Community-Based Approaches to Reducing Health Inequities and Fostering Environmental Justice through Global Youth-Engaged Citizen Science

 , , , , , , ,
, , , , , , ,  , , , , and add
Show full author list
, , , , and add
Show full author list
Abstract
:1. Introduction
2. Methods and Materials for the Our Voice Citizen Science Engagement Model
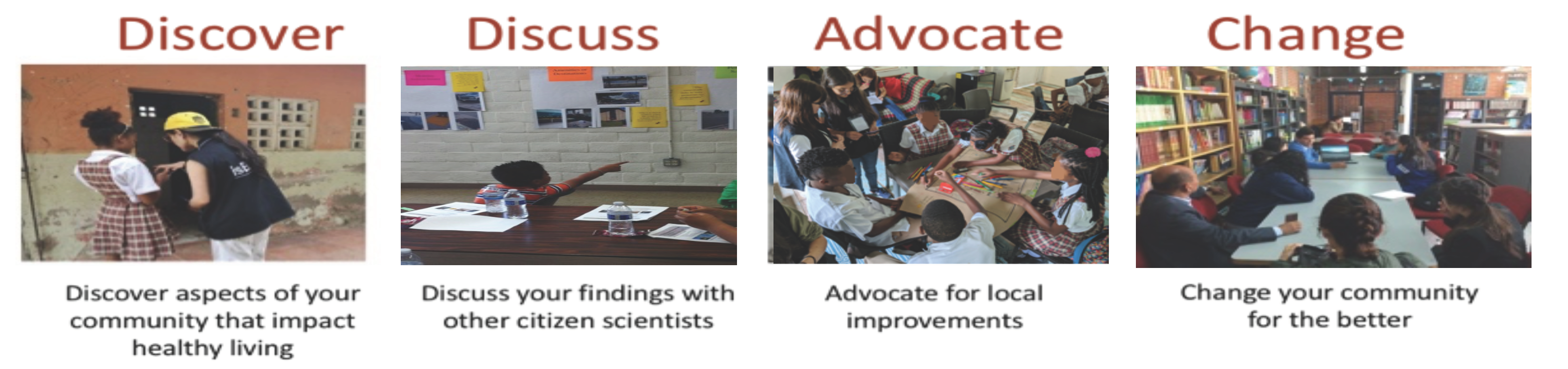
2.1. Overview
2.2. Description of Our Voice Research Projects Aimed at Youth and Young Adult Populations
3. Results
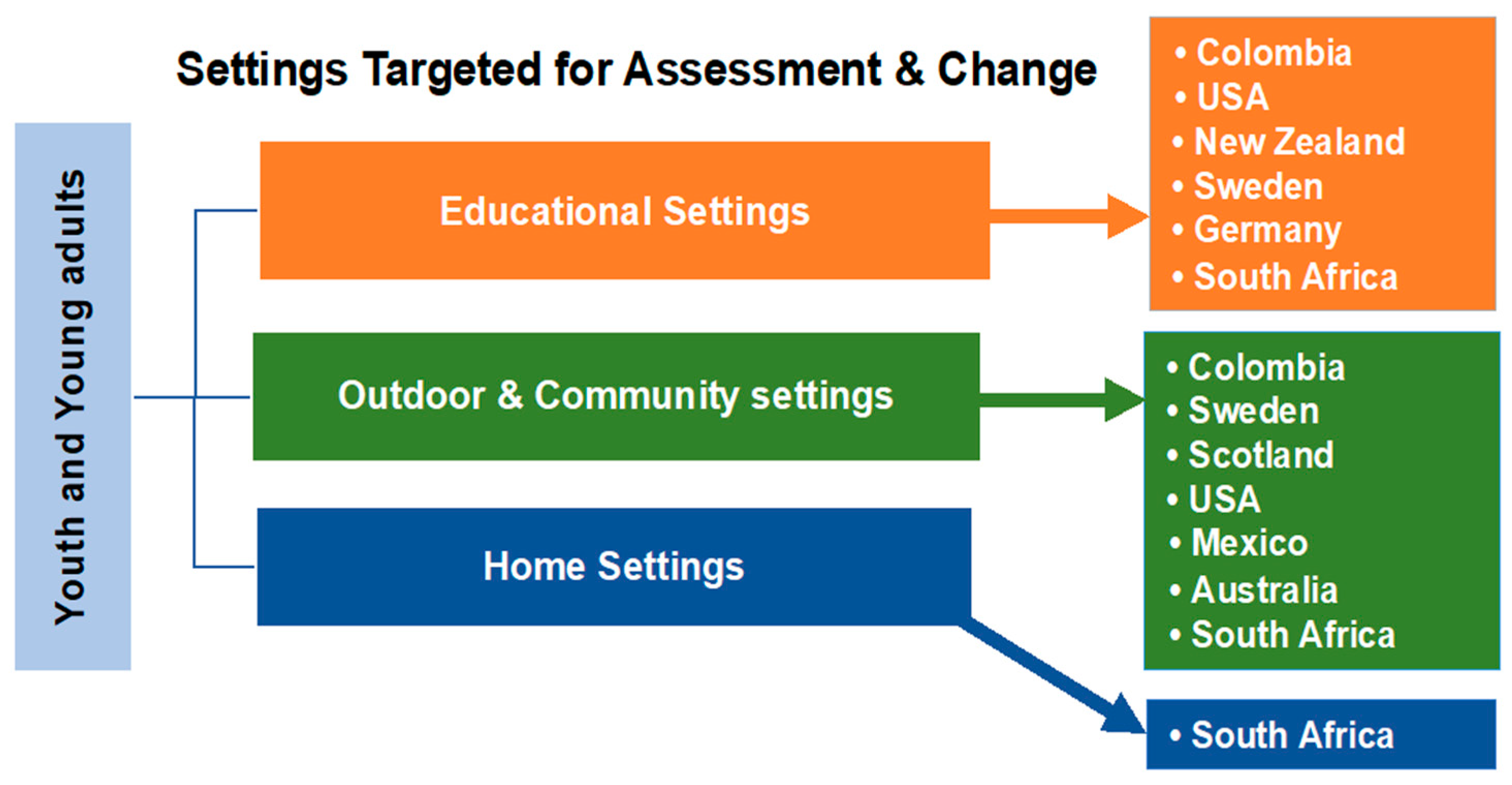
3.1. Summary of Our Voice Youth and Young Adult Projects Completed or in Process
3.2. Intra-Generational Youth Projects in Educational Settings
3.3. Young Adult Projects in Educational Settings
3.4. Inter-Generational Youth Projects in Educational Settings
3.5. Intra-Generational Youth and Young Adult Projects in Outdoor and Community Settings
3.6. Inter-Generational Projects in Outdoor and Community Settings
Addressing Disparities beyond Clinic Walls through Clinic-Community Citizen Science

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Community Features Identified | Strategies Proposed and Changes Enacted | ||||
|---|---|---|---|---|---|
| Positive | Negative | ||||
| Intra-Generational Youth Projects | |||||
| Gilroy, CA (USA) Safe Routes to Middle School [61] | Ethnically diverse school children in grades 6 to 8 from Gilroy, CA (total city population = 53,231); (N = 26 children participated, ages 12–13 yrs., 70% girls) |
|
|
| |
| Bogotá, Colombia Building Healthy Schools through Technology-enabled Citizen Science [58] | 5 urban public schools teaching grades elementary through high school (N = 97 youth participated, ages 9–18, mean age = 13.4 + 2.2 yrs., 64.9% girls) |
|
|
| |
| Barú, Colombia Enhancing Within-School environments [59] | 1 rural public high school (N = 11 adolescents, ages 13–17, 73% girls) |
|
|
| |
| Barú, Colombia Enhancing Neighborhood environments surrounding schools [59] | 1 rural public high school (N = 12 adolescents, ages 13–17, 67% girls) |
|
|
| |
| Västerås, Sweden Capturing prerequisites for safe physical activity among low-SES adolescents [75,76] | Adolescents (N = 24) ages 16–19 (mean age = 16.6 ± 0.8 years, 75% females) from deprived neighborhoods |
|
|
| |
| Auckland, NZ Empowering children to influ-ence changes in school environ-ments for learning, PA, health, wellbeing [60] | Intermediate (middle) school age children in Years 7 & 8 (10–13 years); N = 241 |
|
|
| |
| Glasgow, Scotland Enhancing urban green and blue spaces [64] | Environmental afterschool club in most deprived area of Glasgow; children from 3 elementary schools (N = 18, 48% Girls, age 8–10) took part in data collection, group discussions & recom-mendations; targeted area was the North Glasgow Canal corridor |
|
|
| |
| Inter-Generational Youth Projects | |||||
| Gilroy, CA (USA) Safe Routes to Elementary School (SRTS) [61] | Prospective controlled comparison design involving 2 schools; parents of ethnically diverse elementary school children (grades 6 to 8) from Gilroy, CA (total city pop. = 53,231) N = 6 parents ages 46–49 yrs. (83% women) in School A participated |
|
|
| |
| North Fair Oaks, CA (USA) Neighborhood walkability and security across generations [79] | Assessment of neighborhood built-environment features that help or hinder physical activity (N = 10 adults, mean age 71.3 ± 6.5 yrs.; and 10 adolescent, low-income Latinx; mean age 12.8 ± 0.6 yrs.); 60% of adolescents & all adults female |
|
|
| |
| Cuernavaca, Mexico Supporting intergenerational active living across socio-economic strata [78] | Tested acceptability and feasibility of using Our Voice method to assess walkability environments in four Mexican neighbor-hoods stratified by socioeconomic status & walkability; (N = 32 adults, mean age = 57.3 ± 8.7 yrs., 9 adolescents mean age = 13.3 ± 1.6 yrs.) |
|
|
| |
| Los Altos, CA USA Multi-sectoral impacts of Pop-Up Parks in an urban setting [80] | Multi-generational community residents (N = 9), with four <17 yrs. old; 88% female; collected data before, during & after pop-up park availability |
|
|
| |
| College-Age/Young Adult Projects | |||||
| Palo Alto, CA USA Addressing gender-based violence on college campuses [68] | Feasibility study translating Our Voice model to gender-based violence field; focus on campus social spaces creating comfortable or uncomfortable contexts; Participants = 10 under-graduate women ages 18–20 yrs. |
|
|
| |
| Auckland, NZ Student voices: What features of the university campus environment influence physical activity and eating habits in University students? [70] | Ethnically diverse university students (aged 17–50 years) across 4 university campus sites in Auckland (locations: North, South, City, Millennium) N = 81 (55 F; 26 M) who completed campus walks; 21 (19 F; 2 M) participated in action groups (n = 3 groups) |
|
|
| |
| Palo Alto, CA USA Promoting gender equity on college campuses [81] | Assessed access to single-occupant all-gender restrooms on Stanford Univ. main campus, Medical School, School of Edu-cation & Graduate Busi-ness School by staff, undergraduate & graduate students, community members (N = 23; ages 18–66, mean age 33 years) |
|
|
| |
| Palo Alto, CA USA Enhancing mental health among graduate students, including during COVID-19 pandemic [72] | Graduate students (N = 7) representing PhD, masters and professional programs (29% women) |
|
|
| |
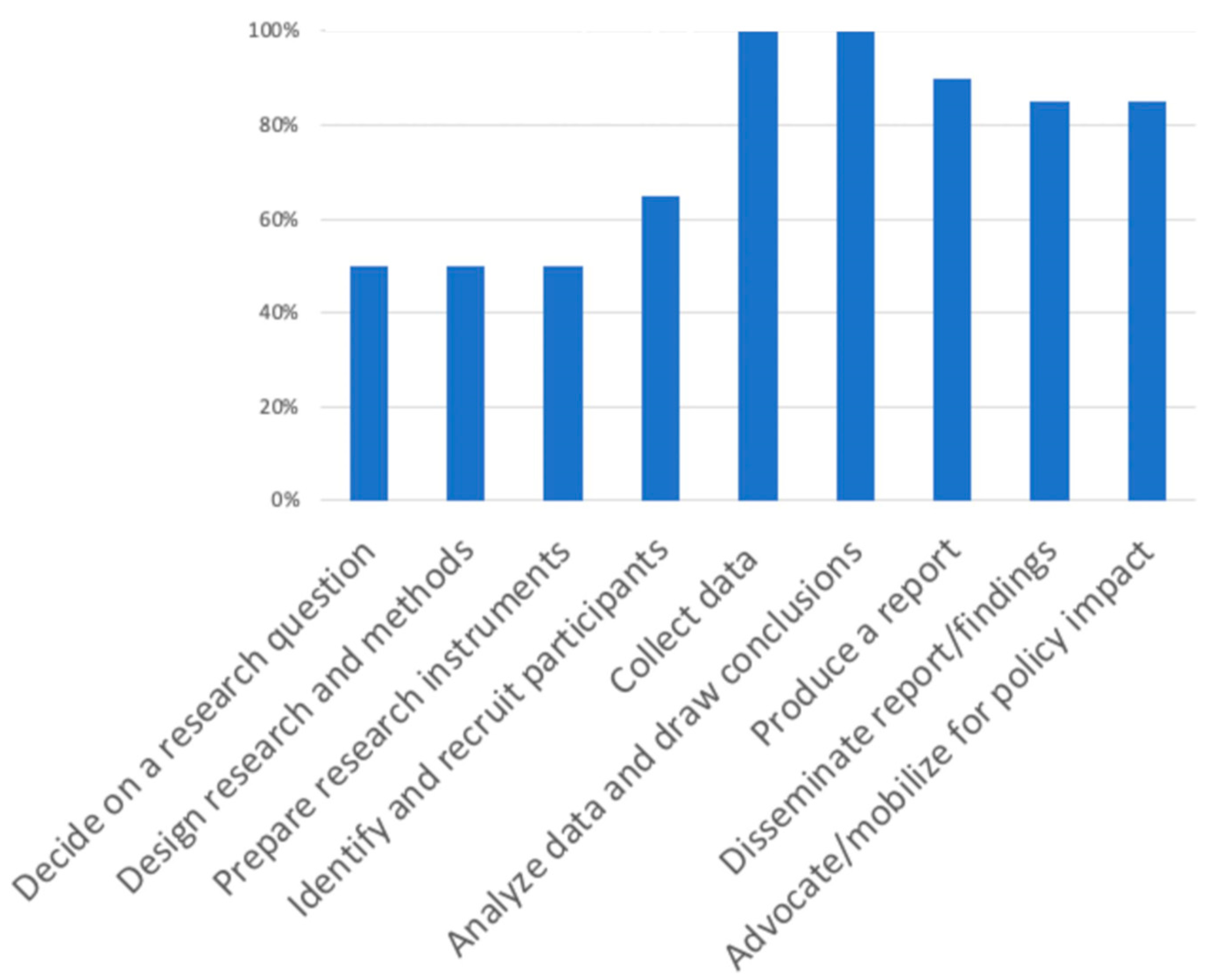
3.7. User Experiences with the Discovery Tool App and Our Voice Process
4. Discussion
4.1. Limitations
4.2. Future Directions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Whitehead, M. The Concepts and Principles of Equity and Health; World Health Organization Regional Office for Europe: Copenhagen, Denmark, 1990. [Google Scholar]
- U.S. Department of Health & Human Services. Healthy People 2020; US Department of Health and Human Services, Office of Disease Prevention and Health Promotion: Washington, DC, USA, 2010. [Google Scholar]
- Abel, T.; Frohlich, K.L. Capitals and capabilities: Linking structure and agency to reduce health inequalities. Soc. Sci. Med. 2012, 74, 236–244. [Google Scholar] [CrossRef] [PubMed]
- Stratton, A.; Hynes, M.; Nepaul, A. Issue Brief—Defining Health Disparities; Connecticut Department of Public Health: Hartford, CT, USA, 2007. [Google Scholar]
- Marmot, M. Fair Society, Healthy Lives; The Marmot Review: London, UK, 2010. [Google Scholar]
- National Academies of Sciences, Engineering and Medicine. Communities in Action: Pathways to Health Equity; The National Academies Press: Washington, DC, USA, 2017. [Google Scholar]
- Backett-Milburn, K.; Cunningham-Burley, S.; Davis, J. Contrasting lives, contrasting views? Understandings of health inequalities from children in differing social circumstances. Soc. Sci. Med. 2003, 57, 613–623. [Google Scholar] [CrossRef]
- Nduna, M.; Jewkes, R. Disempowerment and psychological distress in the lives of young people in Eastern Cape, South Africa. J. Child Fam. Stud. 2012, 21, 1018–1027. [Google Scholar] [CrossRef]
- Schissel, B. Betting against youth: The effects of socioeconomic marginality on gambling among young people. Youth Soc. 2001. [Google Scholar] [CrossRef]
- Credo, K.R.; Lanier, P.A.; Matherne, C., III; Cox, S.S. Narcissism and entitlement in Millennials: The mediating influence of community service self efficacy on engagement. Pers. Individ. Differ. 2016, 101, 192–195. [Google Scholar] [CrossRef]
- Zimmerman, M.A.; Eisman, A.B.; Reischl, T.M.; Morrel-Samuels, S.; Stoddard, S.; Miller, A.L.; Hutchinson, P.; Franzen, S.; Rupp, L. Youth empowerment solutions: Evaluation of an after-school program to engage middle school students in community change. Health Educ. Behav. 2017, 45, 20–31. [Google Scholar] [CrossRef] [Green Version]
- Goulet, M.; Archambault, I.; Janosz, M.; Christenson, S.L. Evaluating the implementation of Check & Connect in various school settings: Is intervention fidelity necessarily associated with positive outcomes? Eval. Program. Plan. 2018, 68, 34–46. [Google Scholar] [CrossRef]
- Heller, S.B.; Shah, A.K.; Guryan, J.; Ludwig, J.; Mullainathan, S.; Pollack, H.A. Thinking, fast and slow? Some field experiments to reduce crime and dropout in Chicago. Quar. J. Econ. 2017, 132, 1–54. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. WHO Guidance to Protect Health from Climate Change through Health Adaptation Planning; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- Lorimer, K.; Knight, R.; Shoveller, J. Improving the health and social wellbeing of young people: Exploring the potential of and for collective agency. Crit. Public Health 2020. [Google Scholar] [CrossRef]
- Peréa, F.C.; Sayles, N.R.; Reich, A.J.; Koomas, A.; McMann, H.; Sprague Martinez, L.S. “Mejorando Nuestras Opportunidades”: Engaging urban youth in environmental health assessment and advocacy to improve health and outdoor play spaces. Int. J. Environ. Res. Public Health 2019, 16, 571. [Google Scholar] [CrossRef] [Green Version]
- CSDH. Closing the Gap in a Generation: Health Equity through Action on the Social Determinants of Health; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- CDC/ATSDR. Principles of Community Engagement, 2nd ed.; CDC: Atlanta, GA, USA, 2013. [Google Scholar]
- Melo, P.; Alves, O. Community empowerment and community partnerships in nursing decision-making. Healthcare 2019, 7, 76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, E.C.; Catalano, R.F.; Fleming, C.B.; Haggerty, K.P.; Abbott, R.D. Adolescent substance use outcomes in the raising healthy children project: A two-part latent growth curve analysis. J. Consult. Clin. Psychol. 2005, 73, 699–710. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eaton, D.K.; Kann, L.; Kinchen, S.; Shanklin, S.; Ross, J.; Hawkins, J.; Harris, W.A.; Lowry, R.; McManus, T.; Chyen, D.; et al. Youth risk behavior surveillance—United States, 2007. MMWR Surveill. Summ. 2008, 57, 1–131. [Google Scholar] [PubMed]
- King, A.C.; Winter, S.J.; Chrisinger, B.W.; Hua, J.; Banchoff, A.W. Maximizing the promise of citizen science to advance health and prevent disease. Prev. Med. 2019, 119, 44–47. [Google Scholar] [CrossRef]
- Ballard, H.L.; Dixon, C.G.H.; Harris, E.M. Youth-focused citizen science: Examining the role of environmental science learning and agency for conservation. Biol. Conserv. 2017, 208, 65–75. [Google Scholar] [CrossRef] [Green Version]
- Organization for Economic Cooperation and Development (OECD). Colombia and Its Education System; OECD Publishing: Paris, France, 2016. [Google Scholar]
- Gibbs, L.; Kornbluh, M.; Marinkovic, K.; Bell, S.; Ozer, E.J. Using technology to scale up youth-led participatory action research: A systematic review. J. Adolesc. Health 2020, 67, S14–S23. [Google Scholar] [CrossRef]
- Ozer, E.J.; Piatt, A.A. Youth-led participatory action research (YPAR): Principles applied to the US and diverse global settings. In Community-Based Participatory Research for Health; Wallerstein, N., Duran, B., Oeztel, J., Minkler, M., Eds.; John Wiley & Sons, Inc.: San Francisco, CA, USA, 2018. [Google Scholar]
- Plough, A.L. Measuring What Matters: Introducing a New Action Framework; Robert Wood Johnson Foundation: Princeton, NJ, USA, 2015. [Google Scholar]
- Ruggeri, D.; Young, D. Community in the information age: Exploring the social potential of web-based technologies in landscape architecture and community design. Front. Archit. Res. 2016, 5, 15–26. [Google Scholar] [CrossRef] [Green Version]
- King, A.C.; King, D.K.; Banchoff, A.; Solomonov, S.; Ben Natan, O.; Hua, J.; Gardiner, P.; Goldman Rosas, L.; Rodriguez Espinosa, P.; Winter, S.J.; et al. Employing participatory citizen science methods to promote age-friendly environments worldwide. Int. J. Environ. Res. Public Health 2020, 17, 1541. [Google Scholar] [CrossRef] [Green Version]
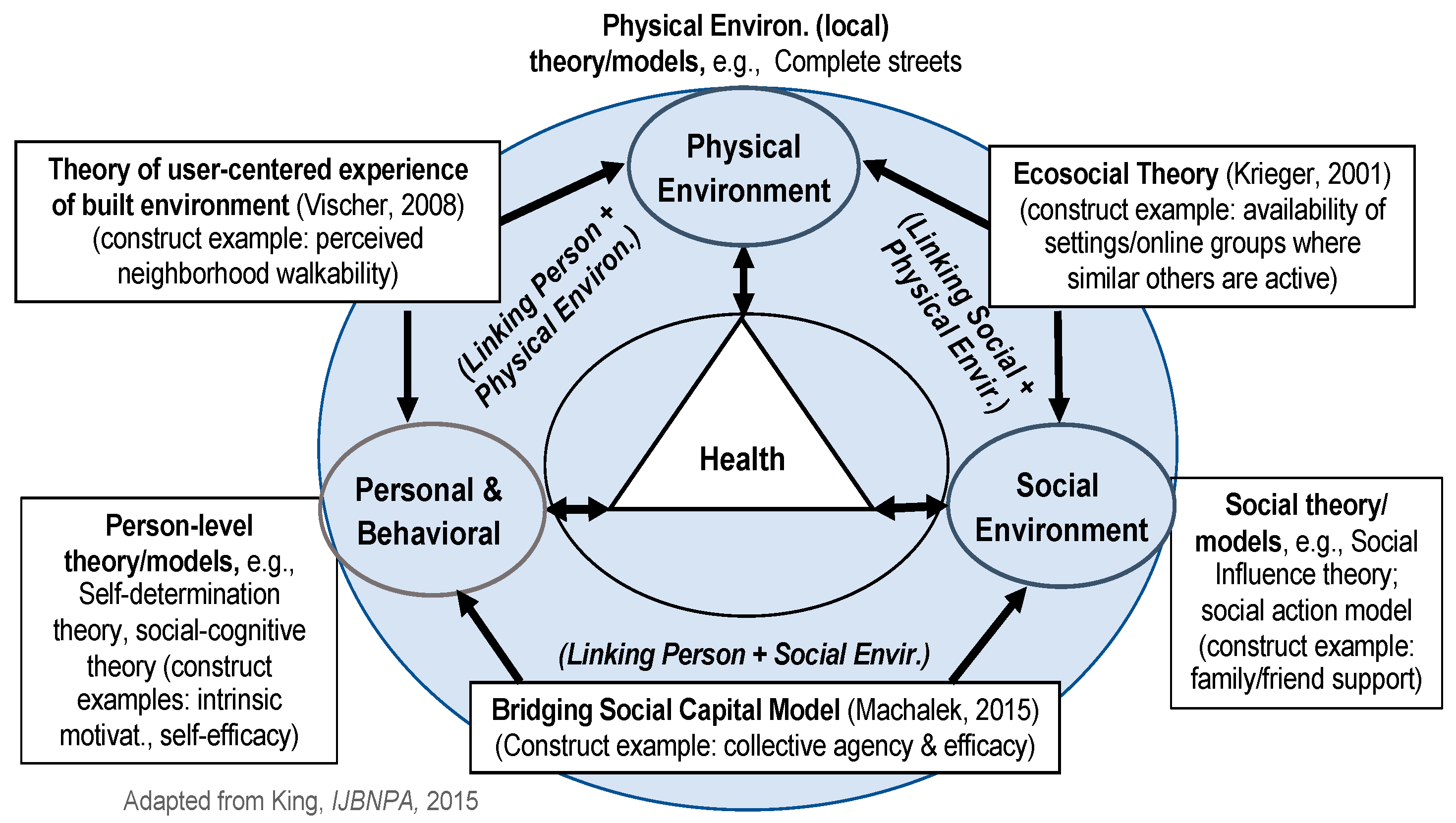
- Sallis, J.F.; Owen, N. Ecological models of health behavior. In Health Behavior and Health Education: Theory, Research, and Practice, 3rd ed.; Glanz, K., Rimer, B.K., Lewis, F.M., Eds.; Jossey-Bass: San Francisco, CA, USA, 2002; pp. 462–484. [Google Scholar]
- King, A.C. Theory’s role in shaping behavioral health research for population health. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 146. [Google Scholar] [CrossRef] [Green Version]
- Bandura, A. Toward a psychology of human agency. Psychol. Sci. 2006, 1, 164–180. [Google Scholar] [CrossRef]
- Ryan, R.M.; Deci, E.L. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am. Psychol. 2000, 55, 68–78. [Google Scholar] [CrossRef]
- Rothman, J. Approaches to community intervention. In Strategies of Community Intervention; Rothman, J., Tropman, J.E., Eds.; Peacock: Itasca, IL, USA, 2001. [Google Scholar]
- Coleman, J. Social capital in the creation of human capital. Am. J. Soc. 1988, 94, S95–S120. [Google Scholar] [CrossRef]
- Krieger, N. Theories for social epidemiology in the 21st century: An ecosocial perspective. Int. J. Epidemiol. 2001, 30, 668–677. [Google Scholar] [CrossRef] [PubMed]
- Machalek, R.; Martin, M.W. Sociobiology and Sociology: A new synthesis. In International Encyclopedia of the Social & Behavioral Sciences, 2nd ed.; Elsevier B.V.: Amsterdam, The Netherlands, 2015; pp. 1–13. [Google Scholar]
- Vischer, J.C. Towards a user-centered theory of the built environment. Build. Res. Inf. 2008, 36, 231–240. [Google Scholar] [CrossRef]
- Damschroder, L.J.; Aron, D.C.; Keith, R.E.; Kirsh, S.R.; Alexander, J.A.; Lowery, J.C. Fostering implementation of health services research findings into practice: A consolidated framework for advancing implementation science. Implement. Sci. 2009, 4, 50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- King, D.K.; Shoup, J.A.; Raebel, M.A.; Anderson, C.B.; Wagner, N.M.; Ritzwoller, D.P.; Bender, B.G. Planning for Implementation Success Using RE-AIM and CFIR Frameworks: A Qualitative Study. Front. Public Health 2020, 8, 59. [Google Scholar] [CrossRef] [Green Version]
- Buman, M.P.; Winter, S.J.; Sheats, J.L.; Hekler, E.B.; Otten, J.J.; Grieco, L.A.; King, A.C. The Stanford Healthy Neighborhood Discovery Tool: A computerized tool to assess active living environments. Am. J. Prev. Med. 2013, 44, e41–e47. [Google Scholar] [CrossRef] [Green Version]
- King, A.C.; Winter, S.J.; Sheats, J.L.; Rosas, L.G.; Buman, M.P.; Salvo, D.; Rodriguez, N.M.; Seguin, R.A.; Moran, M.; Garber, R.; et al. Leveraging citizen science and information technology for population physical activity promotion. Translat. J. ACSM 2016, 1, 30–44. [Google Scholar]
- Tuckett, A.G.; Freeman, A.; Hetherington, S.; Gardiner, P.A.; King, A.C.; on behalf of Burnie Brae Citizen Scientists. Older adults using Our Voice Citizen Science to create change in their neighborhood environment. Int. J. Environ. Res. Public Health 2018, 15, 2685. [Google Scholar] [CrossRef] [Green Version]
- Hinckson, E.; Schneider, M.; Winter, S.J.; Stone, E.; Puhan, M.; Stathi, A.; Porter, M.M.; Gardiner, P.A.; Dos Santos, D.L.; Wolff, A.; et al. Citizen science applied to building healthier community environments: Advancing the field through shared construct and measurement development. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 133. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Global Strategy on Diet, Physical Activity, and Health; WHO: Geneva, Switzerland, 2004. [Google Scholar]
- Devarajan, R.; Prabhakaran, D.; Goenka, S. Built environment for physical activity–An urban barometer, surveillance, and monitoring. Public Health 2019, 21, e12938. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marmot, M.; Allen, J.J. Social determinants of health equity. Am. J. Public Health 2014, 104 (Suppl. S4), S517–S519. [Google Scholar] [CrossRef] [PubMed]
- Gelormino, E.; Melis, G.; Marietta, C.; Costa, G. From built environment to health inequalities: An explanatory framework based on evidence. Prev. Med. Rep. 2015, 2, 737–745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- King, K.E.; Clarke, P.J. A disadvantaged advantage in walkability: Findings from socioeconomic and geographical analysis of national built environment data in the United States. Am. J. Epidemiol. 2015, 181, 17–25. [Google Scholar] [CrossRef] [Green Version]
- Haan, M.; Kaplan, G.A.; Camacho, T. Poverty and health: Prospective evidence from the Alameda County Study. Am. J. Epidemiol. 1987, 125, 989–998. [Google Scholar] [CrossRef]
- United Nations. Sustainable Development Goals; United Nations: New York, NY, USA, 2015. [Google Scholar]
- Ward, E.; Jemal, A.; Cokkinides, V.; Singh, G.K.; Cardinez, C.; Ghafoor, A.; Thun, M. Cancer disparities by race/ethnicity and socioeconomic status. CA A Cancer J. Clin. 2004, 54, 78–93. [Google Scholar] [CrossRef]
- Ozer, E.J. Youth-led participatory action research. In Handbook of Methodological Approaches to Community-Based Research: Qualitative, Quantitative, and Mixed Methods; Jason, L.A., Glenwick, D.S., Eds.; Oxford: New York, NY, USA, 2016; pp. 263–272. [Google Scholar]
- United Nations. United Nations Sustainable Development Goals: Education. Available online: https://www.un.org/sustainabledevelopment/education/ (accessed on 10 October 2020).
- UNESCO. Global Education Monitoring Report; United Nations Educational, Scientific and Cultural Organization: Paris, France, 2019. [Google Scholar]
- Belfield, C.R.; Levin, H.M. The Education Attainment Gap: Who’s Affected, How Much, and Why It Matters. Available online: https://www.brookings.edu/wp-content/uploads/2016/07/pricewepay_chapter.pdf (accessed on 7 September 2020).
- Njong, A.M. The effects of educational attainment on poverty reduction in Cameroon. J. Educ. Adm. Policy Stud. 2010, 2, 1–8. [Google Scholar] [CrossRef]
- Gonzalez, S.A.; Rubio, M.A.; Triana, C.A.; King, A.C.; Banchoff, A.W.; Sarmiento, O.L. Building healthy schools through technology-enabled citizen science: A participatory action model in schools from Bogotá, Colombia. Global Public Health 2021. [Google Scholar] [CrossRef]
- Montes, F.; Sarmiento, O.L.; Rodríguez, A.L.; Guerra, A.M.; Jaramillo, A.M.; Higuera, D.; King, A.C. Physical inactivity and substance use in rural areas: Socially transmitted conditions? In Proceedings of the Latin American Conference on Complex Networks, Cartagena, Colombia, 5–9 August 2019. [Google Scholar]
- Chaudhury, M.; Hinckson, E.; Natasha, N.; King, A.C. Empowering children to influence changes in their school environment for learning, physical activity, health and wellbeing. In Proceedings of the International Society of Behavioral Nutrition and Physical Activity (ISBNPA) XChange, Auckland, New Zealand, 16 June 2020. [Google Scholar]
- Rodriguez, N.M.; Arce, A.; Kawaguchi, A.; Hua, J.; Broderick, B.; Winter, S.J.; King, A.C. Enhancing safe routes to school programs through community-engaged citizen science: Two pilot investigations in lower density areas of Santa Clara County, California, USA. BMC Public Health 2019, 19, 256. [Google Scholar] [CrossRef]
- Frank, L.D.; Sallis, J.F.; Conway, T.L.; Chapman, J.; Saelens, B.E.; Bachman, W. Multiple pathways from land use to health: Walkability associations with active transportation, body mass index, and air quality. J. Am. Plan. Assoc. 2006, 72, 75–87. [Google Scholar] [CrossRef]
- Frank, L.D.; Greenwald, M.J.; Winkelman, S.; Chapman, J.; Kavage, S. Carbonless footprints: Promoting health and climate stabilization through active transportation. Prev. Med. 2010, 50 (Suppl. S1), S99–S105. [Google Scholar] [CrossRef] [PubMed]
- Chastin, S.; Saunders, J.N.; Kelly, P.; Simpson, J.S. Urban green and blue spaces impact on health and health equity: A stakeholder driven logic model. In Proceedings of the International Society of Behavioral Nutrition & Physical Activity Annual Conference, Prague, Czech Republic, 4–9 June 2019. [Google Scholar]
- Oni, T.; Assah, F.; Erzse, A.; Foley, L.; Govia, I.; Hofman, K.J.; Lambert, E.V.; Micklesfield, L.K.; Shung-King, M.; Smith, J.; et al. The global diet and activity research (GDAR) network: A global public health partnership to address upstream NCD risk factors in urban low and middle-income contexts. Global Health 2020, 16, 100. [Google Scholar] [CrossRef] [PubMed]
- Odunitan-Wayas, F.A.; Keuko Njuenji, K.O.; Oni, T.; King, A.C.; Lambert, E.V. Perceived barriers and facilitators to physical activity and healthy eating in South African adolescents from low-income urban communities before and during the COVID-19 pandemic. In Proceedings of the 2021 Annual Conference of Consortium of Universities for Global Health (CUGH), 12 October 2020. (virtual). [Google Scholar]
- Mellins, C.A.; Walsh, K.; Sarvet, A.L.; Wall, M.; Gilbert, L.; Santelli, J.S.; Thompson, M.; Wilson, P.A.; Khan, S.; Benson, S.; et al. Sexual assault incidents among college undergraduates: Prevalence and factors associated with risk. PLoS ONE 2017, 12, e0186471. [Google Scholar] [CrossRef]
- Graham, S.; Zha, C.; King, A.C.; Banchoff, A.W.; Sarnquist, C.; Dauber, M.; Baiocchi, M. A novel approach for generating creative, community-responsive interventions to reduce gender-based violence on college campuses. Unpublished work. 2021. [Google Scholar]
- Christian, H.; Giles-Corti, B.; Knuiman, M.; Timperio, A.; Foster, S. The influence of the built environment, social environment and health behaviors on body mass index: Results from RESIDE. Prev. Med. 2011, 53, 57–60. [Google Scholar] [CrossRef] [PubMed]
- Hinckson, E.; Schneider, M.; Sarmiento, O.L.; Lambert, E.; Triana, C.; Banchoff, A.; Winter, S.; King, A.C. Utilising the Our Voice citizen science model to support and promote active environments at schools and universities in Colombia, New Zealand, South Africa, and the USA. J. Phys. Act. Health 2018, 15, S1. [Google Scholar]
- Chaudhury, M.; Hinckson, E.; Jelleyman, C.; Banchoff, A.W.; King, A.C. Utilising the Our Voice citizen science model to support and promote active and healthy eating university environments. In Proceedings of the International Society of Behavioral Nutrition and Physical Activity (ISBNPA), Prague, Czech Republic, 8 June 2019. [Google Scholar]
- Li, S. The built environment matters for mental health. The Stanford Daily, 21 June 2020; 1–5. [Google Scholar]
- Greguska, E. ASU health students become citizen scientists with app. ASU Now, 3 December 2019; 1–3. [Google Scholar]
- Harrison, E.; Gilbert, B.; Popkin, S.J.; Waxman, J. Research Report–Tackling Food Insecurity by Bringing Data to Communities; Urban Institute: Washington, DC, USA, 2019. [Google Scholar]
- Rydenstam, T.; Fell, T.; Buli, B.G.; King, A.C.; Balter, K. Using citizen science to understand the prerequisites for physical activity among adolescents in low socioeconomic status neighborhoods—The NESLA study. Health Place 2020, 65, 102387. [Google Scholar] [CrossRef]
- Balter, K.; Rydenstam, T.; Fell, T.; King, A.C.; Buli, B.G. Data from an Our Voice citizen science initiative in neighborhoods with low socioeconomic status in Sweden: A proof of concept for collecting complex data. Data Brief 2020, 33, 106394. [Google Scholar] [CrossRef] [PubMed]
- United Nations. United Nations Sustainable Development Goals: Millions Could Escape Poverty by Finishing Secondary Education. Available online: https://www.un.org/sustainabledevelopment/blog/2017/06/ (accessed on 18 November 2020).
- Rosas, L.G.; Salvo, D.; Winter, S.J.; Cortes, D.; Rivera, J.; Rodriguez, N.M.; King, A.C. Harnessing Technology and Citizen Science to Support Neighborhoods that Promote Active Living in Mexico. J. Urban Health 2016, 93, 953–973. [Google Scholar] [CrossRef] [Green Version]
- Winter, S.J.; Goldman Rosas, L.; Padilla Romero, P.; Sheats, J.L.; Buman, M.P.; Baker, C.; King, A.C. Using citizen scientists to gather, analyze, and disseminate information about neighborhood features that affect active living. J. Immigr. Minor. Health 2015. [Google Scholar] [CrossRef] [Green Version]
- Winter, S.J.; Sheats, J.L.; Salvo, D.; Banda, J.A.; Quinn, J.; Rivera, B.R.; King, A.C. A Mixed Method Study to Inform the Implementation and Expansion of Pop-Up Parks for Economic, Behavioral, and Social Benefits. J. Urban Health 2020, 97, 529–542. [Google Scholar] [CrossRef]
- Zha, C.C. Raising our voices: A hypothesis-generating study of the link between political participation, efficacy and health. In Stanford University Human Biology Honors Thesis Symposium; Stanford University: Stanford, CA, USA, 2020. [Google Scholar]
- Block, P.; Hoffman, M.; Raabe, I.J.; Dowd, J.B.; Rahal, C.; Kashyap, R.; Mills, M.C. Social network-based distancing strategies to flatten the COVID-19 curve in a post-lockdown world. Nat. Hum. Behav. 2020, 4, 588–596. [Google Scholar] [CrossRef] [PubMed]
- Sarmiento, O.L.; Higuera-Mendieta, D.; Wilches-Mogollon, M.A.; Guzman, L.A.; Rodriguez, D.A.; Morales, R.; Mendez, D.; Bedoya, C.; Linares-Vasquez, M.; Arevalo, M.I.; et al. Urban Transformations and Health: Methods for TrUST-a Natural Experiment Evaluating the Impacts of a Mass Transit Cable Car in Bogotá, Colombia. Front. Public Health 2020, 8, 64. [Google Scholar] [CrossRef] [PubMed]
- Buman, M.P.; Winter, S.J.; Baker, C.; Hekler, E.B.; Otten, J.J.; King, A.C. Neighborhood Eating and Activity Advocacy Teams (NEAAT): Engaging older adults in policy activities to improve food and physical environments. Transl. Behav. Med. 2012, 2, 249–253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bradley, R.H.; Putnick, D.L. Housing quality and access to material and learning resources within the home environment in developing countries. Child. Dev. 2012, 83, 76–91. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khanolainen, D.; Psyridou, M.; Silinskas, G.; Lerkkanen, M.K.; Niemi, P.; Poikkeus, A.M.; Torppa, M. Longitudinal effects of the home learning environment and parental difficulties on reading and math development across grades 1–9. Front. Psychol. 2020, 11, 1–36. [Google Scholar] [CrossRef]
- Maibach, E.; Steg, L.; Anable, J. Promoting physical activity and reducing climate change: Opportunities to replace short car trips with active transportation. Prev. Med. 2009, 49, 326–327. [Google Scholar] [CrossRef] [Green Version]
- King, A.C. Behavioral medicine in the 21st century: Transforming “the Road Less Traveled” into the “American Way of Life”. Ann. Behav. Med. 2014, 47, 71–78. [Google Scholar] [CrossRef] [Green Version]
- Emery, M.; Higgins, L.; Chazdon, S.; Hansen, D. Using Ripple Effects Mapping to evaluate program impact: Choosing or combining the methods that work best for you. J. Ext. 2015, 53, n2. [Google Scholar]
- Welborn, R.; Downey, L.; Dyk, P.H.; Monroe, P.A.; Tayler-Mackey, C.; Worthy, S.L. Turning the tide on poverty: Documenting impacts through ripple effect mapping. Commun. Dev. 2016, 47, 385–402. [Google Scholar] [CrossRef]
- Washburn, L.T.; Traywick, L.; Thornton, L.; Vincent, J.; Brown, T. Using Ripple Effects Mapping to evaluate a community-based health program: Perspectives of program implementers. Health Promot. Pract. 2018. [Google Scholar] [CrossRef]
- Chrisinger, B.; King, A.C. Stress experiences in neighborhood and social environments (SENSE): A pilot study to integrate the quantified self with citizen science to improve the built environment and health. Inter. J. Health Geogr. 2018, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]





| Participants | Discover | Discuss | Advocate | Change |
|---|---|---|---|---|
| Patient and family | Use Discovery Tool to document factors impacting ability to practice healthy behaviors | In small (remotely connected) groups with other patients and their families, discuss, organize and prioritize findings (facilitated by OV team) | Develop action plans and present to clinicians for discussion | Individual, social, environmental and policy changes are measured |
| Clinician (individual) | Obtain a better understanding of their patients’ neighborhoods | Learn about positive and negative opportunities related to health behaviors (e.g., physical activity, social distancing for COVID-19, local park access & use) | Example: Signing a neighborhood letter for a patient or patient group advocating for a feasible neighbor-hood change | Stronger relationships with patients and community, enriched by contextual knowledge |
| Clinic (group) | Develop interactive neighborhood maps and share in clinic setting and/or online | Highlight areas of opportunities/concern and how the community can help | Example: Clinic helps to advocate for larger collective change at local community or gov-ernmental levels | Clinic becomes a key community hub for citizen science and positive “up-stream” activities |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
King, A.C.; Odunitan-Wayas, F.A.; Chaudhury, M.; Rubio, M.A.; Baiocchi, M.; Kolbe-Alexander, T.; Montes, F.; Banchoff, A.; Sarmiento, O.L.; Bälter, K.; et al. Community-Based Approaches to Reducing Health Inequities and Fostering Environmental Justice through Global Youth-Engaged Citizen Science. Int. J. Environ. Res. Public Health 2021, 18, 892. https://doi.org/10.3390/ijerph18030892
King AC, Odunitan-Wayas FA, Chaudhury M, Rubio MA, Baiocchi M, Kolbe-Alexander T, Montes F, Banchoff A, Sarmiento OL, Bälter K, et al. Community-Based Approaches to Reducing Health Inequities and Fostering Environmental Justice through Global Youth-Engaged Citizen Science. International Journal of Environmental Research and Public Health. 2021; 18(3):892. https://doi.org/10.3390/ijerph18030892
Chicago/Turabian StyleKing, Abby C., Feyisayo A. Odunitan-Wayas, Moushumi Chaudhury, Maria Alejandra Rubio, Michael Baiocchi, Tracy Kolbe-Alexander, Felipe Montes, Ann Banchoff, Olga Lucia Sarmiento, Katarina Bälter, and et al. 2021. "Community-Based Approaches to Reducing Health Inequities and Fostering Environmental Justice through Global Youth-Engaged Citizen Science" International Journal of Environmental Research and Public Health 18, no. 3: 892. https://doi.org/10.3390/ijerph18030892
APA StyleKing, A. C., Odunitan-Wayas, F. A., Chaudhury, M., Rubio, M. A., Baiocchi, M., Kolbe-Alexander, T., Montes, F., Banchoff, A., Sarmiento, O. L., Bälter, K., Hinckson, E., Chastin, S., Lambert, E. V., González, S. A., Guerra, A. M., Gelius, P., Zha, C., Sarabu, C., Kakar, P. A., ... on behalf of the Our Voice Global Citizen Science Research Network. (2021). Community-Based Approaches to Reducing Health Inequities and Fostering Environmental Justice through Global Youth-Engaged Citizen Science. International Journal of Environmental Research and Public Health, 18(3), 892. https://doi.org/10.3390/ijerph18030892