
Refugees in Canada during the First Wave of the COVID-19 Pandemic


{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
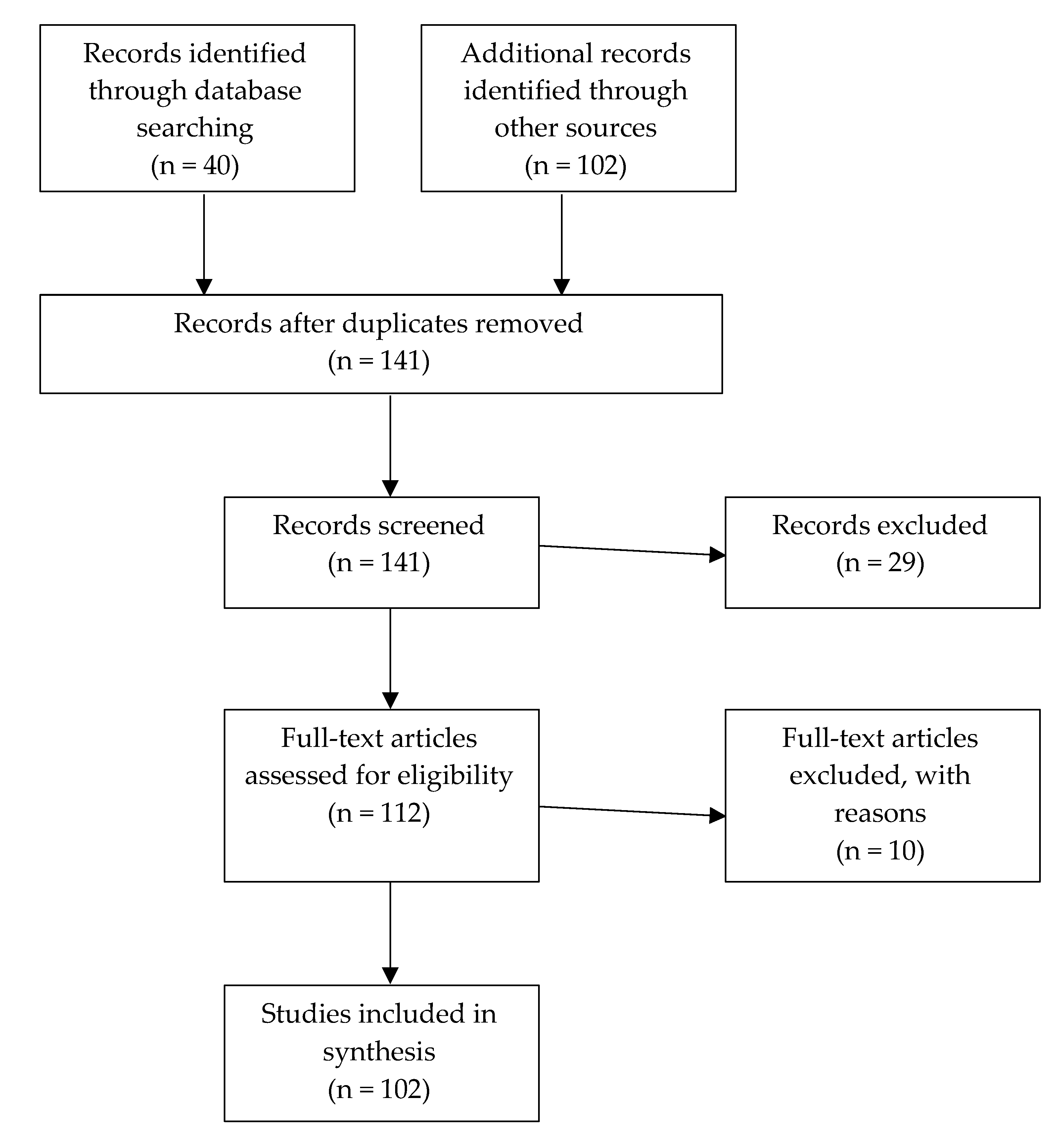
2.1. Search Strategy
2.2. Exclusion Criteria
2.3. Data Extraction
3. Results
3.1. Brief Overview of the Refugee Resettlement Programs in Canada
3.2. Access to Healthcare
3.3. Health Insurance
3.4. Health Literacy
“We don’t have debunking happening in the native language that people are speaking so people are more inclined to believe things that’s coming through WhatsApp or Facebook because it’s either coming from someone that they trust, or it could just be family and friends back home sending it in a language that they emotionally connect with.”[40]
3.5. Personal Protective Equipment and Testing Capacity
3.6. Economic Measures
3.7. Closure of Public Spaces: School
3.8. Closure of Community and Religious Centres
3.9. Closure of Borders
“Canada’s decision is out of step with public health measures designed to curb the spread of COVID-19, and runs counter to our international legal obligations. From moral, public health and legal perspectives, closing the border to refugee claimants is wrong. Turning refugee claimants away—including as a result of the decision to shut down the Canada/US border—exposes refugees, who face increased hardship, danger and ostracization worldwide related to this pandemic, to serious human rights violations, including inhumane immigration detention conditions and the risk of refoulement to torture and other human rights abuses.”[89]
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- JHU CSSE. COVID-19 Dashboard. Baltimore. 2020. Available online: https://gisanddata.maps.arcgis.com/apps/opsdashboard/index.html#/bda7594740fd40299423467b48e9ecf6 (accessed on 6 May 2020).
- Government of Canada. Coronavirus Disease (COVID-19): Outbreak Update. 2020. Available online: https://www.canada.ca/en/public-health/services/diseases/2019-novel-coronavirus-infection.html (accessed on 11 April 2020).
- Heymann, D.; Chen, L.; Takemi, K.; Fidler, D.; Tappero, J.W.; Thomas, M.J.; Kenyon, T.A.; Frieden, T.R.; Yach, D.; Nishtar, S.; et al. Global Health Security: The Wider Lessons from the West African Ebola Virus Disease Epidemic. Lancet 2015, 385, 1884–1901. [Google Scholar] [CrossRef]
- Straehle, C. Ethical Reflections on Who is at Risk: Vulnerability and Global Public Health. In The Handbook of Global Health Policy; Brown, G., Yamey, G., Wamala, S., Eds.; John & Wiley Sons: West Sussex, UK, 2014; pp. 197–207. [Google Scholar]
- UNHCR. Figures at a Glance. 19 June 2019. Available online: https://www.unhcr.org/uk/figures-at-a-glance.html (accessed on 10 October 2019).
- Malebranche, M.; Nerenberg, K.; Metcalfe, A.; Fabreau, G.E. Addressing vulnerability of pregnant refugees. Bull. World Health Organ. 2017, 95, 611. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5578387/ (accessed on 17 April 2020). [CrossRef] [PubMed]
- UNHCR. Global Trends: Forced Displacement in 2018 Geneva. 12 June 2019. Available online: https://www.unhcr.org/dach/wp-content/uploads/sites/27/2019/06/2019-06-07-Global-Trends-2018.pdf (accessed on 11 April 2020).
- UN General Assembly. Convention Relating to the Status of Refugees Geneva. 28 July 1951. Available online: https://www.unhcr.org/1951-refugee-convention.html (accessed on 15 October 2019).
- Government of Canada. Government-Assisted Refugees Program. 9 December 2019. Available online: https://www.canada.ca/en/immigration-refugees-citizenship/services/refugees/help-outside-canada/government-assisted-refugee-program.html (accessed on 4 May 2020).
- Government of Canada. Community Sponsors: About the Process. 18 March 2020. Available online: https://www.canada.ca/en/immigration-refugees-citizenship/services/refugees/help-outside-canada/private-sponsorship-program/community-sponsors.html (accessed on 4 May 2020).
- Government of Canada. Immigration, Refugees and Citizenship Canada Departmental Plan 2019–2020. 14 May 2019. Available online: https://www.canada.ca/en/immigration-refugees-citizenship/corporate/publications-manuals/departmental-plan-2019-2020/departmental-plan.html (accessed on 5 May 2020).
- Government of Canada. Blended Visa Office-Referred Program: About the Process. 18 March 2020. Available online: https://www.canada.ca/en/immigration-refugees-citizenship/services/refugees/help-outside-canada/private-sponsorship-program/blended-visa-office-program.html (accessed on 4 May 2020).
- Hansen, R. The Comprehensive Refugee Response Framework: A Commentary. J. Refug. Stud. 2018, 31, 131–151. [Google Scholar] [CrossRef]
- Government of Canada. Notice—Supplementary Information 2019–2021 Immigration Levels Plan. 31 October 2018. Available online: https://www.canada.ca/en/immigration-refugees-citizenship/news/notices/supplementary-immigration-levels-2019.html (accessed on 5 May 2020).
- Government of Canada. Claiming Asylum in Canada—What Happens? 11 April 2019. Available online: https://www.canada.ca/en/immigration-refugees-citizenship/news/2017/03/claiming_asylum_incanadawhathappens.html (accessed on 4 May 2020).
- Government of Canada. Canada-U.S. Safe Third Country Agreement. 23 June 2016. Available online: https://www.canada.ca/en/immigration-refugees-citizenship/corporate/mandate/policies-operational-instructions-agreements/agreements/safe-third-country-agreement.html (accessed on 4 May 2020).
- Canadian Council for Refugees. Safe Third Country Montreal. Available online: https://ccrweb.ca/en/safe-third-country (accessed on 4 May 2020).
- EQUI-TB. Who Is Most Vulnerable to TB and What Can We Do about It; EQUI-TB: Liverpool, UK, 2005. Available online: https://assets.publishing.service.gov.uk/media/57a08c98e5274a31e00012fa/HTBLivtb_vulnerable.pdf (accessed on 18 June 2020).
- Public Health Agency of Canada. Health Status of Canadians 2016; Public Health Agency of Canada: Ottawa, ON, Canada, 2016. Available online: https://healthycanadians.gc.ca/publications/department-ministere/state-public-health-status-2016-etat-sante-publique-statut/alt/pdf-eng.pdf (accessed on 18 June 2020).
- Morris, M.D.; Popper, S.T.; Rodwell, T.C.; Brodine, S.K.; Brouwer, K.C. Healthcare Barriers of Refugees Post-resettlement. J. Community Health 2009, 34, 529. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2778771/pdf/10900_2009_Article_9175.pdf (accessed on 29 April 2020). [CrossRef] [PubMed] [Green Version]
- Mishori, R.; Aleinikoff, S.; Davis, D. Primary Care for Refugees: Challenges and Opportunities. Am. Fam. Phys. 2017, 96, 112–120. Available online: https://www.aafp.org/afp/2017/0715/p112.pdf (accessed on 29 April 2020).
- Wang, B.; Li, R.; Lu, Z.; Huang, Y. Does comorbidity increase the risk of patients with COVID-19: Evidence from meta-analysis. Aging 2020, 12, 6049–6057. Available online: https://www.ncbi.nlm.nih.gov/pubmed/32267833 (accessed on 29 April 2020). [CrossRef]
- McKenna, T. While Singapore Touts Its COVID-19 Success, Migrant Workers Face the Greatest Risk. CBC, 13 May 2020. Available online: https://www.cbc.ca/news/investigates/singapore-covid-19-1.5564641 (accessed on 15 May 2020).
- Draaisma, M. COVID-19 Affecting Certain Groups in Toronto More than Others, Preliminary Data Suggests. CBC, 5 May 2020. Available online: https://www.cbc.ca/news/canada/toronto/toronto-officials-covid-19-outbreak-may-5-update-1.5556401 (accessed on 6 May 2020).
- CBC. Lower Income People, New Immigrants at Higher COVID-19 Risk in Toronto, Data Suggests; CBC: Toronto, ON, Canada, 2020; Available online: https://www.cbc.ca/news/canada/toronto/low-income-immigrants-covid-19-infection-1.5566384 (accessed on 18 June 2020).
- Martin, D.; Miller, A.P.; Quesnel-Vallee, A.; Caron, N.R.; Vissandjee, B.; Marchildon, G.P. Canada’s universal health-care system: Achieving its potential. Lancet 2018, 391, 1718–1735. Available online: https://www.thelancet.com/action/showPdf?pii=S0140-6736%2818%2930181-8 (accessed on 30 April 2020). [CrossRef]
- Caulford, P.; D’Andrade, J. Health care for Canada’s medically uninsured immigrants and refugees: Whose problem is it? Can. Fam. Phys. 2012, 58, 725–727. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3395500/pdf/0580725.pdf (accessed on 30 April 2020).
- Government of Canada. Interim Federal Health Program—Information for Individuals. 13 September 2017. Available online: https://www.canada.ca/en/immigration-refugees-citizenship/services/refugees/help-within-canada/health-care/interim-federal-health-program.html (accessed on 26 April 2020).
- Government of Canada. Guide 5568—Application for Interim Federal Health Program Coverage (IFHP). 7 March 2019. Available online: https://www.canada.ca/en/immigration-refugees-citizenship/services/application/application-forms-guides/guide-5568-application-interim-federal-health-program-coverage.html (accessed on 29 April 2020).
- Oda, A.; Tuck, A.; Agic, B.; Hynie, M.; Roche, B.; McKenzie, K. Health care needs and use of health care services among newly arrived Syrian refugees: A cross-sectional study. CMAJ 2017, 5, 354–358. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5498307/pdf/cmajo.20160170.pdf (accessed on 2 May 2020). [CrossRef] [PubMed] [Green Version]
- McKeary, M.; Newbold, B. Barriers to Care: The Challenges for Canadian Refugees and their Health Care Providers. J. Refug. Stud. 2010, 23, 523–545. [Google Scholar] [CrossRef]
- Government of Ontario. Apply for OHIP and Get a Health Card. 21 April 2017. Available online: https://www.ontario.ca/page/apply-ohip-and-get-health-card#section-3 (accessed on 30 April 2020).
- Caring for Kids New to Canada. Barriers and Facilitators to Health Care for Newcomers Ottawa. March 2014. Available online: https://www.kidsnewtocanada.ca/care/barriers (accessed on 30 April 2020).
- World Health Organization. Coronavirus Disease 2019 (COVID-19) Situation Report—85 Geneva. 15 April 2020. Available online: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200415-sitrep-86-covid-19.pdf?sfvrsn=c615ea20_4 (accessed on 1 May 2020).
- Richtel, M.; W.H.O. Fights a Pandemic Besides Coronavirus: An ‘Infodemic’. New York Times. 6 February 2020. Available online: https://www.nytimes.com/2020/02/06/health/coronavirus-misinformation-social-media.html?action=click&module=RelatedLinks&pgtype=Article (accessed on 1 May 2020).
- Rootman, I.; Gorden-El-Bihbety, D. A Vision for a Health Literate Canada: Report of the Expert Panel on Health Literacy; Canadian Public Health Association: Ottawa, ON, Canada, 2008; Available online: https://www.cpha.ca/sites/default/files/uploads/resources/healthlit/report_e.pdf (accessed on 30 April 2020).
- Ng, E.; Rasugo Omaribo, D.W. Health Literacy and Immigrants in Canada: Determinants and Effects on Health Outcomes. Statistics Canada, March 2010. Available online: http://en.copian.ca/library/research/ccl/health_lit_immigrants_canada/health_lit_immigrants_canada.pdf (accessed on 1 May 2020).
- Hynes, T. The Issue of ‘Trust’ or ‘Mistrust’ in Research with Refugees: Choices, Caveats and Considerations for Researchers; UNHCR: London, UK, 2003; Available online: https://www.unhcr.org/3fcb5cee1.pdf (accessed on 1 May 2020).
- Lotus STEMM. COVID-19 Debunking; YouTube: Toronto, ON, Canada, 2020; Available online: https://www.youtube.com/channel/UCK1mActu-Y2bwxYshKs4wDw (accessed on 6 May 2020).
- Nguyen, A. Are CERB Payments Getting Lost in Translation? Ricochet, 24 April 2020. Available online: https://ricochet.media/en/3062/are-cerb-payments-getting-lost-in-translation (accessed on 6 May 2020).
- Limaye, R.J.; Sauer, M.; Ali, J.; Bernstein, J.; Wahl, B.; Barnhill, A.; Labrique, A. Building trust while influencing online COVID-19 content in the social media world. Lancet 2020, 2, e277–e278. [Google Scholar] [CrossRef]
- WhatsApp. Keeping WhatsApp Personal and Private. 7 April 2020. Available online: https://blog.whatsapp.com/ (accessed on 2 May 2020).
- World Health Organization. Shortage of Personal Protective Equipment Endangering Health Workers Worldwide; World Health Organization: Geneva, Switzerland, 2020; Available online: https://www.who.int/news-room/detail/03-03-2020-shortage-of-personal-protective-equipment-endangering-health-workers-worldwide (accessed on 30 April 2020).
- Treble, P.; Gregory, S. A Heat Map of Coronavirus Cases in Canada. Maclean’s. Available online: https://www.macleans.ca/news/a-heat-map-of-coronavirus-cases-in-canada/ (accessed on 2 May 2020).
- Walmsley, D. Canada Needs a Lot More Virus Testing. So Where Is It; The Globe and Mail: Toronto, ON, Canada, 2020; Available online: https://www.theglobeandmail.com/opinion/editorials/article-canada-needs-a-lot-more-virus-testing-so-where-is-it/ (accessed on 2 May 2020).
- Tasker, J.P. Canada’s Top Doctor Says Non-Medical Masks Can Help Stop the Spread of COVID-19. CBC, 6 April 2020. Available online: https://www.cbc.ca/news/politics/non-medical-masks-covid-19-spread-1.5523321 (accessed on 30 April 2020).
- CDC. Use of Cloth Face Coverings to Help Slow the Spread of COVID-19; CDC: Atlanta, GA, USA, 2020. Available online: https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/diy-cloth-face-coverings.html (accessed on 2 May 2020).
- CPHA. What Are the Social Determinants of Health; CPHA: Ottawa, ON, Canada, 2005; Available online: https://www.cpha.ca/what-are-social-determinants-health (accessed on 3 May 2020).
- Mikkonen, J.; Raphael, D. Social Determinants of Health: The Canadian Facts; York University School of Health Policy and Management: Toronto, ON, Canada, 2010; Available online: https://www.thecanadianfacts.org/The_Canadian_Facts.pdf (accessed on 3 May 2020).
- C.D. Howe Institute. Business Cycle Council. C.D. Howe Institute. Available online: https://www.cdhowe.org/council/business-cycle-council (accessed on 4 May 2020).
- Hindle, T. Job Postings Plummet in March, Slide Continues in April. In Proceedings of the Conference Board of Canada, Ottawa, ON, Canada, 27 April 2020; Available online: https://www.conferenceboard.ca/insights/blogs/job-postings-plummet-in-march-slide-continues-in-april (accessed on 4 May 2020).
- CEIC. Canada Unemployment Rate. CEIC, 9 April 2020. Available online: https://www.ceicdata.com/en/indicator/canada/unemployment-rate (accessed on 4 May 2020).
- Mask, J. Consequences of Immigrating During a Recession: Evidence from the US Refugee Resettlement Program. MPRA, 16 August 2018. Available online: https://mpra.ub.uni-muenchen.de/88492/1/MPRA_paper_88492.pdf (accessed on 4 May 2020).
- Government of Canada. Government Introduces Canada Emergency Response Benefit to Help Workers and Businesses; Government of Canada: Ottawa, ON, Canada, 2020. Available online: https://www.canada.ca/en/department-finance/news/2020/03/introduces-canada-emergency-response-benefit-to-help-workers-and-businesses.html (accessed on 2 May 2020).
- Government of Canada. Canada Emergency Response Benefit (CERB): Who Can Apply; Government of Canada: Ottawa, ON, Canada, 2020. Available online: https://www.canada.ca/en/revenue-agency/services/benefits/apply-for-cerb-with-cra/who-apply.html (accessed on 3 May 2020).
- Steps to Justice. I Don’t Have Permanent Status in Canada. Will I Qualify for the Canada Emergency Response Benefit (CERB); Steps to Justice: Toronto, ON, Canada, 2020; Available online: https://stepstojustice.ca/questions/covid-19/i-don%E2%80%99t-have-permanent-status-canada-will-i-qualify-canada-emergency-response (accessed on 3 May 2020).
- Government of Canada. Questions and Answers on the Canada Emergency Response Benefit; Government of Canada: Ottawa, ON, Canada, 2020; Available online: https://www.canada.ca/en/services/benefits/ei/cerb-application/questions.html (accessed on 3 May 2020).
- Harris, K. Nearly 6 Million People Have Applied for COVID-19 Emergency Benefits; CBC: Toronto, ON, USA, 13 April 2020; Available online: https://www.cbc.ca/news/politics/covid19-benefits-cerb-1.5530722 (accessed on 3 May 2020).
- Yssaad, L. The Immigrant Labour Force Analysis Series; Ministry of Industry: Ottawa, ON, Canada, 2012. Available online: https://www150.statcan.gc.ca/n1/en/pub/71-606-x/71-606-x2012006-eng.pdf?st=0eYm8aVe (accessed on 6 May 2020).
- Cullen, C.; Everson, K. Canadians Who Don’t Qualify for CERB Are Getting It Anyway—And Could Face Consequences. CBC, 1 May 2020. Available online: https://www.cbc.ca/news/politics/cerb-covid-pandemic-coronavirus-1.5552436 (accessed on 6 May 2020).
- Prosper Canada Centre. Financial Literacy and Newcomers to Canada; Prosper Canada Centre: Toronto, ON, Canada, November 2015; Available online: https://prospercanada.org/getattachment/3ff26769-c2d4-4d9e-82e9-f56467e4eb31/Financial-Literacy-and-Newcomers-to-Canada.aspx (accessed on 6 May 2020).
- Houle, R. Results from the 2016 Census: Syrian Refugees Who Resettled in Canada in 2015 and 2016; Statistics Canada: Ottawa, ON, USA, 12 February 2019. Available online: https://www150.statcan.gc.ca/n1/pub/75-006-x/2019001/article/00001-eng.htm (accessed on 6 May 2020).
- Canadian Council for Refugees. Did You Know…? Facts about Refugees and Refugee Claimants in Canada. Canadian Council for Refugees. Available online: https://ccrweb.ca/en/myths-facts (accessed on 6 May 2020).
- Young, L. Timeline: How Canada Has Changed Since Coronavirus Was Declared a Pandemic. Global News. 11 April 2020. Available online: https://globalnews.ca/news/6800118/pandemic-one-month-timeline/ (accessed on 11 April 2020).
- Cerna, L. Refugee Education: Integration Models and Practices in OECD Countries. OECD Working Papers. 13 May 2019. Available online: http://www.oecd.org/officialdocuments/publicdisplaydocumentpdf/?cote=EDU/WKP(2019)11&docLanguage=En (accessed on 13 April 2020).
- Manitoba Education. Life after War: Education as a Healing Process for Refugee and War Affected Children; Manitoba Education: Winnipeg, MB, Canada, 2012. Available online: https://www.edu.gov.mb.ca/k12/docs/support/law/full_doc.pdf (accessed on 12 April 2020).
- Moumné, R.; Sakai, L.; Rondin, E.; Pearson, C. Protecting the Right to Education for Refugees; UNESCO: Paris, France, 2017; Available online: https://unesdoc.unesco.org/ark:/48223/pf0000251076/PDF/251076eng.pdf.multi (accessed on 11 April 2020).
- General Comment No. 13: The Right to Education (Article 13) (1999). OHCHR, 8 December 1999. Available online: https://www.ohchr.org/EN/Issues/Education/Training/Compilation/Pages/d)GeneralCommentNo13Therighttoeducation(article13)(1999).aspx (accessed on 11 April 2020).
- Peel District School Board. A Community Of Care: Peel District School Board’s Learning and Support Plan; Peel District School Board: Geneva, Switzerland, 17 April 2020; Available online: http://www.peelschools.org/parents/student-health/coronavirus/Documents/A%20Community%20of%20Care%20-%20Peel%20District%20School%20Board%20Learning%20and%20Support%20Plan%20for%20Families.pdf (accessed on 13 April 2020).
- Rushowy, K. Ontario School Boards ‘Moving Mountains’ to Start Teaching Students Online during COVID-19 Lockdown; Queen’s Park Bureau: Toronto, ON, Canada, 2020; Available online: https://www.thestar.com/news/canada/2020/04/05/ontario-school-boards-moving-mountains-to-start-teaching-students-online-during-covid-19-lockdown.html (accessed on 14 April 2020).
- BC Ministry of Education. Frequently Asked Questions (FAQs) on Continuity of Learning; British Columbia Ministry of Education: Victoria, BC, Canada, 13 April 2020. Available online: https://www2.gov.bc.ca/assets/gov/education/administration/kindergarten-to-grade-12/safe-caring-orderly/bc-ministry-of-education-questions-and-answers-continuity-of-learning-k-12-education_system.pdf (accessed on 13 April 2020).
- UNHCR. 2012–2016 Education Strategy; UNHCR: Geneva, Switzerland, 2012; Available online: https://www.unhcr.org/protection/operations/5149ba349/unhcr-education-strategy-2012-2016.html (accessed on 11 April 2020).
- CDC. Children Benefit When Parents Have Safe, Stable, Nurturing Relationships. CDC. Available online: https://www.cdc.gov/violenceprevention/pdf/SSNRs-for-Parents.pdf (accessed on 17 April 2020).
- Government of Canada. Why Does Canada Resettle Refugees? Government of Canada: Ottawa, ON, Canada, 2020. Available online: https://www.cic.gc.ca/english/helpcentre/answer.asp?qnum=097&top=11 (accessed on 17 April 2020).
- Government of Canada. Report on Plans and Priorities 2015–2016; Government of Canada: Ottawa, ON, Canada, 2016. Available online: https://www.canada.ca/en/immigration-refugees-citizenship/corporate/publications-manuals/report-plans-priorities/2015-2016.html#a2.3.1 (accessed on 5 May 2020).
- Hyndman, J. Research Summary on Resettled Refugee Integration in Canada; UNHCR: Toronto, ON, Canada, 2011; Available online: https://www.unhcr.ca/wp-content/uploads/2014/10/RPT-2011-02-resettled-refugee-e.pdf (accessed on 5 May 2020).
- Hynie, M. Refugee Integration: Research and Policy. Peace Confl. J. Peace Psychol. 2018, 24, 265–276. [Google Scholar] [CrossRef]
- CTV News Toronto. Timeline: Emergency Orders Impacting Toronto and Ontario Amid the COVID-19 Pandemic; CTV News: Toronto, ON, Canada, 2020; Available online: https://toronto.ctvnews.ca/timeline-emergency-orders-impacting-toronto-and-ontario-amid-the-covid-19-pandemic-1.4881738 (accessed on 5 May 2020).
- Government of Canada. Resettled Refugees—Monthly IRCC Updates; Government of Canada: Ottawa, ON, Canada, 2018. Available online: https://open.canada.ca/data/en/dataset/4a1b260a-7ac4-4985-80a0-603bfe4aec11#wb-auto-6 (accessed on 24 April 2020).
- Goodall, C. Shouting towards the Sky: The Role of Religious Individuals, Communities, Organisations and Institutions in Support for Refugees and Asylum Seekers; UNHCR: Geneva, Switzerland, April 2015; Available online: https://www.unhcr.org/554764b49.pdf (accessed on 24 April 2020).
- Izri, T. Keeping the Faith during COVID-19: How Churches Are Adapting in the Pandemic Winnipeg. CTV News. 3 May 2020. Available online: https://winnipeg.ctvnews.ca/keeping-the-faith-during-covid-19-how-churches-are-adapting-in-the-pandemic-1.4923241 (accessed on 5 May 2020).
- Knope, J. Toronto Mosques to Broadcast Call to Prayer during Ramadan Amid COVID-19 Restrictions; CBC: Toronto, ON, Canada, 2020; Available online: https://www.cbc.ca/news/canada/toronto/toronto-mosques-call-to-prayer-speaker-ramadan-1.5550122 (accessed on 5 May 2020).
- Government of Northwest Territories. Mental Health and Social Distancing; Government of Northwest Territories: Yellowknife, NT, Canada, 23 April 2020. Available online: https://www.hss.gov.nt.ca/en/services/coronavirus-disease-covid-19/mental-health-and-social-distancing (accessed on 5 May 2020).
- CAMH. Refugee Mental Health; CAMH: Toronto, ON, Canada, 2015; Available online: https://www.camh.ca/en/camh-news-and-stories/refugee-mental-health (accessed on 5 May 2020).
- Bloomberg. The Coronavirus Knows No Borders, Says World Health Organization; Bloomberg: Geneva, Switzerland, 2020; Available online: https://www.bloomberg.com/news/videos/2020-02-27/the-coronavirus-knows-no-borders-says-world-health-organization-video (accessed on 18 April 2020).
- WHO. Updated WHO Recommendations for International Traffic in Relation to COVID-19 Outbreak; WHO: Geneva, Switzerland, 26 February 2020; Available online: https://www.who.int/news-room/articles-detail/updated-who-recommendations-for-international-traffic-in-relation-to-covid-19-outbreak (accessed on 20 April 2020).
- Lao, D. Canada-U.S. Land Border Closure Extended by 30 Days, Trudeau Says. Global News. 18 April 2020. Available online: https://globalnews.ca/news/6836829/coronavirus-trudeau-april-18/ (accessed on 20 April 2020).
- WHO. International Health Regulations (2005); World Health Organization: Geneva, Switzerland, 2006; Available online: https://apps.who.int/iris/bitstream/handle/10665/246107/9789241580496-eng.pdf?sequence=1 (accessed on 15 May 2020).
- Canadian Council for Refugees. Call for Border to be Reopened to Refugees; Canadian Council for Refugees: Montreal, QC, Canada, 2 April 2020; Available online: https://ccrweb.ca/en/media/call-border-be-reopened-refugees-02-04-2020 (accessed on 20 April 2020).
- Canadian Council for Refugees. These Moments Define Our Humanity: We Must Remain Open to Refugees and Vulnerable Migrants; Canadian Council for Refugees: Montreal, QC, Canada, 23 March 2020; Available online: https://ccrweb.ca/en/these-moments-define-our-humanity (accessed on 21 April 2020).
- Amnesty International. Americas: Release Migrants and Asylum-Seekers from Detention during COVID-19 Pandemic; Amnesty International: London, UK, 2020; Available online: https://www.amnesty.org/en/get-involved/take-action/release-migrants-and-asylum-seekers-from-detention-during-covid-19/ (accessed on 21 April 2020).
- Browne, R. The Number of Detainees Held in Canada’s Immigration Holding Centres is Declining Amid COVID-19 Fears. Global News. 3 April 2020. Available online: https://globalnews.ca/news/6774564/coronavirus-immigration-detainees/ (accessed on 2 May 2020).
- Browne, R. Canada Is Releasing Immigration Detainees at ‘Unprecedented’ Rates Amid COVID-19 Fears. Global News. 25 April 2020. Available online: https://globalnews.ca/news/6861756/canada-releasing-immigration-detainees-coronavirus-covid-19/ (accessed on 2 May 2020).
- Dickson, J. Four Asylum Seekers Turned away at Canada-U.S. BORDER; Globe and Mail: Ottawa, ON, Canada, 2020; Available online: https://www.theglobeandmail.com/politics/article-six-asylum-seekers-turned-away-at-canada-us-border/ (accessed on 11 April 2020).
- Canadian Council for Refugees. Background Information about Refugees; Canadian Council for Refugees: Montreal, QC, Canada, 2020; Available online: https://ccrweb.ca/en/information-refugees (accessed on 24 April 2020).
- Immigration and Refugee Board of Canada. Irregular Border Crosser Statistics; Government of Canada: Ottawa, ON, Canada, 2020. Available online: https://www.irb-cisr.gc.ca/en/statistics/Pages/Irregular-border-crosser-statistics.aspx#1 (accessed on 20 April 2020).
- Neuberger, L. Contemporary Asylum Policies between Human Rights Advocacy and Responsibility Outsourcing: The Cases of Australia and Canada. Secur. Peace 2016, 34, 29–37. Available online: https://www.jstor.org/stable/26428940 (accessed on 23 April 2020). [CrossRef]
- Hainsworth, J. Refugee Border Restrictions to Remain in Place. Glacier News. 4 April 2020. Available online: https://www.richmond-news.com/refugee-border-restrictions-to-remain-in-place-1.24112781 (accessed on 20 April 2020).
- Government of Canada. How the Coronavirus Disease (COVID-19) is Affecting Immigration, Refugees, Citizenship and Passport Services: Refugees; Government of Canada: Ottawa, ON, Canada, 2020. Available online: https://www.canada.ca/en/immigration-refugees-citizenship/services/coronavirus-covid19/refugees.html (accessed on 2 May 2020).
- Government of Canada. How Long Does It Take a Refugee to Get to Canada after Their Sponsorship Is Approved; Government of Canada: Ottawa, ON, Canada, 2020. Available online: https://www.cic.gc.ca/english/helpcentre/answer.asp?qnum=1499&top=11 (accessed on 2 May 2020).
- Government of Canada. How Canada’s Refugee System Works; Government of Canada: Ottawa, ON, Canada, 2019; Available online: https://www.canada.ca/en/immigration-refugees-citizenship/services/refugees/canada-role.html (accessed on 2 May 2020).
- Volkin, S. How Are Refugees Affected by COVID-19; John Hopkins University: Baltimore, MD, USA, 2020; Available online: https://hub.jhu.edu/2020/04/20/covid-19-refugees-asylum-seekers/ (accessed on 2 May 2020).

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Edmonds, J.; Flahault, A. Refugees in Canada during the First Wave of the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 947. https://doi.org/10.3390/ijerph18030947
Edmonds J, Flahault A. Refugees in Canada during the First Wave of the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2021; 18(3):947. https://doi.org/10.3390/ijerph18030947
Chicago/Turabian StyleEdmonds, Jennifer, and Antoine Flahault. 2021. "Refugees in Canada during the First Wave of the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 18, no. 3: 947. https://doi.org/10.3390/ijerph18030947
APA StyleEdmonds, J., & Flahault, A. (2021). Refugees in Canada during the First Wave of the COVID-19 Pandemic. International Journal of Environmental Research and Public Health, 18(3), 947. https://doi.org/10.3390/ijerph18030947