
| ET intubation * | 44 (15.6) | 79 (39.9) | <0.001 |
| CPR | 12 (4.3) | 16 (8.1) | 0.078 |
| Epinephrine * | 56 (19.9) | 60 (30.3) | 0.009 |
| Cardioversion or defibrillation | 7 (2.5) | 5 (2.5) | 0.976 |
| Vasopressors | 183 (64.9) | 138 (69.7) | 0.271 |
| Cardiac pacemaker | 3 (1.1) | 1 (0.5) | 0.507 |
| Ventilator support * | 47 (16.7) | 75 (37.9) | <0.001 |
| ECMO or IABP | 1 (0.4) | 4 (2.0) | 0.077 |
| Withdrawal of ET tube | 11 (3.9) | 10 (5.1) | 0.544 |
| Narcotics use * | 144 (51.1) | 124 (62.6) | 0.012 |
| Variable | Univariate Analysis | Multiple Logistic Regression | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p | AOR | 95% CI | p | |
| ET intubation * | 0.278 | (0.181–0.428) | <0.001 | 0.198 | (0.061–0.643) | 0.007 |
| Epinephrine | 0.570 | (0.374–0.868) | 0.009 | 0.639 | (0.404–1.010) | 0.055 |
| Ventilator support | 0.328 | (0.214–0.502) | <0.001 | 1.460 | (0.449–4.752) | 0.529 |
| Narcotics use * | 0.623 | (0.430–0.902) | 0.012 | 0.518 | (0.347–0.772) | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, J.C.-Y.; Yang, C.; Lai, L.-L.; Chen, Y.-J.; Huang, H.-H.; Fan, J.-S.; Hsu, T.-F.; Yen, D.H.-T. Differences in Characteristics, Hospital Care and Outcomes between Acute Critically Ill Emergency Department Patients with Early and Late Do-Not-Resuscitate Orders. Int. J. Environ. Res. Public Health 2021, 18, 1028. https://doi.org/10.3390/ijerph18031028
Chang JC-Y, Yang C, Lai L-L, Chen Y-J, Huang H-H, Fan J-S, Hsu T-F, Yen DH-T. Differences in Characteristics, Hospital Care and Outcomes between Acute Critically Ill Emergency Department Patients with Early and Late Do-Not-Resuscitate Orders. International Journal of Environmental Research and Public Health. 2021; 18(3):1028. https://doi.org/10.3390/ijerph18031028
Chicago/Turabian StyleChang, Julia Chia-Yu, Che Yang, Li-Ling Lai, Ying-Ju Chen, Hsien-Hao Huang, Ju-Sing Fan, Teh-Fu Hsu, and David Hung-Tsang Yen. 2021. "Differences in Characteristics, Hospital Care and Outcomes between Acute Critically Ill Emergency Department Patients with Early and Late Do-Not-Resuscitate Orders" International Journal of Environmental Research and Public Health 18, no. 3: 1028. https://doi.org/10.3390/ijerph18031028
APA StyleChang, J. C. -Y., Yang, C., Lai, L. -L., Chen, Y. -J., Huang, H. -H., Fan, J. -S., Hsu, T. -F., & Yen, D. H. -T. (2021). Differences in Characteristics, Hospital Care and Outcomes between Acute Critically Ill Emergency Department Patients with Early and Late Do-Not-Resuscitate Orders. International Journal of Environmental Research and Public Health, 18(3), 1028. https://doi.org/10.3390/ijerph18031028