
Neighborhood Environmental Factors and Physical Activity Status among Rural Older Adults in Japan

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Subjects
2.3. Outcome
2.4. Exposure Variables: Neighborhood Environmental Factors
2.5. Covariates
2.6. Statistical Analysis
2.7. Ethical Considerations
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Action Plan for the Prevention and Control of Noncommunicable Diseases: 2013–2020. 2013. Available online: http://apps.who.int/iris/bitstream/10665/94384/1/9789241506236_eng.pdf (accessed on 3 June 2020).
- Bull, F.; Goenka, S.; Lambert, V.; Pratt, M.; Prabhakaran, D.; Anand, S.; Gaziano, T.A.; Mbanya, J.-C.; Wu, Y.; Nugent, R. Physical Activity for the Prevention of Cardiometabolic Disease. In Cardiovascular, Respiratory, and Related Disorders, 3rd ed.; World Bank: Washington, DC, USA, 2017; pp. 79–99. Available online: http://www.ncbi.nlm.nih.gov/books/NBK525161/ (accessed on 8 June 2020).
- Ding, D.; Lawson, K.D.; Kolbe-Alexander, T.L.; Finkelstein, E.A.; Katzmarzyk, P.T.; Van Mechelen, W.; Pratt, M. The economic burden of physical inactivity: A global analysis of major non-communicable diseases. Lancet 2016, 388, 1311–1324. [Google Scholar] [CrossRef]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Worldwide trends in insufficient physical activity from 2001 to 2016: A pooled analysis of 358 population-based surveys with 1·9 million participants. Lancet Glob. Health 2018, 6, e1077–e1086. [Google Scholar] [CrossRef] [Green Version]
- Hallal, P.C.; Andersen, L.B.; Bull, F.C.; Guthold, R.; Haskell, W.L.; Ekelund, U.; Lancet Physical Activity Series Working Group. Global physical activity levels: Surveillance progress, pitfalls, and prospects. Lancet 2012, 380, 247–257. [Google Scholar] [CrossRef]
- World Health Organization. Global Strategy on Diet, Physical Activity and Health. 2004. Available online: http://www.who.int/ncds/prevention/global-strategy-diet-physical-activity-2004-goals/en/ (accessed on 30 June 2020).
- World Health Organization. Global Action Plan on Physical Activity 2018–2030: More Active People for a Healthier World. 2018. Available online: https://www.who.int/ncds/prevention/physical-activity/global-action-plan-2018-2030/en/ (accessed on 1 June 2020).
- Sallis, J.F.; Owen, N.; Fotheringham, M.J. Behavioral epidemiology: A systematic framework to classify phases of research on health promotion and disease prevention. Ann. Behav. Med. 2000, 22, 294–298. [Google Scholar] [CrossRef]
- Bauman, A.E.; Reis, R.S.; Sallis, J.F.; Wells, J.C.; Loos, R.J.F.; Martin, B.W. Correlates of physical activity: Why are some people physically active and others not? Lancet 2012, 380, 258–271. [Google Scholar] [CrossRef]
- Sallis, J.F.; Owen, N.; Fisher, E.B. Ecological models of health behavior. In Health Behavior and Health Education: Theory, Research, and Practice, 4th ed.; Jossey-Bass: San Francisco, CA, USA, 2008; pp. 465–485. [Google Scholar]
- UN. Population Division. World Population Ageing. 2019. Available online: http://digitallibrary.un.org/record/3846855 (accessed on 30 June 2020).
- World Health Organization. World Report on Ageing and Health. 2015. Available online: http://www.who.int/ageing/events/world-report-2015-launch/en/ (accessed on 30 June 2020).
- Bauman, A.; Merom, D.; Bull, F.C.; Buchner, D.M.; Singh, M.A.F. Updating the Evidence for Physical Activity: Summative Reviews of the Epidemiological Evidence, Prevalence, and Interventions to Promote “Active Aging”. Gerontologist 2016, 56, S268–S280. [Google Scholar] [CrossRef]
- Duncan, D.T.; Kawachi, I. Neighborhoods and Health: A Progress Report; Oxford University Press: Oxford, UK, 2018; Available online: https://www.oxfordscholarship.com/view/10.1093/oso/9780190843496.001.0001/oso-9780190843496-chapter-1 (accessed on 7 August 2020).
- Barnett, D.W.; Barnett, A.; Nathan, A.; Van Cauwenberg, J.; Cerin, E.; Council on Environment and Physical Activity (CEPA)—Older Adults working group. Built environmental correlates of older adults’ total physical activity and walking: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 1–24. [Google Scholar] [CrossRef] [Green Version]
- Cerin, E.; Nathan, A.; van Cauwenberg, J.; Barnett, D.W.; Barnett, A.; Council on Environment and Physical Activity (CEPA)—Older Adults working group. The neighbourhood physical environment and active travel in older adults: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 1–23. [Google Scholar] [CrossRef] [Green Version]
- Heath, G.W.; Parra, D.C.; Sarmiento, O.L.; Andersen, L.B.; Owen, N.; Goenka, S.; Montes, F.; Brownson, R.C.; for the Lancet Physical Activity Series Working Group. Evidence-based intervention in physical activ-ity: Lessons from around the world. The Lancet 2012, 380, 272–281. [Google Scholar] [CrossRef] [Green Version]
- Berry, N.; Coffee, N.T.; Nolan, R.; Dollman, J.; Sugiyama, T. Neighbourhood Environmental Attributes Associated with Walking in South Australian Adults: Differences between Urban and Rural Areas. Int. J. Environ. Res. Public Health 2017, 14, 965. [Google Scholar] [CrossRef] [Green Version]
- Kikuchi, H.; Nakaya, T.; Hanibuchi, T.; Fukushima, N.; Amagasa, S.; Oka, K.; Sallis, J.F.; Inoue, S. Objectively Measured Neighborhood Walkabil-ity and Change in Physical Activity in Older Japanese Adults: A Five-Year Cohort Study. Int. J. Environ. Res. Public Health 2018, 15, 1814. [Google Scholar] [CrossRef] [Green Version]
- Koohsari, M.J.; Sugiyama, T.; Shibata, A.; Ishii, K.; Liao, Y.; Hanibuchi, T.; Owen, N.; Oka, K. Associations of street layout with walking and sed-entary behaviors in an urban and a rural area of Japan. Health Place 2017, 45, 64–69. [Google Scholar] [CrossRef]
- Eberhardt, M.S.; Pamuk, E.R. The Importance of Place of Residence: Examining Health in Rural and Nonrural Areas. Am. J. Public Health 2004, 94, 1682–1686. [Google Scholar] [CrossRef]
- Bauman, A.E.; Sallis, J.F.; Dzewaltowski, D.A.; Owen, N. Toward a better understanding of the influences on physical activity: The role of determinants, correlates, causal variables, mediators, moderators, and confounders. Am. J. Prev. Med. 2002, 23, 5–14. [Google Scholar] [CrossRef]
- Statistics Information of Shimane. Ageing Rate by Municipalities in Shimane Prefecture. 2018. Available online: https://www.pref.shimane.lg.jp/medical/kenko/kenko/kenko_hukushi/shimanenokenkohukushi2018.data/07-06_sityousonkoureikaritu.pdf?site=sp (accessed on 20 October 2020).
- Statistics Information of Shimane. Statistics Data by Municipalities. 2019. Available online: https://pref.shimane-toukei.jp/index.php?view=3830 (accessed on 13 October 2020).
- Kawakami, R.; Miyachi, M. Validity of a standard questionnaire to assess physical activity for specific medical checkups and health guidance. Jpn. J. Public Health 2010, 57, 891–899. [Google Scholar]
- Abe, T.; Okuyama, K.; Hamano, T.; Takeda, M.; Isomura, M.; Nabika, T. Hilly environment and physical activity among communi-ty-dwelling older adults in Japan: A cross-sectional study. BMJ Open 2020, 10, e033338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujiwara, T.; Takamoto, I.; Amemiya, A.; Hanazato, M.; Suzuki, N.; Nagamine, Y.; Sasaki, Y.; Tani, Y.; Yazawa, A.; Inoue, Y.; et al. Is a hilly neighborhood environment asso-ciated with diabetes mellitus among older people? Results from the JAGES 2010 study. Soc. Sci. Med. 2017, 182, 45–51. [Google Scholar] [CrossRef]
- Hanibuchi, T.; Kawachi, I.; Nakaya, T.; Hirai, H.; Kondo, K. Neighborhood built environment and physical activity of Japanese older adults: Results from the Aichi Gerontological Evaluation Study (AGES). BMC Public Health 2011, 11, 657. [Google Scholar] [CrossRef] [Green Version]
- Okuyama, K.; Abe, T.; Hamano, T.; Takeda, M.; Sundquist, K.; Sundquist, J.; Nabika, T. Hilly neighborhoods are associated with increased risk of weight gain among older adults in rural Japan: A 3-years follow-up study. Int. J. Health Geogr. 2019, 18, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mavoa, S.; Bagheri, N.; Koohsari, M.J.; Kaczynski, A.T.; Lamb, K.E.; Oka, K.; O’Sullivan, D.; Witten, K. How Do Neighbourhood Definitions Influence the Associations between Built Environment and Physical Activity? Int. J. Environ. Res. Public Health 2019, 16, 1501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hosokawa, R.; Kondo, K.; Ito, M.; Miyaguni, Y.; Mizutani, S.; Goto, F.; Abe, Y.; Tsuge, Y.; Handa, Y.; Ojima, T.; et al. The Effectiveness of Japan’s Community Centers in Facilitating Social Participation and Maintaining the Functional Capacity of Older People. Res. Aging 2018, 41, 315–335. [Google Scholar] [CrossRef] [PubMed]
- Soma, Y.; Tsunoda, K.; Kitano, N.; Jindo, T.; Tsuji, T.; Saghazadeh, M.; Okura, T. Relationship between built environment attributes and physical function in Japanese community-dwelling older adults. Geriatr. Gerontol. Int. 2017, 17, 382–390. [Google Scholar] [CrossRef]
- Kurt Omurlu, I.; Ture, M.; Tokatli, F. The comparisons of random survival forests and Cox regression analysis with simulation and an application related to breast cancer. Expert Syst. Appl. 2009, 36, 8582–8588. [Google Scholar] [CrossRef]
- Lübs, L.; Peplies, J.; Drell, C.; Bammann, K. Cross-sectional and longitudinal factors influencing physical activity of 65 to 75-year-olds: A pan European cohort study based on the survey of health, ageing and retirement in Europe (SHARE). BMC Geriatr. 2018, 18, 94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tani, Y.; Suzuki, N.; Fujiwara, T.; Hanazato, M.; Kondo, N.; Miyaguni, Y.; Kondo, K. Neighborhood food environment and mortality among older Japanese adults: Results from the JAGES cohort study. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 101. [Google Scholar] [CrossRef] [PubMed]
- Momosaki, R.; Wakabayashi, H.; Maeda, K.; Shamoto, H.; Nishioka, S.; Kojima, K.; Tani, Y.; Suzuki, N.; Hanazato, M.; Kondo, K. Association between Food Store Availabil-ity and the Incidence of Functional Disability among Community-Dwelling Older Adults: Results from the Japanese Geronto-logical Evaluation Cohort Study. Nutrients 2019, 11, 2369. [Google Scholar] [CrossRef] [Green Version]
- Ishwaran, H.; Kogalur, U.B.; Blackstone, E.H.; Lauer, M.S. Random survival forests. Ann. Appl. Stat. 2008, 2, 841–860. [Google Scholar] [CrossRef]
- Datema, F.R.; Moya, A.; Krause, P.J.; Bäck, T.; Willmes, L.; Langeveld, T.P.M.; De Jong, R.J.B.; Blom, H.M. Novel head and neck cancer survival analysis approach: Random survival forests versus cox proportional hazards regression. Head Neck 2011, 34, 50–58. [Google Scholar] [CrossRef]
- Miao, F.; Cai, Y.-P.; Zhang, Y.-T.; Li, C.-Y. Is Random Survival Forest an Alternative to Cox Proportional Model on Predicting Car-diovascular Disease? In European Conference of the International Federation for Medical and Biological Engineering, 6th ed.; Lacković, I., Vasic, D., Eds.; Springer: Cham, Switzerland, 2015; pp. 740–743. [Google Scholar]
- Chou, W.-T.; Tomata, Y.; Watanabe, T.; Sugawara, Y.; Kakizaki, M.; Tsuji, I. Relationships between changes in time spent walking since middle age and incident functional disability. Prev. Med. 2014, 59, 68–72. [Google Scholar] [CrossRef]
- Wang, D.; Lau, K.K.-L.; Yu, R.H.Y.; Wong, S.Y.S.; Kwok, T.C.Y.; Woo, J. Neighbouring green space and all-cause mortality in elderly people in Hong Kong: A retrospective cohort study. Lancet 2016, 388, S82. [Google Scholar] [CrossRef]
- Ouchi, Y.; Rakugi, H.; Arai, H.; Akishita, M.; Ito, H.; Toba, K.; Kai, I. Joint Committee of Japan Gerontological Society (JGLS) and Japan Geriatrics Society (JGS) on the definition and classification of the elderly. Redefining the elderly as aged 75 years and older: Proposal from the Joint Committee of Japan Gerontological Society and the Japan Geriatrics Society. Geriatr. Gerontol. Int. 2017, 17, 1045–1047. [Google Scholar] [CrossRef] [Green Version]
- Chen, T.; Kishimoto, H.; Honda, T.; Hata, J.; Yoshida, D.; Mukai, N.; Shibata, M.; Ninomiya, T.; Kumagai, S. Patterns and Levels of Sedentary Behavior and Physical Activity in a General Japanese Population: The Hisayama Study. J. Epidemiol. 2018, 28, 260–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, T.; Narazaki, K.; Honda, T.; Chen, S.; Haeuchi, Y.; Nofuji, Y.Y.; Matsuo, E.; Kumagai, S. Tri-Axial Accelerometer-Determined Daily Physical Activity and Sedentary Behavior of Suburban Community-Dwelling Older Japanese Adults. J. Sports Sci. Med. 2015, 14, 507–514. [Google Scholar] [PubMed]
- Takamiya, T.; Inoue, S. Trends in Step-determined Physical Activity among Japanese Adults from 1995 to 2016. Med. Sci. Sports Exerc. 2019, 51, 1852–1859. [Google Scholar] [CrossRef] [PubMed]
- Besser, L.M.; Dannenberg, A.L. Walking to Public TransitSteps to Help Meet Physical Activity Recommendations. Am. J. Prev. Med. 2005, 29, 273–280. [Google Scholar] [CrossRef] [Green Version]
- Rissel, C.; Curac, N.; Greenaway, M.; Bauman, A. Physical Activity Associated with Public Transport Use—A Review and Mod-elling of Potential Benefits. Int. J. Environ. Res. Public Health 2012, 9, 2454–2578. [Google Scholar] [CrossRef] [Green Version]
- Kamada, M.; Kitayuguchi, J.; Inoue, S.; Kamioka, H.; Mutoh, Y.; Shiwaku, K. Environmental correlates of physical activity in driv-ing and non-driving rural Japanese women. Prev. Med. 2009, 49, 490–496. [Google Scholar] [CrossRef]
- Amagasa, S.; Fukushima, N.; Kikuchi, H.; Takamiya, T.; Odagiri, Y.; Oka, K.; Inoue, S. Drivers Are More Physically Active Than Non-Drivers in Older Adults. Int. J. Environ. Res. Public Health 2018, 15, 1094. [Google Scholar] [CrossRef] [Green Version]
- McNeill, L.H.; Kreuter, M.W.; Subramanian, S. Social Environment and Physical activity: A review of concepts and evidence. Soc. Sci. Med. 2006, 63, 1011–1022. [Google Scholar] [CrossRef]
- Levasseur, M.; Généreux, M.; Bruneau, J.-F.; Vanasse, A.; Chabot, É.; Beaulac, C.; Bédard, M.-M. Importance of proximity to resources, social support, transportation and neighborhood security for mobility and social participation in older adults: Results from a scoping study. BMC Public Health 2015, 15, 1–19. [Google Scholar] [CrossRef] [Green Version]
- Tomioka, K.; Kurumatani, N.; Hosoi, H. Positive and negative influences of social participation on physical and mental health among community-dwelling elderly aged 65–70 years: A cross-sectional study in Japan. BMC Geriatr. 2017, 17, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Benefits and risks associated with physical activity. In ACSM’s Guidelines for Exercise Testing and Prescription, 10th ed.; 2017; Available online: https://www.acsm.org/docs/default-source/publications-files/acsm-guidelines-download-10th-edabf32a97415a400e9b3be594a6cd7fbf.pdf?sfvrsn=aaa6d2b2_0 (accessed on 12 October 2020).
- Kim, B.; Hyun, H.S. Associations between Social and Physical Environments, and Physical Activity in Adults from Urban and Rural Regions. Osong Public Health Res. Perspect. 2018, 9, 16–24. [Google Scholar] [CrossRef]
- Perrey, S.; Fabre, N. Exertion during Uphill, Level and Downhill Walking with and without Hiking Poles. J. Sports Sci. Med. 2008, 7, 32–38. [Google Scholar] [PubMed]
- Tsunoda, K.; Tsuji, T.; Kitano, N.; Mitsuishi, Y.; Yoon, J.Y.; Yoon, J.; Okura, T. Associations of physical activity with neighborhood envi-ronments and transportation modes in older Japanese adults. Prev. Med. 2012, 55, 113–118. [Google Scholar] [CrossRef] [Green Version]
- Zhang, F.; Li, D. Multiple Linear Regression-Structural Equation Modeling Based Development of the Integrated Model of Per-ceived Neighborhood Environment and Quality of Life of Community-Dwelling Older Adults: A Cross-Sectional Study in Nanjing, China. Int. J. Environ. Res. Public Health 2019, 16, 4933. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, Y.; Yuan, Y.; Chen, Y.; Lai, S. Association Pathways Between Neighborhood Greenspaces and the Physical and Mental Health of Older Adults—A Cross-Sectional Study in Guangzhou, China. Front. Public Health 2020, 8. [Google Scholar] [CrossRef] [PubMed]
- Kamada, M.; Kitayuguchi, J.; Abe, T.; Taguri, M.; Inoue, S.; Ishikawa, Y.; Harada, K.; Lee, I.M.; Bauman, A.; Miyachi, M. Community-wide promotion of physical activity in middle-aged and older Japanese: A 3-year evaluation of a cluster ran-domized trial. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Mooney, S.J.; Joshi, S.; Cerdá, M.; Kennedy, G.J.; Beard, J.R.; Rundle, A.G. Contextual Correlates of Physical Activity among Older Adults: A Neighborhood Environment-Wide Association Study (NE-WAS). Cancer Epidemiol. Biomark. Prev. 2017, 26, 495–504. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Covariates Adjusted | |
|---|---|
| Model 1 | Age + Sex |
| Model 2 | Age + Sex + Smoking + Drinking + BMI |
| Model 3 | Age + Sex + Smoking + Drinking + BMI + Musculoskeletal disorders + Residential density |
| Variables | Became Physically Inactive | |
|---|---|---|
| No (%) | Yes (%) | |
| N | 1217 | 994 |
| Sex | ||
| Male | 520 (42.7) | 424 (42.7) |
| Female | 697 (57.3) | 570 (57.3) |
| Age | ||
| 60–69 | 538 (44.2) | 521 (52.4) |
| 70–79 | 568 (46.7) | 434 (43.7) |
| 80+ | 111 (9.1) | 39 (3.9) |
| Municipality of residence | ||
| Unnan | 482 (39.6) | 481 (48.4) |
| Oki | 379 (31.1) | 189 (19.0) |
| Onan | 356 (29.3) | 324 (32.6) |
| Smoking | ||
| Yes | 86 (7.1) | 88 (8.9) |
| No | 1131 (92.9) | 906 (91.1) |
| Drinking | ||
| Yes | 320 (26.3) | 278 (28.0) |
| Occasionally | 238 (19.6) | 213 (21.4) |
| No | 659 (54.1) | 503 (50.6) |
| BMI (mean (SD)) | 22.4 (2.8) | 22.4 (3.0) |
| Musculoskeletal disorders | ||
| Yes | 213 (17.5) | 164 (16.5) |
| No | 1004 (82.5) | 830 (83.5) |
| Model 1 a | Model 2 b | Model 3 c | |
|---|---|---|---|
| HR (95%CI) | HR (95%CI) | HR (95%CI) | |
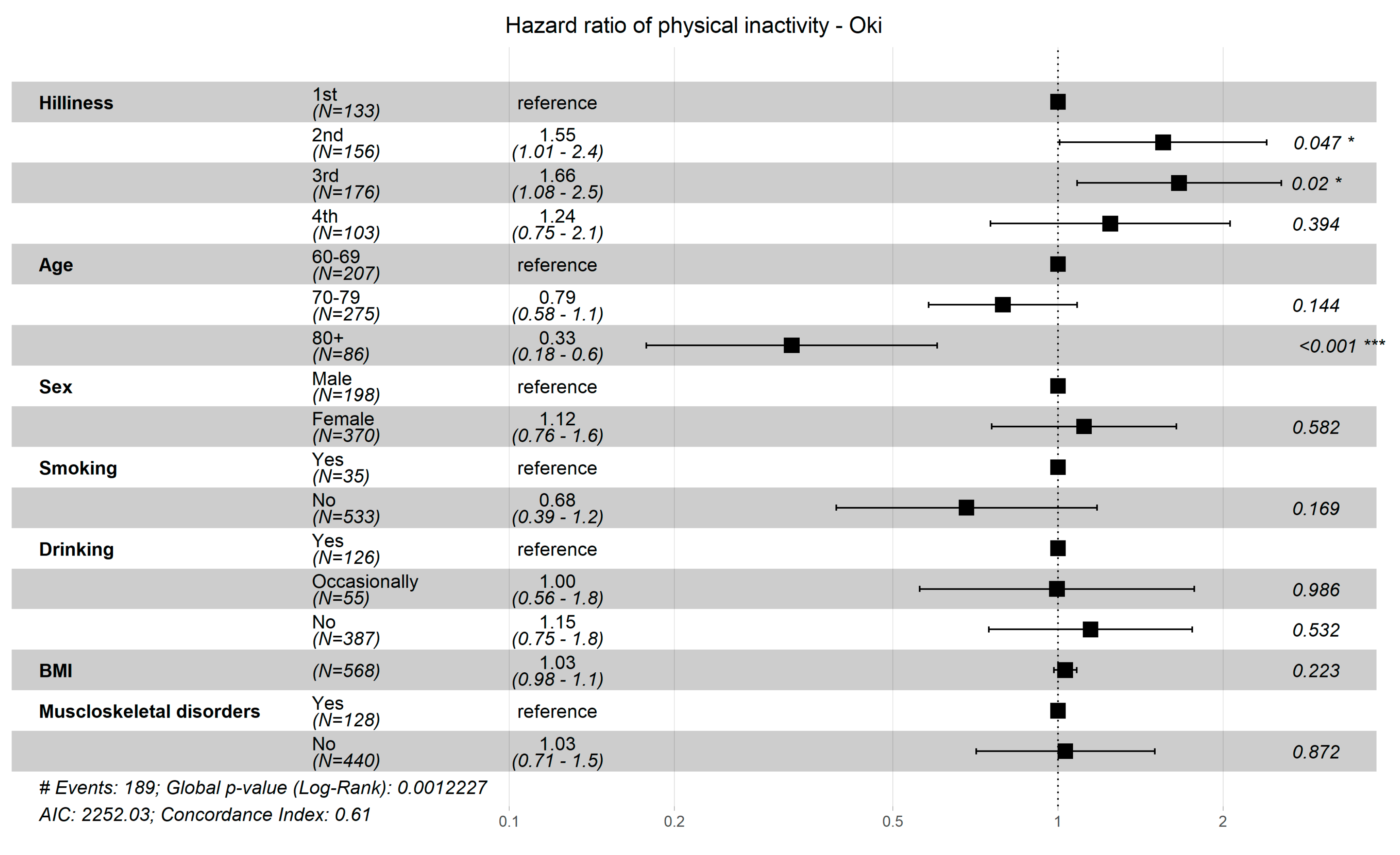
| Slope (ref. 1st, lowest) | |||
| 2nd | 1.12 (0.95, 1.30) | 1.12 (0.94, 1.29) | 1.14 (0.97, 1.32) |
| 3rd | 1.10 (0.93, 1.28) | 1.10 (0.92, 1.28) | 1.13 (0.95, 1.30) |
| 4th (highest) | 1.00 (0.82, 1.17) | 0.99 (0.81, 1.17) | 0.98 (0.80, 1.16) |
| Bus stop density (ref. 1st, lowest) | |||
| 2nd | 1.15 (0.99, 1.32) | 1.16 (1.00, 1.33) | 1.09 (0.92, 1.26) |
| 3rd | 1.18 (1.01, 1.36) | 1.18 (1.01, 1.36) | 1.14 (0.96, 1.31) |
| 4th (highest) | 1.11 (0.93, 1.29) | 1.12 (0.95, 1.30) | 1.04 (0.86, 1.22) |
| Intersection density (ref. 1st, lowest) | |||
| 2nd | 0.94 (0.76, 1.12) | 0.93 (0.75, 1.11) | 0.94 (0.76, 1.13) |
| 3rd | 1.06 (0.89, 1.23) | 1.06 (0.89, 1.23) | 1.03 (0.86, 1.20) |
| 4th (highest) | 1.08 (0.91, 1.26) | 1.09 (0.92, 1.26) | 1.07 (0.90, 1.25) |
| Residential density (ref. 1st, lowest) | |||
| 2nd | 1.06 (0.90, 1.23) | 1.06 (0.90, 1.23) | 1.07 (0.90, 1.24) |
| 3rd | 1.07 (0.90, 1.24) | 1.06 (0.89, 1.23) | 1.07 (0.90, 1.24) |
| 4th (highest) | 0.96 (0.78, 1.13) | 0.96 (0.78, 1.13) | 0.95 (0.78, 1.13) |
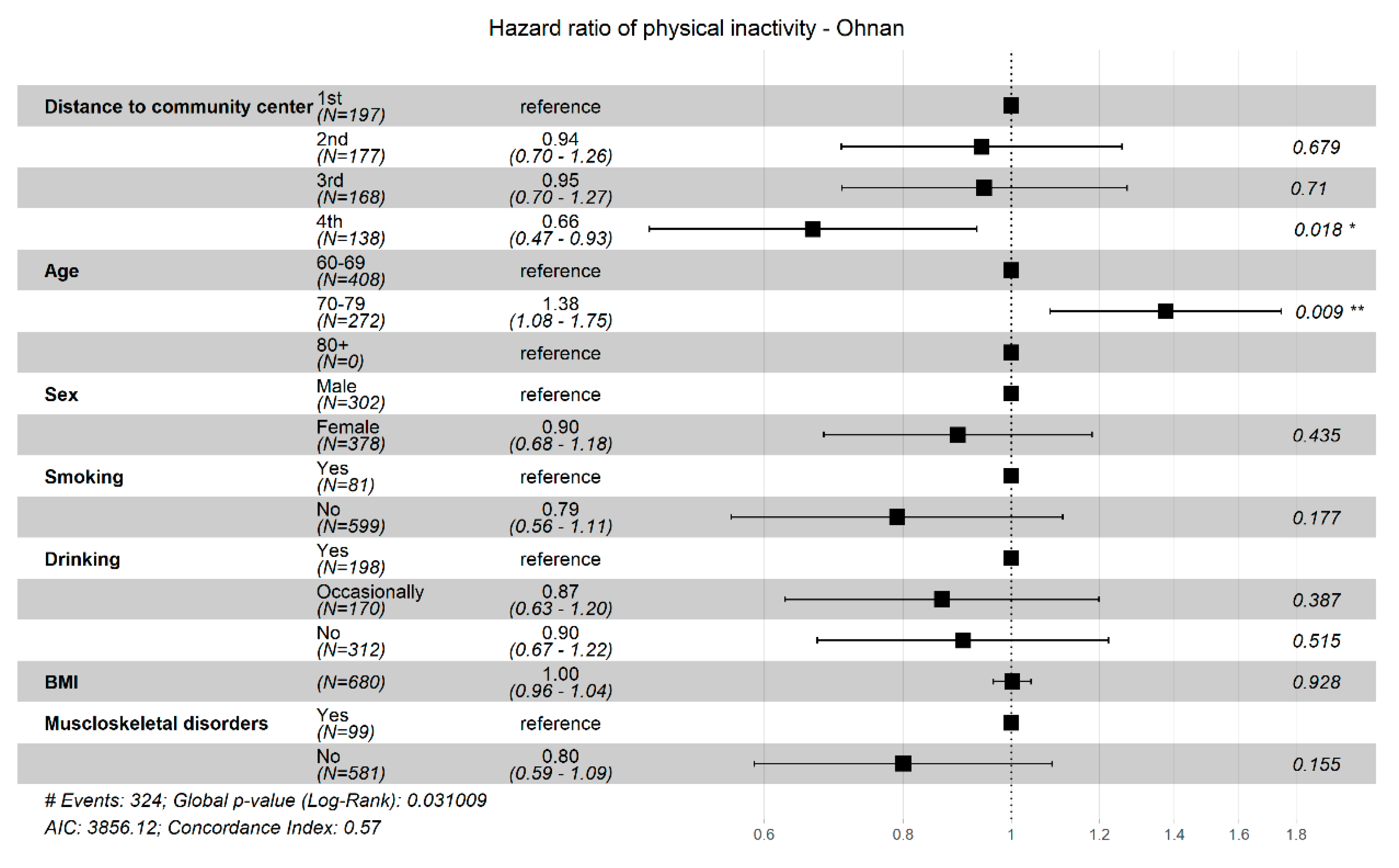
| Distance to community center (ref. 1st, lowest) | |||
| 2nd | 0.94 (0.77, 1.11) | 0.93 (0.76, 1.10) | 0.96 (0.79, 1.13) |
| 3rd | 0.90 (0.73, 1.08) | 0.90 (0.73, 1.07) | 0.90 (0.73, 1.08) |
| 4th (highest) | 0.75 (0.57, 0.93) | 0.75 (0.57, 0.93) | 0.82 (0.64, 1.01) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Okuyama, K.; Abe, T.; Li, X.; Toyama, Y.; Sundquist, K.; Nabika, T. Neighborhood Environmental Factors and Physical Activity Status among Rural Older Adults in Japan. Int. J. Environ. Res. Public Health 2021, 18, 1450. https://doi.org/10.3390/ijerph18041450
Okuyama K, Abe T, Li X, Toyama Y, Sundquist K, Nabika T. Neighborhood Environmental Factors and Physical Activity Status among Rural Older Adults in Japan. International Journal of Environmental Research and Public Health. 2021; 18(4):1450. https://doi.org/10.3390/ijerph18041450
Chicago/Turabian StyleOkuyama, Kenta, Takafumi Abe, Xinjun Li, Yuta Toyama, Kristina Sundquist, and Toru Nabika. 2021. "Neighborhood Environmental Factors and Physical Activity Status among Rural Older Adults in Japan" International Journal of Environmental Research and Public Health 18, no. 4: 1450. https://doi.org/10.3390/ijerph18041450
APA StyleOkuyama, K., Abe, T., Li, X., Toyama, Y., Sundquist, K., & Nabika, T. (2021). Neighborhood Environmental Factors and Physical Activity Status among Rural Older Adults in Japan. International Journal of Environmental Research and Public Health, 18(4), 1450. https://doi.org/10.3390/ijerph18041450