
Pathways among Frailty, Health Literacy, Acculturation, and Social Support of Middle-Aged and Older Korean Immigrants in the USA


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Data Collection
2.3. Theoretical Framework
2.4. Measures
2.5. Data Analysis
3. Results
3.1. Characteristics of Participants
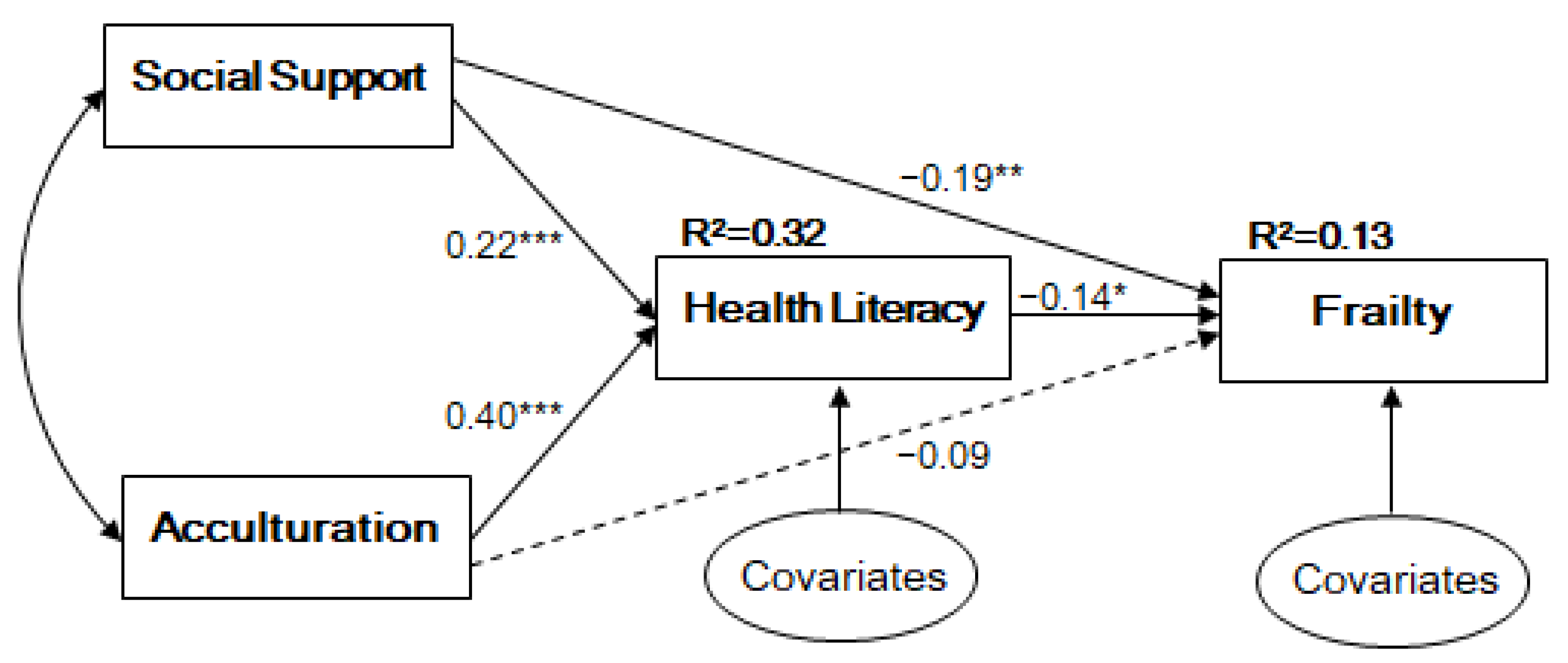
3.2. Path Analysis
3.3. Mediating Effect of Health Literacy
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Fried, L.P.; Ferrucci, L.; Darer, J.; Williamson, J.D.; Anderson, G. Untangling the concepts of disability, frailty, and comorbidity: Implications for improved targeting and care. J. Gerontol. A Biol. Sci. Med. Sci. 2004, 59, 255–263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanlon, P.; Nicholl, B.I.; Jani, B.D.; Lee, D.; McQueenie, R.; Mair, F.S. Frailty and pre-frailty in middle-aged and older adults and its association with multimorbidity and mortality: A prospective analysis of 493 737 UK Biobank participants. Lancet Public Health 2018, 3, 323–332. [Google Scholar] [CrossRef]
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in elderly people. Lancet 2013, 2, 752–762. [Google Scholar] [CrossRef] [Green Version]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Cardiovascular Health Study Collaborative Research Group. Frailty in older adults: Evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, 146–156. [Google Scholar] [CrossRef] [PubMed]
- Gealey, S.G. Quantification of the term frail as applied to the elderly client. J. Am. Acad. Nurse Pract. 1997, 9, 505–510. [Google Scholar] [CrossRef]
- Brown, I.; Renwick, R.; Raphael, D. Frailty: Constructing a common meaning, definition, and conceptual framework. Int. J. Rehabil. Res. 1995, 18, 93–102. [Google Scholar] [CrossRef]
- Khezrian, M.; Myint, P.K.; McNeil, C.; Murray, A.D. A review of frailty syndrome and its physical, cognitive and emotional domains in the elderly. Geriatrics 2017, 2, 36. [Google Scholar] [CrossRef] [Green Version]
- Collard, R.M.; Boter, H.; Schoevers, R.A.; Oude Voshaar, R.C. Prevalence of frailty in community-dwelling older persons: A systematic review. J. Am. Geriatr. Soc. 2012, 60, 1487–1492. [Google Scholar] [CrossRef]
- Morley, J.E.; Malmstrom, T.; Miller, D. A simple frailty questionnaire (FRAIL) predicts outcomes in middle aged African Americans. J. Nutr. Health Aging 2012, 16, 601–608. [Google Scholar] [CrossRef] [Green Version]
- Sørensen, K.; Van den Broucke, S.; Fullam, J.; Doyle, G.; Pelikan, J.; Slonska, Z.; Brand, H. Health literacy and public health: A systematic review and integration of definitions and models. BMC Public Health 2012, 12, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Parker, R. Health literacy: A challenge for American patients and their health care providers. Health Prompt. Int. 2000, 15, 277–283. [Google Scholar] [CrossRef] [Green Version]
- Berkman, N.D.; Sheridan, S.L.; Donahue, K.E.; Halpern, D.J.; Crotty, K. Low health literacy and health outcomes: An updated systematic review. Ann. Intern. Med. 2011, 155, 97–107. [Google Scholar] [CrossRef] [PubMed]
- Bostock, S.; Steptoe, A. Association between low functional health literacy and mortality in older adults: Longitudinal cohort study. BMJ 2012, 344, e1602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kutner, M.; Greenberg, E.; Jin, Y.; Paulsen, C. The Health Literacy of America’s Adults: Results from the 2003 National Assessment of Adult Literacy; U.S. Department of Education: Washington, DC, USA, 2006; pp. 1–76.
- HLCE. Available online: http://healthliteracycentre.eu/all-about-hlce/the-hl-model-result-irohla/ (accessed on 29 September 2020).
- Brach, C.; Agency for Healthcare Research and Quality; Keller, D.; Hernandez, L.; Baur, C.; Parker, R.; Dreyer, B.; Schyve, P.; Lemerise, A.J.; Schillinger, D.; et al. Ten attributes of health literate health care organizations. NAM Perspect. 2012, 1–26. [Google Scholar] [CrossRef]
- Huang, C.H.; Lai, Y.-C.; Lee, Y.C.; Teong, X.T.; Kuzuya, M.; Kuo, K.-M. Impact of health literacy on frailty among community-dwelling seniors. J. Clin. Med. 2018, 7, 481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shirooka, H.; Nishiguchi, S.; Fukutani, N.; Adachi, D.; Tashiro, Y.; Hotta, T.; Morino, S.; Nozaki, Y.; Hirata, H.; Yamaguchi, M.; et al. Association between comprehensive health literacy and frailty level in community-dwelling older adults: A cross-sectional study in Japan. Geriatr. Gerontol. Int. 2017, 17, 804–809. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.; Ferri-Guerra, J.; Nadeem, M.Y.; Salguero, D.; Aparicio-Ugarriza, R.; Desir, M.; Ruiz, J.G. The association of health literacy, numeracy and graph literacy with frailty. Aging Clin. Exp. Res. 2019, 31, 1827–1832. [Google Scholar] [CrossRef]
- Park, S.Y.; Lee, H.; Kang, M. Factors affecting health literacy among immigrants—Systematic review. Eur. J. Public Health 2018, 28, 214–283. [Google Scholar] [CrossRef]
- Derose, K.P.; Escarce, J.J.; Lurie, N. Immigrants and health care: Sources of vulnerability. Health Aff. (Millwood) 2007, 26, 1258–1268. [Google Scholar] [CrossRef]
- Cordasco, K.M.; Asch, S.M.; Franco, I.; Mangione, C.M. Health literacy and English language comprehension among elderly inpatients at an urban safety-net hospital. J. Health Hum. Serv. Adm. 2009, 32, 30–50. [Google Scholar]
- Tennstedt, S.L.; Sullivan, L.M.; McKinlay, J.B.; D’Agostino, R.B. How important is functional status as a predictor of service use by older people? J. Aging. Health 1990, 2, 439–461. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.Y.D.; Gazmararian, J.A.; Arozullah, A.M. Health literacy and social support among elderly Medicare enrollees in a managed care plan. J. Appl. Gerontol. 2006, 25, 324–337. [Google Scholar] [CrossRef]
- Gracie, B.; Moon, S.S.; Basham, R. Inadequate health literacy among elderly immigrants: Characteristics, contributing, and service utilization factors. J. Hum. Behav. Soc. Environ. 2012, 22, 875–895. [Google Scholar] [CrossRef]
- Kim, B.J.; Sangalang, C.C.; Kihl, T. Effects of acculturation and social network support on depression among elderly Korean immigrants. Aging Ment. Health 2012, 16, 787–794. [Google Scholar] [CrossRef] [PubMed]
- Graves, T.D. Psychological Acculturation in a Tri-Ethnic Community. Southwest J. Anthr. 1967, 23, 337–350. [Google Scholar] [CrossRef]
- Gibson, M.A. Immigrant Adaptation and Patterns of Acculturation. Hum. Dev. 2001, 44, 19–23. [Google Scholar] [CrossRef]
- Mui, A.C.; Kang, S.-Y. Acculturation stress and depression among Asian immigrant elders. Soc. Work 2006, 51, 243–255. [Google Scholar] [CrossRef] [Green Version]
- Chao, Y.Y.; Katigbak, C.; Zhang, N.J.; Dong, X. Association between perceived social support and depressive symptoms among community-dwelling older Chinese Americans. Gerontol. Geriatr. Med. 2018, 4, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Li, C.C.; Matthews, A.K.; Dong, X. The influence of health literacy and acculturation on cancer screening behaviors among older Chinese Americans. Gerontol. Geriatr. Med. 2018, 4, 1–8. [Google Scholar] [CrossRef]
- Kline, R.B. Principles and Practice of Structural Equation Modeling, 4th ed.; Guilford Press: New York, NY, USA, 2016; pp. 1–534. [Google Scholar]
- Redfield, R.; Linton, R.; Herskovits, M.J. Memorandum for the study of acculturation. Am. Anthropol. 1936, 38, 149–152. [Google Scholar] [CrossRef]
- Jung, H.W.; Yoo, H.J.; Park, S.Y.; Kim, S.W.; Choi, J.Y.; Yoon, S.J.; Kim, C.H.; Kim, K.I. The Korean version of the FRAIL scale: Clinical feasibility and validity of assessing the frailty status of Korean elderly. Korean J. Intern. Med. 2016, 31, 594–600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abellan van Kan, G.; Rolland, Y.; Morley, J.E.; Vellas, B. Frailty: Toward a clinical definition. J. Am. Med. Dir. Assoc. 2008, 9, 71–72. [Google Scholar] [CrossRef] [PubMed]
- Finbråten, H.S.; Wilde-Larsson, B.; Nordström, G.; Pettersen, K.S.; Trollvik, A.; Guttersrud, Ø. Establishing the HLS-Q12 short version of the European Health Literacy Survey Questionnaire: Latent trait analyses applying Rasch modelling and confirmatory factor analysis. BMC Health Serv. Res. 2018, 18, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Choi, J.; Park, D.J. The relationship between sub-dimensions of health literacy and health-related behaviors among Korean adults. Health Soc. Welf. Rev. 2019, 39, 334–364. [Google Scholar] [CrossRef]
- Sørensen, K.; Van den Broucke, S.; Pelikan, J.M.; Fullam, J.; Doyle, G.; Slonska, Z.; Kondilis, B.; Stoffels, V.; Osborne, R.H.; Brand, H.; et al. Measuring health literacy in populations: Illuminating the design and development process of the European Health Literacy Survey Questionnaire (HLS-EU-Q). BMC Public Health 2013, 13, 948. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zimet, G.D.; Dahlem, N.W.; Zimet, S.G.; Farley, G.K. The multidimensional scale of perceived social support. J. Pers. Assess 1988, 52, 30–41. [Google Scholar] [CrossRef] [Green Version]
- Barry, D.T. Development of a new scale for measuring acculturation: The East Asian Acculturation Measure (EAAM). J. Immigr. Health 2001, 3, 193–197. [Google Scholar] [CrossRef]
- Krause, M.R.; Serlin, R.C.; Ward, S.E.; Rony, R.Y.Z.; Ezenwa, M.O.; Naab, F. Testing mediating in nursing research: Beyond baron and kenny. Nurs Res. 2010, 59, 288–294. [Google Scholar] [CrossRef]
- Hooper, D.; Coughlan, J.; Mullen, M. Structural equation modeling: Guidelines for determining model fit. Electron. J. Bus. Res. Meth. 2008, 6, 53–60. [Google Scholar] [CrossRef]
- Brothers, T.D.; Theou, O.; Rockwood, K. Frailty and migration in middle-aged and older Europeans. Arch Gerontol. Geriatr. 2014, 58, 63–68. [Google Scholar] [CrossRef]
- Liu, Y.-B.; Hou, P.; Xue, H.-P.; Mao, X.-E.; Li, Y.-N. Social support, health literacy, and health care utilization among older adults. Asia Pac. J. Public Health 2019, 31, 359–366. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.Y.D.; Arozullah, A.M.; Cho, Y.I.; Crittenden, K.; Vicencio, D. Health literacy, social support, and health status among older adults. Educ. Gerontol. 2009, 35, 191–201. [Google Scholar] [CrossRef]
- Pew Research Center. Available online: https://www.pewresearch.org/hispanic/2020/08/20/facts-on-u-s-immigrants/ (accessed on 24 November 2020).


{kind=link}
| Variables | Category | N (%) or M ± SD |
|---|---|---|
| Age | Total | 64.05 ± 9.46 |
| 50–59 | 96 (39.3) | |
| 60–69 | 71 (29.1) | |
| 70≤ | 77 (31.6) | |
| Gender | Male | 119 (48.8) |
| Female | 125 (51.2) | |
| Length of residency (years) | <5 | 4 (1.6) |
| 5≤~<10 | 44 (18.0) | |
| 10≤~<15 | 60 (24.6) | |
| 15≤ | 136 (55.7) | |
| Educational attainment | Middle | 16 (6.6) |
| High | 72 (29.5) | |
| Bachelor | 114 (46.7) | |
| Graduate | 42 (17.2) | |
| Monthly income (dollars) | None | 17 (7.0) |
| <1000 | 34 (13.9) | |
| 1000≤~<3000 | 65 (26.6) | |
| 3000≤~<5000 | 64 (26.2) | |
| >5000 | 63 (25.8) | |
| Acculturation (range: 1–7) | Total | 3.83 ± 0.66 |
| Assimilation | 2.25 ± 1.08 | |
| Separation | 5.14 ± 0.94 | |
| Integration | 3.29 ± 1.16 | |
| Marginalization | 3.15 ± 0.95 | |
| Social support (range: 1–7) | 5.32 ± 1.02 | |
| Health literacy (range: 1–4) | 2.55 ± 0.59 | |
| Frailty | Robust | 143 (58.6) |
| Prefrail | 87 (35.7) | |
| Frail | 14 (5.7) |
| Variable | Acculturation | Social Support | Health Literacy | Frailty |
|---|---|---|---|---|
| Acculturation | 1.00 | 0.32 *** | 0.42 *** | −0.25 *** |
| Social support | 1.00 | 0.51 *** | −0.23 *** | |
| Health literacy | 1.00 | −0.28 *** | ||
| Frailty | 1.00 |
| Model Pathway | β | S.E. | p | ||
|---|---|---|---|---|---|
| Health literacy | ← | Acculturation | 0.40 | 0.06 | <0.001 |
| Social support | 0.22 | 0.05 | <0.001 | ||
| Gender | 0.03 | 0.05 | 0.518 | ||
| Length of residency | 0.16 | 0.05 | 0.003 | ||
| Frailty | ← | Health literacy | −0.14 | 0.07 | 0.032 |
| Acculturation | −0.09 | 0.08 | 0.253 | ||
| Social support | −0.19 | 0.07 | 0.009 | ||
| Age | 0.12 | 0.08 | 0.149 | ||
| Gender | −0.05 | 0.07 | 0.472 | ||
| Income | 0.08 | 0.07 | 0.280 | ||
| Length of residency | 0.08 | 0.07 | 0.278 | ||
| Model fit indices | χ2 (2) = 2.144 (p = 0.342), RMSEA = 0.017, CFI = 0.999, TLI = 0.991, SRMR = 0.020 | ||||
| Model Pathway | Effect | β | S.E. | p |
|---|---|---|---|---|
| Frailty ← Social support | Total | −0.22 | 0.07 | 0.003 |
| Indirect | −0.03 | 0.02 | 0.045 | |
| Direct | −0.19 | 0.07 | 0.009 | |
| Frailty ← Acculturation | Total | −0.15 | 0.07 | 0.038 |
| Indirect | −0.06 | 0.03 | 0.048 | |
| Direct | −0.09 | 0.08 | 0.253 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sagong, H.; Yoon, J.Y. Pathways among Frailty, Health Literacy, Acculturation, and Social Support of Middle-Aged and Older Korean Immigrants in the USA. Int. J. Environ. Res. Public Health 2021, 18, 1245. https://doi.org/10.3390/ijerph18031245
Sagong H, Yoon JY. Pathways among Frailty, Health Literacy, Acculturation, and Social Support of Middle-Aged and Older Korean Immigrants in the USA. International Journal of Environmental Research and Public Health. 2021; 18(3):1245. https://doi.org/10.3390/ijerph18031245
Chicago/Turabian StyleSagong, Hae, and Ju Young Yoon. 2021. "Pathways among Frailty, Health Literacy, Acculturation, and Social Support of Middle-Aged and Older Korean Immigrants in the USA" International Journal of Environmental Research and Public Health 18, no. 3: 1245. https://doi.org/10.3390/ijerph18031245
APA StyleSagong, H., & Yoon, J. Y. (2021). Pathways among Frailty, Health Literacy, Acculturation, and Social Support of Middle-Aged and Older Korean Immigrants in the USA. International Journal of Environmental Research and Public Health, 18(3), 1245. https://doi.org/10.3390/ijerph18031245