A Systematic Review of the Prevalence of Gestational Diabetes in Norway



Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Eligibility Criteria
2.3. Search Strategy
2.4. Study Selection and Data Extraction
2.5. Quality Assessment and Risk of Bias
3. Results
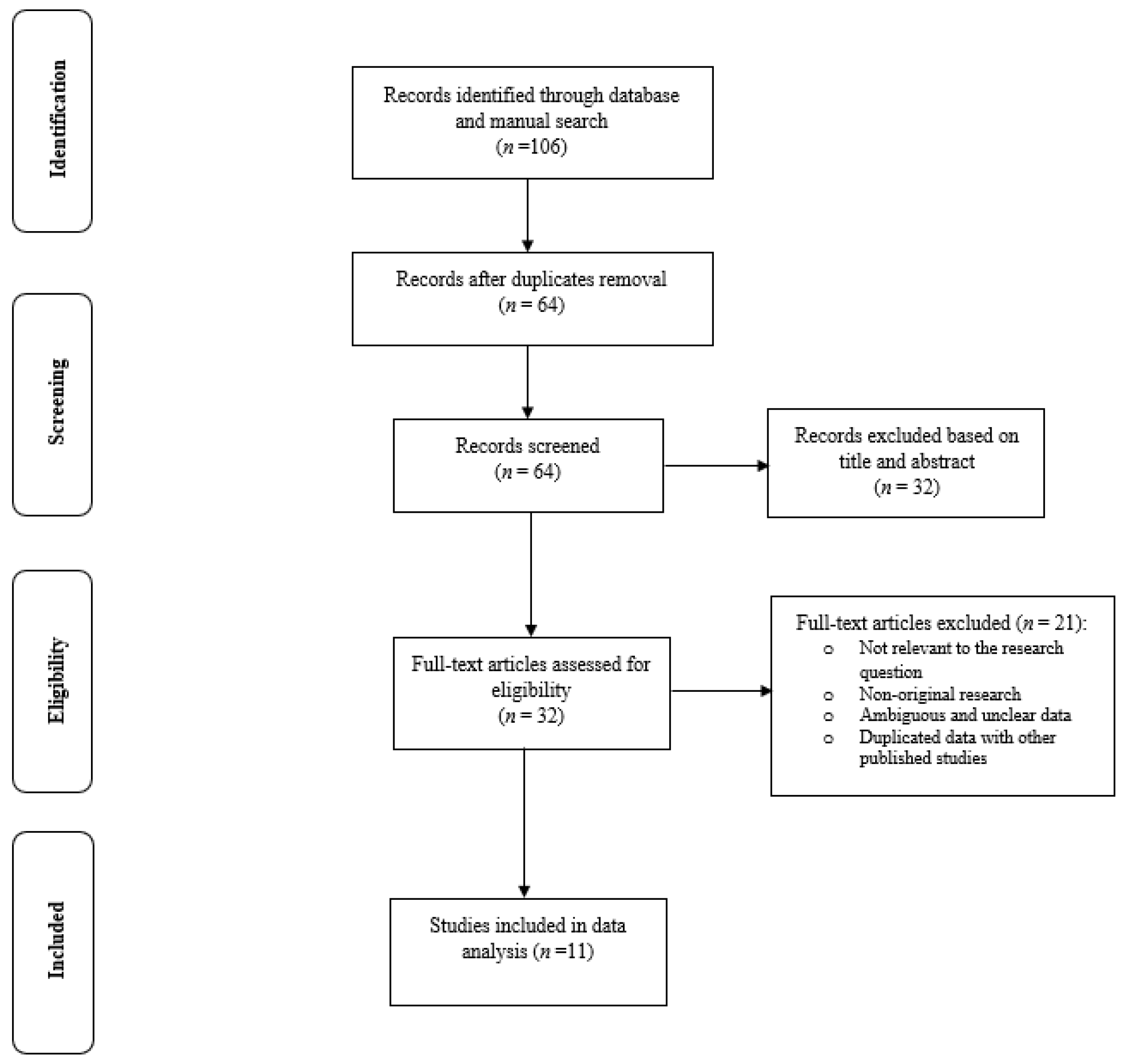
3.1. Search Results and Study Selections
3.2. General Characteristics of the Selected Studies
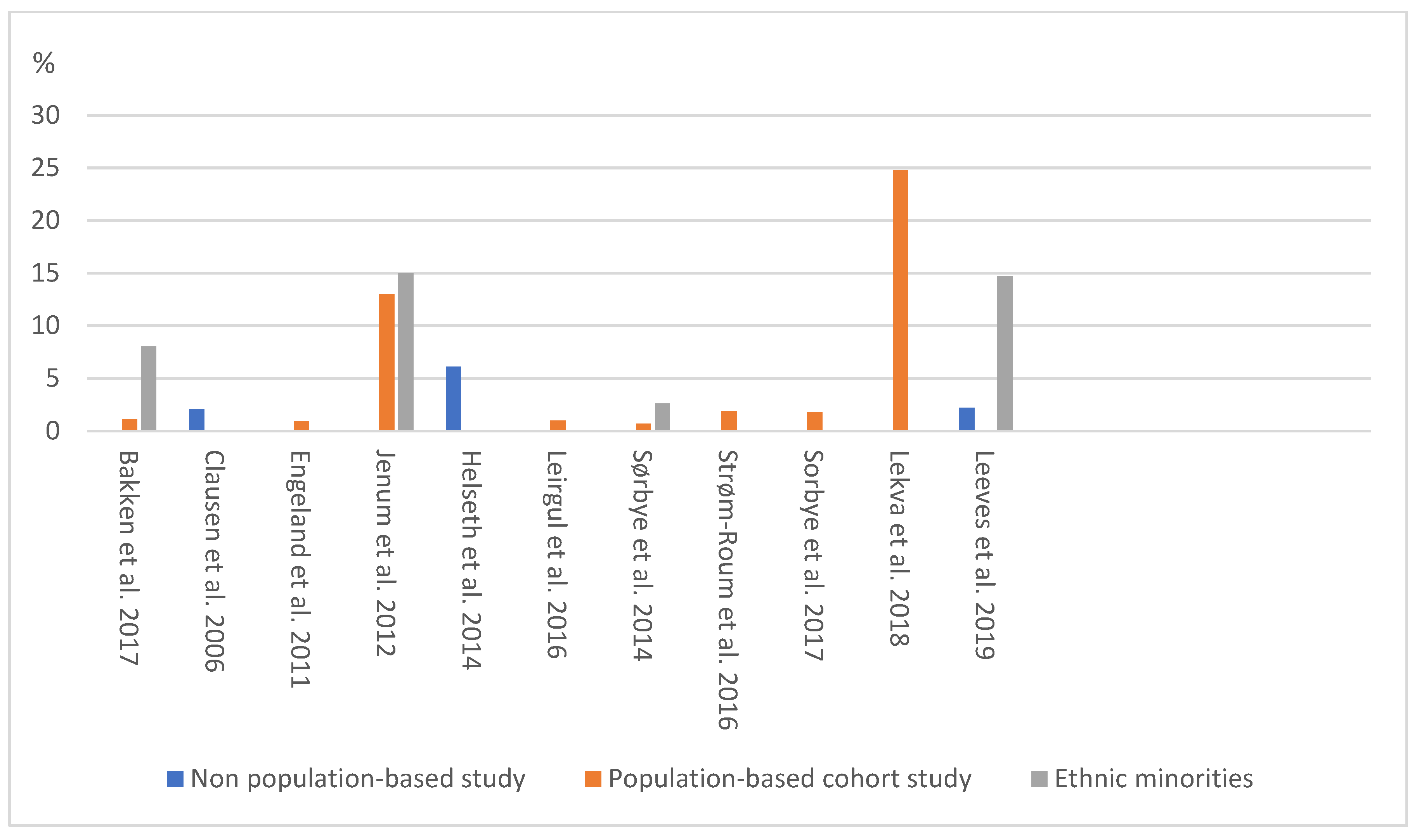
3.3. Prevalence of Gestational Diabetes Mellitus (GDM) in Norway
3.4. Quality Assessment and Risk of Bias Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Saravanan, P.; Diabetes in Pregnancy Working Group; Maternal Medicine Clinical Study Group; Royal College of Obstetricians. Gestational diabetes: Opportunities for improving maternal and child health. Lancet Diabetes Endocrinol. 2020, 8, 793–800. [Google Scholar] [CrossRef]
- American Diabetes Association. 2. Classification and diagnosis of diabetes: Standards of medical care in diabetes—2020. Diabetes Care 2020, 43, S14–S31. [Google Scholar] [CrossRef] [Green Version]
- Behboudi-Gandevani, S.; Amiri, M.; Yarandi, R.B.; Tehrani, F.R. The impact of diagnostic criteria for gestational diabetes on its prevalence: A systematic review and meta-analysis. Diabetol. Metab. Syndr. 2019, 11, 1–18. [Google Scholar] [CrossRef] [Green Version]
- Lee, K.W.; Ching, S.M.; Ramachandran, V.; Yee, A.; Hoo, F.K.; Chia, Y.; Sulaiman, W.A.W.; Suppiah, S.; Mohamed, M.H.; Veettil, S.K. Prevalence and risk factors of gestational diabetes mellitus in Asia: A systematic review and meta-analysis. BMC Pregnancy Childbirth 2018, 18, 1–20. [Google Scholar] [CrossRef] [Green Version]
- Muche, A.A.; Olayemi, O.O.; Kebede, Y. Prevalence and determinants of gestational diabetes mellitus in Africa based on the updated international diagnostic criteria: A systematic review and meta-analysis. Arch. Public Health 2019, 77, 1–20. [Google Scholar] [CrossRef] [Green Version]
- Eades, C.E.; Cameron, D.M.; Evans, J.M. Prevalence of gestational diabetes mellitus in Europe: A meta-analysis. Diabetes Res. Clin. Pr. 2017, 129, 173–181. [Google Scholar] [CrossRef]
- Plows, J.F.; Stanley, J.L.; Baker, P.; Reynolds, C.M.; Vickers, M.H. The Pathophysiology of Gestational Diabetes Mellitus. Int. J. Mol. Sci. 2018, 19, 3342. [Google Scholar] [CrossRef] [Green Version]
- Catalano, P.M. Trying to understand gestational diabetes. Diabet. Med. 2014, 31, 273–281. [Google Scholar] [CrossRef]
- Barbour, L.A.; McCurdy, C.E.; Hernandez, T.L.; Kirwan, J.P.; Catalano, P.M.; Friedman, J.E. Cellular Mechanisms for Insulin Resistance in Normal Pregnancy and Gestational Diabetes. Diabetes Care 2007, 30, S112–S119. [Google Scholar] [CrossRef] [Green Version]
- Sonagra, A.D.; Biradar, S.M.; Dattatreya, K.; DS, J.M. Normal Pregnancy—A State of Insulin Resistance. J. Clin. Diagn. Res. 2014, 8, CC01–3. [Google Scholar] [CrossRef] [PubMed]
- Domanski, G.; Lange, A.E.; Ittermann, T.; Allenberg, H.; Spoo, R.A.; Zygmunt, M.; Heckmann, M. Evaluation of neonatal and maternal morbidity in mothers with gestational diabetes: A population-based study. BMC Pregnancy Childbirth 2018, 18, 1–11. [Google Scholar] [CrossRef]
- Vounzoulaki, E.; Khunti, K.; Abner, S.C.; Tan, B.K.; Davies, M.J.; Gillies, C.L. Progression to type 2 diabetes in women with a known history of gestational diabetes: Systematic review and meta-analysis. BMJ 2020, 369, m1361. [Google Scholar] [CrossRef]
- Kramer, C.K.; Campbell, S.; Retnakaran, R. Gestational diabetes and the risk of cardiovascular disease in women: A systematic review and meta-analysis. Diabetologia 2019, 62, 905–914. [Google Scholar] [CrossRef] [Green Version]
- Xu, Y.; Shen, S.; Sun, L.; Yang, H.; Jin, B.; Cao, X. Metabolic Syndrome Risk after Gestational Diabetes: A Systematic Review and Meta-Analysis. PLoS ONE 2014, 9, e87863. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Behboudi-Gandevani, S.; Tehrani, F.R.; Rahmati, M.; Amiri, M.; Azizi, F. Trend of various adiposity indices in women with and without history of gestational diabetes: A population-based cohort study. BMC Endocr. Disord. 2019, 19, 24. [Google Scholar] [CrossRef] [PubMed]
- McMahon, L.E.; O’Malley, E.G.; Reynolds, C.M.E.; Turner, M.J. The impact of revised diagnostic criteria on hospital trends in gestational diabetes mellitus rates in a high income country. BMC Health Serv. Res. 2020, 20, 1–11. [Google Scholar] [CrossRef]
- Ferrara, A. Increasing Prevalence of Gestational Diabetes Mellitus: A public health perspective. Diabetes Care 2007, 30, S141–S146. [Google Scholar] [CrossRef] [Green Version]
- Brown, F.M.; Wyckoff, J. Application of One-Step IADPSG Versus Two-Step Diagnostic Criteria for Gestational Diabetes in the Real World: Impact on Health Services, Clinical Care, and Outcomes. Curr. Diabetes Rep. 2017, 17, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fadl, H.E.; Simmons, D. Trends in diabetes in pregnancy in Sweden 1998–2012. BMJ Open Diabetes Res. Care 2016, 4, e000221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeppesen, C.; Maindal, H.T.; Kristensen, J.K.; Ovesen, P.G.; Witte, D.R. National study of the prevalence of gestational diabetes mellitus among Danish women from 2004 to 2012. Scand. J. Public Health 2017, 45, 811–817. [Google Scholar] [CrossRef]
- Statistics Norway. Mean Age of Parent at First Child’s Birth 1961–2019. 2021. Available online: https://www.ssb.no/en/statbank/table/07872 (accessed on 20 January 2021).
- Norwegian Institute for Public Health. Diabetes-in-Norway. 2017. Available online: https://www.fhi.no/en/op/hin/health-disease/diabetes-in-norway---public-health-/ (accessed on 20 January 2021).
- Helsedirektoratet. Diabetes: Retningslinjer om Diabetes og Svangerskapsdiabetes. Opplæringsmateriell til helsepersonell. 2020. Available online: https://www.helsedirektoratet.no/retningslinjer/svangerskapsdiabetes (accessed on 9 January 2021).
- The Norwegian Institute of Public Health. The Effectiveness of Screening all Pregnant Women Versus Pregnant Women with Risk Factors for Gestational Diabetes. 2019. Available online: https://www.fhi.no/en/publ/2019/effekten-av-a-screene-alle-gravide-sammenlignet-med-a-screene-gravide-med-r/ (accessed on 9 January 2021).
- Borgen, I.; Garnweidner-Holme, L.; Jacobsen, A.F.; Fayyad, S.; Småstuen, M.C.; Lukasse, M. Knowledge of gestational diabetes mellitus at first consultation in a multi-ethnic pregnant population in the Oslo region, Norway—A cross-sectional study. Ethn. Health 2019, 2019, 1–14. [Google Scholar] [CrossRef]
- Jenum, A.K.; Mørkrid, K.; Sletner, L.; Vangen, S.; Torper, J.L.; Nakstad, B.; Voldner, N.; Rognerud-Jensen, O.H.; Berntsen, S.; Mosdøl, A.; et al. Impact of ethnicity on gestational diabetes identified with the WHO and the modified International Association of Diabetes and Pregnancy Study Groups criteria: A population-based cohort study. Eur. J. Endocrinol. 2012, 166, 317–324. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [Green Version]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomized Studies in Meta-Analyses; Ottawa Hospital Research Institute: Ottawa, ON, Canada; Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp. (accessed on 16 December 2019).
- Clausen, T.; Øyen, N.; Henriksen, T. Pregnancy complications by overweight and residential area. A prospective study of an urban Norwegian cohort. Acta Obstet. Gynecol. Scand. 2006, 85, 526–533. [Google Scholar] [CrossRef] [PubMed]
- Engeland, A.; Bjørge, T.; Daltveit, A.K.; Skurtveit, S.; Vangen, S.; Vollset, S.E.; Furu, K. Risk of diabetes after gestational diabetes and preeclampsia. A registry-based study of 230,000 women in Norway. Eur. J. Epidemiol. 2011, 26, 157–163. [Google Scholar] [CrossRef] [Green Version]
- Helseth, R.; Salvesen, Ø.; Stafne, S.N.; Mørkved, S.; Salvesen, K.Å.; Carlsen, S.M. Gestational diabetes mellitus among Nordic Caucasian women: Prevalence and risk factors according to WHO and simplified IADPSG criteria. Scand. J. Clin. Lab. Investig. 2014, 74, 620–628. [Google Scholar] [CrossRef]
- Leirgul, E.; Brodwall, K.; Greve, G.; Vollset, S.E.; Holmstrøm, H.; Tell, G.S.; Øyen, N. Maternal Diabetes, Birth Weight, and Neonatal Risk of Congenital Heart Defects in Norway, 1994–2009. Obstet. Gynecol. 2016, 128, 1116–1125. [Google Scholar] [CrossRef] [PubMed]
- Strøm-Roum, E.M.; Tanbo, T.; Eskild, A. The associations of maternal body mass index with birthweight and placental weight. Does maternal diabetes matter? A population study of 106 191 pregnancies. Acta Obstet. Gynecol. Scand. 2016, 95, 1162–1170. [Google Scholar] [CrossRef]
- Sørbye, L.M.; Skjaerven, R.; Klungsøyr, K.; Morken, N.-H. Gestational diabetes mellitus and interpregnancy weight change: A population-based cohort study. PLoS Med. 2017, 14, e1002367. [Google Scholar] [CrossRef]
- Lekva, T.; Godang, K.; Michelsen, A.E.; Qvigstad, E.; Normann, K.R.; Norwitz, E.R.; Aukrust, P.; Henriksen, T.; Bollerslev, J.; Roland, M.C.P.; et al. Prediction of Gestational Diabetes Mellitus and Pre-diabetes 5 Years Postpartum using 75 g Oral Glucose Tolerance Test at 14-16 Weeks’ Gestation. Sci. Rep. 2018, 8, 13392. [Google Scholar] [CrossRef] [PubMed]
- Leeves, L.T.; Andreasen, C.; Marrable, S.; Glasø, M.U.; Rostad, M.-K.; Olsen, I.P.; Bjørnerem, Å. Prevalens av diabetes blant gravide og svangerskapsutfall i Nordland og Troms 2004–15. Tidsskr. Den Nor. Legeforening 2019, 139. [Google Scholar] [CrossRef] [PubMed]
- Sørbye, I.K.; Daltveit, A.K.; Sundby, J.; Vangen, S. Preterm subtypes by immigrants’ length of residence in Norway: A population-based study. BMC Pregnancy Childbirth 2014, 14, 239. [Google Scholar] [CrossRef] [Green Version]
- Bakken, K.S.; Skjeldal, O.H.; Stray-Pedersen, B. Obstetric Outcomes of First- and Second-Generation Pakistani Immigrants: A Comparison Study at a Low-Risk Maternity Ward in Norway. J. Immigr. Minor. Health 2015, 19, 33–40. [Google Scholar] [CrossRef]
- Poolsup, N.; Suksomboon, N.; Amin, M. Effect of Treatment of Gestational Diabetes Mellitus: A Systematic Review and Meta-Analysis. PLoS ONE 2014, 9, e92485. [Google Scholar] [CrossRef] [Green Version]
- Lavery, J.A.; Friedman, A.M.; Keyes, K.M.; Wright, J.D.; Ananth, C.V. Gestational diabetes in the United States: Temporal changes in prevalence rates between 1979 and 2010. BJOG: Int. J. Obstet. Gynaecol. 2017, 124, 804–813. [Google Scholar] [CrossRef]
- Zhu, Y.; Zhang, C.-L. Prevalence of Gestational Diabetes and Risk of Progression to Type 2 Diabetes: A Global Perspective. Curr. Diabetes Rep. 2016, 16, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Buckley, B.S.; Harreiter, J.; Damm, P.; Corcoy, R.; Chico, A.; Simmons, D.; Vellinga, A.; Dunne, F.; on behalf of the DALI Core Investigator group. Gestational diabetes mellitus in Europe: Prevalence, current screening practice and barriers to screening. A review. Diabet. Med. 2012, 29, 844–854. [Google Scholar] [CrossRef]
- Nijs, H.; Benhalima, K. Gestational Diabetes Mellitus and the Long-Term Risk for Glucose Intolerance and Overweight in the Offspring: A Narrative Review. J. Clin. Med. 2020, 9, 599. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Billionnet, C.; Mitanchez, D.; Weill, A.; Nizard, J.; Alla, F.; Hartemann, A.; Jacqueminet, S. Gestational diabetes and adverse perinatal outcomes from 716,152 births in France in 2012. Diabetologia 2017, 60, 636–644. [Google Scholar] [CrossRef]
- Miao, M.; Dai, M.; Zhang, Y.; Sun, F.; Guo, X.; Sun, G. Influence of maternal overweight, obesity and gestational weight gain on the perinatal outcomes in women with gestational diabetes mellitus. Sci. Rep. 2017, 7, 1–8. [Google Scholar] [CrossRef]
- Kuo, C.-H.; Chen, S.-C.; Fang, C.-T.; Nien, F.-J.; Wu, E.-T.; Lin, S.-Y.; Chuang, L.-M.; Lee, C.-N.; Li, H. Screening gestational diabetes mellitus: The role of maternal age. PLoS ONE 2017, 12, e0173049. [Google Scholar] [CrossRef] [PubMed]
- Hedderson, M.M.; Darbinian, J.A.; Ferrara, A. Disparities in the risk of gestational diabetes by race-ethnicity and country of birth. Paediatr. Périnat. Epidemiol. 2010, 24, 441–448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pu, J.; Zhao, B.; Wang, E.J.; Nimbal, V.; Osmundson, S.; Kunz, L.; Popat, R.A.; Chung, S.; Palaniappan, L.P. Racial/Ethnic Differences in Gestational Diabetes Prevalence and Contribution of Common Risk Factors. Paediatr. Périnat. Epidemiol. 2015, 29, 436–443. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Authors, Year | Research Design | Eligibility Criteria of the Population | Data Resource | Research Year | GDM Diagnostic Criteria | Sample Size, n | GDM Prevalence n (%) |
|---|---|---|---|---|---|---|---|
| Bakken et al., (2017) [38] | Population-based study | Inclusion: First registered birth for women of Pakistani and Norwegian origin who delivered at Baerum Hospital Exclusion: Stillbirths cases, women of other country origin, type 1 diabetes, preterm labor before week 35, pregnancies with more than two fetuses, or fetuses with known health issues | Baerum Hospital and Medical Birth Registry of Norway and Statistics Norway | 2006–2013 | National Criteria: FBS ≥7.0 mmol/L and/or OGTT BS-2h ≥7.8 mmol/L | 1. Norwegian origin: 8237 2. Pakistan origin: 287 | 1. 1. Norwegian origin: 1.1 2. Pakistan origin: 8.01 |
| Clausen et al., (2006) [29] | Non population-based study | Inclusion: Norwegian-speaking women, living in Oslo city that had childbirth at Aker Hospital Exclusion: Type 1 diabetes, multiple pregnancies, abortion | Aker Hospital | 1995–1997 | National Criteria: OGTT BS-2h > 7.8 mmol/L | 3677 | 78 (2.1) |
| Engeland et al., (2011) [30] | Population-based cohort study | Inclusion: First pregnancy, lasting more than 22 weeks Exclusion: Pregestational diabetes and hypertension, polycystic ovary syndrome | Medical Birth Registry of Norway and Norwegian Prescription Database | 2004–2008 | National Criteria: WHO-1999: FBS ≥7.0 mmol/L and/or OGTT BS-2h ≥7.8 mmol/L | 1. 2004: 55,131 2. 2005: 52,529 3. 2006: 45,737 4: 2007: 38,039 6. 2008: 35,396 Total: 226,832 | 1. 2004: 472 (0.85) 2. 2005: 433 (0.82) 3. 2006: 478 (1.04) 4: 2007: 388 (1.02) 6. 2008: 427 (1.20) Total: 2198 (0.96) |
| Jenum, et al., (2012) [26] | Population-based study | Inclusion: Living in the districts, planned to give birth in the study hospitals, <20 weeks, ability to communicate and give written consent Exclusion: Pregestational diabetes or other diseases, need for intensive hospital follow-up during pregnancy | Three Public Child Health Clinics in Groruddalen in Oslo | 2008–2010 | 1. National Criteria: WHO-1999: FBS ≥7.0 mmol/L and/or OGTT BS-2h ≥7.8 mmol/L: 2. modified IADPSG: FBS ≥5.1 mmol/L and/or OGTT BS-2h ≥8.5 mmol/L; | Total: 759 Western Europeans: 313 Ethnic minorities: 446 | 1. Total: 99 (13) 1. Western Europeans: 34 (11) 1. Ethnic minorities 67 (15) 2. Total: 239 (31.5) 2. Western Europeans: 75 (24) 2. Ethnic minorities 165 (37) |
| Helseth, et al., (2014) [31] | Non population-based study | Inclusion: Age ≥18 years, singleton live fetus Exclusion: High-risk pregnancies, diseases that interfered with participation in the study | St. Olavs Hospital, Trondheim University Hospital; Stavanger University Hospital | 2007–2009 | 1. National Criteria: WHO-1999: FBS ≥7.0 mmol/L and/or OGTT BS-2h ≥7.8 mmol/L; 2. Simplified IADPSG: FBS ≥5.1 mmol/L and/or OGTT BS-2h ≥8.5 mmol/L | 687 | 1. 42 (6.1) 2. 51 (7.4) |
| Leirgul et al., (2016) [32] | Population-based study | Inclusion: Registered birth Exclusion: Antidiabetic medication during pregnancy without a registered diabetes diagnosis, fetal chromosomal aberrations and relevant genetic disorders, multiple births | Medical Birth Registry of Norway | 1994–2009 | National Criteria: WHO-1999: FBS ≥7.0 mmol/L and/or OGTT BS-2h ≥7.8 mmol/L | 914,427 | 9726 (1) |
| Sørbye et al., (2014) [37] | Population-based study | Inclusion: Singletons born Exclusion: Stillbirths <28 weeks, births that occurred before registered immigration, missing information on gestational length and cases with improbable birthweights based on gestational length and sex | Medical Birth Registry of Norway | 1990–2009 | National Criteria: FBS ≥7.0 mmol/L and/or OGTT BS-2h ≥7.8 mmol/L | 1.Norway: 868,832 2. immigrant: 40,709 | 1. 0.7 2. 2.6 |
| Strøm-Roum et al., (2016) [33] | Population-based study | Inclusion: Singleton pregnancies during the study period Exclusion: Missing information on maternal weight and height, offspring birthweight between 250–6500 g, recorded placental weight between 25–2500 g, pregnancy on weeks 22–45 | Medical Birth Registry of Norway | 2009–2012 | National Criteria: WHO-1999: OGTT BS-2h ≥7.8–11 mmol/L | 105,458 | 2078 (1.9) |
| Sorbye et al., (2017) [34] | Population-based study | Inclusion: Mothers with 1st and 2nd child Exclusion: Prepregnant BMI <15, interpregnancy weight change ±30 | Medical Birth Registry of Norway | 2006–2014 | National Criteria: WHO-1999: OGTT BS-2h ≥7.8–11 mmol/L | 24,198 | 439 (1.8) |
| Lekva, et al., (2018) [35] | Population-based study | Inclusion: Low-risk women of Scandinavian heritage Exclusion: Multiple pregnancies, known pre-gestational diabetes and any severe chronic diseases (lung, cardiac, gastrointestinal or renal). | Oslo University Hospital | 2002–2008 | 1. WHO 2013: FBS ≥5.1 mmol/L, OGTT BS-1h ≥10 mmol/L, OGTT BS-2h ≥8.5 mmol/L; 2. 2017-Revised National criteria: FBS ≥5.3 mmol/L, OGTT BS-2h ≥9 mmol/L | 1. 985; 2. 987 | 1. 244 (24.8) 2. 91 (9.2) |
| Leeves, et al., (2019) [36] | Population-based study | Inclusion: Women gave birth at study hospitals Exclusion: Multiple pregnancy | Hospitals in Nordland and Troms counties | 2004–2015 | National Criteria: FBS ≥7.0 mmol/L and/or OGTT BS-2h ≥7.8 mmol/L | 1. 2004–2006: 7227; 2. 2007–2009: 9457; 3. 2010–2012:9318; 4. 2013–2015: 8913; 5. Total: 34,915; 6. non-European ethnicity: 755 | 1. 2004–2006: 72 (1) 2. 2007–2009: NM 3. 2010–2012: NM 4. 2013–2015: 356 (4) 5. Total: 782 (2.2) 6. non-European ethnicity: 111 (14.7) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Behboudi-Gandevani, S.; Parajuli, R.; Vaismoradi, M. A Systematic Review of the Prevalence of Gestational Diabetes in Norway. Int. J. Environ. Res. Public Health 2021, 18, 1423. https://doi.org/10.3390/ijerph18041423
Behboudi-Gandevani S, Parajuli R, Vaismoradi M. A Systematic Review of the Prevalence of Gestational Diabetes in Norway. International Journal of Environmental Research and Public Health. 2021; 18(4):1423. https://doi.org/10.3390/ijerph18041423
Chicago/Turabian StyleBehboudi-Gandevani, Samira, Ranjan Parajuli, and Mojtaba Vaismoradi. 2021. "A Systematic Review of the Prevalence of Gestational Diabetes in Norway" International Journal of Environmental Research and Public Health 18, no. 4: 1423. https://doi.org/10.3390/ijerph18041423
APA StyleBehboudi-Gandevani, S., Parajuli, R., & Vaismoradi, M. (2021). A Systematic Review of the Prevalence of Gestational Diabetes in Norway. International Journal of Environmental Research and Public Health, 18(4), 1423. https://doi.org/10.3390/ijerph18041423