
Development of the “National Asbestos Profile” to Eliminate Asbestos-Related Diseases in 195 Countries

 , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Country | Reference |
|---|---|
| Australia | Asbestos Safety and Eradiation Agency. 2017. National Asbestos Profile for Australia. Available online: https://www.asbestossafety.gov.au/sites/default/files/documents/2017-12/ASEA_National_Asbestos_Profile_interactive_Nov17.pdf (accessed on 11 January 2021). [26] |
| Bangladesh | Bangladesh Occupational Safety, Health and Environment Foundation. 2016. National Asbestos Profile of Bangladesh. Obtained via personal communication: 20 April 2020. [27] |
| Bulgaria | Vangelova, K.; Dimitrova, S.; Dimitrova, I. 2015. National Asbestos Profile of Bulgaria. Available online: https://ncpha.government.bg/files/National%20Asbestos%20Profile_Bulgaria_2015-en.pdf (accessed on 11 January 2021). [28] |
| Cambodia | Ministry of Labor and Vocational Training. 2019. Cambodia National Asbestos Profile. Personal Communication, 2020. [29] |
| Germany | Federal Institute for Occupational Health and Safety. 2014. National Asbestos Profile for Germany. Available online: https://www.baua.de/EN/Service/Publications/Report/Gd80.pdf?__blob=publicationFile&v=8 (accessed on 11 January 2021). [30] |
| India | People’s Training & Research and Centre. 2017. India: National Asbestos Profile. Available online: https://amrc.org.hk/sites/default/files/NAP%20India.pdf (accessed on 11 January 2021). [31] |
| Indonesia | Indonesia Ban Asbestos Network. 2017. National Asbestos Profile Indonesia. Obtained via personal communication: 28 April 2020. [32] |
| Japan | Furuya, S.; Takahashi, K.; Mohaved, M.; Jiang, Y. 2013. National Asbestos Profile of Japan. Available online: https://www.researchgate.net/publication/237839114_National_Asbestos_Profile_of_Japan_-_Based_on_the_National_Asbestos_Profile_by_the_ILO_and_the_WHO (accessed on 11 January 2021) [33] |
| Laos | Laos Ministry of Industry and Commerce. 2017. National Asbestos Profile of Laos. Personal Communication, 2020. [34] |
| North Macedonia | Institute of Occupational Health of the Republic of Macedonia. 2014. National Asbestos Profile for the Republic of Macedonia. Personal Communication, 2020. [35] |
| Mongolia | Health Sciences University of Mongolia. 2012. National Asbestos Profile of Mongolia. Personal Communication, 2020. [36] |
| Nepal | Sah, R.C. 2016. National Asbestos Profile of Nepal. Available online: http://anroev.org/aban/wp-content/uploads/2016/10/National-Abestos-Profile-of-Nepal.pdf (accessed on 11 January 2021). [37] |
| Philippines | Republic of Philippines, Environmental and Occupational Health Office. 2013. National Asbestos Profile Philippines. Available online: https://www.informea.org/en/national-asbestos-profile-nap-philippines (accessed on 11 January 2021). [38] |
| Vietnam | Pham, V.H.; Tran, T.N.L.; Le, G.V.; Movahed, M.; Jiang, Y.; Pham, N.H.; Ogawa, H; Takahashi, K. Asbestos and asbestos-related diseases in Vietnam: In reference to the International Labor Organization/World Health Organization National Asbestos Profile. Saf. Health Work. 2013, 4, 117–121. doi:10.1016/j.shaw.2013.04.002. [39] |
| Asbestos Data | Disease Data | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Countries 1 | World Bank Income Group 2 | Asbestos Ban Status 3 | NAP Country Category 4 | Consumption of Raw Asbestos (USGS) 5 | Asbestos-Containing Material (UN Comtrade) 6 | Reported Mortality of Mesothelioma or Asbestosis (WHO MDB) 7 | Estimated Incidence of Mesothelioma (GBD) 8 | Estimated Mortality of Mesothelioma (WHO GHE) 9 | Reported or estimated Mortality of Mesothelioma (WHO GCO) 10 | |
| 1 | Afghanistan | LI | No-Ban | C | Yes | No | No | Yes | Yes | Yes |
| 2 | Albania | UMI | No-Ban | C | Yes | Yes | No | Yes | Yes | Yes |
| 3 | Algeria | LMI | Ban | C | Yes | Yes | No | Yes | Yes | Yes |
| 4 | Andorra | HI | No-Ban | C | No | Yes | No | Yes | No | No |
| 5 | Angola | LMI | No-Ban | D | Yes | Yes | No | Yes | Yes | Yes |
| 6 | Antigua and Barbuda | HI | No-Ban | D | Yes | Yes | No | Yes | No | No |
| 7 | Argentina | UMI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 8 | Armenia | UMI | No-Ban | D | Yes | Yes | Yes | Yes | Yes | Yes |
| 9 | Australia | HI | Ban | A | Yes | Yes | Yes | Yes | Yes | Yes |
| 10 | Austria | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 11 | Azerbaijan | UMI | No-Ban | C | Yes | Yes | No | Yes | Yes | Yes |
| 12 | Bahamas | HI | No-Ban | C | Yes | Yes | Yes | No | Yes | No |
| 13 | Bahrain | HI | Ban | B | No | Yes | Yes | Yes | Yes | Yes |
| 14 | Bangladesh | LMI | No-Ban | A | Yes | Yes | No | Yes | Yes | Yes |
| 15 | Barbados | HI | No-Ban | B | Yes | Yes | Yes | Yes | Yes | No |
| 16 | Belarus | UMI | No-Ban | D | Yes | Yes | No | Yes | Yes | Yes |
| 17 | Belgium | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 18 | Belize | UMI | No-Ban | D | Yes | Yes | Yes | Yes | Yes | No |
| 19 | Benin | LMI | No-Ban | D | Yes | Yes | No | Yes | Yes | Yes |
| 20 | Bhutan | LMI | No-Ban | C | Yes | Yes | No | Yes | Yes | No |
| 21 | Bolivia | LMI | No-Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 22 | Bosnia and Herzegovina | UMI | No-Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 23 | Botswana | UMI | No-Ban | C | Yes | Yes | No | Yes | Yes | No |
| 24 | Brazil | UMI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 25 | Brunei | HI | Ban | C | Yes | Yes | No | Yes | Yes | No |
| 26 | Bulgaria | UMI | Ban | A | Yes | Yes | Yes | Yes | Yes | Yes |
| 27 | Burkina Faso | LI | No-Ban | D | No | Yes | No | Yes | Yes | Yes |
| 28 | Burundi | LI | No-Ban | D | Yes | Yes | No | Yes | Yes | Yes |
| 29 | Cambodia | LMI | No-Ban | A | Yes | Yes | No | Yes | Yes | Yes |
| 30 | Cameroon | LMI | No-Ban | D | Yes | Yes | No | Yes | Yes | No |
| 31 | Canada | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 32 | Cape Verde | LMI | No-Ban | C | No | Yes | No | Yes | Yes | No |
| 33 | Central African Republic | LI | No-Ban | D | No | Yes | No | Yes | Yes | No |
| 34 | Chad | LI | No-Ban | C | Yes | No | No | Yes | Yes | No |
| 35 | Chile | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 36 | China | UMI | No-Ban | B | Yes | Yes | No | Yes | Yes | Yes |
| 37 | Colombia | UMI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 38 | Comoros | LMI | No-Ban | D | No | Yes | No | Yes | Yes | No |
| 39 | Congo–Brazzaville | LMI | No-Ban | D | Yes | Yes | No | Yes | Yes | Yes |
| 40 | Congo–Kinshasa (DR Congo) | LI | No-Ban | C | Yes | No | No | Yes | No | Yes |
| 41 | Costa Rica | UMI | No-Ban | B | Yes | Yes | Yes | Yes | Yes | No |
| 42 | Côte d’Ivoire | LMI | No-Ban | C | Yes | Yes | No | Yes | Yes | Yes |
| 43 | Croatia | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 44 | Cuba | UMI | No-Ban | C | Yes | Yes | Yes | Yes | Yes | Yes |
| 45 | Cyprus | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 46 | Czech Republic | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 47 | Denmark | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 48 | Djibouti | LMI | Ban | C | Yes | No | No | Yes | Yes | No |
| 49 | Dominica | UMI | No-Ban | D | Yes | Yes | No | Yes | Yes | No |
| 50 | Dominican Republic | UMI | No-Ban | D | Yes | Yes | Yes | Yes | Yes | Yes |
| 51 | Ecuador | UMI | No-Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 52 | Egypt | LMI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 53 | El Salvador | LMI | No-Ban | D | Yes | Yes | Yes | Yes | Yes | No |
| 54 | Equatorial Guinea | UMI | No-Ban | D | No | No | No | Yes | Yes | No |
| 55 | Eritrea | LI | No-Ban | D | Yes | No | No | Yes | Yes | Yes |
| 56 | Estonia | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 57 | Eswatini Swaziland | LMI | No-Ban | C | Yes | Yes | No | Yes | Yes | No |
| 58 | Ethiopia | LI | No-Ban | C | Yes | Yes | No | Yes | Yes | Yes |
| 59 | Fiji | UMI | No-Ban | B | Yes | Yes | Yes | Yes | No | No |
| 60 | Finland | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 61 | France | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 62 | Gabon | UMI | Ban | C | Yes | Yes | No | Yes | Yes | No |
| 63 | Gambia | LI | No-Ban | C | No | Yes | No | Yes | Yes | No |
| 64 | Georgia | UMI | No-Ban | C | Yes | Yes | Yes | Yes | Yes | Yes |
| 65 | Germany | HI | Ban | A | Yes | Yes | Yes | Yes | Yes | Yes |
| 66 | Ghana | LMI | No-Ban | B | Yes | Yes | No | Yes | Yes | Yes |
| 67 | Greece | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 68 | Grenada | UMI | No-Ban | C | No | Yes | Yes | Yes | No | No |
| 69 | Guatemala | UMI | No-Ban | C | Yes | Yes | Yes | Yes | Yes | No |
| 70 | Guinea | LI | No-Ban | D | Yes | Yes | No | Yes | Yes | No |
| 71 | Guinea-Bissau | LI | No-Ban | D | No | Yes | No | Yes | Yes | No |
| 72 | Guyana | UMI | No-Ban | C | Yes | Yes | Yes | Yes | Yes | No |
| 73 | Haiti | LI | No-Ban | C | Yes | No | No | Yes | Yes | Yes |
| 74 | Honduras | LMI | Ban | C | Yes | Yes | No | Yes | Yes | Yes |
| 75 | Hong Kong 1 | HI | No-Ban | B | Yes | Yes | Yes | No | No | No |
| 76 | Hungary | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 77 | Iceland | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 78 | India | LMI | No-Ban | A | Yes | Yes | No | Yes | Yes | Yes |
| 79 | Indonesia | UMI | No-Ban | A | Yes | Yes | No | Yes | Yes | Yes |
| 80 | Iran | UMI | No-Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 81 | Iraq | UMI | Ban | B | Yes | No | Yes | Yes | Yes | Yes |
| 82 | Ireland | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 83 | Israel | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 84 | Italy | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 85 | Jamaica | UMI | No-Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 86 | Japan | HI | Ban | A | Yes | Yes | Yes | Yes | Yes | Yes |
| 87 | Jordan | UMI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 88 | Kazakhstan | UMI | No-Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 89 | Kenya | LMI | No-Ban | B | Yes | Yes | No | Yes | Yes | Yes |
| 90 | Kiribati | LMI | No-Ban | B | No | Yes | No | Yes | Yes | No |
| 91 | Kuwait | HI | Ban | C | Yes | Yes | Yes | Yes | Yes | Yes |
| 92 | Kyrgyzstan | LMI | No-Ban | D | Yes | Yes | Yes | Yes | Yes | Yes |
| 93 | Laos | LMI | No-Ban | A | Yes | Yes | No | Yes | Yes | Yes |
| 94 | Latvia | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 95 | Lebanon | UMI | No-Ban | B | Yes | Yes | No | Yes | Yes | Yes |
| 96 | Lesotho | LMI | No-Ban | B | No | Yes | No | Yes | Yes | Yes |
| 97 | Liberia | LI | No-Ban | B | Yes | No | No | Yes | Yes | Yes |
| 98 | Libya | UMI | No-Ban | B | Yes | Yes | No | Yes | Yes | Yes |
| 99 | Liechtenstein | HI | Ban | B | No | No | No | No | No | No |
| 100 | Lithuania | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 101 | Luxembourg | HI | Ban | C | Yes | Yes | Yes | Yes | Yes | Yes |
| 102 | Madagascar | LI | No-Ban | C | Yes | Yes | No | Yes | Yes | Yes |
| 103 | Malawi | LI | No-Ban | C | Yes | Yes | No | Yes | Yes | No |
| 104 | Malaysia | UMI | No-Ban | B | Yes | Yes | No | Yes | Yes | Yes |
| 105 | Maldives | UMI | No-Ban | C | Yes | Yes | Yes | Yes | Yes | No |
| 106 | Mali | LI | No-Ban | D | Yes | Yes | No | Yes | Yes | Yes |
| 107 | Malta | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 108 | Marshall Islands | UMI | No-Ban | B | No | No | No | Yes | No | No |
| 109 | Mauritania | LMI | No-Ban | D | No | Yes | No | Yes | Yes | No |
| 110 | Mauritius | HI | Ban | B | Yes | Yes | Yes | Yes | No | No |
| 111 | Mexico | UMI | No-Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 112 | Micronesia | LMI | No-Ban | B | No | Yes | No | Yes | Yes | No |
| 113 | Moldova | LMI | No-Ban | C | Yes | Yes | Yes | Yes | Yes | Yes |
| 114 | Monaco | HI | Ban | B | No | No | No | No | No | No |
| 115 | Mongolia | LMI | No-Ban | A | Yes | Yes | Yes | Yes | Yes | Yes |
| 116 | Montenegro | UMI | No-Ban | C | Yes | Yes | Yes | Yes | Yes | No |
| 117 | Morocco | LMI | No-Ban | C | Yes | Yes | Yes | Yes | Yes | Yes |
| 118 | Mozambique | LI | Ban | B | Yes | Yes | No | Yes | Yes | Yes |
| 119 | Myanmar | LMI | No-Ban | D | Yes | Yes | No | Yes | Yes | Yes |
| 120 | Namibia | UMI | No-Ban | C | Yes | Yes | No | Yes | Yes | Yes |
| 121 | Nauru | HI | No-Ban | B | No | No | No | No | No | No |
| 122 | Nepal | LMI | No-Ban | A | Yes | Yes | No | Yes | Yes | Yes |
| 123 | Netherlands | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 124 | New Zealand | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 125 | Nicaragua | LMI | No-Ban | D | Yes | Yes | Yes | Yes | Yes | Yes |
| 126 | Niger | LI | No-Ban | D | Yes | Yes | No | Yes | Yes | No |
| 127 | Nigeria | LMI | No-Ban | B | Yes | Yes | No | Yes | Yes | Yes |
| 128 | North Korea | LI | No-Ban | D | Yes | No | No | Yes | Yes | Yes |
| 129 | North Macedonia | UMI | Ban | A | Yes | Yes | Yes | Yes | Yes | No |
| 130 | Norway | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 131 | Oman | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 132 | Pakistan | LMI | No-Ban | B | Yes | Yes | No | Yes | Yes | Yes |
| 133 | Palau | HI | No-Ban | B | No | Yes | No | No | No | No |
| 134 | Panama | HI | No-Ban | C | Yes | Yes | Yes | Yes | Yes | Yes |
| 135 | Papua New Guinea | LMI | No-Ban | C | No | Yes | No | Yes | Yes | Yes |
| 136 | Paraguay | UMI | No-Ban | C | Yes | Yes | Yes | Yes | Yes | No |
| 137 | Peru | UMI | No-Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 138 | Philippines | LMI | No-Ban | A | Yes | Yes | Yes | Yes | Yes | Yes |
| 139 | Poland | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 140 | Portugal | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 141 | Qatar | HI | Ban | B | Yes | Yes | No | Yes | Yes | Yes |
| 142 | Romania | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 143 | Russia | UMI | No-Ban | B | Yes | Yes | No | Yes | Yes | Yes |
| 144 | Rwanda | LI | No-Ban | B | Yes | Yes | No | Yes | Yes | Yes |
| 145 | Saint Kitts and Nevis | HI | No-Ban | C | No | Yes | No | No | No | No |
| 146 | Saint Lucia | UMI | No-Ban | C | No | Yes | Yes | Yes | Yes | No |
| 147 | Saint Vincent and Grenadines | UMI | No-Ban | D | Yes | Yes | No | Yes | No | No |
| 148 | Samoa | UMI | No-Ban | B | Yes | Yes | No | Yes | Yes | No |
| 149 | San Marino | HI | No-Ban | B | No | Yes | No | No | No | No |
| 150 | São Tomé and Príncipe | LMI | No-Ban | C | No | Yes | No | Yes | Yes | No |
| 151 | Saudi Arabia | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 152 | Senegal | LMI | No-Ban | C | Yes | Yes | No | Yes | Yes | Yes |
| 153 | Serbia | UMI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 154 | Seychelles | HI | Ban | C | Yes | Yes | No | Yes | Yes | No |
| 155 | Sierra Leone | LI | No-Ban | D | Yes | Yes | No | Yes | Yes | No |
| 156 | Singapore | HI | No-Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 157 | Slovakia | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 158 | Slovenia | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 159 | Solomon Islands | LMI | No-Ban | B | No | Yes | No | Yes | Yes | No |
| 160 | Somalia | LI | No-Ban | D | No | No | No | Yes | Yes | Yes |
| 161 | South Africa | UMI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 162 | South Korea | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 163 | South Sudan | LI | No-Ban | B | No | Yes | No | Yes | Yes | Yes |
| 164 | Spain | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 165 | Sri Lanka | LMI | No-Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 166 | Sudan | LI | No-Ban | C | Yes | Yes | No | Yes | Yes | Yes |
| 167 | Suriname | UMI | No-Ban | D | Yes | Yes | Yes | Yes | Yes | No |
| 168 | Sweden | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 169 | Switzerland | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 170 | Syria | LI | No-Ban | C | Yes | Yes | No | Yes | Yes | Yes |
| 171 | Taiwan 1 | HI | Ban | B | Yes | No | No | Yes | No | No |
| 172 | Tajikistan | LI | No-Ban | B | Yes | Yes | No | Yes | Yes | No |
| 173 | Tanzania | LMI | No-Ban | C | Yes | Yes | No | Yes | Yes | No |
| 174 | Thailand | UMI | No-Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 175 | Timor-Leste | LMI | No-Ban | B | No | Yes | No | Yes | Yes | No |
| 176 | Togo | LI | No-Ban | C | Yes | Yes | No | Yes | Yes | Yes |
| 177 | Tonga | UMI | No-Ban | B | No | Yes | No | Yes | Yes | No |
| 178 | Trinidad and Tobago | HI | No-Ban | C | Yes | Yes | Yes | Yes | Yes | No |
| 179 | Tunisia | LMI | No-Ban | C | Yes | Yes | Yes | Yes | Yes | Yes |
| 180 | Turkey | UMI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 181 | Turkmenistan | UMI | No-Ban | D | Yes | Yes | No | Yes | Yes | Yes |
| 182 | Tuvalu | UMI | No-Ban | B | No | Yes | No | No | No | No |
| 183 | Uganda | LI | No-Ban | B | Yes | Yes | No | Yes | Yes | Yes |
| 184 | Ukraine | LMI | No-Ban | B | Yes | Yes | No | Yes | Yes | Yes |
| 185 | United Arab Emirates | HI | No-Ban | B | Yes | Yes | No | Yes | Yes | Yes |
| 186 | United Kingdom | HI | Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 187 | United States of America | HI | No-Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 188 | Uruguay | HI | Ban | C | Yes | Yes | Yes | Yes | Yes | Yes |
| 189 | Uzbekistan | LMI | No-Ban | C | Yes | Yes | Yes | Yes | Yes | Yes |
| 190 | Vanuatu | LMI | No-Ban | B | Yes | Yes | No | Yes | Yes | No |
| 191 | Venezuela | UMI | No-Ban | B | Yes | Yes | Yes | Yes | Yes | Yes |
| 192 | Vietnam | LMI | No-Ban | A | Yes | Yes | No | Yes | Yes | Yes |
| 193 | Yemen | LI | No-Ban | D | Yes | Yes | No | Yes | Yes | Yes |
| 194 | Zambia | LMI | No-Ban | C | Yes | Yes | No | Yes | Yes | Yes |
| 195 | Zimbabwe | LMI | No-Ban | B | Yes | Yes | No | Yes | Yes | Yes |
| Total (Yes) | 165 | 179 | 96 | 186 | 178 | 134 | ||||
| Theme | Items of National Asbestos Profile | International Sources | National Sources, etc. | |||||
|---|---|---|---|---|---|---|---|---|
| Asbestos Data | Disease Data | |||||||
| Consumption of Raw Asbestos (USGS 1) | Asbestos-Containing Material (UN Comtrade 2) | Reported Mortality of Mesothelioma or Asbestosis (WHO MDB 3) | Estimated Incidence of Mesothelioma (GBD 4) | Estimated Mortality of Mesothelioma (WHO GHE 5) | Reported or estimated Mortality of Mesothelioma (WHO GCO 6) | |||
| Legislation | I-1. Current regulations on the different forms of asbestos I-15. National enforceable occupational exposure limits for chrysotile asbestos I-16. The system for inspection and enforcement of the exposure limits | I-1, I-15, I-16: Existing government laws and regulations | ||||||
| Asbestos | I-2. Import and consumption of asbestos per year (total and per major uses and forms) I-3. Import of asbestos-containing materials I-4. Domestic production of asbestos (if applicable) I-5. Domestic production of asbestos-containing materials | I-2, I-4 | I-3, I-5 | I-2, I-3: National trade statistics; I-4: National mining statistics; I-5: National manufacturing statistics | ||||
| Diseases | I-9. Estimate of the burden of diseases related to asbestos: disability adjusted life years and deaths attributable to asbestos exposure I-10. Prevalence of asbestosis – national data, a breakdown by industries if available I-11. Incidence of lung cancer among workers exposed to asbestos I-12. Incidence of mesothelioma I-17. Estimated economic losses due to asbestos-related diseases I-18. Major studies on epidemiology of asbestos-related diseases in the country | I-9 (reported deaths) | I-9, I-10, I-11, I-12 deaths, DALY) | I-9, I-12 (estimated | I-9, I-12 (reported a/o estimated deaths) | I-10: National compensation statistics; I-12: National/Regional Cancer Registry data; I-18: PUBMED | ||
| Risk Assessment | I-6. Estimated total number of workers exposed to asbestos in the country I-7. Full list of industries where exposure to asbestos is present in the country and list of industries with the largest numbers of workers potentially exposed to asbestos I-8. Industries with high risk of exposure (where overexposure is documented as exceeding occupational exposure limits) and estimated total number of workers at high risk I-13. Estimates on the percentage of house stock and vehicle fleet containing asbestos I-14. Total number of workers eligible for compensation for asbestos-related diseases, such as asbestosis, lung cancer and mesothelioma (per year) and the numbers of individuals compensated yearly | I-6, I-8: Industrial hygiene or occupational health data; I-7, I-13: Specific industry inventory; I-14: Occupational disease compensation data. | ||||||
References
- Institute for Health Metrics and Evaluation, Global Health Data Exchange. Global Burden of Disease Data. 2018. Available online: http://ghdx.healthdata.org/gbd-results-tool (accessed on 15 January 2021).
- World Health Organization. Elimination of Asbestos-Related Diseases. 2006. Available online: https://www.who.int/occupational_health/publications/asbestosrelateddiseases.pdf (accessed on 15 January 2021).
- International Labor Organization and World Health Organization. Outline for the Development of National Programs for Elimination of Asbestos-Related Diseases. 2007. Available online: https://www.who.int/occupational_health/publications/elim_asbestos_doc_en.pdf?ua=1 (accessed on 15 January 2021).
- International Labor Organization. Thirteenth Session of the Joint ILO/WHO Committee on Occupational Health. 2003. Available online: https://www.ilo.org/wcmsp5/groups/public/---ed_protect/---protrav/---safework/documents/publication/wcms_110478.pdf (accessed on 15 January 2021).
- Kazan-Allen, L. Current Asbestos Bans. 2019. Available online: http://www.ibasecretariat.org/alpha_ban_list.php (accessed on 15 January 2021).
- Takahashi, K.; Landrigan, P.J.; Ramazzini, C. The global health dimensions of asbestos and asbestos-related diseases. Ann. Glob. Health 2016, 82, 209–213. [Google Scholar] [CrossRef] [PubMed]
- Park, E.K.; Takahashi, K.; Hoshuyama, T.; Cheng, T.J.; Delgermaa, V.; Le, G.V.; Sorahan, T. Global magnitude of reported and unreported mesothelioma. Environ. Health Persp. 2011, 119, 514–518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, R.T.; Takahashi, K.; Karjalainen, A.; Hoshuyama, T.; Wilson, D.; Kameda, T.; Chan, C.C.; Wen, C.P.; Furuya, S.; Higashi, T.; et al. Ecological association between asbestos-related diseases and historical asbestos consumption: An international analysis. Lancet 2007, 369, 844–849. [Google Scholar] [CrossRef]
- Delgermaa, V.; Takahashi, K.; Park, E.K.; Le, G.V.; Hara, T.; Sorahan, T. Global mesothelioma deaths reported to the World Health Organization between 1994 and 2008. Bull. World Health Organ. 2011. [Google Scholar] [CrossRef] [PubMed]
- Chimed-Ochir, O.; Takahashi, K.; Sorahan, T.; Driscoll, T.; Fitzmaurice, C.; Yoko-o, M.; Sawanyawisuth, K.; Furuya, S.; Tanaka, F.; Horie, S.; et al. Estimation of the global burden of mesothelioma deaths from incomplete national mortality data. Occup. Environ. Med. 2017, 89, 716–724. [Google Scholar] [CrossRef] [Green Version]
- GBD 2016 Occupational Carcinogens Collaborators. Global and Regional Burden of Cancer in 2016 Arising from Occupational Exposure to Selected Carcinogens: A Systematic Analysis for the Global Burden of Disease Study 2016. Occup. Environ. Med. 2020, 77, 151–159. [Google Scholar] [CrossRef] [PubMed]
- Carbone, M.; Adusumilli, P.S.; Alexander, H.R., Jr.; Baas, P.; Bardelli, F.; Bononi, A.; Bueno, R.; Felley-Bosco, E.; Galateau-Salle, F.; Jablons, D.; et al. Mesothelioma: Scientific clues for prevention, diagnosis, and therapy. Cancer J. Clin. 2019, 69, 402–429. [Google Scholar] [CrossRef] [Green Version]
- United Nations. List of Member States. 2019. Available online: https://www.un.org/en/member-states/index.html (accessed on 15 January 2021).
- World Bank. World Bank Country and Lending Groups. Fiscal Year. 2021. Available online: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups (accessed on 15 January 2021).
- World Health Organization. List of WHO Member States. 2019. Available online: https://www.who.int/choice/demography/by_country/en/ (accessed on 15 January 2021).
- United States Geological Survey. Asbestos Statistics and Information, Minerals Yearbook 1920–2017 (Personal Communication Included). Available online: https://www.usgs.gov/centers/nmic/asbestos-statistics-and-information (accessed on 15 January 2021).
- United Nations Statistics Division. United Nations International Trade Statistics Database, UN Comtrade. Available online: https://comtrade.un.org/data/ (accessed on 15 January 2021).
- World Health Organization. WHO Mortality Database. 2019. Available online: https://www.who.int/data/data-collection-tools/who-mortality-database (accessed on 15 January 2021).
- World Health Organization. Global Health Estimates 2016: Deaths by Cause, Age, Sex, by Country and by Region, 2000–2016. Available online: https://www.who.int/healthinfo/global_burden_disease/en/ (accessed on 15 January 2021).
- World Health Organization. Global Cancer Observatory: Cancer Today. 2018. Available online: https://gco.iarc.fr/today (accessed on 15 January 2021).
- Wolff, H.; Vehmas, T.; Oksa, P.; Rantanen, J.; Vainio, H. Consensus Report: Asbestos, asbestosis, and cancer, the Helsinki criteria for diagnosis and attribution. Scand. J. Work. Environ. Health 2015, 41, 5–15. [Google Scholar] [CrossRef] [PubMed]
- Kameda, T.; Takahashi, K.; Kim, R.; Jiang, Y.; Movahed, M.; Park, E.K.; Rantanen, J. Asbestos: Use, bans and disease burden in Europe. Bull. World Health Organ. 2014, 92, 790–797. [Google Scholar] [CrossRef]
- Le, G.V.; Takahashi, K.; Park, E.K.; Delgermaa, V.; Oak, C.; Qureshi, A.M.; Aljunid, S.M. Asbestos use and asbestos-related diseases in Asia: Past, present and future. Respirology 2011, 16, 767–775. [Google Scholar] [CrossRef]
- World Health Organization Regional Office for Europe. Parma Declaration on Environment and Health. 2010. Available online: http://www.euro.who.int/__data/assets/pdf_file/0011/78608/E93618.pdf (accessed on 15 January 2021).
- National Institute for Occupational Safety and Health. Improving Workers’ Health across the Globe. 2016. Available online: https://www.cdc.gov/niosh/docs/2016-118/pdfs/success-stories_v01_nr04_n-compressed.pdf (accessed on 15 January 2021).
- Asbestos Safety and Eradiation Agency. National Asbestos Profile for Australia. 2017. Available online: https://www.asbestossafety.gov.au/sites/default/files/documents/2017-12/ASEA_National_Asbestos_Profile_interactive_Nov17.pdf (accessed on 11 January 2021).
- Bangladesh Occupational Safety, Health and Environment Foundation. 2016. National Asbestos Profile of Bangladesh. Per-sonal Communication. 2020.
- Vangelova, K.; Dimitrova, S.; Dimitrova, I. National Asbestos Profile of Bulgaria. 2015. Available online: https://ncpha.government.bg/files/National%20Asbestos%20Profile_Bulgaria_2015-en.pdf (accessed on 11 January 2021).
- Ministry of Labor and Vocational Training. 2019. Cambodia National Asbestos Profile. Obtained via personal communication: 04 May 2020.
- Federal Institute for Occupational Health and Safety. National Asbestos Profile for Germany. 2014. Available online: https://www.baua.de/EN/Service/Publications/Report/Gd80.pdf?__blob=publicationFile&v=8 (accessed on 11 January 2021).
- People’s Training & Research and Centre. India: National Asbestos Profile. 2017. Available online: https://amrc.org.hk/sites/default/files/NAP%20India.pdf (accessed on 11 January 2021).
- Indonesia Ban Asbestos Network. 2017. National Asbestos Profile Indonesia. Personal Communication, 2020.
- Furuya, S.; Takahashi, K.; Mohaved, M.; Jiang, Y. National Asbestos Profile of Japan. 2013. Available online: https://www.researchgate.net/publication/237839114_National_Asbestos_Profile_of_Japan_-_Based_on_the_National_Asbestos_Profile_by_the_ILO_and_the_WHO (accessed on 11 January 2021).
- Laos Ministry of Industry and Commerce. 2017. National Asbestos Profile of Laos. Personal Communication, 2020.
- Institute of Occupational Health of the Republic of Macedonia. 2014. National Asbestos Profile for the Republic of Macedonia. Obtained via personal communication: 15 July 2020.
- Health Sciences University of Mongolia. 2012. National Asbestos Profile of Mongolia. Personal Communication. 2020.
- Sah, R.C. National Asbestos Profile of Nepal. 2016. Available online: http://anroev.org/aban/wp-content/uploads/2016/10/National-Abestos-Profile-of-Nepal.pdf (accessed on 11 January 2021).
- Republic of Philippines, Environmental and Occupational Health Office. National Asbestos Profile Philippines. 2013. Available online: https://www.informea.org/en/national-asbestos-profile-nap-philippines (accessed on 11 January 2021).
- Pham, V.H.; Tran, T.N.L.; Le, G.V.; Movahed, M.; Jiang, Y.; Pham, N.H.; Ogawa, H.; Takahashi, K. Asbestos and asbestos-related diseases in Vietnam: In reference to the International Labor Organization/World Health Organization National Asbestos Profile. Saf. Health Work 2013, 4, 117–121. [Google Scholar] [CrossRef] [PubMed] [Green Version]

| Country Category | Document Category | Document Description |
|---|---|---|
| A | “bona fide NAP” | a single document that describes the national situation of asbestos and asbestos-related diseases (ARDs) in adherence to the NAP format published by the WHO/ILO3 |
| B | “proxy NAP” | a single document or multiple documents that describe the national situation of asbestos and ARDs but does (do) not satisfy the criterion for a bona fide NAP; * includes government statements and/or decrees, scientific articles and third-party organization reports |
| C | “relevant published information” | information that does not satisfy the criteria for a bona fide or proxy NAP but refers to asbestos and/or ARDs; includes online information on asbestos as part of wider occupational health and safety policies, toxic chemical waste management policies, ARD case studies and media releases on asbestos and/or ARDs |
| D | “no relevant information” | status that lacked any of the above |
| Country Category | Number of Countries | Income Category 1 | Region | Status of Asbestos Ban | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| HI | UMI | LMI | LI | Western Pacific | South East Asia | Europe | Americas | Africa | East Mediterranean | Banned | No-Ban | ||
| A: Countries that have bona fide NAP 2 | 14 | 3 | 3 | 8 | 0 | 7 | 4 | 3 | 0 | 0 | 0 | 5 | 9 |
| (7%) | (5%) | (6%) | (16%) | (0%) | (28%) | (36%) | (6%) | (0%) | (0%) | (0%) | (8%) | (7%) | |
| B: Countries that do not have bona fide NAP but have proxy NAP 3 | 98 | 49 | 28 | 15 | 6 | 17 | 4 | 39 | 14 | 12 | 12 | 51 | 47 |
| (50%) | (78%) | (52%) | (31%) | (21%) | (68%) | (36%) | (72%) | (40%) | (26%) | (57%) | (78%) | (36%) | |
| C: Countries that have neither bona fide or proxy NAP but have other relevant published information | 51 | 10 | 14 | 16 | 11 | 2 | 2 | 8 | 13 | 19 | 7 | 9 | 42 |
| (26%) | (16%) | (26%) | (33%) | (38%) | (8%) | (18%) | (15%) | (37%) | (40%) | (33%) | (14%) | (32%) | |
| D: Countries with no relevant published information | 32 | 1 | 9 | 10 | 12 | 1 | 1 | 4 | 8 | 16 | 2 | 0 | 32 |
| (16%) | (2%) | (17%) | (20%) | (41%) | (4%) | (9%) | (7%) | (23%) | (34%) | (10%) | (0%) | (25%) | |
| All countries | 195 | 63 | 54 | 49 | 29 | 27 | 11 | 54 | 35 | 47 | 21 | 65 | 130 |
| (100%) | (100%) | (100%) | (100%) | (100%) | (100%) | (100%) | (100%) | (100%) | (100%) | (100%) | (100%) | (100%) | |
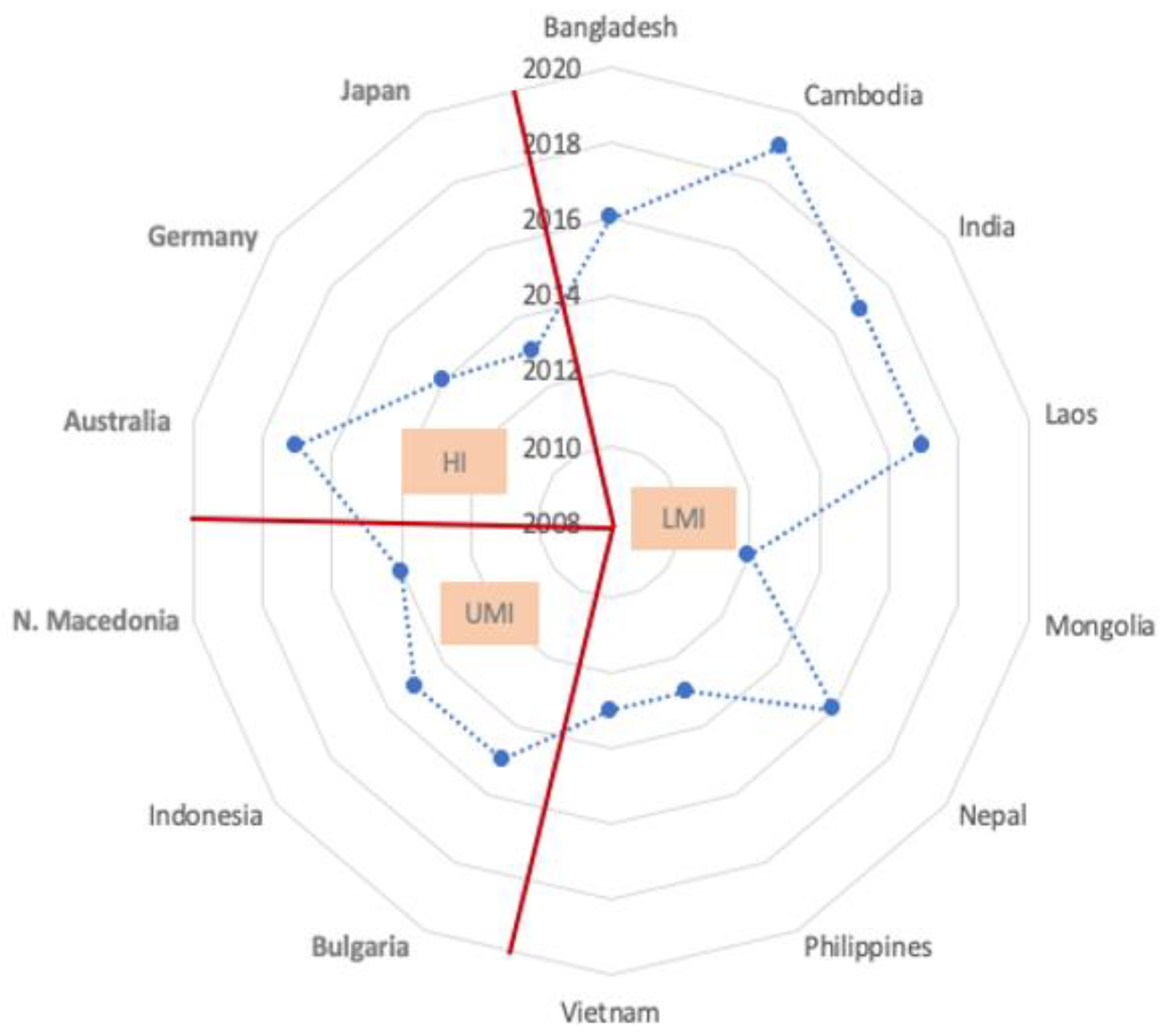
| Country | NAP Publication Year | National Income Category 1 | Region 2 | Asbestos Ban | Authors 3 |
|---|---|---|---|---|---|
| Australia | 2017 | HI | WP | 2003 | G |
| Bangladesh | 2016 | LMI | SEA | No-ban | NG |
| Bulgaria | 2015 | UMI | EUR | 2005 | G |
| Cambodia | 2019 | LMI | WP | No-ban | G, MS |
| Germany | 2014 | HI | EUR | 2005 | G |
| India | 2017 | LMI | SEA | No-ban | NG |
| Indonesia | 2015 | UMI | SEA | No-ban | NG, MS |
| Japan | 2013 | HI | WP | 2007 | NG, MS |
| Laos | 2017 | LMI | WP | No-ban | G, MS |
| North Macedonia | 2014 | UMI | EUR | 2014 | NG, MS |
| Mongolia | 2012 | LMI | WP | No-ban | G, MS |
| Nepal | 2016 | LMI | SEA | No-ban | NG, MS |
| Philippines | 2013 | LMI | WP | No-ban | G, MS |
| Vietnam | 2013 | LMI | WP | No-ban | G, MS |
| Country Category | Data Availability | |||||
|---|---|---|---|---|---|---|
| Asbestos Data | Disease Data | |||||
| Consumption of Raw Asbestos < USGS 1 > (Row %) | Asbestos-Containing Material, Cement, Textiles or Friction Material < UN Comtrade 2 > (row %) | Reported Mortality of Mesothelioma or Asbestosis 3 < WHO MDB 3 > (Row%) | Estimated Incidence of Mesothelioma < GBD 4 > (Row %) | Estimated Mortality of Mesothelioma < WHO GHE 5 > (Row %) | Reported or Estimated Mortality of Mesothelioma < WHO GCO 6 > (Row%) | |
| A (n = 14) | 14 (100%) | 14 (100%) | 7 (50%) | 14 (100%) | 14 (100%) | 13 (93%) |
| B (n = 98) | 83 (85%) | 91 (93%) | 63 (64%) | 91 (93%) | 87 (89%) | 77 (79%) |
| C (n = 51) | 43 (84%) | 46 (90%) | 19 (37%) | 49 (96%) | 47 (92%) | 27 (53%) |
| D (n = 32) | 25 (78%) | 28 (88%) | 7 (22%) | 32 (100%) | 30 (94%) | 17 (53%) |
| All countries (n = 195) | 165 (85%) | 179 (92%) | 96 (49%) | 186 (95%) | 178 (91%) | 134 (69%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arachi, D.; Furuya, S.; David, A.; Mangwiro, A.; Chimed-Ochir, O.; Lee, K.; Tighe, P.; Takala, J.; Driscoll, T.; Takahashi, K. Development of the “National Asbestos Profile” to Eliminate Asbestos-Related Diseases in 195 Countries. Int. J. Environ. Res. Public Health 2021, 18, 1804. https://doi.org/10.3390/ijerph18041804
Arachi D, Furuya S, David A, Mangwiro A, Chimed-Ochir O, Lee K, Tighe P, Takala J, Driscoll T, Takahashi K. Development of the “National Asbestos Profile” to Eliminate Asbestos-Related Diseases in 195 Countries. International Journal of Environmental Research and Public Health. 2021; 18(4):1804. https://doi.org/10.3390/ijerph18041804
Chicago/Turabian StyleArachi, Diana, Sugio Furuya, Annette David, Alexander Mangwiro, Odgerel Chimed-Ochir, Kenneth Lee, Peter Tighe, Jukka Takala, Tim Driscoll, and Ken Takahashi. 2021. "Development of the “National Asbestos Profile” to Eliminate Asbestos-Related Diseases in 195 Countries" International Journal of Environmental Research and Public Health 18, no. 4: 1804. https://doi.org/10.3390/ijerph18041804
APA StyleArachi, D., Furuya, S., David, A., Mangwiro, A., Chimed-Ochir, O., Lee, K., Tighe, P., Takala, J., Driscoll, T., & Takahashi, K. (2021). Development of the “National Asbestos Profile” to Eliminate Asbestos-Related Diseases in 195 Countries. International Journal of Environmental Research and Public Health, 18(4), 1804. https://doi.org/10.3390/ijerph18041804