
Psychosocial Interventions to Improve Psychological, Social and Physical Wellbeing in Family Members Affected by an Adult Relative’s Substance Use: A Systematic Search and Review of the Evidence

 ,
,  and
and
Abstract
:1. Introduction
Study Objectives
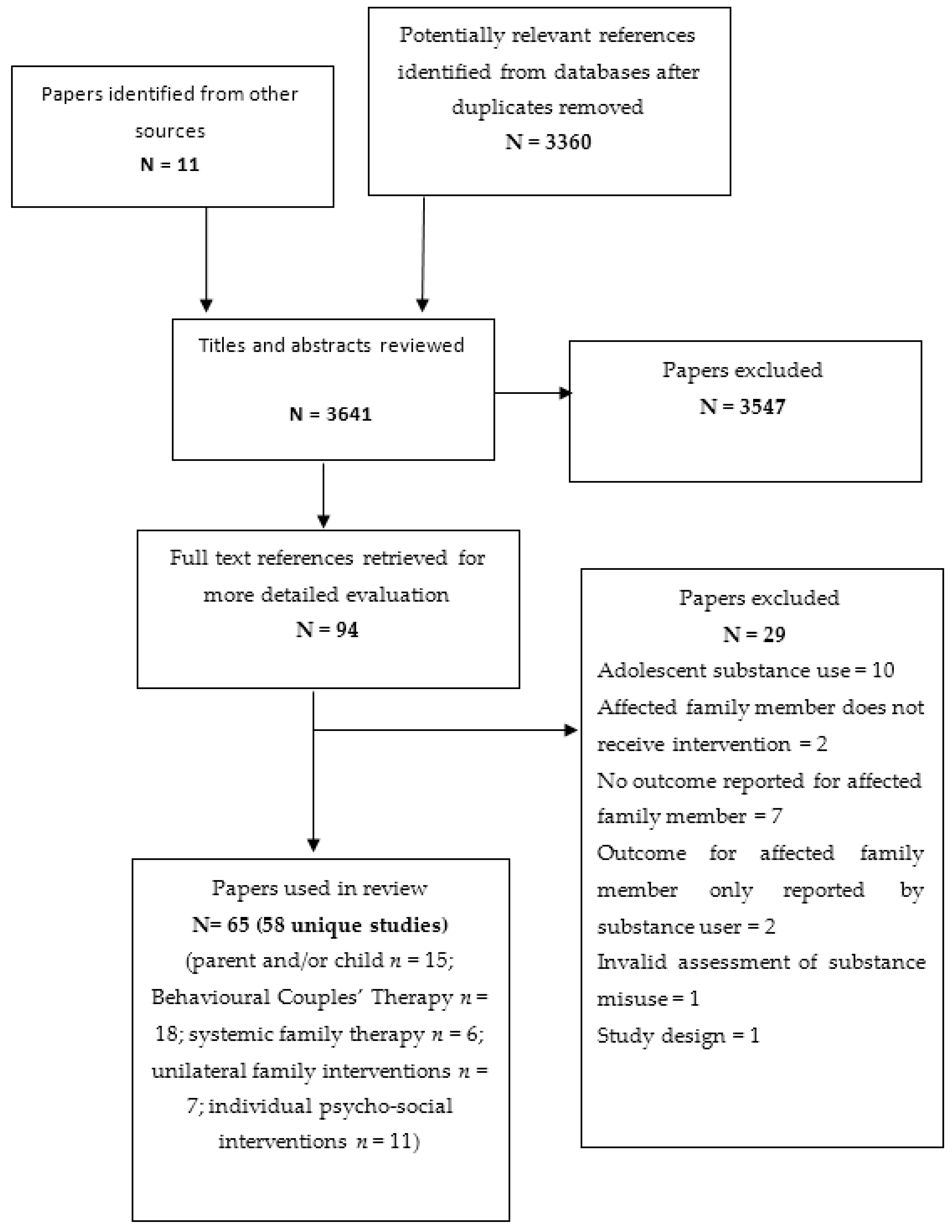
2. Methods
Review Inclusion Criteria
3. Results
3.1. Description of Studies
3.2. Parental and Child Interventions (15 Trials)
3.3. Behavioural Couples and Family Therapy (19 Trials)
3.4. Systemic Family Interventions (6 Trials)
3.5. Unilateral Family Interventions (7 Trials)
3.6. Psychosocial Interventions for the Individual Affected Family Member (11 Trials)
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Peacock, A.; Leung, J.; Larney, S.; Colledge, S.; Hickman, M.; Rehm, J.; Giovino, A.G.; West, R.; Hall, W.; Griffiths, P.; et al. Global statistics on alcohol, tobacco and illicit drugs: 2017 status report. Addiction 2018, 113, 1905–1926. [Google Scholar] [CrossRef] [Green Version]
- GBD 2016 Alcohol and Drug Use Collaborators. The global burden of disease attributable to alcohol and drug use in 195 countries and territories, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2018, 5, 987–1012. [Google Scholar]
- Orford, J.; Velleman, R.; Natera, G.; Templeton, L.; Copello, A. Addiction in the family is a major but neglected contributor to the global burden of adult ill-health. Soc. Sci. Med. 2013, 78, 70–77. [Google Scholar] [CrossRef] [Green Version]
- Orford, J. Coping with Disorder in the Family. Croom Helm: London, UK, 1987. [Google Scholar]
- Laslett, A.; Catalano, P.; Chikritzhs, T.; Dale, C.; Doran, C.; Ferris, J.; Jainullabudeen, A.; Livingston, M.J.; Matthews, S.; Mugavin, J.; et al. The Range and Magnitude of Alcohol’s Harm to Others: Beyond the Drinker: Alcohol’s Hidden Costs; AER Foundation: Dublin, Ireland, 2010; ISBN 978-0-9808243-1-5. [Google Scholar]
- Ray, G.T.; Mertens, J.R.; Weisner, C. Family members of people with alcohol or drug dependence: Health problems and medical cost compared to family members of people with diabetes and asthma. Addiction 2009, 104, 203–214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Newton, E.; Shepherd, N.; Orford, J.; Copello, A. Could the substance misuse of a relative be an important factor for those seeking help for anxiety and depression? A preliminary prevalence study within improving access to psychological therapies (IAPT). Behav. Cogn. Psychother. 2016, 44, 723–729. [Google Scholar] [CrossRef]
- Orford, J.; Natera, G.; Copello, A.; Atkinson, C.; Mora, J.; Velleman, R. Coping with alcohol and drug problems. In The Experiences of Family Members in Three Contrasting Cultures; Brunner-Routledge: London, UK, 2005. [Google Scholar]
- Orford, J.; Velleman, R.; Copello, A.; Templeton, L.; Ibanga, A. The experiences of affected family members: A summary of two decades of qualitative research. Drugs Educ. Prev. Policy 2010, 17, 44–62. [Google Scholar] [CrossRef] [Green Version]
- Cafferky, B.M.; Mendez, M.; Anderson, J.R.; Stith, S.M. Substance use and intimate partner violence: A meta-analytic review. Psychol. Violence 2018, 8, 110–131. [Google Scholar] [CrossRef]
- Foran, H.M.; O’Leary, K.D. Alcohol and intimate partner violence: A meta-analytic review. Clin. Psychol. Rev. 2008, 28, 1222–1234. [Google Scholar] [CrossRef]
- Devries, K.M.; Child, J.C.; Bacchus, L.J.; Mak, J.; Falder, G.; Graham, K.; Watts, C.; Heise, L. Intimate partner violence victimization and alcohol consumption in women: A systematic review and meta-analysis. Addiction 2014, 109, 379–391. [Google Scholar] [CrossRef]
- Graham, K.; Bernards, S.; Wilsnack, S.C.; Gmel, G. Alcohol may not cause partner violence but it seems to make it worse: A cross national comparison of the relationship between alcohol and severity of partner violence. J. Interpers. Violence 2010, 26, 1503–1523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGovern, R.; Gilvarry, E.; Addison, M.; Geijer-Simpson, E.; Lingham, R.; Smart, D.; Kaner, E. The association between child adverse health, psychological, educational and social outcomes and non-dependent parental substance misuse: A rapid evidence assessment. Trauma Violence Abus. 2018, 21, 470–483. [Google Scholar] [CrossRef] [Green Version]
- Canfield, M.; Radcliffe, P.; Marlow, S.; Boreham, M.; Gilchrist, G. Maternal substance use and child protection: A rapid evidence assessment of factors associated with loss of child care. Child Abus. Negl. 2017, 70, 11–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baker, R.; Orton, E.; Tata, L.J.; Kendrick, D. Risk factors for long-bone fractures in children up to 5 years of age: A nested case-control study. Arch. Dis. Child. 2015, 100, 432–437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cleaver, H.; Unell, I.; Aldgate, J. Children’s needs: Parenting capacity. In Child abuse: Parental Mental Illness, Learning Disability, Substance Misuse, and Domestic Violence; Department for Education: London, UK, 2011. [Google Scholar]
- Barnard, M. Drug Addiction and Families; Jessica Kingsley Publishers: London, UK, 2007. [Google Scholar]
- Berg, L.; Back, K.; Vinnerljung, B.; Hjern, A. Parental alcohol-related disorders and school performance in 16-year-olds—A Swedish national cohort study. Addiction 2016, 111, 1795–1803. [Google Scholar] [CrossRef]
- Velleman, R. The policy context: Reversing a state of neglect. Drugs Educ. Prev. Policy 2010, 17, 8–35. [Google Scholar] [CrossRef]
- Rane, A.; Church, S.; Bhatia, U.; Orford, J.; Velleman, R.; Nadkarni, A. Psychosocial interventions for addiction-affected families in low and middle income countries: A systematic review. Addict. Behav. 2017, 74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Templeton, L.; Velleman, R.; Russell, C. Psychological interventions with families of alcohol misusers: A systematic review. Addict. Res. Theory 2010, 18, 616–648. [Google Scholar] [CrossRef]
- Grant, M.J.; Booth, A. A typology of reviews: An analysis of 14 review types and associated methodologies. Health Inf. Libr. J. 2009, 26, 91–108. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. 2011. Available online: www.cochrane-handbook.org (accessed on 12 December 2020).
- Catalano, R.F.; Gainey, R.R.; Fleming, C.B.; Haggerty, K.P.; Johnson, N.O. An experimental intervention with families of substance abusers: One-year follow-up of the focus on families project. Addiction 1999, 94, 241–254. [Google Scholar] [CrossRef] [PubMed]
- Lam, W.K.; Fals-Stewart, W.; Kelley, M.L. Parent training with behavioral couples therapy for fathers’ alcohol abuse: Effects on substance use, parental relationship, parenting, and CPS involvement. Child Maltreat. 2009, 14, 243–254. [Google Scholar] [CrossRef] [PubMed]
- Orte, C.; Touza, C.; Ballester, L.; March, M. Children of drug-dependent parents: Prevention programme outcomes. Educ. Res. 2008, 50, 249–260. [Google Scholar] [CrossRef]
- Bennun, I. Treating the system or symptom? Investigating family therapy for alcohol problems. Behav. Psychother. 1988, 16, 165–176. [Google Scholar] [CrossRef]
- Donohue, B.; Azrin, N.H.; Bradshaw, K.; Van Hasselt, V.B.; Cross, C.L.; Urgelles, J.; Romero, V.; Hill, H.H.; Allen, D.N. A controlled evaluation of family behavior therapy in concurrent child neglect and drug abuse. J. Consult. Clin. Psychol. 2014, 82, 706–720. [Google Scholar] [CrossRef] [Green Version]
- Kelley, M.L.; Fals-Stewart, W. Couples- versus individual-based therapy for alcohol and drug abuse: Effects on children’s psychosocial functioning. J. Consult. Clin. Psychol. 2002, 70, 417–427. [Google Scholar] [CrossRef]
- Haggerty, K.P.; Skinner, M.; Fleming, C.B.; Gainey, R.R.; Catalano, R.F. Long-term effects of the Focus on Families project on substance use disorders among children of parents in methadone treatment. Addiction 2008, 103, 2008–2016. [Google Scholar] [CrossRef]
- Broning, S.; Sack, P.-M.; Haevelmann, A.; Wartberg, L.; Moesgen, D.; Klein, M.; Thomasius, R. A new preventive intervention for children of substance-abusing parents: Results of a randomized controlled trial. Child Fam. Soc. Work. 2019, 24, 537–546. [Google Scholar] [CrossRef]
- Hojjat, S.K.; Rezaei, M.; Namadian, G.; Hatami, S.E.; Khalili, M.N. Effectiveness of emotional intelligence group training on anger in adolescents with substance-abusing fathers. J. Child Adolesc. Subst. Abus. 2017, 26, 24–29. [Google Scholar] [CrossRef]
- Hojjat, S.K.; Golmakani, E.; Norozi Khalili, M.; Shakeri Chenarani, M.; Hamidi, M.; Akaberi, A.; Ardani, R.A. The effectiveness of group assertiveness training on happiness in rural adolescent females with substance abusing parents. Glob. J. Health Sci. 2015, 8, 156–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kingree, J.; Thompson, M. Mutual help groups, perceived status benefits, and well-being: A test with adult children of alcoholics with personal substance abuse problems. Am. J. Community Psychol. 2000, 28, 325–342. [Google Scholar] [CrossRef] [PubMed]
- Kuhns, M.L. Treatment outcomes with adult children of alcoholics: Depression. Adv. Pract. Nurs. Q. 1997, 3, 64–69. [Google Scholar]
- Gustafson, D.H.; McTavish, F.M.; Schubert, C.J.; Johnson, R.A. The effect of a computer-based intervention on adult children of alcoholics. J. Addict. Med. 2012, 6, 24–28. [Google Scholar] [CrossRef] [PubMed]
- Osterndorf, C.L.; Enright, R.D.; Holter, A.C.; Klatt, J.S. Treating adult children of alcoholics through forgiveness therapy. Alcohol. Treat. Q. 2011, 29, 274–292. [Google Scholar] [CrossRef]
- Hansson, H.; Rundberg, J.; Zetterlind, U.; Johnsson, K.O.; Berglund, M. An intervention program for university students who have parents with alcohol problems: A randomized controlled trial. Alcohol Alcohol. 2006, 41, 655–663. [Google Scholar] [CrossRef] [Green Version]
- Fals-Stewart, W.; Clinton-Sherrod, M. Treating intimate partner violence among substance-abusing dyads: The effect of couples therapy. Prof. Psychol. Res. Pract. 2009, 40, 257–263. [Google Scholar] [CrossRef]
- Fals-Stewart, W.; Kashdan, T.B.; O’Farrell, T.J.; Birchler, G.R. Behavioral couples therapy for drug-abusing patients: Effects on partner violence. J. Subst. Abus. Treat. 2002, 22, 87–96. [Google Scholar] [CrossRef]
- Fals-Stewart, W.; Birchler, G.R.; Kelley, M.L. Learning sobriety together: A randomized clinical trial examining behavioral couples therapy with alcoholic female patients. J. Consult. Clin. Psychol. 2006, 74, 579–591. [Google Scholar] [CrossRef] [PubMed]
- Walitzer, K.; Dermen, K.; Shyhalla, K.; Kubiak, A. Couple communication among problem drinking males and their spouses: A randomized controlled trial. J. Fam. Ther. 2013, 35, 229–251. [Google Scholar] [CrossRef]
- Halford, W.K.; Price, J.; Kelly, A.B.; Bouma, R.; Young, R.M. Helping the female partners of men abusing alcohol: A comparison of three treatments. Addiction 2001, 96, 1497–1508. [Google Scholar] [CrossRef]
- Schumm, J.A.; O’Farrell, T.J.; Kahler, C.W.; Murphy, M.M.; Muchowski, P. A randomized clinical trial of behavioral couples therapy versus individually based treatment for women with alcohol dependence. J. Consult. Clin. Psychol. 2014, 82, 993–1004. [Google Scholar] [CrossRef] [Green Version]
- Winters, J.; Fals-Stewart, W.; O’Farrell, T.J.; Birchler, G.R.; Kelley, M.L. Behavioral couples therapy for female substance-abusing patients: Effects on substance use and relationship adjustment. J. Consult. Clin. Psychol. 2002, 70, 344–355. [Google Scholar] [CrossRef]
- Fals-Stewart, W.; O’Farrell, T.J.; Birchler, G.R. Behavioral couples therapy for male methadone maintenance patients: Effects on drug-using behavior and relationship adjustment. Behav. Ther. 2001, 32, 391–411. [Google Scholar] [CrossRef]
- O’Farrell, T.J.; Cutter, H.S.; Floyd, F.J. Evaluating behavioral marital therapy for male alcoholics: Effects on marital adjustment and communication from before to after treatment. Behav. Ther. 1985, 16, 147–167. [Google Scholar] [CrossRef]
- McCrady, B.; Noel, N.; Abrams, D.B.; Stout, R.; Nelson, H.; Hay, W. Comparative effectiveness of three types of spouse involvement in outpatient behavioral alcoholism treatment. J. Stud. Alcohol 1986, 47, 459–467. [Google Scholar] [CrossRef] [PubMed]
- O’Farrell, T.J.; Schumm, J.A.; Dunlap, L.J.; Murphy, M.M.; Muchowski, P. A randomized clinical trial of group versus standard behavioral couples therapy plus individually based treatment for patients with alcohol dependence. J. Consult. Clin. Psychol. 2016, 84, 497–510. [Google Scholar] [CrossRef] [PubMed]
- O’Farrell, T.J.; Schumm, J.A.; Murphy, M.M.; Muchowski, P.M. A randomized clinical trial of behavioral couples therapy versus individually-based treatment for drug-abusing women. J. Consult. Clin. Psychol. 2017, 85, 309–322. [Google Scholar] [CrossRef]
- Fals-Stewart, W.; O’Farrell, T.J.; Lam, W.K. Behavioral couple therapy for gay and lesbian couples with alcohol use disorders. J. Subst. Abus. Treat. 2009, 37, 379–387. [Google Scholar] [CrossRef] [Green Version]
- Fals-Stewart, W.; Klostermann, K.; Yates, B.T.; O’Farrell, T.J.; Birchler, G.R. Brief relationship therapy for alcoholism: A randomized clinical trial examining clinical efficacy and cost-effectiveness. Psychol. Addict. Behav. 2005, 19, 363–371. [Google Scholar] [CrossRef] [Green Version]
- McCrady, B.; Stout, R.; Noel, N.; Abrams, D.B.; Nelson, H. Effectiveness of three types of spouse-involved behavioral alcoholism treatment. Br. J. Addict. 1991, 86, 1415–1424. [Google Scholar] [CrossRef]
- O’Farrell, T.J.; Choquette, K.A.; Cutter, H.S.; Brown, E.D.; McCourt, W.F. Behavioral marital therapy with and without additional couples relapse prevention sessions for alcoholics and their wives. J. Stud. Alcohol 1993, 54, 652–666. [Google Scholar] [CrossRef]
- O’Farrell, T.J.; Choquette, K.A.; Cutter, H.S. Couples relapse prevention sessions after behavioral marital therapy for male alcoholics: Outcomes during the three years after starting treatment. J. Stud. Alcohol. 1998, 59, 357–370. [Google Scholar] [CrossRef]
- O’Farrell, T.J.; Cutter, H.S.; Choquette, K.A.; Floyd, F.J.; Bayog, R.D. Behavioral marital therapy for male alcoholics: Marital and drinking adjustment during the two years after treatment. Behav. Ther. 1992, 23, 529–549. [Google Scholar] [CrossRef]
- Vedel, E.; Emmelkamp, P.M.; Schippers, G.M. Individual cognitive-behavioral therapy and behavioral couples therapy in alcohol use disorder: A comparative evaluation in community-based addiction treatment centers. Psychother. Psychosom. 2008, 77, 280–288. [Google Scholar] [CrossRef]
- Walitzer, K.S.; Dermen, K.H. Alcohol-focused spouse involvement and behavioral couples therapy: Evaluation of enhancements to drinking reduction treatment for male problem drinkers. J. Consult. Clin. Psychol. 2004, 72, 944–955. [Google Scholar] [CrossRef]
- O’Farrell, T.J.; Murphy, M.; Alter, J.; Fals-Stewart, W. Behavioral family counseling for substance abuse: A treatment development pilot study. Addict. Behav. 2010, 35. [Google Scholar] [CrossRef] [Green Version]
- Kuenzler, A.; Beutler, L.E. Couple alcohol treatment benefits patients’ partners. J. Clin. Psychol. 2003, 59, 791–806. [Google Scholar] [CrossRef]
- Ahmad-Abadi, F.K.; Maarefvand, M.; Aghaei, H.; Hosseinzadeh, S.; Abbasi, M.; Khubchandani, J. effectiveness of satir-informed family-therapy on the codependency of drug dependents’ family members in Iran: A randomized controlled trial. J. Evid. Inf. Soc. Work. 2017, 14, 301–310. [Google Scholar] [CrossRef] [PubMed]
- Mueser, K.T.; Glynn, S.M.; Cather, C.; Xie, H.; Zarate, R.; Smith, L.F.; Clark, E.R.; Gottlieb, D.J.; Wolfe, R.; Feldman, J. A randomized controlled trial of family intervention for co-occurring substance use and severe psychiatric disorders. Schizophr. Bull. 2013, 39, 658–672. [Google Scholar] [CrossRef] [Green Version]
- Li, L.; Hien, N.T.; Lin, C.; Tuan, N.A.; Tuan, L.A.; Farmer, S.C.; Detels, R. An intervention to improve mental health and family well-being of injecting drug users and family members in Vietnam. Psychol. Addict. Behav. 2014, 28, 607–613. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghasemi, A.; Rahimi Foroshani, A.; Kheibar, N.; Latifi, M.; Khanjani, N.; Eshagh Afkari, M.; Taghdisi, H.M.; Ghasemi, F.; Shojaeizadeh, D.; Dastoorpour, M. Effects of family-centered empowerment model based education program on quality of life in methamphetamine users and their families. Iran. Red Crescent Med. J. 2014, 16, e13375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zweben, A.; Pearlman, S.; Li, S. A comparison of brief advice and conjoint therapy in the treatment of alcohol abuse: The results of the martial systems study. Br. J. Addict. 1988, 83, 899–916. [Google Scholar] [CrossRef] [PubMed]
- Barber, J.G.; Gilbertson, R. An experimental study of brief unilateral intervention for the partners of heavy drinkers. Res. Soc. Work. Pract. 1996, 6, 325–336. [Google Scholar] [CrossRef]
- Barber, J.G.; Gilbertson, R. Evaluation of a self-help manual for the female partners of heavy drinkers. Res. Soc. Work. Pract. 1998, 8, 141–151. [Google Scholar] [CrossRef]
- Barber, J.G.; Crisp, B.R. The “pressures to change” approach to working with the partners of heavy drinkers. Addiction 1995, 90, 269–276. [Google Scholar] [PubMed]
- Miller, W.R.; Meyers, R.J.; Tonigan, J.S. Engaging the unmotivated in treatment for alcohol problems: A comparison of three strategies for intervention through family members. J. Consult. Clin. Psychol. 1999, 67, 688–697. [Google Scholar] [CrossRef]
- Kirby, K.C.; Marlowe, D.B.; Festinger, D.S.; Garvey, K.A.; La Monaca, V. Community reinforcement training for family and significant others of drug abusers: A unilateral intervention to increase treatment entry of drug users. Drug Alcohol Depend. 1999, 56, 85–96. [Google Scholar] [CrossRef]
- Bischof, G.; Iwen, J.; Freyer-Adam, J.; Rumpf, H.J. Efficacy of the Community Reinforcement and Family Training for concerned significant others of treatment-refusing individuals with alcohol dependence: A randomized controlled trial. Drug Alcohol Depend. 2016, 163, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Eek, N.; Romberg, K.; Siljeholm, O.; Johansson, M.; Andreasson, S.; Lundgren, T.; Fahlke, C.; Ingesson, S.; Bäckman, L.; Hammarberg, A. Efficacy of an internet-based community reinforcement and family training program to increase treatment engagement for AUD and to improve psychiatric health for CSOs: A randomized controlled trial. Alcohol Alcohol. 2020, 55, 187–195. [Google Scholar] [CrossRef]
- Rychtarik, R.G.; McGillicuddy, N.B. Coping skills training and 12-step facilitation for women whose partner has alcoholism: Effects on depression, the partner’s drinking, and partner physical violence. J. Consult. Clin. Psychol. 2005, 73, 249–261. [Google Scholar] [CrossRef] [Green Version]
- Velleman, R.; Orford, J.; Templeton, L.; Copello, A.; Patel, A.; Moore, L.; Macleod, J.; Godfrey, C. 12-month follow-up after brief interventions in primary care for family members affected by the substance misuse problem of a close relative. Addict. Res. Theory 2011, 19, 362–374. [Google Scholar] [CrossRef] [Green Version]
- Copello, A.; Templeton, L.; Orford, J.; Velleman, R.; Patel, A.; Moore, L.; MacLeod, J.; Godfrey, C. The relative efficacy of two levels of a primary care intervention for family members affected by the addiction problem of a close relative: A randomized trial. Addiction 2009, 104, 49–58. [Google Scholar] [CrossRef]
- Zetterlind, U.; Hansson, H.; Aberg-Orbeck, K.; Berglund, M. Effects of coping skills training, group support, and information for spouses of alcoholics: A controlled randomized study. Nord. J. Psychiatry 2001, 55, 257–262. [Google Scholar] [CrossRef] [PubMed]
- Hansson, H.; Zetterlind, U.; Aberg-Orbeck, K.; Berglund, M. Two-year outcome of coping skills training, group support and information for spouses of alcoholics: A randomized controlled trial. Alcohol Alcohol. 2004, 39, 135–140. [Google Scholar] [CrossRef] [Green Version]
- Osilla, K.C.; Trail, T.E.; Pedersen, E.R.; Gore, K.L.; Tolpadi, A.; Rodriguez, L.M. Efficacy of a web-based intervention for concerned spouses of service members and veterans with alcohol misuse. J. Marital. Fam. Ther. 2018, 44, 292–306. [Google Scholar] [CrossRef] [PubMed]
- Dittrich, J.E.; Trapold, M.A. A treatment program for wives of alcoholics: An evaluation. Bull. Soc. Psychol. Addict. Behav. 1984, 3, 91–102. [Google Scholar]
- Rodriguez, L.M.; Osilla, K.C.; Trail, T.E.; Gore, K.L.; Pedersen, E.R. Alcohol use among concerned partners of heavy drinking service members and veterans. J. Marital. Fam. Ther. 2018, 44, 277–291. [Google Scholar] [CrossRef] [PubMed]
- de los Angeles Cruz-Almanza, M.; Gaona-Marquez, L.; Sanchez-Sosa, J.J. Empowering women abused by their problem drinker spouses: Effects of a cognitive-behavioral intervention. Salud Ment. 2006, 29, 25–31. [Google Scholar]
- Bortolon, C.B.; Moreira, T.C.; Signor, L.; Guahyba, B.L.; Figueiro, L.R.; Ferigolo, M.; Tannhauser, M.H. Six-month outcomes of a randomized, motivational tele-intervention for change in the codependent behavior of family members of drug users. Subst. Use Misuse 2017, 52, 164–174. [Google Scholar] [CrossRef] [PubMed]
- Faghih, M.; Pahlavanzadeh, S. The effect of cognitive behavioral therapy on the burden in drug dependent persons’ caregivers: A randomized controlled clinical trial. Iran. J. Nurs. Midwifery Res. 2019, 24, 131–136. [Google Scholar]
- Haddock, G.; Barrowclough, C.; Tarrier, N.; Moring, J.; O’Brien, R.; Schofield, N.; Quinn, J.; Palmer, S.; Davies, L.; Lowens, I.; et al. Cognitive-behavioural therapy and motivational intervention for schizophrenia and substance misuse. 18-month outcomes of a randomised controlled trial. Br. J. Psychiatry 2003, 183, 418–426. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.K.; Lee, M. Effectiveness of forgiveness therapy on resilience, self-esteem, and spirituality of wives of alcoholics. J. Korean Acad. Nurs. 2014, 44, 237–247. [Google Scholar] [CrossRef] [Green Version]
- McCrady, B.S.; Wilson, A.D.; Muñoz, R.E.; Fink, B.C.; Fokas, K.; Borders, A. Alcohol-focused behavioral couple therapy. Fam. Process. 2016, 55, 443–459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Epstein, E.E.; McCrady, B.S. Behavioral couples treatment of alcohol and drug use disorders: Current status and innovations. Clin. Psychol. Rev. 1998, 18, 689–711. [Google Scholar] [CrossRef]
- Powers, M.B.; Vedel, E.; Emmelkamp, P.M. Behavioral couples therapy (BCT) for alcohol and drug use disorders: A meta-analysis. Clin. Psychol. Rev. 2008, 28, 952–962. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Excellence. Depression in Adults: Recognition and Management; NICE: London, UK, 2009. [Google Scholar]
- Orford, J. How does the common core to the harm experienced by affected family members vary by relationship, social and cultural factors? Drugs Educ. Prev. Policy 2017, 24, 9–16. [Google Scholar] [CrossRef]


{kind=link}
 | ||||
| Parent/child interventions | Evidence of effect |  | Evidence of no effect/adverse effect |  |
| Behavioural couples’ therapy | Evidence of effect |  | Evidence of no effect/adverse effect |  |
| Systemic family therapy | Evidence of effect |  | Evidence of no effect/adverse effect |  |
| Unilateral family intervention | Evidence of effect |  | Evidence of no effect/adverse effect |  |
| Psychosocial interventions | Evidence of effect |  | Evidence of no effect/adverse effect |  |
| Author, Date, Country | Participants | Intervention | Comparison | Experimental Intervention Outcome | Risk of Bias Summary |
|---|---|---|---|---|---|
| Parent and Child Intervention | |||||
| Parental alcohol use and dependent age children | |||||
| Bennun (1988) UK | n = 12 families; alcohol misusing parents and children; mean age 16 years | Milan systems therapy * | Problem-solving treatment based on social learning theory * | Non-Significant (NS) effect on Marital Adjustment Test (MAT) and Family Satisfaction Rating (FS) at 6 months. | Unclear |
| Lam (2009) USA | n = 30 families; females and their male alcohol misusing partners, with at least one child aged 8–12 years | (1) Parent skills plus BCT (PSBCT); (2) BCT; 24 sessions each | IBT; 24 sessions | PSBCT-improved parental style (Parenting Scale-PS) and both PSBCT and BCT-reduced spousal violence using Timeline Followback Spouse Violence (TLFB-SV) and improved spousal relationship satisfaction on the Dyadic Adjustment Scale (DAS) at 6 and 12 months follow-up. | Low |
| Parental alcohol use and adult children | |||||
| Hansson (2006) Sweden | n = 82; adult children of parents with alcohol problems; mean age 25.6 years; 61% female alcohol | (1) Coping (CBT) only; (2) Coping and alcohol intervention * | Alcohol intervention focusing upon the adult child’s drinking only * | NS on Short Index of Problems (SIP), Symptom Checklist-90 item (SCL-90), Interview Schedule for Social Interaction (ISSI), questionnaire coping with parents’ abuse at 12 months follow-up. | Low |
| Gustafson (2012) USA | n = 23; adult children of alcoholic parents, aged 18 years and older; 63% female | (1) Computer-based intervention only; (2) Computer-based intervention plus group therapy * | Group therapy only * | No significance test conducted due to small sample size. Self-constructed questionnaire measuring responsibility and blame, depression, anxiety, loneliness, personal growth, positive relations, and self-acceptance completed post intervention. | High |
| Kingree (2000) USA | n = 114; adult children of alcoholics, mean age 34.5 years; 32% female | Al-anon (family support groups); 12 meetings | Substance abuse education classes * | Improved perceived status benefits (self-constructed questionnaire) and depression (CES-D) at 6 months post treatment | Unclear |
| Kuhns (1997) USA | n = 64; adult children of alcoholic parents, mean age 20.4 years | (1) Self-help; (2) Psychotherapy; 8 sessions | No intervention | Both self-help and psychotherapy reduced depression on Centre for Epidemiological Studies Depression Scale (CES-D) 3 months post treatment | Unclear |
| Osterndorf (2011) USA | n = 12; adult children of alcoholics, 91.7% female | Forgiveness therapy; 12 sessions | Conflict resolution; 12 sessions | NS on Enright Forgiveness Inventory (EFI); Anxiety on State-Trait Anxiety Inventory (STAI); anger on State-Trait Anger expression Inventory (STAXI); Beck Depression Inventory (BDI-II), Positive Relations with Others (PRO) at 3-month follow-up. | Unclear |
| Parental drug use and dependent age children | |||||
| Catalano (1999); Haggerty (2008) USA | n = 130 families; parents in receipt of methadone; 75% female; child aged 3–14 years | Focus on Families; parent skill training and case management; 33 sessions | Methadone treatment * | Higher parental involvement (self-constructed questionnaire) at 6-month follow-up. Adolescent males less likely to have an alcohol or marijuana use disorder; NS for females (Composite International Diagnostic Interview—CIDI) at 12–14-year follow-up. | Low |
| Hojjat (2016) Iran | n = 57; female children with both parents being dependent upon opium, aged 12–15 years | Group assertiveness training; 8 sessions | Wait-list control | Increased happiness (Oxford Happiness Scale) and assertiveness (Gambrill–Richey Assertion Inventory) one month post intervention. | High |
| Hojjat (2017) Iran | n = 57; male children aged 14–18 years who have an opium dependent father | Emotional intelligence training; 8 sessions | No intervention | Reduced anger (STAXI-(2) at 4-month follow-up. | High |
| Parental alcohol and/or drug use and dependent age children | |||||
| Donohue (2014) | n = 72 substance abusing mothers referred to child welfare for neglect, and their children | Family behavioural therapy * plus standard treatment | Standard treatment * | Significant reductions in child maltreatment potential at 6 and 10 months follow-up. | Low |
| Kelley (2002) USA | n = 135 families; all female partners of substance abusing male, with at least one child aged 6–16 years | (1) BCT; (2) Individual behavioural therapy (IBT); 32 sessions each | Couples based psychoeducational attention control (PACT); 32 sessions | Improved child psychosocial functioning (Pediatric Symptom Checklist—PSC) and relationship satisfaction (DAS) at 6 (in both alcohol and drug using group) and 12 months (drug using group). | Low |
| Orte (2008) Spain | n = 93; children of dependent substance misusing parents; mean age 10.6 years | Family competence programme; 14 sessions | Standard outpatient drug treatment * | Improved family relationships, parental involvement, family communication, family bonds, and family cohesion (Strengthening Families Programme validated instruments) at 3-month follow-up | High |
| Bröning (2019) Germany | n = 218; children of substance misusing parents, aged 8–12 years; 47.7% female; participants excluded if in receipt of additional intervention | Psych-educational intervention; 9 sessions | Non educational play and fun sessions * | NS on coping measures (adapted version Stress and Stress Management in childhood and adolescence—SSKJ); self-efficacy (Generalised Self-Efficacy Scale); self-concept (Self-Perception Profile for Children, child version—SPPC); health-related quality of life (KIDSCREEN-27); self-constructed questionnaires on parent relationship, mental distress, and social isolation at 6-month follow-up. | Low |
| Bartle-Haring (2018) USA | n = 183 families; children of substance-using mothers, mean age 11.54 years | Ecologically based family therapy; 12 sessions | Women’s health education; 12 sessions | Short term immediate decrease (6 months) in alcohol and tobacco followed by an increase (12 and 18 months). NS for cannabis (Timeline Followback—90 item; TLFB-90). | Unclear |
| Behavioural couples and family therapy | |||||
| Interventions for partners/families of an adult who uses alcohol | |||||
| Fals-Stewart (2005) USA | n = 60 dyads; female partners of male alcohol misusers | (1) Brief BCT; 18 sessions; (2) standard BCT; 24 sessions | (1) Couples psychoeducational attention control (PACT); (2) IBT; 18 sessions each | Brief and standard BCT significantly improved relationship satisfaction (DAS); however, brief BCT was not equivalent to standard at 12-month follow-up. | Low |
| Fals-Stewart (2006) USA | n = 138 dyads; male partners of female alcohol misusers | (1) BCT; (2) IBT; 32 sessions each | PACT; 32 sessions | BCT group less acts of violence TLFB-SV and improved relationship (DAS) at 12-month follow-up. | Low |
| Fals-Stewart (2009b) USA | n = 100 dyads; same sex couples where one partner has alcohol use disorder | BCT; 32 sessions | IBT; 32 sessions | Increased relationship satisfaction (DAS) throughout follow-up period (3, 6, 9, and 12 months). | Low |
| Halford (2001) Australia | n = 44 dyads; female partners of alcohol abusing males | (1) Stress management; (2) Alcohol focused couples’ therapy; 15 sessions each | Non-directive counselling; 15 sessions | NS results for stress and burden (Relative Stress Scale and General Health Questionnaire—GHQ); relationship satisfaction (DAS and Martial Status Inventory—MSI); and physical aggression within relationship (Conflict Tactics Scale—CTS) at 6-month follow-up. | High |
| Kuenzler (2003) USA | n= 50 dyads; partners also drank alcohol; 70% above recommended levels | BCT * | Family systems therapy * | NS for partners’ psychological wellbeing as measured by BDI post treatment. | High |
| Lam (2009) USA | n = 30 families; females and their male alcohol misusing partners, with at least one child aged 8–12 years | (1) Parent skills plus BCT (PSBCT); (2) BCT; 24 sessions each | IBT; 24 sessions | Both PSBCT and BCT reduced spousal violence (TLFB-SV) and improved spousal relationship satisfaction (DAS) at 6 and 12 months follow-up. | Low |
| McCrady (1986); McCrady (1991) USA | n = 47 dyads; partners of alcohol abusers | (1) Alcohol-focused couple involvement (AFSI); (2) Alcohol behavioural martial therapy (ABMT) * | Minimal spouse involvement * | Increased relationship satisfaction (MAT) and psychological status (Psychosocial Functioning Inventory) in ABMT at 6 months follow-up. | Low |
| O’Farrell (1985); O’Farrell (1992) USA | n= 34 dyads; female spouses of male alcoholics | (1) Couples attended mutual support group; (2) BCT; 10 sessions each | Individual peer counselling * | BCT significantly higher relationship satisfaction (MAT) and higher martial stability (Martial Stability Inventory—MSI) at 6 and 12 months. | Low |
| O’Farrell (1993); O’Farrell (1997) USA | n = 59 dyads; female partners of male alcoholics | BCT and relapse prevention; 25 sessions | BCT; 10 sessions | Higher relationship satisfaction (MAT) at 12 months effect not found at 18 or 24 months follow-up. | Low |
| O’Farrell (2016) USA | n = 101 dyads; partners of alcohol dependent patients; 29.7% female | Group BCT; 23 sessions | Standard BCT; 23 sessions | Group BCT significantly lower relationship satisfaction (DAS) than standard BCT at 3 and 6 months follow-up. | Low |
| Schumm (2014); USA | n = 105 dyads; male partners of alcohol dependent females | BCT; 26 sessions | IBT; 26 sessions | NS on relationship satisfaction (DAS and Relationship Happiness Scale -RHS) or intimate partner violence (CTS) at 12 months follow-up. | Low |
| Vedel (2008) Netherlands | n = 64 dyads; partners (male and female) of alcohol misusers | BCT; 10 sessions | IBT; 10 sessions | NS on relationship satisfaction (Maudsley Martial Questionnaire) at 6 months follow-up. | Low |
| Walitzer (2004) USA | n = 64 dyads; female partners of problem drinkers | (1) Couples alcohol focused; (2) Couples alcohol focused and BCT; 10 sessions | Individual focused; 10 sessions | NS on relationship satisfaction (DAS) or spouse support measures (Partner Interaction Questionnaire and Significant-other Behaviour Questionnaire) at 6 and 12 months follow-up. | Unclear |
| Walitzer (2013) USA | n = 64 dyads; female partners of problem drinkers | (1) Couples alcohol focused (CAF); (2) CAF and BCT; 10 sessions | Individual focused; 10 sessions | Decrease in conflictual communication in two couple-involved groups (Rapid Martial Interaction Coding System) post treatment. | Low |
| Interventions for partners/families of an adult who uses drugs | |||||
| Fals-Stewart (2001) USA | n = 36 dyads; female partners of men in receipt of methadone | BCT; 24 sessions | IBT; 24 sessions | Increased relationships satisfaction (DAS and MHS) post treatment. | Low |
| O’Farrell (2017) USA | n = 61 dyads; male partners of female drug users; 45% of males were also drug users | BCT; 26 sessions | IBT; 26 sessions | NS on relationship satisfaction (DAS), lower days separated (% of days) at 12 months follow-up. | Low |
| Interventions for partners/families of an adult who uses alcohol and/or drugs | |||||
| Fals-Stewart (2002) USA | n = 80 dyads; female partners of male substance misusers | BCT; 34 sessions | IBT; 22 sessions | Less male to female acts of violence (CTS) at 12 months follow-up. | Low |
| Fals-Stewart (2009a) USA | n = 207 dyads; female partners of substance misusing males | BCT; 32 sessions | IBT; 32 sessions | Lower male to female violence (TLFB-SV) at 12 months follow-up. | Low |
| O’Farrell (2010) USA | n = 29 dyads; family members other than spouses of substance misusing relative | Behavioural family therapy; 24 sessions | IBT; 24 sessions | NS on relationship satisfaction (RHS) at 3 and 6 months follow-up. | Low |
| Winters (2002) USA | n = 75 dyads; male partners of female substance misusers | BCT; mean 39.5 sessions | IBT; mean 38.4 sessions | Increased relationships satisfaction (DAS and RHS) at 12 months follow-up. | Unclear |
| Systemic family therapy | |||||
| Interventions for families of an adult who uses alcohol | |||||
| McKay (1993) USA | n = 51; family of alcohol misusers | Conjoint systemic therapy * | Non conjoint alcohol coping * | NS difference in family functioning as measured on the Family Assessment Device (FAD) at 6 months follow-up. | High |
| Zweben (1988) USA | n = 116 dyads; partners (male and female) of alcohol abusers | Couples martial therapy * | Couples advice counselling * | NS on Revised Martial Relationship Scale (RMRS), DAS, and Edmonds Martial Conventionality Scale (EMC) at 6, 12, and 18 months follow-up. | Low |
| Interventions for families of an adult who uses drugs | |||||
| Ahmad-Abadi (2017) Iran | n = 61; co-dependent partners of drug users | Communication family therapy; 10 sessions | Counselling; 1–3 sessions | Reduced co-dependency as measured on the Holyoake co-dependency index (HCI) at 3 months follow-up. | Unclear |
| Ghasemi (2014) Iran | n = 285; male and female family of methamphetamine users | Family empowerment model * | No intervention | Improved quality of life as measured on the Short Form Health Survey-36 post treatment. | Unclear |
| Li (2014) Vietnam | n = 83; family members of IV drug users; 100% female | Family and user sessions delivered separately; 6 sessions | Standard care * | Improved coping (brief COPE scale) at 3 months only, depression (Zung Self-Rating Depression Scale) at 6-month follow-up only and family functioning (adapted from Family Functioning Scale) at 6 and 12 months. | Low |
| Interventions for families of an adult who uses alcohol and/or drugs | |||||
| Mueser (2012) USA | n = 108; family of dually diagnosed patients | Family intervention * (18-month intervention period) | Education for family * | Improved knowledge (self-reported), mental health (as measured by SF-12), worry, and stigma (Family Experiences Interview Schedule—FEIS) at 36-month follow-up. | Low |
| Unilateral family interventions | |||||
| Interventions for families of an adult who uses alcohol | |||||
| Barber (1995) Australia | n = 23; partners of heavy drinkers; 96% female | (1) Pressures to Change (individual); (2) Pressures to Change (group) * | Wait-list | NS on Martial consensus scale (MCS), Life Satisfaction Scale (LSS), personal problems (self-report) post treatment and 3 months later. | Unclear |
| Barber (1996) Australia | n= 48; mostly partners (daughters and mothers also) of heavy drinkers, 94% female | (1) Pressures to Change (individual); (2) Pressures to Change (group) * | (1) Wait-list; (2) Al-anon (family support group) * | Individual-improved marriage discord-measured Drinkers Partner Distress Scale (DPDS), personal problems (self-report). NS on depression (DPDS) post treatment. | Unclear |
| Barber (1998) Australia | n = 38, female partners of male heavy drinkers | (1) Pressures to Change (individual); (2) Pressures to Change (self-help manual) * | (1) Wait-list control | Individual-improved marriage satisfaction (DPDS), NS on life satisfaction (LSS) only when combined pressures to change groups decreased depression (DPDS) 1 month post treatment. | Unclear |
| Bischof (2016) Germany | n = 78; majority female (97.9%) and partners (79.1%), of alcohol-dependent relatives | CRAFT * | Wait-list control * | Improvements in mental health on Mental Health Inventory but not on BDI or SCL-90. Improvements in and relationship satisfaction (RHS) at 12 months follow-up. | Low |
| Eek (2020) Sweden | n = 94; majority female (92.3%) and partners (86.2%), of mostly alcohol-dependent relatives (94.7%) | iCRAFT; 10–12 weekly sessions | Wait-list control | All mental health outcomes were NS at 12 and 24 weeks follow-up (as measured by Montgomery–Åsberg Depression Rating Scale-Self Assessment (MADRS-S) and Depression, Anxiety and Stress Scale (DASS)). | Unclear |
| Miller (1999) USA | n = 130 family members of alcohol users | (1) CRAFT; 12 sessions; (2) Johnson Institute Intervention; 6 sessions | Al-anon; 12 sessions | All outcomes relating to affected family member were NS (as measured on BDI, State-Trait Anxiety Inventory, STAXI, Spouse Enabling Inventory and Spouse Influence Inventory, self-esteem scale (self-reported) and physical symptoms scale (self-reported) Family Environment Scale (FES), DAS, and (RHS) at 3, 6, 9, and 12 months follow-up. | Low |
| Interventions for families of an adult who uses drugs | |||||
| Kirby (1999) USA | n = 32; family members of drug users; 94.4% female | CRAFT; 14 sessions | Al-anon; 10 sessions | All outcomes relating to affected family member were NS (as measured on Family Impact Survey (FIS), Profile of Mood States (POMS), Social Adjustment Scale, and Self-Esteem Scale) post treatment. | Unclear |
| Psychosocial interventions for the individual affected family member | |||||
| Interventions for families of an adult who uses alcohol | |||||
| Copello (2009); Velleman (2011) UK | n = 136 family members of substance misusers | Stress-strain-coping-support model; 1 session | Self-help manual with similar content | NS on two validated tools measuring physical and psychological coping (Symptom Rating Test and Coping Questionnaire) at 12 months follow-up. | Low |
| Cruz-Almanza (2006) Mexico | n = 35; female partners of alcohol misusing men | Rational-Emotive Behavioural Therapy; 18 sessions | Wait-list control | Increased self-esteem (Self-Esteem Inventory), coping (Birmingham Coping Inventory), and likelihood of assertiveness (Assertion Inventory) at 3, 6, and 18 months follow-up. | High |
| Dittrich (1984) USA | n = 23 wives of alcoholics | Group intervention; 8 sessions (and optional) | Wait-list control | Improved self-concept (Tennessee self-concept scale); decreased anxiety (Taylor Manifest Anxiety Scale) and enabling behaviour Memphis Enabling Behaviors Inventory (MEBI) post treatment and 6 months later. | Unclear |
| Kim (2014) Korea | n = 29; wives of alcoholics | Forgiveness therapy; 12 sessions | Standard care * | Improved resilience and self-esteem at 3-month follow-up. | Low |
| Osilla (2018); Rodriguez (2018); USA | n = 306; partners of heavy drinking service members and veterans; 95% female | Partners Connect (web-based intervention) * | Wait-list control | Lower anxiety (General Anxiety Scale—GAD-7), depression (Patient Health Questionnaire—PHQ-9), and increased social support (Medical Outcome Study survey). NS relationship quality (Quality of Marriage Index—QMI), anger (State-Trait Anger Expression Inventory—STAXI), or family conflict (Family Environment Scale-FES) at 5 months follow-up. | Low |
| Rubio (2013) Spain | n = 188; mainly wives (90.4%) of alcohol misusers | Family self-help; 10 sessions | Standard care | Improvements in somatization, depression, anxiety, and phobia as measured on Symptom Checklist—90 (SCL-90), mental health and social role as measured on short form—36 (SF-36) at 6 months follow-up. | Low |
| Rychtarik (2005) USA | n = 36; female partners of alcohol misusers | (1) Coping skills training (CST); (2) Al-anon * | Wait-list control | CST and Al-anon reduced depression on Beck Depression Inventory (BDI-1A). CTS lower incident of partner violence (self-report) at 12 months follow-up. | Low |
| Zetterlind (2001) Hansson (2004) Sweden | n = 39; partners of alcoholics; 92.3% female | (1) Coping skills (individual) 5 sessions; (2) CBT (group) 13 sessions | Standard information session; 1 session | NS on coping behaviour scale; the SCL-90, global severity index, Alcohol Use Disorder Identification Test (AUDIT) (affected other alc use) at 12 months follow-up. | Low |
| Interventions for families of an adult who uses drugs | |||||
| Bortolon (2017) Brazil | n = 335, 88.7% female; mostly mothers (62%) of drug users | Tele-intervention; 9 telephone sessions | Bibliotherapy | Twice as likely to modify their co-dependent behaviour (Holyoake co-dependency index—HCI) at 6 months follow-up. | Low |
| Faghih (2019) Iran | n = 64; family members of drug dependent relative; 78% female | CBT; 16 sessions | No intervention | Reduced burden of care as measured on Zarit Burden Scale at 3 months follow-up. | Low |
| Interventions for families of an adult who uses alcohol and/or drugs | |||||
| Haddock (2003) UK | n = 36; mostly parents (66.6%) and females (75%) of dually diagnosed relatives | CBT; 29 sessions | Standard care * | NS on physical and mental health (GHQ, BDI), Social Behaviour Assessment Schedule (SBAS), and Relatives Cardinal Needs Schedule (RCNS) at 12 months follow-up. | Low |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
McGovern, R.; Smart, D.; Alderson, H.; Araújo-Soares, V.; Brown, J.; Buykx, P.; Evans, V.; Fleming, K.; Hickman, M.; Macleod, J.; et al. Psychosocial Interventions to Improve Psychological, Social and Physical Wellbeing in Family Members Affected by an Adult Relative’s Substance Use: A Systematic Search and Review of the Evidence. Int. J. Environ. Res. Public Health 2021, 18, 1793. https://doi.org/10.3390/ijerph18041793
McGovern R, Smart D, Alderson H, Araújo-Soares V, Brown J, Buykx P, Evans V, Fleming K, Hickman M, Macleod J, et al. Psychosocial Interventions to Improve Psychological, Social and Physical Wellbeing in Family Members Affected by an Adult Relative’s Substance Use: A Systematic Search and Review of the Evidence. International Journal of Environmental Research and Public Health. 2021; 18(4):1793. https://doi.org/10.3390/ijerph18041793
Chicago/Turabian StyleMcGovern, Ruth, Debbie Smart, Hayley Alderson, Vera Araújo-Soares, Jamie Brown, Penny Buykx, Vivienne Evans, Kate Fleming, Matt Hickman, John Macleod, and et al. 2021. "Psychosocial Interventions to Improve Psychological, Social and Physical Wellbeing in Family Members Affected by an Adult Relative’s Substance Use: A Systematic Search and Review of the Evidence" International Journal of Environmental Research and Public Health 18, no. 4: 1793. https://doi.org/10.3390/ijerph18041793
APA StyleMcGovern, R., Smart, D., Alderson, H., Araújo-Soares, V., Brown, J., Buykx, P., Evans, V., Fleming, K., Hickman, M., Macleod, J., Meier, P., & Kaner, E. (2021). Psychosocial Interventions to Improve Psychological, Social and Physical Wellbeing in Family Members Affected by an Adult Relative’s Substance Use: A Systematic Search and Review of the Evidence. International Journal of Environmental Research and Public Health, 18(4), 1793. https://doi.org/10.3390/ijerph18041793