
Risk Factors of Undiagnosed Diabetes Mellitus among Korean Adults: A National Cross-Sectional Study Using the KNHANES Data

 , , , , ,
, , , , , 
Abstract
:1. Introduction
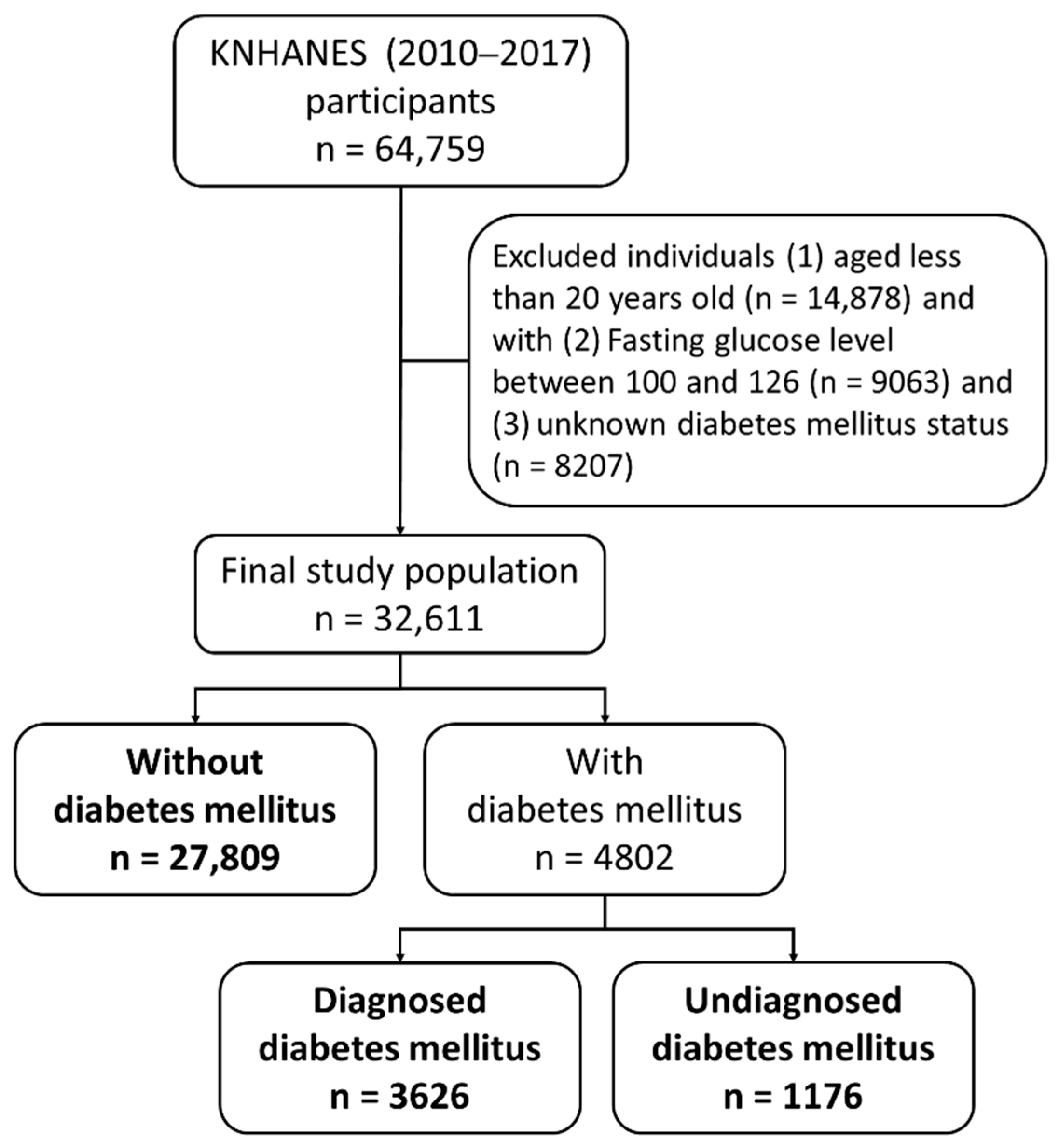
2. Materials and Methods
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cho, N.H.; Shaw, J.E.; Karuranga, S.; Huang, Y.; da Rocha Fernandes, J.D.; Ohlrogge, A.W.; Malanda, B. IDF Diabetes Atlas: Global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res. Clin. Pract. 2018, 138, 271–281. [Google Scholar] [CrossRef] [PubMed]
- Bommer, C.; Sagalova, V.; Heesemann, E.; Manne-Goehler, J.; Atun, R.; Bärnighausen, T.; Davies, J.; Vollmer, S. Global economic burden of diabetes in adults: Projections from 2015 to 2030. Diabetes Care 2018, 41, 963–970. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.; Kang, H.T.; Lim, H.J.; Park, B. Trends in diabetes prevalence among Korean adults based on Korean National Health and Nutrition Examination Surveys III–VI. Diabetes Res. Clin. Pract. 2018, 138, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Beagley, J.; Guariguata, L.; Weil, C.; Motala, A.A. Global estimates of undiagnosed diabetes in adults. Diabetes Res. Clin. Pract. 2014, 103, 150–160. [Google Scholar] [CrossRef] [PubMed]
- Baena-Díez, J.M.; Peñafiel, J.; Subirana, I.; Ramos, R.; Elosua, R.; Marín-Ibañez, A.; Guembe, M.J.; Rigo, F.L.; Tormo-Diaz, J.; Moreno-Iribas, C.; et al. Risk of cause-specific death in individuals with diabetes: A competing risks analysis. Diabetes Care 2016, 39, 1987–1995. [Google Scholar]
- Fowler, M.J. Microvascular and macrovascular complications of diabetes. Clin. Diabetes 2008, 26, 6. [Google Scholar] [CrossRef] [Green Version]
- Kweon, S.; Kim, Y.; Jang, M.J.; Kim, Y.; Kim, K.; Choi, S.; Chun, C.; Khang, Y.H.; Oh, K. Data resource profile: The Korea National Health and Nutrition Examination Survey (KNHANES). Int. J. Epidemiol. 2014, 43, 69–77. [Google Scholar] [CrossRef] [Green Version]
- Rosella, L.C.; Lebenbaum, M.; Fitzpatrick, T.; Zuk, A.; Booth, G.L. Prevalence of prediabetes and undiagnosed diabetes in canada (2007–2011) according to fasting plasma glucose and HbA 1c screening criteria. Diabetes Care 2015, 38, 1299–1305. [Google Scholar] [CrossRef] [Green Version]
- Choi, Y.J.; Kim, H.C.; Kim, H.M.; Park, S.W.; Kim, J.; Kim, D.J. Prevalence and management of diabetes in Korean adults: Korea National Health and Nutrition Examination Surveys 1998–2005. Diabetes Care 2009, 32, 2016–2020. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.H.; Bang, H.; Kim, H.C.; Kim, H.M.; Park, S.W.; Kim, D.J. A Simple screening score for diabetes for the Korean population: Development, validation, and comparison with other scores. Diabetes Care 2012, 35, 1723–1730. [Google Scholar] [CrossRef] [Green Version]
- Mendola, N.D.; Eberhardt, M.S. Prevalence of total, diagnosed, and undiagnosed diabetes among adults: United States, 2013–2016. NCHS Data Brief 2018, 319, 1–8. [Google Scholar]
- Saeedi, P.; Petersohn, I.; Salpea, P.; Malanda, B.; Karuranga, S.; Unwin, N.; Colagiuri, S.; Guariguata, L.; Motala, A.A.; Ogurtsova, K.; et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res. Clin. Pract. 2019, 157, 107843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Min, H.; Chang, J.; Balkrishnan, R. Sociodemographic risk factors of diabetes and hypertension prevalence in Republic of Korea. Int. J. Hypertens. 2010, 2010, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, D.S.; Kim, Y.J.; Han, H.R. Sex differences in the association between socio-economic status and type 2 diabetes: Data from the 2005 Korean National Health and Nutritional Examination Survey (KNHANES). Public Health 2013, 127, 554–560. [Google Scholar] [CrossRef]
- Bantie, G.M.; Wondaye, A.A.; Arike, E.B.; Melaku, M.T.; Ejigu, S.T.; Lule, A.; Lingerew, W.L.; Tamirat, K.S. Prevalence of undiagnosed diabetes mellitus and associated factors among adult residents of Bahir Dar city, northwest Ethiopia: A community-based cross-sectional study. BMJ Open 2019, 9, e030158. [Google Scholar] [CrossRef] [Green Version]
- Hwang, J.; Shon, C. Relationship between socioeconomic status and type 2 diabetes: Results from Korea National Health and Nutrition Examination Survey (KNHANES) 2010–2012. BMJ Open 2014, 4, e005710. [Google Scholar] [CrossRef] [Green Version]
- Holt, R.I.G.; Phillips, D.I.W.; Jameson, K.A.; Cooper, C.; Dennison, E.M.; Peveler, R.C. The relationship between depression and diabetes mellitus: Findings from the Hertfordshire Cohort Study. Diabet. Med. 2009, 26, 641–648. [Google Scholar] [CrossRef]
- Lee, T.C.; Glynn, R.J.; Peña, J.M.; Paynter, N.P.; Conen, D.; Ridker, P.M.; Pradhan, A.D.; Albert, M.A. Socioeconomic status and incident type 2 diabetes mellitus: Data from the women’s health study. PLoS ONE 2011, 6, e27670. [Google Scholar] [CrossRef]
- Chamarthi, B.; Williams, G.H.; Ricchiuti, V.; Srikumar, N.; Hopkins, P.N.; Luther, J.M.; Jeynemaitre, X.; Thomas, A. Inflammation and Hypertension: The interplay of interleukin-6, dietary sodium, and the renin-angiotensin system in humans. Am. J. Hypertens. 2011, 24, 1143–1148. [Google Scholar] [CrossRef]
- Taddei, S.; Virdis, A.; Ghiadoni, L.; Sudano, I.; Salvetti, A. Antihypertensive drugs and reversing of endothelial dysfunction in hypertension. Curr. Hypertens. Rep. 2000, 2, 64–70. [Google Scholar] [CrossRef]
- Meigs, J.B.; Hu, F.B.; Rifai, N.; Manson, J.E. Biomarkers of endothelial dysfunction and risk of type 2 diabetes mellitus. JAMA 2004, 291, 1978–1986. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Long, A.N.; Dagogo-Jack, S. Comorbidities of diabetes and hypertension: Mechanisms and approach to target organ protection. J. Clin. Hypertens. 2011, 13, 244–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Emdin, C.A.; Anderson, S.G.; Woodward, M.; Rahimi, K. Usual blood pressure and risk of new-onset diabetes. J. Am. Coll Cardiol. 2015, 66, 1552–1562. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.; Armstrong, E.J.; Kim, G.; Oh, J.; Kang, S.M.; Lee, B.W.; Ahn, C.W.; Cha, B.S.; Lee, H.C.; Mantzoros, C.S.; et al. Undiagnosed diabetes is prevalent in younger adults and associated with a higher risk cardiometabolic profile compared to diagnosed diabetes. Am. Heart J. 2015, 170, 760–769.e2. [Google Scholar] [CrossRef]
- Rathmann, W.; Haastert, B.; Icks, A.; Löwel, H.; Meisinger, C.; Holle, R.; Giani, G. High prevalence of undiagnosed diabetes mellitus in Southern Germany: Target populations for efficient screening. The KORA survey 2000. Diabetologia 2003, 46, 182–189. [Google Scholar] [CrossRef]
- Selvin, E.; Wang, D.; Lee, A.K.; Bergenstal, R.M.; Coresh, J. Identifying trends in undiagnosed diabetes in u.s. adults by using a confirmatory definition: A cross-sectional study. Ann Intern Med. 2017, 167, 769. [Google Scholar] [CrossRef]
- Algoblan, A.; Alalfi, M.; Khan, M. Mechanism linking diabetes mellitus and obesity. Diabetes Metab. Syndr. Obes. Targets Ther. 2014, 7, 587–591. [Google Scholar] [CrossRef] [Green Version]
- Lyu, Y.S.; Kim, S.Y.; Bae, H.Y.; Kim, J.H. Prevalence and risk factors for undiagnosed glucose intolerance status in apparently healthy young adults aged <40 years: The Korean National Health and Nutrition Examination Survey 2014–2017. Int. J. Environ. Res. Public Health 2019, 16, 2393. [Google Scholar] [CrossRef]
- Cui, J.; Sun, J.; Wang, W.; Xin, H.; Qiao, Q.; Baloch, Z.; Ma, A. The association of triglycerides and total cholesterol concentrations with newly diagnosed diabetes in adults in China. Oncotarget 2017, 8, 103477–103485. [Google Scholar] [CrossRef] [Green Version]
- Ginsberg, H.N.; Zhang, Y.L.; Hernandez-Ono, A. Regulation of plasma triglycerides in insulin resistance and diabetes. Arch Med. Res. 2005, 36, 232–240. [Google Scholar] [CrossRef]
- Willi, C.; Bodenmann, P.; Ghali, W.A.; Faris, P.D.; Cornuz, J. Active smoking and the risk of type 2 diabetes: A systematic review and meta-analysis. JAMA 2007, 298, 2654. [Google Scholar] [CrossRef] [PubMed]
- Baliunas, D.O.; Taylor, B.J.; Irving, H.; Roerecke, M.; Patra, J.; Mohapatra, S.; Rehm, J. Alcohol as a risk factor for type 2 diabetes: A systematic review and meta-analysis. Diabetes Care 2009, 32, 2123–2132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knott, C.; Bell, S.; Britton, A. Alcohol consumption and the risk of type 2 diabetes: A systematic review and dose-response meta-analysis of more than 1.9 million individuals from 38 observational studies. Diabetes Care 2015, 38, 1804–1812. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.M.; Lee, J.S.; Lee, J.; Na, J.K.; Han, J.H.; Yoon, D.K.; Baik, S.H.; Choi, D.S.; Choi, K.M. Prevalence of diabetes and impaired fasting glucose in Korea: Korean National Health and Nutrition Survey 2001. Diabetes Care 2006, 29, 226–231. [Google Scholar] [CrossRef] [Green Version]
- Aune, D.; Norat, T.; Leitzmann, M.; Tonstad, S.; Vatten, L.J. Physical activity and the risk of type 2 diabetes: A systematic review and dose–response meta-analysis. Eur. J. Epidemiol. 2015, 30, 529–542. [Google Scholar] [CrossRef]
- Hu, F.B.; Sigal, R.J.; Rich-Edwards, J.W.; Colditz, G.A.; Solomon, C.G.; Willett, W.C.; Speizer, F.E.; Manson, J.E. Walking compared with vigorous physical activity and risk of type 2 diabetes in women: A prospective study. JAMA 1999, 282, 1433–1439. [Google Scholar] [CrossRef] [Green Version]
- Hsia, J.; Wu, L.; Allen, C.; Oberman, A.; Lawson, W.E.; Torréns, J.; Saffird, M.; Limacher, M.C.; Howard, B.V. Physical activity and diabetes risk in postmenopausal women. Am. J. Prev. Med. 2005, 28, 19–25. [Google Scholar] [CrossRef]
- Sato, K.K.; Hayashi, T.; Kambe, H.; Nakamura, Y.; Harita, N.; Endo, G.; Yoneda, T. Walking to work is an independent predictor of incidence of type 2 diabetes in japanese men: The Kansai Healthcare Study. Diabetes Care 2007, 30, 2296–2298. [Google Scholar] [CrossRef] [Green Version]
- Park, J.H.; Lee, Y.E. Effects of exercise on glycemic control in type 2 diabetes mellitus in Koreans: The fifth Korea National Health and Nutrition Examination Survey (KNHANES V). J. Phys. Ther. Sci. 2015, 27, 3559–3564. [Google Scholar] [CrossRef] [Green Version]
- Lee, M.R.; Jung, S.M.; Bang, H.; Kim, H.S.; Kim, Y.B. Association between muscle strength and type 2 diabetes mellitus in adults in Korea: Data from the Korea national health and nutrition examination survey (KNHANES) VI. Medicine (Baltimore) 2018, 97, e10984. [Google Scholar] [CrossRef]
- Warner, E.A.; Ziboh, A.U. The effects of outpatient management on hospitalization for ambulatory care sensitive conditions associated with diabetes mellitus. South Med. J. 2008, 101, 815–817. [Google Scholar] [CrossRef] [PubMed]
- Organisation for Economic Co-Operation and Development. Health at a Glance 2015: OECD Indicators. 2015. Available online: https://www.oecd-ilibrary.org/social-issues-migration-health/health-at-a-glance-2015_health_glance-2015-en (accessed on 29 December 2019).
- Kim, H.; Cheng, S.H. Assessing quality of primary diabetes care in South Korea and Taiwan using avoidable hospitalizations. Health Policy 2018, 122, 1222–1231. [Google Scholar] [CrossRef] [PubMed]
- Hillier, T.A.; Pedula, K.L. Characteristics of an adult population with newly diagnosed type 2 diabetes: The relation of obesity and age of onset. Diabetes Care 2001, 24, 1522–1527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bando, Y.; Kanehara, H.; Aoki, K.; Katoh, K.; Toya, D.; Tanaka, N. Characteristics of undiagnosed diabetes mellitus in a population undergoing health screening in Japan: Target populations for efficient screening. Diabetes Res. Clin. Pract. 2009, 83, 341–346. [Google Scholar] [CrossRef] [PubMed]
- Lim, N.K.; Park, S.H.; Choi, S.J.; Lee, K.S.; Park, H.Y. A risk score for predicting the incidence of type 2 diabetes in a middle-aged Korean cohort. Circ. J. 2012, 76, 1904–1910. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.S.; Ko, S.H.; Baeg, M.K.; Han, K.D. A simple screening score to predict diabetes in cancer patients: A Korean nationwide population-based cohort study. Medicine (Baltimore) 2019, 98, e18354. [Google Scholar] [CrossRef] [PubMed]
- Ryu, K.S.; Kang, H.Y.J.; Lee, S.W.; Park, H.W.; You, N.Y.; Kim, J.H.; Hwangbo, Y.; Choi, S.K.; Cha, H.S. Screening model for estimating undiagnosed diabetes among people with a family history of diabetes mellitus: A KNHANES-based study. Int. J. Environ. Res. Public Health 2020, 17, 8903. [Google Scholar] [CrossRef]
- Song, S.O.; Song, Y.D.; Nam, J.Y.; Park, K.H.; Yoon, J.H.; Son, K.M.; Ko, Y.; Lim, D.H. Epidemiology of type 1 diabetes mellitus in korea through an investigation of the national registration project of type 1 diabetes for the reimbursement of glucometer strips with additional analyses using claims data. Diabetes Metab. J. 2016, 40, 35–45. [Google Scholar] [CrossRef] [Green Version]
- American Diabetes Association. Prevention or delay of type 2 diabetes. Diabetes Care 2017, 40, S44–S47. [Google Scholar] [CrossRef] [Green Version]
- Valdez, R. Detecting undiagnosed type 2 diabetes: Family history as a risk factor and screening tool. J. Diabetes Sci. Technol. 2009, 3, 722–726. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variables | Basic Characteristics | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Without DM | DM | UDM | p-Value | |||||||
| n | %(mean) | SD | n | %(mean) | SD | n | %(mean) | SD | ||
| Demographic characteristics | ||||||||||
| Age | 27,809 | 42.62 | 0.15 | 3626 | 61.55 | 0.26 | 1176 | 53.21 | 0.44 | <0.0001 b |
| 20–29 | 4299 | 23.52 | 0.42 | 14 | 0.86 | 0.26 | 29 | 4.21 | 0.85 | <0.0001 a |
| 30–39 | 6151 | 23.57 | 0.42 | 73 | 2.98 | 0.39 | 99 | 10.54 | 1.17 | |
| 40–49 | 5546 | 21.69 | 0.36 | 263 | 11.57 | 0.76 | 231 | 26.16 | 1.66 | |
| 50–59 | 5038 | 16.62 | 0.28 | 720 | 26.66 | 0.95 | 295 | 28.72 | 1.63 | |
| 60–69 | 3694 | 8.29 | 0.19 | 1230 | 29.13 | 0.88 | 295 | 17.68 | 1.11 | |
| ≥70 | 3081 | 6.31 | 0.18 | 1326 | 28.79 | 0.86 | 227 | 12.69 | 0.94 | |
| Sex | ||||||||||
| Female | 17,129 | 54.00 | 0.34 | 1828 | 46.86 | 1.02 | 500 | 36.43 | 1.56 | <0.0001 a |
| Male | 10,680 | 46.00 | 0.34 | 1798 | 53.14 | 1.02 | 676 | 63.57 | 1.56 | |
| Educational attainment | ||||||||||
| High school or less | 14,508 | 45.82 | 0.52 | 2982 | 79.48 | 0.88 | 842 | 67.01 | 1.77 | <0.0001 a |
| Higher than high school | 12,901 | 52.62 | 0.52 | 568 | 18.22 | 0.84 | 292 | 29.61 | 1.73 | |
| No response | 400 | 1.55 | 0.13 | 76 | 2.29 | 0.30 | 42 | 3.38 | 0.64 | |
| Marital status | ||||||||||
| Not married | 5219 | 27.24 | 0.45 | 90 | 4.00 | 0.46 | 72 | 9.74 | 1.24 | <0.0001 a |
| Married | 22,586 | 72.76 | 0.45 | 3535 | 95.97 | 0.46 | 1103 | 90.24 | 1.24 | |
| No response | 4 | 0.00 | 0.00 | 1 | 0.03 | 0.03 | 1 | 0.02 | 0.02 | |
| Income level | ||||||||||
| Low | 6435 | 24.51 | 0.45 | 995 | 29.01 | 0.96 | 358 | 31.86 | 1.63 | <0.0001 a |
| Middle–low | 6955 | 25.13 | 0.42 | 918 | 25.14 | 0.87 | 288 | 23.96 | 1.49 | |
| Middle | 7139 | 25.26 | 0.40 | 832 | 22.48 | 0.84 | 266 | 20.95 | 1.35 | |
| High | 7109 | 24.39 | 0.51 | 857 | 22.70 | 0.89 | 247 | 21.82 | 1.46 | |
| No response | 171 | 0.71 | 0.08 | 24 | 0.67 | 0.17 | 17 | 1.42 | 0.40 | |
| Health status | ||||||||||
| Family history of diabetes | ||||||||||
| No | 23,621 | 84.11 | 0.28 | 2834 | 74.24 | 0.95 | 927 | 75.28 | 1.60 | <0.0001 a |
| Yes | 4188 | 15.89 | 0.28 | 792 | 25.76 | 0.95 | 249 | 24.72 | 1.60 | |
| Hypertension status | ||||||||||
| Normal | 14,963 | 57.58 | 0.42 | 619 | 19.71 | 0.84 | 225 | 20.72 | 1.41 | <0.0001 a |
| At high risk | 6615 | 24.22 | 0.34 | 650 | 20.02 | 0.86 | 321 | 28.78 | 1.58 | |
| Hypertension | 6175 | 18.20 | 0.29 | 2347 | 60.27 | 1.01 | 627 | 50.50 | 1.79 | |
| Obesity | ||||||||||
| Underweight | 1487 | 5.69 | 0.18 | 46 | 1.11 | 0.19 | 10 | 0.60 | 0.26 | <0.0001 a |
| Normal | 12,671 | 45.18 | 0.37 | 1027 | 28.68 | 0.94 | 237 | 19.31 | 1.38 | |
| Overweight | 6343 | 22.33 | 0.30 | 897 | 23.71 | 0.85 | 250 | 20.25 | 1.41 | |
| Obesity | 7255 | 26.60 | 0.33 | 1648 | 46.25 | 1.00 | 678 | 59.59 | 1.73 | |
| No response | 53 | 0.20 | 0.03 | 8 | 0.25 | 0.10 | 1 | 0.25 | 0.25 | |
| BMI (kg/m2) | 27,756 | 23.21 | 0.03 | 3618 | 25.04 | 0.08 | 1175 | 26.26 | 0.14 | <0.0001 b |
| Health determinants | ||||||||||
| Current smoking status | ||||||||||
| No | 22,581 | 76.82 | 0.36 | 2901 | 76.68 | 0.87 | 867 | 67.57 | 1.72 | <0.0001 a |
| Yes | 5064 | 22.62 | 0.36 | 669 | 21.51 | 0.86 | 287 | 30.35 | 1.69 | |
| No response | 164 | 0.57 | 0.05 | 56 | 1.81 | 0.27 | 22 | 2.08 | 0.51 | |
| Heavy alcohol consumption | ||||||||||
| No | 25,034 | 87.90 | 0.26 | 3272 | 87.04 | 0.78 | 969 | 79.18 | 1.46 | <0.0001 a |
| Yes | 2608 | 11.54 | 0.26 | 304 | 11.30 | 0.72 | 188 | 19.09 | 1.43 | |
| No response | 167 | 0.56 | 0.05 | 50 | 1.66 | 0.27 | 19 | 1.73 | 0.47 | |
| Walking | ||||||||||
| No | 9180 | 30.73 | 0.63 | 1055 | 28.76 | 1.02 | 332 | 28.91 | 1.65 | <0.0001 a |
| Yes | 5561 | 19.77 | 0.45 | 686 | 17.60 | 0.84 | 174 | 14.03 | 1.23 | |
| No response | 13,068 | 49.50 | 0.91 | 1885 | 53.64 | 1.33 | 670 | 57.06 | 1.91 | |
| Muscle training | ||||||||||
| No | 21,875 | 76.77 | 0.34 | 2904 | 79.12 | 0.84 | 917 | 77.51 | 1.49 | <0.0001 a |
| Yes | 5528 | 21.64 | 0.33 | 644 | 18.52 | 0.81 | 216 | 18.67 | 1.38 | |
| No response | 406 | 1.58 | 0.13 | 78 | 2.36 | 0.31 | 43 | 3.82 | 0.71 | |
| Healthcare accessibility | ||||||||||
| Undergone national health screening | ||||||||||
| No | 10,479 | 41.29 | 0.41 | 1196 | 33.70 | 0.97 | 459 | 41.69 | 1.77 | <0.0001 a |
| Yes | 16,972 | 57.30 | 0.41 | 2370 | 64.46 | 0.98 | 681 | 55.26 | 1.79 | |
| No response | 358 | 1.40 | 0.12 | 60 | 1.85 | 0.28 | 36 | 3.05 | 0.62 | |
| Undergone cancer screening | ||||||||||
| No | 12,568 | 52.34 | 0.41 | 1328 | 38.06 | 1.00 | 524 | 49.41 | 1.70 | <0.0001 a |
| Yes | 14,879 | 46.24 | 0.40 | 2237 | 60.07 | 1.01 | 614 | 47.42 | 1.68 | |
| No response | 362 | 1.42 | 0.12 | 61 | 1.87 | 0.28 | 38 | 3.17 | 0.63 | |
| Laboratory tests | ||||||||||
| Total cholesterol (mg/dL) | 27,808 | 188.18 | 0.28 | 3625 | 175.70 | 0.79 | 1176 | 206.06 | 1.62 | <0.0001 b |
| Systolic blood pressure (mmHg) | 27,776 | 114.60 | 0.13 | 3621 | 125.70 | 0.34 | 1175 | 126.82 | 0.58 | <0.0001 b |
| Diastolic blood pressure (mmHg) | 27,776 | 74.89 | 0.09 | 3621 | 74.64 | 0.22 | 1175 | 80.88 | 0.40 | <0.0001 b |
| Fasting blood glucose (mg/dL) | 27,809 | 89.43 | 0.05 | 3626 | 139.64 | 0.86 | 1176 | 155.99 | 1.67 | <0.0001 b |
| Triglyceride concentration (mg/dL) | 27,808 | 120.34 | 0.77 | 3625 | 168.96 | 2.95 | 1176 | 220.93 | 7.44 | <0.0001 b |
| Variables | DM a,b | UDM a,b |
|---|---|---|
| OR [95% CI] | OR [95% CI] | |
| Demographic characteristics | ||
| Age | ||
| 20–29 | Reference | Reference |
| 30–39 | 3.45 [1.80–6.61] | 2.45 [1.53–3.92] |
| 40–49 | 14.45 [7.73–26.98] | 6.68 [4.30–10.38] |
| 50–59 | 43.67 [23.70–80.44] | 9.64 [6.29–14.77] |
| 60–69 | 95.52 [51.77–176.24] | 11.90 [7.80–18.16] |
| ≥70 | 124.08 [67.45–228.24] | 11.23 [7.23–17.44] |
| Sex | ||
| Female | Reference | Reference |
| Male | 1.34 [1.22–1.46] | 2.05 [1.79–2.36] |
| Educational attainment | ||
| High school or less | Reference | Reference |
| Higher than high school | 0.20 [0.18–0.22] | 0.39 [0.33–0.45] |
| Marital status | ||
| Not married | Reference | Reference |
| Married | 8.96 [7.07–11.35] | 3.45 [2.61–4.55] |
| Income level | ||
| Low | Reference | Reference |
| Middle–low | 0.85 [0.76–0.95] | 0.74 [0.61–0.89] |
| Middle | 0.75 [0.67–0.85] | 0.63 [0.53–0.77] |
| High | 0.85 [0.76–0.95] | 0.74 [0.61–0.89] |
| Health status | ||
| Family history of diabetes | ||
| No | Reference | Reference |
| Yes | 1.84 [1.66–2.03] | 1.71 [1.44–2.03] |
| Hypertension status | ||
| Normal | Reference | Reference |
| At high risk | 2.41 [2.10–2.78] | 3.30 [2.71–4.03] |
| Hypertension | 9.67 [8.67–10.80] | 7.71 [6.43–9.25] |
| Obesity | ||
| Underweight | 0.31 [0.22–0.43] | 0.25 [0.11–0.58] |
| Normal | Reference | Reference |
| Overweight | 1.67 [1.49–1.88] | 2.12 [1.70–2.65] |
| Obesity | 2.73 [2.47–3.02] | 5.20 [4.34–6.24] |
| Health determinants | ||
| Current smoking status | ||
| No | Reference | Reference |
| Yes | 3.25 [2.27–4.66] | 4.35 [2.61–7.25] |
| Heavy alcohol consumption | ||
| No | Reference | Reference |
| Yes | 0.99 [0.85–1.15] | 1.82 [1.51–2.20] |
| Walking | ||
| No | Reference | Reference |
| Yes | 0.96 [0.84–1.09] | 0.74 [0.60–0.93] |
| Muscle training | ||
| No | Reference | Reference |
| Yes | 0.83 [0.74–0.93] | 0.84 [0.70–1.01] |
| Healthcare accessibility | ||
| Undergone national health screening | ||
| No | Reference | Reference |
| Yes | 1.38 [1.26–1.51] | 0.96 [0.83–1.11] |
| Undergone cancer screening | ||
| No | Reference | Reference |
| Yes | 1.78 [1.63–1.95] | 1.08 [0.94–1.24] |
| Laboratory tests | ||
| Total cholesterol (mg/dL) | 0.99 [0.99–0.99] | 1.02 [1.01–1.01] |
| Systolic blood pressure (mmHg) | 1.00 [0.99–1.00] | 1.05 [1.05–1.06] |
| Diastolic blood pressure (mmHg) | 1.04 [1.04–1.04] | 1.04 [1.04–1.05] |
| Fasting blood glucose (mg/dL) | 1.34 [1.31–1.37] | 1.35 [1.32–1.38] |
| Triglyceride concentration (mg/dL) | 1.00 [1.00–1.00] | 1.01 [1.00–1.01] |
| Variables | Crude Model a,c | Age-/Sex-Adjusted Model b,c |
|---|---|---|
| OR [95% CI] | AOR [95% CI] | |
| Demographic characteristics | ||
| Age | ||
| 20–29 | Reference | |
| 30–39 | 0.71 [ 0.32–1.58] | |
| 40–49 | 0.46 [0.22–0.99] | |
| 50–59 | 0.22 [0.11–0.46] | |
| 60–69 | 0.13 [0.06–0.26] | |
| ≥70 | 0.09 [0.04–0.19] | |
| Sex | ||
| Female | Reference | |
| Male | 1.54 [1.31–1.80] | |
| Educational attainment | ||
| High school or less | Reference | Reference |
| Higher than high school | 1.94 [1.60–2.36] | 1.11 [0.89–1.39] |
| Marital status | ||
| Not married | Reference | Reference |
| Married | 0.49 [0.27–0.55] | 1.05 [0.71–1.56] |
| Income level | ||
| Low | Reference | Reference |
| Middle–low | 0.88 [0.70–1.10] | 0.89 [0.71–1.11] |
| Middle | 0.84 [0.68–1.04] | 0.90 [0.72–1.13] |
| High | 0.878 [0.70–1.10] | 0.94 [0.74–1.18] |
| Health status | ||
| Family history of diabetes | ||
| No | Reference | Reference |
| Yes | 0.93 [0.77–1.13] | 0.54 [0.43–0.66] |
| Hypertension status | ||
| Normal | Reference | Reference |
| At high risk | 1.37 [1.09–1.72] | 1.65 [1.29–2.11] |
| Hypertension | 0.80 [0.65–0.98] | 1.32 [1.06–1.64] |
| Obesity | ||
| Underweight | 0.81 [0.33–2.02] | 0.98 [0.36–2.65] |
| Normal | Reference | Reference |
| Overweight | 1.27 [1.00–1.62] | 1.22 [0.95–1.58] |
| Obesity | 1.90 [1.55–2.34] | 1.67 [1.34–2.08] |
| Health determinants | ||
| Current smoking status | ||
| No | Reference | Reference |
| Yes | 1.62 [1.34–1.95] | 1.06 [0.86–1.31] |
| Heavy alcohol consumption | ||
| No | Reference | Reference |
| Yes | 1.84 [1.46–2.32] | 1.20 [0.93–1.55] |
| Walking | ||
| No | Reference | Reference |
| Yes | 0.78 [0.61–1.00] | 0.78 [0.60–1.02] |
| Muscle training | ||
| No | Reference | Reference |
| Yes | 1.01 [0.83–1.24] | 0.85 [0.68–1.05] |
| Healthcare accessibility | ||
| Undergone national health screening | ||
| No | Reference | Reference |
| Yes | 0.70 [0.59–0.83] | 0.74 [0.62–0.89] |
| Undergone cancer screening | ||
| No | Reference | Reference |
| Yes | 0.61 [0.52–0.71] | 0.71 [0.60–0.85] |
| Laboratory tests | ||
| Total cholesterol (mg/dL) | 1.02 [1.02–1.02] | 1.02 [1.02–1.02] |
| Systolic blood pressure (mmHg) | 1.00 [1.00–1.01] | 1.01 [1.01–1.02] |
| Diastolic blood pressure (mmHg) | 1.06 [1.05–1.07] | 1.04 [1.03–1.05] |
| Fasting blood glucose (mg/dL) | 1.01 [1.01–1.01] | 1.01 [1.00–1.01] |
| Triglyceride concentration (mg/dL) | 1.00 [1.00–1.00] | 1.00 [1.00–1.00] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.; Ryu, K.S.; Kang, H.Y.J.; You, N.Y.; Choi, K.S.; Hwangbo, Y.; Lee, J.W.; Cha, H.S. Risk Factors of Undiagnosed Diabetes Mellitus among Korean Adults: A National Cross-Sectional Study Using the KNHANES Data. Int. J. Environ. Res. Public Health 2021, 18, 1195. https://doi.org/10.3390/ijerph18031195
Lee S, Ryu KS, Kang HYJ, You NY, Choi KS, Hwangbo Y, Lee JW, Cha HS. Risk Factors of Undiagnosed Diabetes Mellitus among Korean Adults: A National Cross-Sectional Study Using the KNHANES Data. International Journal of Environmental Research and Public Health. 2021; 18(3):1195. https://doi.org/10.3390/ijerph18031195
Chicago/Turabian StyleLee, Sangwon, Kwang Sun Ryu, Ha Ye Jin Kang, Na Young You, Kui Son Choi, Yul Hwangbo, Jae Wook Lee, and Hyo Soung Cha. 2021. "Risk Factors of Undiagnosed Diabetes Mellitus among Korean Adults: A National Cross-Sectional Study Using the KNHANES Data" International Journal of Environmental Research and Public Health 18, no. 3: 1195. https://doi.org/10.3390/ijerph18031195
APA StyleLee, S., Ryu, K. S., Kang, H. Y. J., You, N. Y., Choi, K. S., Hwangbo, Y., Lee, J. W., & Cha, H. S. (2021). Risk Factors of Undiagnosed Diabetes Mellitus among Korean Adults: A National Cross-Sectional Study Using the KNHANES Data. International Journal of Environmental Research and Public Health, 18(3), 1195. https://doi.org/10.3390/ijerph18031195