
Prevalence of Undernutrition and Effect of Body Weight Loss on Survival among Pediatric Cancer Patients in Northeastern Hungary



Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Assessment of Nutritional Status
2.3. Statistical Analysis
3. Results
3.1. Patient Characterization and Follow-Up
3.2. Nutritional Status of Patients at Baseline and during Follow-Up
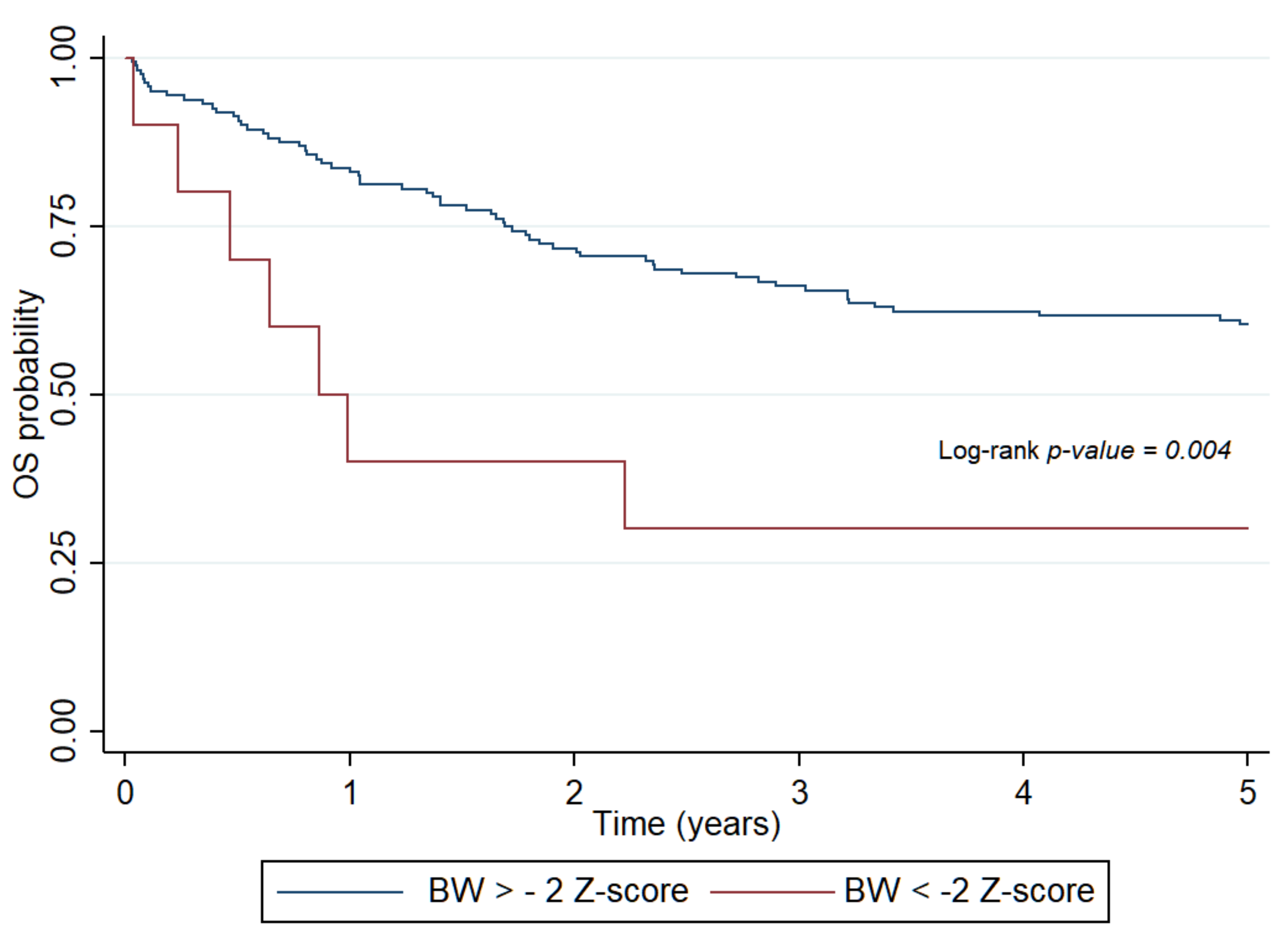
3.3. Survival and Nutritional Status
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Marotta, C.; Di Gennaro, F.; Pizzol, D.; Madeira, G.; Monno, L.; Saracino, A.; Putoto, G.; Casuccio, A.; Mazzucco, W. At Risk Child Clinic (ARCC): 3 Years of Health Activities in Support of the Most Vulnerable Children in Beira, Mozambique. Int. J. Environ. Res. Public Health 2018, 15, 1350. [Google Scholar] [CrossRef] [Green Version]
- Inaba, H.; Surprise, H.C.; Pounds, S.; Cao, X.; Howard, S.C.; Ringwald-Smith, K.; Buaboonnam, J.; Dahl, G.; Bowman, W.P.; Taub, J.W.; et al. Effect of body mass index on the outcome of children with acute myeloid leukemia. Cancer 2012, 118, 5989–5996. [Google Scholar] [CrossRef] [Green Version]
- Lange, B.J.; Gerbing, R.B.; Feusner, J.H.; Skolnik, J.; Sacks, N.; Smith, F.O.; Alonzo, T.A. Mortality in overweight and underweight children with acute myeloid leukemia. JAMA 2005, 293, 203–211. [Google Scholar] [CrossRef]
- Butturini, A.M.; Dorey, F.J.; Lange, B.J.; Henry, D.W.; Gaynon, P.S.; Fu, C.; Franklin, J.; Siegel, S.E.; Seibel, N.L.; Rogers, P.C.; et al. Obesity and outcome in pediatric acute lymphoblastic leukemia. J. Clin. Oncol. 2007, 25, 2063–2069. [Google Scholar] [CrossRef]
- Yazbeck, N.; Samia, L.; Saab, R.; Abboud, M.R.; Solh, H.; Muwakkit, S. Effect of Malnutrition at Diagnosis on Clinical Outcomes of Children With Acute Lymphoblastic Leukemia. J. Pediatr. Hematol. Oncol. 2016, 38, 107–110. [Google Scholar] [CrossRef]
- Rogers, P.C. Importance of nutrition in pediatric oncology. Indian J. Cancer 2015, 52, 176–178. [Google Scholar] [CrossRef]
- Joffe, L.; Ladas, E.J. Nutrition during childhood cancer treatment: Current understanding and a path for future research. Lancet Child Adolesc. Health 2020. [Google Scholar] [CrossRef]
- Radhakrishnan, V.; Ganesan, P.; Rajendranath, R.; Ganesan, T.S.; Sagar, T.G. Nutritional profile of pediatric cancer patients at Cancer Institute, Chennai. Indian J. Cancer 2015, 52, 207–209. [Google Scholar] [CrossRef]
- Iniesta, R.R.; Paciarotti, I.; Brougham, M.F.; McKenzie, J.M.; Wilson, D.C. Effects of pediatric cancer and its treatment on nutritional status: A systematic review. Nutr. Rev. 2015, 73, 276–295. [Google Scholar] [CrossRef]
- Martin-Trejo, J.A.; Nunez-Enriquez, J.C.; Fajardo-Gutierrez, A.; Medina-Sanson, A.; Flores-Lujano, J.; Jimenez-Hernandez, E.; Amador-Sanchez, R.; Peñaloza-Gonzalez, J.G.; Alvarez-Rodriguez, F.J.; Bolea-Murga, V.; et al. Early mortality in children with acute lymphoblastic leukemia in a developing country: The role of malnutrition at diagnosis. A multicenter cohort MIGICCL study. Leuk Lymphoma 2017, 58, 898–908. [Google Scholar] [CrossRef]
- Shah, P.; Jhaveri, U.; Idhate, T.B.; Dhingra, S.; Arolkar, P.; Arora, B. Nutritional status at presentation, comparison of assessment tools, and importance of arm anthropometry in children with cancer in India. Indian J. Cancer 2015, 52, 210–215. [Google Scholar]
- Mahony, B.O.; Savini, L.; Hara, J.O.; Bok, A. Haemophilia care in Europe—A survey of 37 countries. Haemophilia 2017, 23, e259–e266. [Google Scholar] [CrossRef] [PubMed]
- Kadar, M.; Szőllősi, G.J.; Molnar, S.Z.; Szabo, L. The incidence of malnutrition between 1 and 5 years of age on the basis of the preventive primary care data. Dev. Heath Sci. 2019, 2, 9–14. [Google Scholar]
- Available online: https://curesearch.org/5-year-survival-rate (accessed on 15 November 2020).
- Available online: https://www.iarc.fr (accessed on 15 November 2020).
- Available online: https://www.acco.org/global-childhood-cancer-statistics/ (accessed on 15 November 2020).
- Rogers, P.C.; Melnick, S.J.; Ladas, E.J.; Halton, J.; Baillargeon, J.; Sacks, N. Children’s Oncology Group (COG) Nutrition Committee. Pediatr. Blood Cancer 2008, 50 (Suppl. S2), 447–450. [Google Scholar] [CrossRef]
- Brinksma, A.; Sanderman, R.; Roodbol, P.F.; Sulkers, E.; Burgerhof, J.G.; de Bont, E.S.; Tissing, W.J.E. Malnutrition is associated with worse health-related quality of life in children with cancer. Support. Care Cancer 2015, 23, 3043–3052. [Google Scholar] [CrossRef] [Green Version]
- Brinksma, A.; Roodbol, P.F.; Sulkers, E.; Kamps, W.A.; de Bont, E.S.; Boot, A.M.; Burgerhof, J.G.M.; Tamminga, R.Y.J.; Tissing, W.J.E. Changes in nutritional status in childhood cancer patients: A prospective cohort study. Clin. Nutr. 2015, 34, 66–73. [Google Scholar] [CrossRef]
- Joubert, K. (Ed.) Results of the National Longitudinal Child-Growth Study from Birth to 18 Years; Demographic Research Institute: Hungary, Budapest, 2006. [Google Scholar]
- Available online: https://www.who.int/nutgrowthdb/about/introduction/en/index4.html (accessed on 15 November 2020).
- Murphy, A.J.; White, M.; Davies, P.S. The validity of simple methods to detect poor nutritional status in paediatric oncology patients. Br. J. Nutr. 2009, 101, 1388–1392. [Google Scholar] [CrossRef] [Green Version]
- Kiss, C.; Kiss, M.; Szegedi, I.; Arvai, K.; Toth, J.; Olah, E. Interferon-alpha therapy in children with malignant diseases: Clinical experience in twenty-four patients treated in a single pediatric oncology unit. Med. Pediatr. Oncol. 2002, 39, 115–119. [Google Scholar] [CrossRef] [PubMed]
- Jakab, Z.; Balogh, E.; Kiss, C.; Olah, E. Epidemiologic studies in a population-based childhood cancer registry in Northeast Hungary. Med. Pediatr. Oncol. 2002, 38, 338–344. [Google Scholar] [CrossRef]
- Zimmermann, K.; Ammann, R.A.; Kuehni, C.E.; De Geest, S.; Cignacco, E. Malnutrition in pediatric patients with cancer at diagnosis and throughout therapy: A multicenter cohort study. Pediatr. Blood Cancer 2013, 60, 642–649. [Google Scholar] [CrossRef]
- Martin, E.; Belleton, F.; Lallemand, Y.; Goy, F.; Perol, D.; Bachmann, P.; Marec-Bérard, P. Malnutrition in pediatric oncology: Prevalence and screening. Arch. Pediatr. 2006, 13, 352–357. [Google Scholar] [CrossRef]
- Ottery, F.D. Definition of standardized nutritional assessment and interventional pathways in oncology. Nutrition 1996, 12 (Suppl. S1), S15–S19. [Google Scholar] [CrossRef]
- Blum, D.; Strasser, F. Cachexia assessment tools. Curr. Opin. Support. Palliat. Care 2011, 5, 350–355. [Google Scholar] [CrossRef] [Green Version]
- Boleo-Tome, C.; Monteiro-Grillo, I.; Camilo, M.; Ravasco, P. Validation of the Malnutrition Universal Screening Tool (MUST) in cancer. Br. J. Nutr. 2012, 108, 343–348. [Google Scholar] [CrossRef]
- Brinksma, A.; Roodbol, P.F.; Sulkers, E.; Hooimeijer, H.L.; Sauer, P.J.; van Sonderen, E.; De Bont, E.S.; Tissing, W.J.E. Weight and height in children newly diagnosed with cancer. Pediatr. Blood Cancer 2015, 62, 269–273. [Google Scholar] [CrossRef]
- Rivera-Luna, R.; Olaya-Vargas, A.; Velasquez-Avina, M.; Frenk, S.; Cardenas-Cardos, R.; Leal-Leal, C.; Perez-Gonzalez, O.; Martínez-Avalos, A. Early death in children with acute lymphoblastic leukemia: Does malnutrition play a role? Pediatr. Hematol. Oncol. 2008, 25, 17–26. [Google Scholar] [CrossRef]
- Pribnow, A.K.; Ortiz, R.; Baez, L.F.; Mendieta, L.; Luna-Fineman, S. Effects of malnutrition on treatment-related morbidity and survival of children with cancer in Nicaragua. Pediatr. Blood Cancer 2017, 64, e26590. [Google Scholar] [CrossRef] [Green Version]
- Eissa, H.M.; Zhou, Y.; Panetta, J.C.; Browne, E.K.; Jeha, S.; Cheng, C.; Relling, M.V.; Campana, D.; Pui, C.-H.; Inaba, H. The effect of body mass index at diagnosis on clinical outcome in children with newly diagnosed acute lymphoblastic leukemia. Blood Cancer J. 2017, 7, e531. [Google Scholar] [CrossRef]
- Brinksma, A.; Huizinga, G.; Sulkers, E.; Kamps, W.; Roodbol, P.; Tissing, W. Malnutrition in childhood cancer patients: A review on its prevalence and possible causes. Crit. Rev. Oncol. Hematol. 2012, 83, 249–275. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Tumor Subtypes | Number | Mean Age | Gender | Outcome | |||
|---|---|---|---|---|---|---|---|
| Male/Female | Alive/Relapsed | Death | |||||
| (Years ±SD) | (Min–Max) | N | % | N | N | ||
| Total | 174 | 7.34 ± 5.10 | (1.01–16.79) | 100/74 | 57.47/42.53 | 106 | 69 |
| Onco-hematologic malignancy | 100 | 8.04 ± 4.84 | (1.16–16.79) | 57/43 | 57.00/43 | 73 | 26 |
| Solid tumor | 74 | 6.40 ± 5.32 | (1.01–17.07) | 43/31 | 58.11/41.89 | 33 | 43 |
| Follow-Up Points | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Patient Group | At Diagnosis | Nadir during Therapy | End of Therapy | ||||||
| Mean | SD | Min–Max | Mean | SD | Min–Max | Mean | SD | Min–Max | |
| BW | |||||||||
| total | −0.18 | 1.29 | −2.76–5.31 | −0.87 | 1.26 | −3.92–4.81 | −0.18 | 1.33 | −3.51–6.01 |
| H | −0.068 | 1.2 | −0.31–0.18 | −0.71 | 1.27 | −0.96–−0.46 | 0.16 | 1.29 | −0.11–0.44 |
| S | −0.33 | 1.32 | −2.75–5.31 | −1.1 | 1.21 | −3.25–4.81 | −0.70 | 1.22 | −3.51–4.46 |
| WFH | |||||||||
| total | −0.29 | 1.19 | −3.0–3.48 | −1.09 | 1.15 | −4.44–2.99 | 0.25 | 1.35 | −3.24–5.77 |
| H | −0.20 | 1.1 | −0.42–0.12 | −0.99 | 1.11 | −1.21–−0.77 | 0.4 | 1.34 | 0.11–0.69 |
| S | −0.41 | 1.3 | −3.0–3.46 | −1.23 | −3.63 | −3.63–4.81 | −0.53 | 1.18 | −3.24–3.28 |
| BMI | |||||||||
| total | −0.17 | 1.21 | −2.66–4.84 | −0.97 | 1.18 | −2.66–4.84 | 0.085 | 1.3 | −2.94–5.08 |
| H | −0.07 | 1.15 | −0.3–0.15 | −0.86 | 1.13 | −1.09–−0.63 | 0.41 | 1.26 | 0.14–0.68 |
| S | −0.3 | 1.28 | −2.66–4.84 | −1.11 | 1.24 | −3.33–4.27 | −0.4 | 1.21 | −2.94–4.2 |
| IBW% | |||||||||
| total | 99.15 | 15.6 | 62.96–161.53 | 88.87 | 14.1 | 56.6–153.84 | 103.12 | 17.5 | 69.41–166.46 |
| H | 100.46 | 14.79 | 97.52–103.39 | 90.19 | 12.96 | 87.6–92.78 | 108 | 17.42 | 104.26–111.73 |
| S | 97.39 | 16.69 | 62.96–161.53 | 87.16 | 15.46 | 83.5–90.82 | 95.88 | 15.05 | 91.92–99.84 |
| Anthropometric Parameter | Tumor Subtypes | During Therapy to Diagnosis | During Therapy to End of Treatment | Diagnosis to End of Treatment |
|---|---|---|---|---|
| p | p | p | ||
| BW | Total | <0.001 | <0.001 | 0.970 |
| H | <0.001 | <0.001 | 0.215 | |
| S | <0.001 | 0.006 | 0.200 | |
| WFH | Total | <0.001 | <0.001 | <0.001 |
| H | <0.001 | <0.001 | <0.001 | |
| S | <0.001 | <0.001 | 0.590 | |
| BMI | Total | <0.001 | <0.001 | 0.070 |
| H | <0.001 | 0.007 | 0.007 | |
| S | <0.001 | 0.001 | 0.650 | |
| IBW% | Total | <0.001 | <0.001 | 0.033 |
| H | <0.001 | <0.001 | 0.002 | |
| S | <0.001 | 0.002 | 0.590 |
| Timepoint | BW | BW | BW | WFH | WFH | WFH | BMI | BMI | BMI | IBW% | IBW% | IBW% | WL% | WL% | WL% |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total | H | S | Total | H | S | Total | H | S | Total | H | S | Total | H | S | |
| (%) | (%) | (%) | (%) | (%) | |||||||||||
| At diagnosis | 5.75 | 5 | 6.76 | 4.62 | 4.04 | 5.41 | 4.02 | 3 | 5.11 | 30.45 | 26 | 32.4 | NA | NA | NA |
| During treatment | 14.11 | 12.12 | 16.9 | 20.58 | 15.15 | 28.1 | 17.6 | 11.11 | 26.7 | 57 | 55.55 | 59.1 | 44.94 | 43.43 | 43.5 |
| End of treatment | 4.1 | 0 | 10.34 | 3.4 | 0 | 8.6 | 1.38 | 0 | 3.44 | 18.75 | 6.98 | 36.2 | NA | NA | NA |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kadenczki, O.; Nagy, A.C.; Kiss, C. Prevalence of Undernutrition and Effect of Body Weight Loss on Survival among Pediatric Cancer Patients in Northeastern Hungary. Int. J. Environ. Res. Public Health 2021, 18, 1478. https://doi.org/10.3390/ijerph18041478
Kadenczki O, Nagy AC, Kiss C. Prevalence of Undernutrition and Effect of Body Weight Loss on Survival among Pediatric Cancer Patients in Northeastern Hungary. International Journal of Environmental Research and Public Health. 2021; 18(4):1478. https://doi.org/10.3390/ijerph18041478
Chicago/Turabian StyleKadenczki, Orsolya, Attila Csaba Nagy, and Csongor Kiss. 2021. "Prevalence of Undernutrition and Effect of Body Weight Loss on Survival among Pediatric Cancer Patients in Northeastern Hungary" International Journal of Environmental Research and Public Health 18, no. 4: 1478. https://doi.org/10.3390/ijerph18041478
APA StyleKadenczki, O., Nagy, A. C., & Kiss, C. (2021). Prevalence of Undernutrition and Effect of Body Weight Loss on Survival among Pediatric Cancer Patients in Northeastern Hungary. International Journal of Environmental Research and Public Health, 18(4), 1478. https://doi.org/10.3390/ijerph18041478