
Markers of Cardiovascular Disease among Adults Exposed to Smoke from the Hazelwood Coal Mine Fire

 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
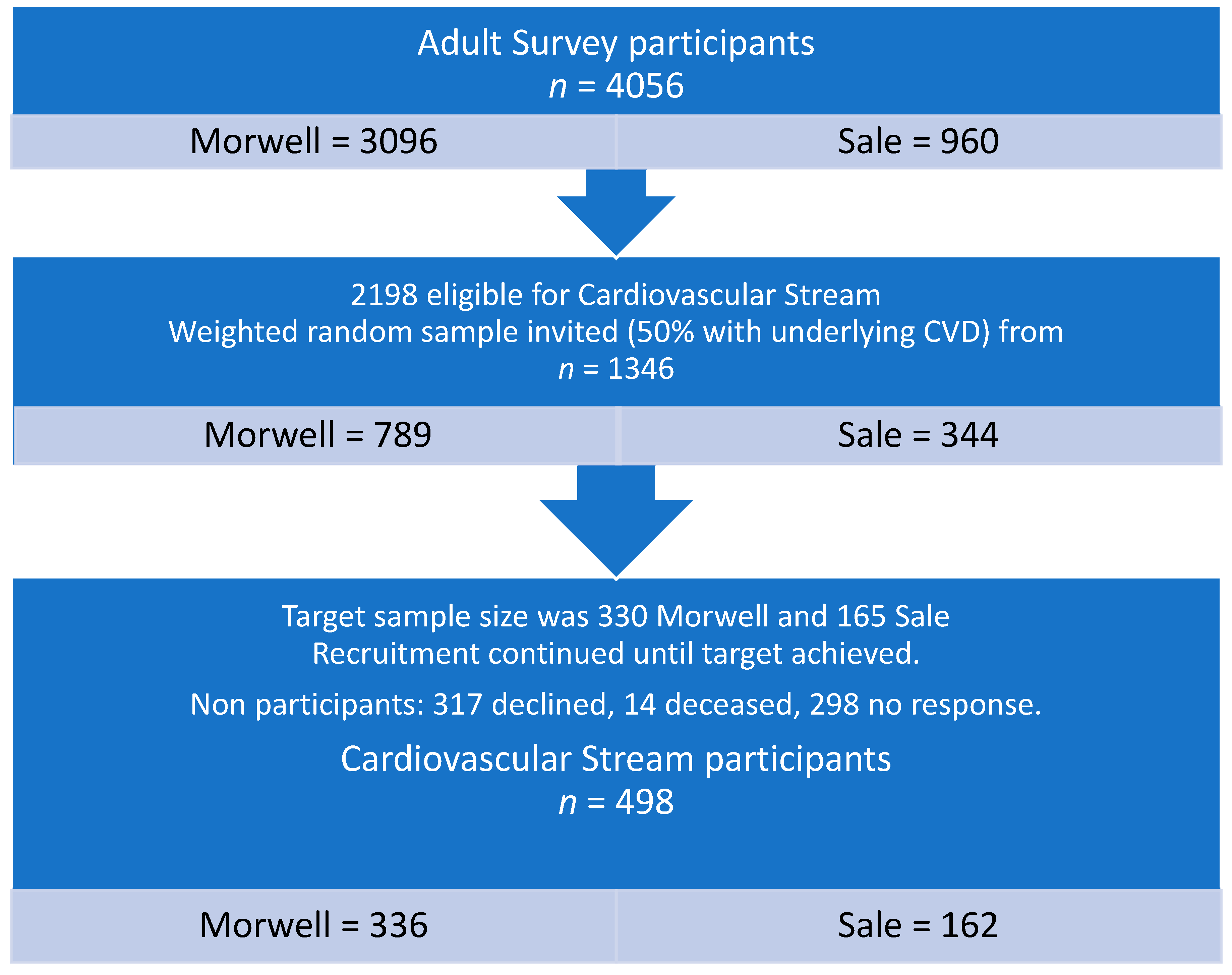
2.1. Study Design, Setting and Participants
2.2. Outcome and Confounding Variables
2.3. Statistical Analyses
2.4. Ethical Considerations
3. Results
3.1. Participants
3.2. Outcomes
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Newby, D.E.; Mannucci, P.M.; Tell, G.S.; Baccarelli, A.A.; Brook, R.D.; Donaldson, K.; Forastiere, F.; Franchini, M.; Franco, O.H.; Graham, I.; et al. Expert position paper on air pollution and cardiovascular disease. Eur. Hear. J. 2015, 36, 83–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franklin, B.A.; Brook, R.; Pope, C.A. Air pollution and cardiovascular disease. Curr. Probl. Cardiol. 2015, 40, 207–238. [Google Scholar] [CrossRef]
- Atkinson, R.W.; Kang, S.; Anderson, R.; Mills, I.; Walton, H. Epidemiological time series studies of PM2.5 and daily mortality and hospital admissions: A systematic review and meta-analysis. Thorax 2014, 69, 660–665. [Google Scholar] [CrossRef] [Green Version]
- Haikerwal, A.; Akram, M.; Del Monaco, A.; Smith, K.; Sim, M.R.; Meyer, M.; Tonkin, A.M.; Abramson, M.J.; Dennekamp, M. Impact of fine particulate matter (PM2.5) Exposure during wildfires on cardiovascular health outcomes. J. Am. Hear. Assoc. 2015, 4, e001653. [Google Scholar] [CrossRef] [Green Version]
- Cohen, A.J.; Brauer, M.; Burnett, R.; Anderson, H.R.; Frostad, J.; Estep, K.; Balakrishnan, K.; Brunekreef, B.; Dandona, L.; Dandona, R.; et al. Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: An analysis of data from the Global Burden of Diseases Study 2015. Lancet 2017, 389, 1907–1918. [Google Scholar] [CrossRef] [Green Version]
- Barrett, J.R. Subtle but potentially serious: Long-term ambient PM2.5 exposure and risk of cardiopulmonary mortality. Environ. Health Perspect. 2020, 128, 24001. [Google Scholar] [CrossRef]
- Chang, L.T.-C.; Scorgie, Y.; Duc, H.N.; Monk, K.; Fuchs, D.; Trieu, T. Major source contributions to ambient PM2.5 and exposures within the New South Wales greater metropolitan region. Atmosphere 2019, 10, 138. [Google Scholar] [CrossRef] [Green Version]
- Amsalu, E.; Wang, T.; Li, H.; Liu, Y.; Wang, A.; Liu, X.; Tao, L.; Luo, Y.; Zhang, F.; Yang, X.; et al. Acute effects of fine particulate matter (PM2.5) on hospital admissions for cardiovascular disease in Beijing, China: A time-series study. Environ. Health 2019, 18, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Johnston, F.H.; Purdie, S.; Jalaludin, B.; Martin, K.L.; Henderson, S.B.; Morgan, G.G. Air pollution events from forest fires and emergency department attendances in Sydney, Australia 1996–2007: A case-crossover analysis. Environ. Health 2014, 13, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Emmerson, K.; Reisen, F.; Luhar, A.; Williamson, G.; Cope, M. Air Quality Modelling of Smoke Exposure from the Hazelwood Mine Fire Australia: CSIRO. In Hezelwood Health Study Annual Report 2 15th November 2016; Available online: https://hazelwoodhealthstudy.org.au/study-findings/study-reports (accessed on 25 November 2020).
- Luhar, A.K.; Emmerson, K.M.; Reisen, F.; Williamson, G.J.; Cope, M.E. Modelling smoke distribution in the vicinity of a large and prolonged fire from an open-cut coal mine. Atmos. Environ. 2020, 229, 117471. [Google Scholar] [CrossRef]
- Melody, S.M.; Johnston, F. Coal mine fires and human health: What do we know? Int. J. Coal Geol. 2015, 152, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Hazelwood Health Study Website. Available online: https://hazelwoodhealthstudy.org.au (accessed on 25 November 2020).
- National Environment Protection (Ambient Air Quality) Measure. Available online: https://www.legislation.gov.au/Details/F2016C00215 (accessed on 11 January 2021).
- Guo, Y.; Dimitriadis, C.; Gao, C.X.; Wolfe, R.; Ikin, J.; Gabbe, B.; Abramson, M.J.; Sim, M.R. Hazelinks Mortality Report Time Series Analyses for the Period July 2009 to June 2015. Version 1.2. 2020. Available online: https://hazelwoodhealthstudy.org.au/study-findings/study-reports (accessed on 10 November 2020).
- Zhao, B.; Johnston, F.H.; O’Sullivan, T.; Williamson, G.J.; Melody, S.; Dalton, M.; Venn, A.; Negishi, K. Early life exposure to coal mine fire and tobacco smoke affect subclinical vascular function. Arch. Dis. Child. 2019, 105, 539–544. [Google Scholar] [CrossRef]
- Broder, J.; Gao, C.X.; Abramson, M.J.; Wolf, R.; Dimitriasdis, C.; Ilkin, J.; Sim, M.R.; Del Monaco, A.; Johnston, F.; Carroll, M.; et al. Long-term impact of exposure to coalmine fire emitted PM2.5 on emergency ambulance attendances: Hazelwood Health Study. manuscript in preparation.
- Elvidge, T.; Matthews, I.P.; Gregory, C.; Hoogendoorn, B. Feasibility of using biomarkers in blood serum as markers of effect following exposure of the lungs to particulate matter air pollution. J. Environ. Sci. Health Part C 2013, 31, 1–44. [Google Scholar] [CrossRef]
- Singh, T.; Morris, D.; Smith, S.; Moxon, J.; Golledge, J. Systematic review and meta-analysis of the association between C-reactive protein and major cardiovascular events in patients with peripheral artery disease. Eur. J. Vasc. Endovasc. Surg. 2017, 54, 220–233. [Google Scholar] [CrossRef]
- Gallacher, J.E. C-reactive protein concentration and risk of coronary heart disease, stroke, and mortality: An individual participant meta-analysis. Lancet 2010, 375, 132–140. [Google Scholar] [CrossRef] [Green Version]
- Ridker, P.M. A test in context. J. Am. Coll. Cardiol. 2016, 67, 712–723. [Google Scholar] [CrossRef] [PubMed]
- Ikin, J.F.; Carroll, M.T.C.; Guo, Y.; Johnston, F.; Liew, D.; Maybery, D.; Thompson, B.; Sim, M.; Abramson, M.J.; Walker, J.; et al. Cohort profile: The Hazelwood Health Study adult cohort. Int. J. Epidemiol. 2020. [Google Scholar] [CrossRef]
- Pope, A.C.; Muhlestein, J.B.; May, H.T.; Renlund, D.G.; Anderson, J.L.; Horne, B.D. Ischemic heart disease events triggered by short-term exposure to fine particulate air pollution. Circulation 2006, 114, 2443–2448. [Google Scholar] [CrossRef] [Green Version]
- Abbott Laboratories Inc. ARCHITECT ci 16200 Analyser Manual. Available online: https://www.ilexmedical.com/files/PDF/CRPVARIO_ARC_CHEM.pdf (accessed on 11 January 2021).
- National Health and Medical Research Council. Clinical Practice Guidelines for the Management of Overweight and Obesity in Adults, Adolescents and Children in Australia; National Health and Medical Research Council: Melbourne, Australia, 2013.
- Liang, Y.-L.; Teede, H.; Kotsopoulos, D.; Shiel, L.; Cameron, J.D.; Dart, A.M.; McGrath, B.P. Non-invasive measurements of arterial structure and function: Repeatability, interrelationships and trial sample size. Clin. Sci. 1998, 95, 669–679. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Meneses-Gaya, C.; Zuardi, A.W.; Loureiro, S.R.; Crippa, J.A.S. Alcohol use disorders identification test (AUDIT): An updated systematic review of psychometric properties. Psychol. Neurosci. 2009, 2, 83. [Google Scholar] [CrossRef] [Green Version]
- Frank, D.; DeBenedetti, A.F.; Volk, R.J.; Williams, E.C.; Kivlahan, D.R.; Bradley, K.A. Effectiveness of the AUDIT-C as a screening test for alcohol misuse in three race/Ethnic groups. J. Gen. Intern. Med. 2008, 23, 781–787. [Google Scholar] [CrossRef] [Green Version]
- ATC/DDD Index. Available online: https://www.whocc.no/atc_ddd_index (accessed on 3 October 2017).
- Australian Bureau of Statistics. 2011.0.55.001 Information Paper: Census of Population and Housing-Products and Services, 2011–2012. Available online: http://www.abs.gov.au/ausstats/[email protected]/lookup/2011.0.55.001Main%20Features22011 (accessed on 20 October 2020).
- Fiordelisi, A.; Piscitelli, P.; Trimarco, B.; Coscioni, E.; Iaccarino, G.; Sorriento, D. The mechanisms of air pollution and particulate matter in cardiovascular diseases. Hear. Fail. Rev. 2017, 22, 337–347. [Google Scholar] [CrossRef]
- Yang, B.-Y.; Qian, Z.; Howard, S.W.; Vaughn, M.G.; Fan, S.-J.; Liu, K.-K.; Dong, G.-H. Global association between ambient air pollution and blood pressure: A systematic review and meta-analysis. Environ. Pollut. 2018, 235, 576–588. [Google Scholar] [CrossRef]
- Brook, R.D.; Shin, H.H.; Bard, R.L.; Burnett, R.T.; Vette, A.; Croghan, C.; Thornburg, J.; Rodes, C.; Williams, R. Exploration of the rapid effects of personal fine particulate matter exposure on arterial hemodynamics and vascular function during the same day. Environ. Health Perspect. 2011, 119, 688–694. [Google Scholar] [CrossRef] [Green Version]
- Song, X.; Liu, Y.; Hu, Y.; Zhao, X.-Y.; Tian, J.; Ding, G.; Wang, S. Short-term exposure to air pollution and cardiac arrhythmia: A meta-analysis and systematic review. Int. J. Environ. Res. Public Health 2016, 13, 642. [Google Scholar] [CrossRef] [Green Version]
- Huttunen, K.; Siponen, T.; Salonen, I.; Yli-Tuomi, T.; Aurela, M.; Dufva, H.; Hillamo, R.; Linkola, E.; Pekkanen, J.; Pennanen, A.; et al. Low-level exposure to ambient particulate matter is associated with systemic inflammation in ischemic heart disease patients. Environ. Res. 2012, 116, 44–51. [Google Scholar] [CrossRef] [PubMed]
- Tinling, M.A.; West, J.J.; Cascio, W.E.; Kilaru, V.; Rappold, A.G. Repeating cardiopulmonary health effects in rural North Carolina population during a second large peat wildfire. Environ. Health 2016, 15, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Dennekamp, M.; Straney, L.D.; Tonkin, A.M.; Erbas, B.; Abramson, M.J.; Keywood, M.; Smith, K.; Sim, M.R.; Glass, D.C.; Del Monaco, A.; et al. Forest fire smoke exposures and out-of-hospital cardiac arrests in melbourne, australia: A case-crossover study. Environ. Health Perspect. 2015, 123, 959–964. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dubowsky, S.D.; Suh, H.H.; Schwartz, J.; Coull, B.A.; Gold, D.R. Diabetes, obesity, and hypertension may enhance associations between air pollution and markers of systemic inflammation. Environ. Health Perspect. 2006, 114, 992–998. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Y.; Rittenhouse-Olson, K.; Scheider, W.L.; Mu, L. Effect of particulate matter air pollution on C-reactive protein: A review of epidemiologic studies. Rev. Environ. Health 2012, 27, 133–149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ridker, P.M.; Danielson, E.; Nordestgaard, B.G.; Shepherd, J.; Willerson, J.T.; Glynn, R.J.; Fonseca, F.A.H.; Genest, J.; Gotto, A.M.; Kastelein, J.J.P.; et al. Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein. N. Engl. J. Med. 2008, 359, 2195–2207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janicki-Deverts, D.; Cohen, S.; Kalra, P.; Matthews, K.A. The prospective association of socioeconomic status with C-reactive protein levels in the CARDIA study. Brain Behav. Immun. 2012, 26, 1128–1135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Medenwald, D.; Loppnow, H.; Kluttig, A.; Nuding, S.; Greiser, K.H.; Thiery, J.; Tiller, D.A.; Herzog, B.; Werdan, K.; Haerting, J. Educational level and chronic inflammation in the elderly-the role of obesity: Results from the population-based CARLA study. Clin. Obes. 2015, 5, 256–265. [Google Scholar] [CrossRef]
- Abramson, M.J.; Blackman, J.; Carroll, M.; Dimitriadis, C.; Del Monaco, A.; Dennekamp, M.; Denny, D.; Gao, C.; Liew, D.; Maybery, D. Hazelwood Health Study Adult Survey Report: Volume 1 Comparison of Morwell and Sale. 2017. Available online: https://hazelwoodhealthstudy.org.au/study-findings/study-reports (accessed on 11 January 2021).
- Lucht, S.A.; Hennig, F.; Matthiessen, C.; Ohlwein, S.; Icks, A.; Moebus, S.; Jöckel, K.-H.; Jakobs, H.; Hoffmann, B. Air pollution and glucose metabolism: An analysis in non-diabetic participants of the Heinz Nixdorf recall study. Environ. Health Perspect. 2018, 126, 047001. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, J.D.; Adar, S.D.; Roux, A.V.D.; Jacobs, D.R.; Kronmal, R.A.; Larson, T.V.; Liu, S.L.-J.; Lumley, T.; Navas-Acien, A.; O’Leary, D.H.; et al. Prospective study of particulate air pollution exposures, subclinical atherosclerosis, and clinical cardiovascular disease: The multi-ethnic study of atherosclerosis and air pollution (Mesa air). Am. J. Epidemiol. 2012, 176, 825–837. [Google Scholar] [CrossRef] [Green Version]
- Oikonomou, E.; Lazaros, G.; Georgiopoulos, G.; Christoforatou, E.; Papamikroulis, G.A.; Vogiatzi, G.; Chasikidis, C.; Zacharia, E.; Giannaki, A.; Bourouki, E.; et al. Environment and cardiovascular disease: Rationale of the Corinthia study. Hell. J. Cardiol. 2016, 57, 194–197. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Characteristic | Morwell (Exposed) N = 336 | Sale (Unexposed) N = 162 | p-Value | ||
|---|---|---|---|---|---|
| n | Weighted % | n | Weighted % | ||
| Age Category | |||||
| 55–69 years | 150 | 45.9 | 72 | 49.1 | 0.785 |
| 70–79 | 127 | 35.7 | 63 | 32.6 | |
| 80+ | 59 | 18.4 | 27 | 18.3 | |
| Gender (female) | 150 | 45.2 | 70 | 43 | 0.618 |
| Ethnicity (Caucasian/white) | 320 | 95.8 | 157 | 99.1 | 0.033 |
| Employment status | |||||
| Employed | 50 | 16.9 | 41 | 29.1 | 0.013 |
| Retired | 261 | 75.2 | 111 | 65.8 | |
| Other | 25 | 7.9 | 8 | 5.1 | |
| Highest educational qualification | |||||
| Secondary ≤ year 10 | 136 | 40.5 | 55 | 32.7 | 0.288 |
| Secondary years 11 or 12 | 53 | 15.7 | 33 | 21.1 | |
| Certificate (trade/apprenticeship/technicians) | 106 | 31.9 | 55 | 35.3 | |
| University/Tertiary degree | 39 | 11.9 | 18 | 10.9 | |
| IRSD Score | Weighted Mean | SEM | Weighted Mean | SEM | p-value |
| 867.4 | 8.5 | 928.2 | 4.7 | <0.001 | |
| Characteristic | Morwell (Exposed) N = 336 | Sale (Unexposed) N = 162 | p-Value | ||
|---|---|---|---|---|---|
| n | Weighted % | n | Weighted % | ||
| History of cardiovascular diseases * | |||||
| Prior to 2014 | 113 | 28.2 | 62 | 33 | 0.559 |
| Since 2014 | 49 | 12.6 | 18 | 11.8 | |
| Diabetes † | 84 | 22.9 | 29 | 16.1 | 0.096 |
| Smoking status | |||||
| Non-smoker | 157 | 46.4 | 86 | 54.1 | 0.123 |
| Ex-smoker | 151 | 44.6 | 68 | 41.4 | |
| Current smoker | 28 | 9 | 8 | 4.4 | |
| Alcohol consumption | |||||
| Non-drinker | 87 | 25 | 37 | 23 | 0.341 |
| Low risk | 125 | 36.3 | 50 | 31.1 | |
| High risk | 124 | 38.7 | 74 | 46 | |
| Taking antihypertensive medications | 237 | 67.8 | 99 | 59.7 | 0.091 |
| Taking lipid-lowering therapy | 168 | 47.7 | 63 | 37.1 | 0.038 |
| Taking anti-inflammatory or immunosuppressant medications | 75 | 20.6 | 23 | 12.7 | 0.031 |
| Engaged in adequate physical activity | 150 | 45.2 | 98 | 60.3 | 0.003 |
| BMI | |||||
| Underweight/normal | 56 | 17.6 | 40 | 24.4 | 0.105 |
| Overweight | 112 | 33.9 | 57 | 36.5 | |
| Obese | 168 | 48.5 | 65 | 39.1 | |
| eGFR | |||||
| <60 mL/min/1.73 m2 | 60 | 17.1 | 22 | 13.5 | 0.323 |
| HbA1c (%) | Weighted Mean | SEM | Weighted Mean | SEM | p-value |
| 6.1 | 0.1 | 5.8 | 0.1 | <0.001 | |
| Outcome Variable | Morwell (Exposed) N = 336 | Sale (Unexposed) N = 162 | p-Value | ||
|---|---|---|---|---|---|
| Weighted Median | IQR | Weighted Median | IQR | ||
| Biomarkers | |||||
| hsCRP (mg/L) | 1.9 | 1.0–3.9 | 1.6 | 0.8–3.4 | 0.273 * |
| Fibrinogen (g/L) | 3.6 | 3.2–4.1 | 3.5 | 3.1–4.0 | 0.406 |
| NTproBNP (ng/L) | 99.0 | 55.0–241.0 | 100.0 | 50.0–186.0 | 0.349 * |
| Troponin (ng/L) | 3.0 | 2.0–5.0 | 3.0 | 2.0–5.0 | 0.079 * |
| Total cholesterol (mmol/L) | 4.5 | 3.9–5.2 | 4.9 | 4.1–5.4 | 0.005 |
| HDL (mmol/L) | 1.3 | 1.0–1.6 | 1.3 | 1.0–1.5 | 0.286 |
| LDL (mmol/L) | 2.3 | 1.7–3.0 | 2.7 | 2.1–3.2 | 0.005 |
| Triglycerides (mmol/L) | 1.7 | 1.2–2.4 | 1.6 | 1.2–2.3 | 0.236 |
| Peak FMD (%) † | 3.8 | 2.0–5.3 | 3.6 | 2.0–5.5 | 0.999 |
| Blood pressure | |||||
| Systolic BP (mmHg) | 132 | 120–145 | 134 | 126–146 | 0.059 |
| Diastolic BP (mmHg) | 71 | 64–79 | 74 | 67–81 | 0.059 |
| n | Weighted % | N | Weighted % | p-value | |
| ECG | |||||
| Rhythm abnormality | |||||
| No | 229 | 92.3 | 102 | 89.4 | 0.583 |
| Atrial Fibrillation | 17 | 5.6 | 12 | 8.6 | |
| Other | 7 | 2.1 | 2 | 2.1 | |
| Evidence of underlying IHD | |||||
| Yes | 57 | 15.9 | 21 | 10.9 | 0.120 |
| Predictors | Mean Diff | 95% CI | p-Value | Adj Mean Diff * | 95% CI | p-Value |
|---|---|---|---|---|---|---|
| Exposure group (Morwell) | 0.13 | −0.09, 0.35 | 0.240 | 0.06 | −0.15, 0.27 | 0.583 |
| Age (per 5 years) | 0.02 | −0.04, 0.09 | 0.459 | 0.05 | −0.02, 0.13 | 0.140 |
| Gender (Female) | 0.06 | −0.13, 0.26 | 0.530 | 0.13 | −0.07, 0.33 | 0.187 |
| Employment status (Employed) | −0.09 | −0.34, 0.15 | 0.455 | 0.10 | −0.16, 0.35 | 0.457 |
| Highest educational qualification | ||||||
| Secondary ≤ year 10 | Ref | Ref | ||||
| Secondary years 11 or 12 | −0.08 | −0.35, 0.19 | 0.552 | 0.17 | −0.10, 0.43 | 0.229 |
| Certificate (trade/ apprenticeship/technicians) | −0.04 | −0.29, 0.20 | 0.716 | 0.08 | −0.16, 0.31 | 0.510 |
| University/Tertiary degree | −0.54 | −0.81, −0.28 | <0.001 | −0.29 | −0.57, 0.00 | 0.046 |
| Smoking status | ||||||
| Non-smoker | Ref | Ref | ||||
| Ex-smoker | 0.06 | −0.15, 0.26 | 0.601 | 0.06 | −0.15, 0.28 | 0.572 |
| Current smoker | 0.40 | 0.08, 0.72 | 0.015 | 0.52 | 0.21, 0.84 | 0.001 |
| Alcohol consumption | ||||||
| Non-drinker | Ref | Ref | ||||
| Low risk | −0.05 | −0.31, 0.21 | 0.695 | −0.06 | −0.30, 0.17 | 0.590 |
| High risk | −0.13 | −0.37, 0.11 | 0.298 | −0.03 | −0.26, 0.21 | 0.818 |
| Adequate physical activity | −0.17 | −0.37, 0.03 | 0.093 | −0.05 | −0.24, 0.15 | 0.642 |
| Taking lipid-lowering therapy | −0.19 | −0.38, 0.01 | 0.058 | −0.29 | −0.49, −0.08 | 0.006 |
| Taking anti-inflammatory or immunosuppressant medications | 0.05 | −0.22, 0.33 | 0.697 | −0.02 | −0.27, 0.23 | 0.886 |
| BMI | ||||||
| Underweight/Normal (BMI < 25 kg/m2) | Ref | Ref | ||||
| Overweight (25 ≤ BMI <3 0) | 0.44 | 0.16, 0.72 | 0.002 | 0.54 | 0.25, 0.83 | <0.001 |
| Obese (BMI >30 kg/m2) | 0.74 | 0.48, 1.01 | <0.001 | 0.79 | 0.52, 1.06 | <0.001 |
| HbA1c (%) | 0.13 | 0.05, 0.21 | 0.001 | 0.11 | 0.04, 0.18 | 0.004 |
| Outcomes | Exposed vs. Unexposed | |||
|---|---|---|---|---|
| Crude Mean Diff (95% CI) | p-Value | Adj Mean Diff * (95% CI) | p-Value | |
| Serum Biomarkers | ||||
| Log NTproBNP | 0.06 (−0.14, 0.27) | 0.550 | 0.07 (−0.11, 0.25) | 0.451 |
| Log Troponin | 0.13 (0.00, 0.27) | 0.046 | 0.09 (−0.03, 0.21) | 0.124 |
| Total cholesterol | −0.28 (−0.46, −0.09) | 0.004 | −0.14 (−0.30, 0.01) | 0.070 |
| HDL | −0.04 (−0.12, 0.04) | 0.286 | 0.02 (−0.04, 0.08) | 0.539 |
| LDL | −0.28 (−0.45, −0.10) | 0.002 | −0.15 (−0.30, −0.01) | 0.038 |
| Triglycerides | 0.11 (−0.08, 0.31) | 0.257 | 0.00 (−0.18, 0.19) | 0.975 |
| Peak FMD (%) ‡ | 0.08 (−0.48, 0.64) | 0.773 | −0.01 (−0.54, 0.52) | 0.967 |
| Blood pressure | ||||
| Systolic BP (mmHg) | −3.28 (−6.68, 0.13) | 0.059 | −3.75 (−7.23, −0.26) | 0.035 |
| Diastolic BP (mmHg) | −2.07 (−4.21, 0.08) | 0.059 | −1.74 (−3.80, 0.31) | 0.097 |
| Crude OR (95% CI) | p-value | Adj OR † (95% CI) | p-value | |
| ECG | ||||
| Atrial Fibrillation | 0.68 (0.31, 1.52) | 0.350 | 0.41 (0.14, 1.16) | 0.094 |
| Other rhythm abnormality | 0.75 (0.36, 1.56) | 0.442 | 0.50 (0.20, 1.23) | 0.130 |
| Evidence of underlying IHD | 1.55 (0.89, 2.69) | 0.122 | 1.52 (0.83, 2.78) | 0.177 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Betts, J.; Dewar, E.M.; Stub, D.; Gao, C.X.; Brown, D.W.; Ikin, J.F.; Zeleke, B.M.; Biswas, S.; Abramson, M.J.; Liew, D. Markers of Cardiovascular Disease among Adults Exposed to Smoke from the Hazelwood Coal Mine Fire. Int. J. Environ. Res. Public Health 2021, 18, 1587. https://doi.org/10.3390/ijerph18041587
Betts J, Dewar EM, Stub D, Gao CX, Brown DW, Ikin JF, Zeleke BM, Biswas S, Abramson MJ, Liew D. Markers of Cardiovascular Disease among Adults Exposed to Smoke from the Hazelwood Coal Mine Fire. International Journal of Environmental Research and Public Health. 2021; 18(4):1587. https://doi.org/10.3390/ijerph18041587
Chicago/Turabian StyleBetts, Juliana, Elizabeth M. Dewar, Dion Stub, Caroline X. Gao, David W. Brown, Jillian F. Ikin, Berihun M. Zeleke, Sinjini Biswas, Michael J. Abramson, and Danny Liew. 2021. "Markers of Cardiovascular Disease among Adults Exposed to Smoke from the Hazelwood Coal Mine Fire" International Journal of Environmental Research and Public Health 18, no. 4: 1587. https://doi.org/10.3390/ijerph18041587
APA StyleBetts, J., Dewar, E. M., Stub, D., Gao, C. X., Brown, D. W., Ikin, J. F., Zeleke, B. M., Biswas, S., Abramson, M. J., & Liew, D. (2021). Markers of Cardiovascular Disease among Adults Exposed to Smoke from the Hazelwood Coal Mine Fire. International Journal of Environmental Research and Public Health, 18(4), 1587. https://doi.org/10.3390/ijerph18041587