
Early-Life Exposure to Environmental Air Pollution and Autism Spectrum Disorder: A Review of Available Evidence

 , , ,
, , ,  , ,
, ,  , ,
, , 

Abstract
:1. Introduction
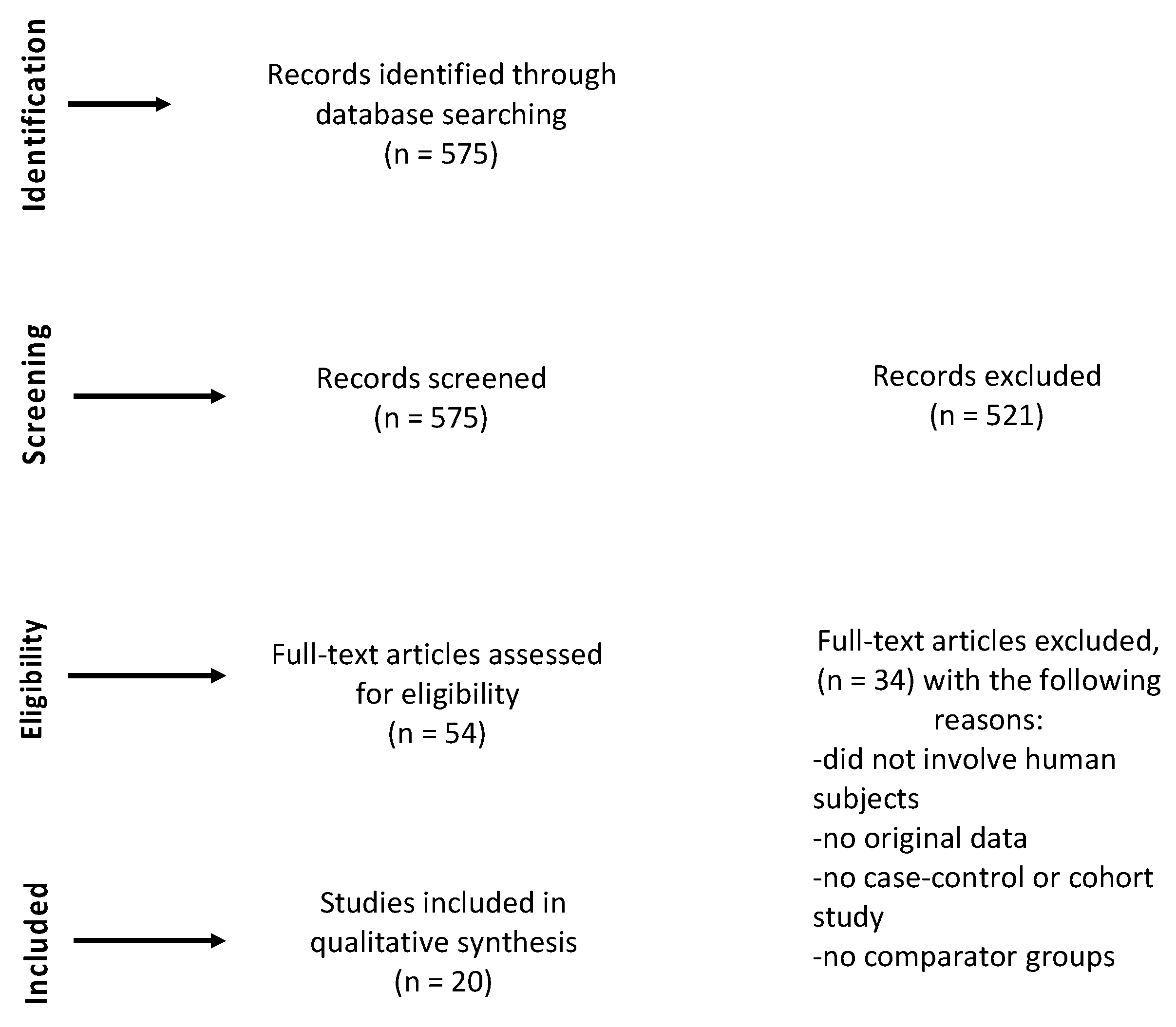
2. Materials and Methods
- human studies;
- full-text articles in English;
- assessment of exposure to airborne environmental pollutants during pregnancy or in the first years of the baby’s life;
- only case-control studies or cohort studies.
- authors and year;
- study design;
- sample size;
- exposure assessment measures;
- method of analysis;
- adjustment variables;
- ASD outcome assessment;
- time window of exposure;
- main findings.
3. Results
3.1. Association between PM and ASD

{kind=link}
| Authors and Year | Study Design | Sample Size/Country | ASD Outcome Assessment | Exposure Assessment | Method of Analysis | Adjustment Variables | Time Window of Exposure | Main Findings |
|---|---|---|---|---|---|---|---|---|
| McGuinn et al., 2020 [23] | Case-control | 674 ASD cases and 855 controls from California, Colorado, Georgia, Maryland, North Carolina, and Pennsylvania | ASD case classification based on the results from the ADOS (Autism Diagnostic Observation Schedule) and ADI-R (Autism Diagnostic Interview-Revised) | Satellite-based model to assign air pollutant exposure (PM2.5, O3) averages during several critical periods of neurodevelopment | Logistic regression model | -study site -maternal age -maternal education -maternal race -maternal smoking, -month and year of birth. | -3 months before pregnancy -each trimester of pregnancy -the entire pregnancy -first year of life | The strongest association was found between PM2.5 in the first year of life, with an odds ratio (OR) = 1.3 (95%CI: 1.0, 1.6) for 1.6 µg/m3 increase in PM2.5 |
| Kaufman et al., 2019 [25] | Case-control | 428 ASD cases and 6420 controls from metropolitan Cincinnati area in southwest Ohio | ASD diagnosis according to International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM). | Daily PM2.5 individual exposure estimations provided by the United States Environmental Protection Agency (US EPA), based on their residential address | Logistic regression model | -maternal and birth-related confounders -multiple temporal exposure windows | -each trimester pregnancy -first year of life -second year of life | Odds Ratios related to second trimester, the first year of life and the cumulative period (that included the period from pregnancy to the second year of life) were: 1.41 (95%CI: 0.89, 2.24), 1.54 (95%CI: 0.98, 2.40), 1.52 (95%CI: 1.00, 2.31), respectively |
| McGuinn et al., 2019 [24] | Case-control | 674 ASD cases and 855 controls from California, Colorado, Georgia, Maryland, North Carolina, and Pennsylvania | ASD case classification based on the results from the ADOS (Autism Diagnostic Observation Schedule) and ADI-R (Autism Diagnostic Interview-Revised) | Air pollution was assessed by roadway proximity and particulate matter <2.5 µm (PM2.5) exposure | Logistic regression model | -neighborhood deprivation | -pregnancy -first year of life | The association between exposure to PM2.5 and the risk of ASD in the first year of life was found stronger among those presenting a higher deprivation state (OR = 2.42, 95%CI = 1.20, 4.86) than those living in a low deprivation state (OR = 1.46, 95%CI = 0.80, 2.65) |
| Ritz et al., 2018 [26] | Case-control | 15,387 ASD cases and 68,139 controls from Denmark | ASD diagnosis according to International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) | Exposures estimates provided by the dispersion models (AirGIS) for the detected pollutants (NO2, SO2, PM2.5 and PM10) in relation to the maternal residence during the examined periods | Conditional logistic regression | -parental age -neighborhood -socio-economic indicators -maternal smoking | -pregnancy -9 months after pregnancy | Exposure to PM2.5 and PM10 during the 9 months after pregnancy increases the risk of a diagnosis of ASD with an adjusted OR of 1.06 (95%CI: 1.01, 1.11) for 3.61 μg/m3 increase of PM2.5 and an OR of 1.04 (95 % CI: 1.01, 1.15) per each increase of 3.8 μg/m3 PM10 in IQR value, respectively |
| Chen et al., 2018 [27] | Case-control | 124 ASD cases and 1240 controls from China | ASD cases were diagnosed by pediatricians according to Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-V) | Air pollution was assessed with satellite remote sensing data | Conditional logistic regression | -birth weight -gestational weeks -disease history -trauma history -maternal age, -familial mental health history -parents’ marital status -parental relationship -parenting, -parents’ educational level -smoking status | -first year of life -second year of life -third year of life | Strong association with PM2.5 in the second and third years of life with an OR of 1.50 (1.01, 2.22) in the second year and an OR 1.78 (1.05, 3.02) in the third year, respectively for each increase of 3.4 μg/m3 in the IQR Strong association with PM10 during the first three years of life and ASD with an OR of 1.16 (0.91, 1.49) in the first year, 1.73 (1.11, 2.68) in the second year and 1.58 (0.98, 2.56), per interquartile range (IQR) increase per 4.9 μg/m3 |
| Raz et al., 2015 [28] | Case-control | 245 ASD cases and 1522 controls from United States | Final ASD case classification was based on the results from the ADI-R Autism Diagnostic Interview-Revised) and SRS scores (Social Responsiveness Scale) | Exposure to PM2.5 and PM10 assessed by using a space-time model and linked to maternal residence addresses | Logistic regression model | -child’s birth year -birth month -sex -maternal age at birth -paternal age at birth | -9 months before pregnancy -trimester 1,2,3 -entire pregnancy -9 months after birth | Association with PM2.5 during the third trimester of pregnancy and ASD. OR of 1.42 (1.09, 1.86) per IQR increase per 4.40 μg/m3 No significant association between PM10 and ASD |
| Talbot et al., 2015 [29] | Case-control | 217 ASD cases and 226 controls from southwestern Pennsylvania | A case of ASD was defined as any child who scored a 15 or above on the Social Communication Questionnaire (SCQ), and had written documentation, including the Autism Diagnostic Observation Schedule (ADOS) or diagnosis of an ASD from a child psychologist or psychiatrist | Person- and time specific PM2.5 estimates for individual and cumulative key developmental time periods | Logistic regression model | -college education -smoking status -race -maternal age | -pre-pregnancy -each trimester, pregnancy -first year of life -second year of life -cumulative (starting from pre-pregnancy) | Both prenatal exposures and those occurred in the first two years of life are associated with an increased risk of ASD expressed by an Odds Ratio of 1.51, 95%CI = 1.10–2.26) |
| Becerra et al., 2013 [30] | Case-control | 7603 ASD cases and 10 controls per case from Los Angeles, California | The diagnosis of ASD was based on the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition, Text Revision (DSM-IV-R) | Modeled concentrations of PM2.5 from air monitoring station 1993-2006, assigned by residential address at delivery/birth | Conditional logistic regression | -maternal age -maternal place of birth -race -education -type of birth -parity -insurance type -gestational age at birth | -pregnancy | Association with PM2.5 during pregnancy and ASD with an OR of 1.15 (1.06, 1.24) per interquartile range (IQR) increase per 4.68 μg/m3 |
| Volk et al., 2013 [31] | Case-control | 279 ASD cases and 245 controls from California | ASD case classification based on the results from the ADOS (Autism Diagnostic Observation Schedule) and ADI-R (Autism Diagnostic Interview-Revised) | Traffic-related air pollution was assigned to each mother’s location using a line-source air-quality dispersion model | Logistic additive models | -child gender -child ethnicity -maximal education of parents -maternal age -prenatal smoking | -pregnancy -trimester 1, 2, 3, -year 1 | Exposure to PM 2.5, during pregnancy and during the first year of life was associated with ASD with an OR of 2.08 (95%CI, 1.93–2.25) Exposure to PM10 in the prenatal period was associated with ASD with an OR of 2.17 (1.49, 3.16) per each increase of 14.6 μg/m3 in IQR value |
| Jo et al., 2019 [32] | Cohort | 246,420 children from Southern California | ASD diagnosis according to International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) | PM2.5 measured at regulatory air monitoring stations was interpolated to estimate exposures during preconception and each pregnancy trimester, and first year of life at each child’s birth address | Cox regression models | -birth year -relevant maternal and child characteristics | -preconception -trimester 1,2,3 -year 1 | Statistically significant association between exposures to PM2.5 and risk of ASD quantified by the following Hazard Ratios (HR) per each increase of 6.5 μg/m3 in IQR values in different phases of the pregnancy: 1.17 (95%CI 1.04–1.33) in the entire 9-months period; 1.10 (95%CI, 1.02–1.19) in the first trimester of pregnancy, 1.08 (95%CI, 1.00–1.18) in the third trimester of pregnancy; 1.21 (95%CI, 1.05–1.40) in the first year of life |
| Pagalan et al., 2019 [33] | Cohort | Cohort of 129,439 children: 1276 were diagnosed with ASD from Metro Vancouver, British Columbia, Canada | ASD case classification based on the results from the ADOS (Autism Diagnostic Observation Schedule) and ADI-R (Autism Diagnostic Interview-Revised) | Monthly mean exposures to PM 2.5, at the maternal residence during pregnancy were estimated with temporally adjusted, high-resolution land use regression models | Logistic regression model | -child sex -birth month -birth year -maternal age -maternal birthplace -neighborhood level urbanicity and income band | -pregnancy | No significant association between PM2.5 and ASD |
| Guxens et al., 2016 [34] | Cohort | 8079 children from four European population-based birth/child cohorts (Sweden, Netherlands, Italy, and Spain) | Autistic traits were assessed in children using:-the Autism Spectrum Disorder module of the Autism—Tics, Attention Deficit and Hyperactivity Disorders, and Other Comorbidities (A-TAC) inventory in the Swedish cohort-the Pervasive Developmental Problems (PDP) subscale of the Child Behavior Checklist for Toddlers in the Dutch cohort and in the Italian cohort-an adapted 18-item version of the Social Responsiveness Scale (SRS) in the Dutch cohort at age 6 years;-the Childhood Autism Spectrum Test (CAST) in the Spanish cohorts | PM2.5 and PM10 absorbance were estimated for birth addresses by land-use regression models based on monitoring campaigns performed between 2008 and 2011. Levels of exposures were extrapolated back in time to exact pregnancy periods | Logistic regression model | -age at delivery -educational level -country of birth -prenatal smoking -parity -maternal height -pre-pregnancy weight -pre-pregnancy body mass index -child’s sex -date of birth -child’s age at autistic trait assessment -information on the evaluator of the autistic traits -urbanity at child’s birth address | -pregnancy | No significant association between PM2.5, PM10 and ASD |
| Kalkbrenner et al., 2015 [35] | Case-Control | 979 ASD cases and 14,666 controls from North Carolina and San Francisco Bay Area in California | The diagnosis of ASD was based on the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition, Text Revision (DSM-IV-R) | Exposure to PM10 at the birth address was assigned to each child by a geostatistical interpolation method using daily concentrations from air pollution regulatory monitors | Logistic generalized additive models | -year -state -race -maternal education -maternal age -the calendar week of the child’s birth | -pre-conception -trimester 1,2,3 -postnatal | The results obtained showed an association with the third trimester of pregnancy, with an OR of 1.36 (1.13, 1.63) per 10 μg/m3 increase in IQR value |
| Yousefian et al., 2018 [36] | Case-Control | 134 ASD cases and 388 controls from Tehran, Iran | The diagnosis of ASD was based on the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition, Text Revision (DSM-IV-R) | Land-use regression models were used to estimate their annual mean exposure to ambient PM10 | Logistic regression | -maternal age at birth -maternal education -paternal education -cousin marriage -maternal smoking during pregnancy -birth order -gestational age (weeks) -multiple births -maternal disease -paternal disease | -pregnancy | No significant association between PM10 and ASD |
| Gong et al., 2017 [37] | Case-Control | 5136 ASD cases 18,237 controls from Sweden | The diagnosis of ASD was based on the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition, Text Revision (DSM-IV-R) | Levels of PM 10 from road traffic were estimated at residential addresses during mother’s pregnancy and the child’s first year of life by dispersion models | Logistic regression model | -municipality -calendar year of birth | -pregnancy -first year of life | No significant association between PM10 and ASD |
| Jung et al., 2013 [39] | Case-Control | 49,073 children from Taiwan | ASD diagnosis according to International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) | Inverse distance weighting method was used to form exposure parameter for PM10 | Cox proportional hazards (PH) model | -age -anxiety -gender -intellectual disabilities -preterm -SES | -postnatal | No significant association between PM10 and ASD during the first for years of life |
| Gong et al., 2014 [38] | Longitudinal cohort | 3426 twins born in Stockholm during 1992–2000 | The diagnosis of ASD was based on the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition, Text Revision (DSM-IV-R) | Residence time-weighted concentrations of PM10 from road traffic were estimated at participants’ addresses using dispersion modeling, controlling for seasonal variation | Multivariate regression models | -parity -gender -maternal age during pregnancy -maternal smoking during pregnancy -maternal marital status at birth year -parental education -family income -neighborhood deprivation at birth year | -pregnancy -year 1 -year 9 | No significant association between PM10 and ASD |
3.2. Association between NO2 and ASD
3.3. Association between O3 and ASD
3.4. Association between SO2 and ASD
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Lai, M.C.; Lombardo, M.V.; Baron-Cohen, S. Autism. Lancet 2014, 383, 896–910. [Google Scholar] [CrossRef]
- Maenner, M.J.; Shaw, K.A.; Baio, J.; Washington, A.; Patrick, M.; Di Rienzo, M.; Christensen, D.L.; Wiggins, L.D.; Pettygrove, S.; Andrews, J.G. Prevalence of autism spectrum disorder among children aged 8 years—Autism and developmental disabilities monitoring network, 11 sites, United States, 2016. MMWR Surveill. Summ. 2020, 69, 1. [Google Scholar]
- Baio, J.; Wiggins, L.; Christensen, D.L.; Maenner, M.J.; Daniels, J.; Warren, Z.; Kurzius-Spencer, M.; Zahorodny, W.; Robinson Rosenberg, C.; White, T. Prevalence of autism spectrum disorder among children aged 8 years—Autism and developmental disabilities monitoring network, 11 sites, United States, 2014. MMWR Surveill. Summ. 2018, 67, 1. [Google Scholar] [CrossRef] [PubMed]
- Christensen, D.L.; Braun, K.V.N.; Baio, J.; Bilder, D.; Charles, J.; Constantino, J.N.; Daniels, J.; Durkin, M.S.; Fitzgerald, R.T.; Kurzius-Spencer, M. Prevalence and characteristics of autism spectrum disorder among children aged 8 years—Autism and developmental disabilities monitoring network, 11 sites, United States, 2012. MMWR Surveill. Summ. 2018, 65, 1. [Google Scholar] [CrossRef] [PubMed]
- Elsabbagh, M.; Divan, G.; Koh, Y.J.; Kim, Y.S.; Kauchali, S.; Marcín, C.; Yasamy, M.T. Global prevalence of autism and other pervasive developmental disorders. Autism Res. 2012, 5, 160–179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®); American Psychiatric Pub: Washington, DC, USA, 2013. [Google Scholar]
- Rice, C.E.; Rosanoff, M.; Dawson, G.; Durkin, M.S.; Croen, L.A.; Singer, A.; Yeargin-Allsopp, M. Evaluating Changes in the Prevalence of the Autism Spectrum Disorders (ASDs). Public Health Rev. 2012, 34, 17. [Google Scholar] [CrossRef] [Green Version]
- Dawson, G.; Bernier, R. A quarter century of progress on the early detection and treatment of autism spectrum disorder. Dev. Psychopathol. 2013, 25 Pt 2, 1455–1472. [Google Scholar]
- Belger, A.; Carpenter, K.L.; Yucel, G.H.; Cleary, K.M.; Donkers, F.C. The neural circuitry of autism. Neurotox. Res. 2011, 20, 201–214. [Google Scholar] [CrossRef] [Green Version]
- Chaste, P.; Leboyer, M. Autism risk factors: Genes, environment, and gene-environment interactions. Dialogues Clin. Neurosci. 2012, 14, 281–292. [Google Scholar]
- Banerjee, S.; Riordan, M.; Bhat, M.A. Genetic aspects of autism spectrum disorders: Insights from animal models. Front. Cell. Neurosci. 2014, 8, 5. [Google Scholar]
- Bourgeron, T. From the genetic architecture to synaptic plasticity in autism spectrum disorder. Nat. Rev. Neurosci. 2015, 16, 551–563. [Google Scholar] [CrossRef] [PubMed]
- Courchesne, E. Brain development in autism: Early overgrowth followed by premature arrest of growth. Ment. Retard. Dev. Disabil. Res. Rev. 2004, 10, 106–111. [Google Scholar] [CrossRef] [PubMed]
- Hertz-Picciotto, I.; Schmidt, R.J.; Krakowiak, P. Understanding environmental contributions to autism: Causal concepts and the state of science. Autism Res. 2018, 11, 554–586. [Google Scholar] [PubMed]
- Lam, J.; Sutton, P.; Kalkbrenner, A.; Windham, G.; Halladay, A.; Koustas, E.; Lawler, C.; Davidson, L.; Daniels, N.; Newschaffer, C.; et al. A Systematic Review and Meta-Analysis of Multiple Airborne Pollutants and Autism Spectrum Disorder. PLoS ONE 2016, 11, e0161851. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grova, N.; Schroeder, H.; Olivier, J.-L.; Turner, J.D. Epigenetic and Neurological Impairments Associated with Early Life Exposure to Persistent Organic Pollutants. Int. J. Genom. 2019, 2019, 1–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buoli, M.; Serati, M.; Caldiroli, A.; Cremaschi, L.; Carlo Altamura, A. Neurodevelopmental versus neurodegenerative model of schizophrenia and bipolar disorder: Comparison with physiological brain development and aging. Psychiatr. Danub. 2017, 29, 24–27. [Google Scholar]
- Calderón-Garcidueñas, L.; Torres-Jardón, R.; Avila-Ramírez, J.; Kulesza, R.J.; Angiulli, A.D. Air pollution and your brain: What do you need to know right now. Prim. Health Care Res. Dev. 2014, 16, 329–345. [Google Scholar] [CrossRef] [Green Version]
- Madrigano, J.; Baccarelli, A.; Mittleman, M.A.; Sparrow, D.; Vokonas, P.S.; Tarantini, L.; Schwartz, J. Aging and epigenetics: Longitudinal changes in gene-specific DNA methylation. Epigenetics 2012, 7, 63–70. [Google Scholar]
- Brockmeyer, S.; D’Angiulli, A. How air pollution alters brain development: The role of neuroinflammation. Transl. Neurosci. 2016, 7, 24–30. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- CEBM Levels of Evidence. 2009. Available online: www.cebm.net/oxford-centre-evidence-based-medicine-levels-evidence-march-2009/ (accessed on 15 July 2020).
- McGuinn, L.A.; Windham, G.C.; Kalkbrenner, A.E.; Bradley, C.; Di, Q.; Croen, L.A.; Fallin, M.D.; Hoffman, K.; Ladd-Acosta, C.; Schwartz, J. Early Life Exposure to Air Pollution and Autism Spectrum Disorder: Findings from a Multisite Case–Control Study. Epidemiology 2020, 31, 103–114. [Google Scholar] [CrossRef] [PubMed]
- McGuinn, L.A.; Windham, G.C.; Messer, L.C.; Di, Q.; Schwartz, J.; Croen, L.A.; Lisa, A.f.; Moody, E.J.; Rappold, A.G.; Richardson, D.B. Air pollution, neighborhood deprivation, and autism spectrum disorder in the Study to Explore Early Development. Environ. Epidemiol. 2019, 3, e067. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, J.A.; Wright, J.M.; Rice, G.; Connolly, N.; Bowers, K.; Anixt, J. Ambient ozone and fine particulate matter exposures and autism spectrum disorder in metropolitan Cincinnati, Ohio. Environ. Res. 2019, 171, 218–227. [Google Scholar] [CrossRef]
- Ritz, B.; Liew, Z.; Yan, Q.; Cui, X.; Virk, J.; Ketzel, M.; Raaschou-Nielsen, O. Air pollution and autism in Denmark. Environ. Epidemiol. 2018, 2, e028. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.; Jin, Z.; Li, S.; Jin, X.; Tong, S.; Liu, S.; Yang, Y.; Huang, H.; Guo, Y. Early life exposure to particulate matter air pollution (PM1, PM2.5 and PM10) and autism in Shanghai, China: A case-control study. Environ. Int. 2018, 121, 1121–1127. [Google Scholar] [CrossRef] [PubMed]
- Raz, R.; Roberts, A.L.; Lyall, K.; Hart, J.E.; Just, A.C.; Laden, F.; Weisskopf, M.G. Autism Spectrum Disorder and Particulate Matter Air Pollution before, during, and after Pregnancy: A Nested Case–Control Analysis within the Nurses’ Health Study II Cohort. Environ. Health Perspect. 2015, 123, 264–270. [Google Scholar] [CrossRef] [PubMed]
- Talbott, E.O.; Arena, V.C.; Rager, J.R.; Clougherty, J.E.; Michanowicz, D.R.; Sharma, R.K.; Stacy, S.L. Fine particulate matter and the risk of autism spectrum disorder. Environ. Res. 2015, 140, 414–420. [Google Scholar] [CrossRef]
- Becerra, T.A.; Wilhelm, M.; Olsen, J.; Cockburn, M.; Ritz, B. Ambient Air Pollution and Autism in Los Angeles County, California. Environ. Health Perspect. 2013, 121, 380–386. [Google Scholar]
- Volk, H.E.; Lurmann, F.; Penfold, B.; Hertz-Picciotto, I.; McConnell, R. Traffic-Related Air Pollution, Particulate Matter, and Autism. JAMA Psychiatry 2013, 70, 71–77. [Google Scholar] [CrossRef]
- Jo, H.; Eckel, S.P.; Wang, X.; Chen, J.-C.; Cockburn, M.; Martinez, M.P.; Chow, T.; Molshatzki, N.; Lurmann, F.W.; Funk, W.E.; et al. Sex-specific associations of autism spectrum disorder with residential air pollution exposure in a large Southern California pregnancy cohort. Environ. Pollut. 2019, 254, 113010. [Google Scholar]
- Pagalan, L.; Bickford, C.; Weikum, W.; Lanphear, B.; Bauer, M.; Lanphear, N.; Hanley, G.E.; Oberlander, T.F.; Winters, M. Association of Prenatal Exposure to Air Pollution with Autism Spectrum Disorder. JAMA Pediatr. 2019, 173, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Guxens, M.; Ghassabian, A.; Gong, T.; Garcia-Esteban, R.; Porta, D.; Giorgis-Allemand, L.; Almqvist, C.; Aranbarri, A.; Beelen, R.; Badaloni, C.; et al. Air Pollution Exposure during Pregnancy and Childhood Autistic Traits in Four European Population-Based Cohort Studies: The ESCAPE Project. Environ. Health Perspect. 2016, 124, 133–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalkbrenner, A.E.; Windham, G.C.; Serre, M.L.; Akita, Y.; Wang, X.; Hoffman, K.; Thayer, B.P.; Daniels, J.L. Particulate Matter Exposure, Prenatal and Postnatal Windows of Susceptibility, and Autism Spectrum Disorders. Epidemiology 2015, 26, 30–42. [Google Scholar] [CrossRef] [PubMed]
- Yousefian, F.; Mahvi, A.H.; Yunesian, M.; Hassanvand, M.S.; Kashani, H.; Amini, H. Long-term exposure to ambient air pollution and autism spectrum disorder in children: A case-control study in Tehran, Iran. Sci. Total Environ. 2018, 643, 1216–1222. [Google Scholar] [CrossRef] [PubMed]
- Gong, T.; Dalman, C.; Wicks, S.; Dal, H.; Magnusson, C.; Lundholm, C.; Almqvist, C.; Pershagen, G. Perinatal Exposure to Traffic-Related Air Pollution and Autism Spectrum Disorders. Environ. Health Perspect. 2017, 125, 119–126. [Google Scholar] [CrossRef] [Green Version]
- Gong, T.; Almqvist, C.; Bölte, S.; Lichtenstein, P.; Anckarsäter, H.; Lind, T.; Lundholm, C.; Pershagen, G. Exposure to air pollution from traffic and neurodevelopmental disorders in Swedish twins. Twin Res. Hum. Genet. 2014, 17, 553–562. [Google Scholar]
- Jung, C.-R.; Lin, Y.-T.; Hwang, B.-F. Air Pollution and Newly Diagnostic Autism Spectrum Disorders: A Population-Based Cohort Study in Taiwan. PLoS ONE 2013, 8, e75510. [Google Scholar] [CrossRef] [Green Version]
- Raz, R.; Levine, H.; Pinto, O.; Broday, D.M.; Yuval; Weisskopf, M.G. Traffic-Related Air Pollution and Autism Spectrum Disorder: A Population-Based Nested Case-Control Study in Israel. Am. J. Epidemiol. 2018, 187, 717–725. [Google Scholar] [CrossRef]
- Goodrich, A.J.; Volk, H.; Tancredi, D.J.; McConnell, R.; Lurmann, F.W.; Hansen, R.L.; Schmidt, R.J. Joint effects of prenatal air pollutant exposure and maternal folic acid supplementation on risk of autism spectrum disorder. Autism Res. 2018, 11, 69–80. [Google Scholar] [CrossRef]
- Oudin, A.; Frondelius, K.; Haglund, N.; Källén, K.; Forsberg, B.; Gustafsson, P.; Malmqvist, E. Prenatal exposure to air pollution as a potential risk factor for autism and ADHD. Environ. Int. 2019, 133, 105149. [Google Scholar] [CrossRef]
- Davis, E.P.; Pfaff, D. Sexually dimorphic responses to early adversity: Implications for affective problems and autism spectrum disorder. Psychoneuroendocrinology 2014, 49, 11–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tau, G.Z.; Peterson, B.S. Normal Development of Brain Circuits. Neuropsychopharmacology 2009, 35, 147–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, X.; Ha, S.U.; Basnet, R. A Review of Epidemiological Research on Adverse Neurological Effects of Exposure to Ambient Air Pollution. Front. Public Health 2016, 4, 157. [Google Scholar] [CrossRef] [Green Version]
- Pope III, C.A.; Coleman, N.; Pond, Z.A.; Burnett, R.T. Fine particulate air pollution and human mortality: 25+ years of cohort studies. Environ. Res. 2020, 183, 108924. [Google Scholar]
- Clifford, A.; Lang, L.; Chen, R.; Anstey, K.J.; Seaton, A. Exposure to air pollution and cognitive functioning across the life course—A systematic literature review. Environ. Res. 2016, 147, 383–398. [Google Scholar] [CrossRef]
- Ailshire, J.; Crimmins, E.M. Fine Particulate Matter Air Pollution and Cognitive Function among Older US Adults. Am. J. Epidemiol. 2014, 180, 359–366. [Google Scholar]
- Luyten, L.J.; Saenen, N.D.; Janssen, B.G.; Vrijens, K.; Plusquin, M.; Roels, H.A.; Debacq-Chainiaux, F.; Nawrot, T.S. Air pollution and the fetal origin of disease: A systematic review of the molecular signatures of air pollution exposure in human placenta. Environ. Res. 2018, 166, 310–323. [Google Scholar] [CrossRef]
- Weitzman, M.; Gortmaker, S.; Sobol, A. Maternal smoking and behavior problems of children. Pediatrics 1992, 90, 342–349. [Google Scholar] [CrossRef]
- Julvez, J.; Ribas-Fitó, N.; Torrent, M.; Forns, M.; Garcia-Esteban, R.; Sunyer, J. Maternal smoking habits and cognitive development of children at age 4 years in a population-based birth cohort. Int. J. Epidemiol. 2007, 36, 825–832. [Google Scholar] [CrossRef] [Green Version]
- Miranda, M.L.; Edwards, S.E.; Keating, M.H.; Paul, C. Making the Environmental Justice Grade: The Relative Burden of Air Pollution Exposure in the United States. Int. J. Environ. Res. Public Health 2011, 8, 1755–1771. [Google Scholar] [CrossRef]
- Briggs, D.J.; de Hoogh, C.; Gulliver, J.; Wills, J.; Elliott, P.; Kingham, S. A regression-based method for mapping traffic-related air pollution: Application and testing in four contrasting urban environments. Sci. Total Environ. 2000, 253, 151–167. [Google Scholar] [CrossRef]
- Gilbert, N.L.; Goldberg, M.S.; Beckerman, B.; Brook, J.R.; Jerrett, M. Assessing Spatial Variability of Ambient Nitrogen Dioxide in Montréal, Canada, with a Land-Use Regression Model. J. Air Waste Manag. Assoc. 2005, 55, 1059–1063. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Panico, A.; Grassi, T.; Bagordo, F.; Idolo, A.; Serio, F.; Tumolo, M.R.; De Giorgi, M.; Guido, M.; Tutino, M.; De Donno, A. Micronucleus Frequency in Exfoliated Buccal Cells of Children Living in an Industrialized Area of Apulia (Italy). Int. J. Environ. Res. Public Health 2020, 17, 1208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Villarini, M.; Levorato, S.; Salvatori, T.; Ceretti, E.; Bonetta, S.; Carducci, A.; Grassi, T.; Vannini, S.; Donato, F.; Bonetta, S.; et al. Buccal micronucleus cytome assay in primary school children: A descriptive analysis of the MAPEC_LIFE multicenter cohort study. Int. J. Hyg. Environ. Health 2018, 221, 883–892. [Google Scholar] [CrossRef] [PubMed]
- Crews, D.; Gillette, R.; Miller-Crews, I.; Gore, A.C.; Skinner, M.K. Nature, nurture and epigenetics. Mol. Cell. Endocrinol. 2014, 398, 42–52. [Google Scholar] [CrossRef] [Green Version]
- Motta, V.; Bonzini, M.; Grevendonk, L.; Iodice, S.; Bollati, V. Epigenetics applied to epidemiology: Investigating environmental factors and lifestyle influence on human health. Med. Lav. 2017, 108, 10–23. [Google Scholar]
- Tumolo, M.R.; Panico, A.; De Donno, A.; Mincarone, P.; Leo, C.G.; Guarino, R.; Bagordo, F.; Serio, F.; Idolo, A.; Grassi, T.; et al. The expression of microRNAs and exposure to environmental contaminants related to human health: A review. Int. J. Environ. Health Res. 2020, 1–23. [Google Scholar] [CrossRef]
- Panico, A.; Tumolo, M.R.; Leo, C.G.; De Donno, A.; Grassi, T.; Bagordo, F.; Serio, F.; Idolo, A.; De Masi, R.; Mincarone, P.; et al. The influence of lifestyle factors on miRNA expression and signal pathways: A review. Epigenomics 2020. [Google Scholar] [CrossRef]
- Kotsyfakis, M.; Patelarou, E. MicroRNAs as biomarkers of harmful environmental and occupational exposures: A systematic review. Biomarkers 2019, 24, 623–630. [Google Scholar]
- Szelenberger, R.; Kacprzak, M.; Saluk-Bijak, J.; Zielinska, M.; Bijak, M. Plasma MicroRNA as a novel diagnostic. Clin. Chim. Acta 2019, 499, 98–107. [Google Scholar] [CrossRef]
- Mandy, W.; Lai, M.-C. Annual Research Review: The role of the environment in the developmental psychopathology of autism spectrum condition. J. Child Psychol. Psychiatry 2016, 57, 271–292. [Google Scholar] [CrossRef] [PubMed]
- Vijayakumar, N.T.; Judy, M. Autism spectrum disorders: Integration of the genome, transcriptome and the environment. J. Neurol. Sci. 2016, 364, 167–176. [Google Scholar] [CrossRef] [PubMed]
- Yu, L.; Wu, Y.; Wu, B. Genetic architecture, epigenetic influence and environment exposure in the pathogenesis of Autism. Sci. China Life Sci. 2015, 58, 958–967. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vasu, M.M.; Sumitha, P.S.; Rahna, P.; Thanseem, I.; Anitha, A. microRNAs in Autism Spectrum Disorders. Curr. Pharm. Des. 2020, 25, 4368–4378. [Google Scholar] [CrossRef] [PubMed]

| Authors and Year | Study Design | Sample Size/Country | ASD Outcome Assessment | Exposure Assessment | Method of Analysis | Adjustment Variables | Time Window of Exposure | Main Findings |
|---|---|---|---|---|---|---|---|---|
| Ritz et al., 2018 [26] | Case-control | 15,387 ASD cases and 68,139 controls from Denmark | ASD diagnosis according to International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) | Exposures estimates provided by the dispersion models (AirGIS) for the detected pollutants (NO2, SO2, PM2.5 and PM10) in relation to the maternal residence during the examined periods | Conditional logistic regression | -parental age -neighborhood -socio-economic indicators -maternal smoking | -pregnancy -9 months after pregnancy | The data obtained showed that exposure during the entire period of pregnancy to NO2 increases the risk of a diagnosis of ASD. In particular, the authors estimated an adjusted ORs for ASD per IQR increase for 11.41 μg/m3 with NO2 of 1.08 (95%CI: 1.01, 1.15) |
| Becerra et al., 2013 [30] | Case-control | 7603 ASD cases and 10 controls per case from Los Angeles, California | The diagnosis of ASD was based on the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition, Text Revision (DSM-IV-R) | Modeled concentrations of PM2.5 from air monitoring station 1993–2006, assigned by residential address at delivery/birth | Conditional logistic regression | -maternal age -maternal place of birth -race -education -type of birth -parity -insurance type -gestational age at birth | -pregnancy | The results obtained highlighted an association between the development of ASD and prenatal exposure to NO2 |
| Volk et al., 2013 [31] | Case-control | 279 ASD cases and 245 controls from California | ASD case classification based on the results from the ADOS (Autism Diagnostic Observation Schedule) and ADI-R (Autism Diagnostic Interview-Revised) | Traffic-related air pollution was assigned to each mother’s location using a line-source air-quality dispersion model | Logistic additive models | -child gender -child ethnicity -maximal education of parents -maternal age -prenatal smoking | -pregnancy -trimester 1, 2, 3, -year 1 | The results confirmed an association in the prenatal period and the risk of ASD with an OR of 1.81 |
| Pagalan et al., 2019 [33] | Cohort | Cohort of 129,439 children: 1276 were diagnosed with ASD from Metro Vancouver, British Columbia, Canada | ASD case classification based on the results from the ADOS (Autism Diagnostic Observation Schedule) and ADI-R (Autism Diagnostic Interview-Revised) | Monthly mean exposures to PM2.5, at the maternal residence during pregnancy were estimated with temporally adjusted, high-resolution land use regression models | Logistic regression model | -child sex -birth month -birth year -maternal age -maternal birthplace -neighborhood level urbanicity and income band. | -pregnancy | No significant association between NO2 and ASD |
| Guxens et al., 2016 [34] | Cohort | 8079 children from four European population-based birth/child cohorts (Sweden, Netherlands, Italy, and Spain) | Autistic traits were assessed in children using: -the Autism Spectrum Disorder module of the Autism—Tics, Attention Deficit and Hyperactivity Disorders, and Other Comorbidities (A-TAC) inventory in the Swedish cohort -the Pervasive Developmental Problems (PDP) subscale of the Child Behavior Checklist for Toddlers in the Dutch cohort and in the Italian cohort -an adapted 18-item version of the Social Responsiveness Scale (SRS) in the Dutch cohort at age 6 years; -the Childhood Autism Spectrum Test (CAST) in the Spanish cohorts | PM2.5 absorbance was estimated for birth addresses by land-use regression models based on monitoring campaigns performed between 2008 and 2011. Levels of exposures were extrapolated back in time to exact pregnancy periods | Logistic regression model | -age at delivery -educational level -country of birth -prenatal smoking -parity -maternal height -pre-pregnancy weight -pre-pregnancy body mass index -child’s sex -date of birth -child’s age at autistic trait assessment -information on the evaluator of the autistic traits -urbanity at child’s birth address | -pregnancy | No significant association between NO2 and ASD |
| Jung et al., 2013 [39] | Case-Control | 49,073 children from Taiwan | ASD diagnosis according to International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) | Inverse distance weighting method was used to form exposure parameter for PM10 | Cox proportional hazards (PH) model | -age -anxiety -gender -intellectual disabilities -preterm -SES | -postnatal | The study provided evidence of association between NO2 in the first 4 years of life and an increased risk of ASD |
| Gong et al., 2014 [38] | Longitudinal cohort | 3426 twins born in Stockholm during 1992–2000 | The diagnosis of ASD was based on the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition, Text Revision (DSM-IV-R) | Residence time-weighted concentrations of PM10 from road traffic were estimated at participants’ addresses using dispersion modeling, controlling for seasonal variation | Multivariate regression models | -parity -gender -maternal age during pregnancy -maternal smoking during pregnancy -maternal marital status at birth year -parental education -family income -neighborhood deprivation at birth year | -pregnancy -year 1 -year 9 | No significant association between NO2 and ASD |
| Goodrich et al., 2018 [41] | Case-Control | 346 ASD cases and 260 controls from California | ASD case classification based on the results from the ADOS (Autism Diagnostic Observation Schedule) and ADI-R (Autism Diagnostic Interview-Revised) | Estimates of exposure to near roadway air pollution (NRP) and criteria air pollutant measures were assigned based on maternal residential history | Logistic regression model | -self-reported FA intake for each month of pregnancy | -pregnancy -trimester 1, 2, 3 | This study showed that taking folic acid during pregnancy reduces the risk of ASD among those exposed to prenatal high NO2 levels |
| Raz et al., 2018 [40] | Case-Control | 2098 ASD cases and 54,191 controls from Israel | The diagnosis of ASD was based on the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition, Text Revision (DSM-IV-R) | NO2 Exposure was based on an optimized dispersion model | Logistic regression | -year of birth -calendar month of birth -population group -paternal age -socioeconomic status | -pre-conception -pregnancy -9 months after birth | Postnatal exposure to NO2 is associated with an increased risk of ASD diagnosis with values of 1.40 (95%CI: 1.09, 1.80) per IQR increase for 5.85 ppb |
| Oudin et al., 2019 [42] | Longitudinal cohort | 48,571 children born between 1999 and 2009 in southern Sweden | ASD diagnosis according to International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) | Modelled nitrogen oxide (NOx) levels derived from a Gaussian dispersion model | Logistic regression model | -maternal residency during pregnancy -perinatal factors collected from a regional birth registry -socio-economic factors | -pregnancy | Positive associations between NOx exposure during pregnancy and ASD with an adjusted Odds Ratio (OR) of 1.40 (95%CI: 1.02–1.93) |
| Authors and Year | Study Design | Sample Size/Country | ASD Outcome Assessment | Exposure Assessment | Method of Analysis | Adjustment Variables | Time Window of Exposure | Main Findings |
|---|---|---|---|---|---|---|---|---|
| McGuinn et al., 2020 [23] | Case-control | 674 ASD cases and 855 controls fromCalifornia, Colorado, Georgia, Maryland, North Carolina, and Pennsylvania | ASD case classification based on the results from the ADOS (Autism Diagnostic Observation Schedule) and ADI-R (Autism Diagnostic Interview-Revised) | Satellite-based model to assign air pollutant exposure (PM2.5, O3) averages during several critical periods of neurodevelopment | Logistic regression model | -study site -maternal age -maternal education -maternal race -maternal smoking, -month and year of birth | -3 months before pregnancy -each trimester of pregnancy -the entire pregnancy -first year of life | There was a variation by exposure time period for the O3–ASD relation, with a stronger association observed during the third trimester of pregnancy and an OR of 1.2 (95%CI: 1.1, 1.4) per 6.6 ppb increase in O3 |
| Kaufman et al., 2019 [25] | Case-control | 428 ASD cases and 6420 controls from metropolitan Cincinnati area in southwest Ohio | ASD diagnosis according to International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) | Daily PM2.5 individual exposure estimations provided by the United States Environmental Protection Agency (US EPA), based on their residential address | Logistic regression model | -maternal and birth-related confounders -multiple temporal exposure windows | -each trimester pregnancy -first year of life -second year of life | Positive association with O3 exposure during the 2nd year of life (OR range across categories: (1.29–1.42) |
| Becerra et al., 2013 [30] | Case-control | 7603 ASD cases and 10 controls per case from Los Angeles, California | The diagnosis of ASD was based on the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition, Text Revision (DSM-IV-R) | Modeled concentrations of PM2.5 from air monitoring station 1993–2006, assigned by residential address at delivery/birth | Conditional logistic regression | -maternal age -maternal place of birth -race -education -type of birth -parity -insurance type -gestational age at birth | -pregnancy | Positive association with O3 during pregnancy and ASD. 1.12 (95%CI, 1.06, 1.19) per 11.54 ppb increase in O3 |
| Jo et al., 2019 [32] | Cohort | 246,420 children from Southern California | ASD diagnosis according to International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) | PM2.5 measured at regulatory air monitoring stations was interpolated to estimate exposures during preconception and each pregnancy trimester, and first year of life at each child’s birth address | Cox regression models | -birth year -relevant maternal and child characteristics | -preconception -trimester 1,2,3 -year 1 | No significant association between O3 and ASD |
| Jung et al., 2013 [39] | Case-Control | 49,073 children from Taiwan | ASD diagnosis according to International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) | Inverse distance weighting method was used to form exposure parameter for PM10 | Cox proportional hazards (PH) model | -age -anxiety -gender -intellectual disabilities -preterm -SES | -postnatal | The study suggested an association between O3 exposure in the first for years of life and ASD |
| Authors and Year | Study Design | Sample Size/Country | ASD Outcome Assessment | Exposure Assessment | Method of Analysis | Adjustment Variables | Time Window of Exposure | Main Findings |
|---|---|---|---|---|---|---|---|---|
| Ritz et al., 2018 [26] | Case-control | 15,387 ASD cases and 68,139 controls from Denmark | ASD diagnosis according to International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) | Exposures estimates provided by the dispersion models (AirGIS) for the detected pollutants (NO2, SO2, PM2.5 and PM10) in relation to the maternal residence during the examined periods | Conditional logistic regression | -parental age -neighborhood -socio-economic indicators -maternal smoking | -pregnancy -9 months after pregnancy | The authors estimated an OR of 1.21 (95%CI: 1.13, 1.29) for ASD onset per each increase of 2.8 μg/m3 SO2 in IQR value, 9 months after pregnancy |
| Yousefian et al., 2018 [36] | Case-Control | 134 ASD cases and 388 controls from Tehran, Iran | The diagnosis of ASD was based on the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition, Text Revision (DSM-IV-R) | Land-use regression models were used to estimate their annual mean exposure to ambient PM10 | Logistic regression | -maternal age at birth -maternal education -paternal education -cousin marriage -maternal smoking during pregnancy -birth order -gestational age (weeks) -multiple births -maternal disease -paternal disease | -pregnancy | No significant association between SO2 and ASD |
| Jung et al., 2013 [39] | Case-Control | 49,073 children from Taiwan | ASD diagnosis according to International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM). | Inverse distance weighting method was used to form exposure parameter for PM10 | Cox proportional hazards (PH) model | -age -anxiety -gender -intellectual disabilities -preterm -SES | -postnatal | The researchers highlighted a 17% increased risk for ASD per each increase of 1 ppb in SO2 levels (95%CI 1.09–1.27) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Imbriani, G.; Panico, A.; Grassi, T.; Idolo, A.; Serio, F.; Bagordo, F.; De Filippis, G.; De Giorgi, D.; Antonucci, G.; Piscitelli, P.; et al. Early-Life Exposure to Environmental Air Pollution and Autism Spectrum Disorder: A Review of Available Evidence. Int. J. Environ. Res. Public Health 2021, 18, 1204. https://doi.org/10.3390/ijerph18031204
Imbriani G, Panico A, Grassi T, Idolo A, Serio F, Bagordo F, De Filippis G, De Giorgi D, Antonucci G, Piscitelli P, et al. Early-Life Exposure to Environmental Air Pollution and Autism Spectrum Disorder: A Review of Available Evidence. International Journal of Environmental Research and Public Health. 2021; 18(3):1204. https://doi.org/10.3390/ijerph18031204
Chicago/Turabian StyleImbriani, Giovanni, Alessandra Panico, Tiziana Grassi, Adele Idolo, Francesca Serio, Francesco Bagordo, Giovanni De Filippis, Donato De Giorgi, Gianfranco Antonucci, Prisco Piscitelli, and et al. 2021. "Early-Life Exposure to Environmental Air Pollution and Autism Spectrum Disorder: A Review of Available Evidence" International Journal of Environmental Research and Public Health 18, no. 3: 1204. https://doi.org/10.3390/ijerph18031204
APA StyleImbriani, G., Panico, A., Grassi, T., Idolo, A., Serio, F., Bagordo, F., De Filippis, G., De Giorgi, D., Antonucci, G., Piscitelli, P., Colangelo, M., Peccarisi, L., Tumolo, M. R., De Masi, R., Miani, A., & De Donno, A. (2021). Early-Life Exposure to Environmental Air Pollution and Autism Spectrum Disorder: A Review of Available Evidence. International Journal of Environmental Research and Public Health, 18(3), 1204. https://doi.org/10.3390/ijerph18031204