
How a Depressive Medical Doctor Profited in the Long-Term from a New and Short Psychological Group-Treatment against Major Depressive Disorder

 ,
,
Abstract
:1. Introduction
2. Case Description
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5®); American Psychiatric Pub.: Washington, DC, USA, 2013; p. 795ff. [Google Scholar]
- Munkholm, K.; Paludan-Müller, A.S.; Boesen, K. Considering the methodological limitations in the evidence base of antidepressants for depression: A reanalysis of a network meta-analysis. BMJ Open 2019, 9, e024886. [Google Scholar] [CrossRef] [Green Version]
- Hengartner, M.P. Scientific debate instead of beef; challenging misleading arguments about the efficacy of antidepressants. Acta Neuropsychiatr. 2019, 31, 235–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Covi, L.; Lipman, R.; Pattison, J.; Derogatis, L.; Uhlenhuth, E. Length of treatment with anxiolytic sedatives and response to their sudden withdrawal. Acta Psychiatr. Scand. 1973, 49, 51–64. [Google Scholar] [CrossRef]
- Fontaine, R.; Chouinard, G.; Annable, L. Rebound anxiety in anxious patients after abrupt withdrawal of benzodiazepine treatment. Am. J. Psychiatry 1984, 141, 848–852. [Google Scholar] [PubMed]
- Chouinard, G.; Chouinard, V.-A. New classification of selective serotonin reuptake inhibitor withdrawal. Psychother. Psychosom. 2015, 84, 63–71. [Google Scholar] [CrossRef]
- World Health Organization. WHO Expert Committee on Drug Dependence: Thirty-Third Report; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Cipriani, A.; Furukawa, T.A.; Salanti, G.; Chaimani, A.; Atkinson, L.Z.; Ogawa, Y.; Leucht, S.; Ruhe, H.G.; Turner, E.H.; Higgins, J.P.T.; et al. Comparative efficacy and acceptability of 21 antidepressant drugs for the acute treatment of adults with major depressive disorder: A systematic review and network meta-analysis. Focus 2018, 16, 420–429. [Google Scholar] [CrossRef] [PubMed]
- Hengartner, M.P.; Plöderl, M. Newer-generation antidepressants and suicide risk in randomized controlled trials: A re-analysis of the FDA database. Psychother. Psychosom. 2019, 88, 247–248. [Google Scholar] [CrossRef] [PubMed]
- Hengartner, M.P.; Plöderl, M. Statistically significant antidepressant-placebo differences on subjective symptom-rating scales do not prove that the drugs work: Effect size and method bias matter! Front. Psychiatry 2018, 9, 517. [Google Scholar] [CrossRef] [PubMed]
- Gaynes, B.N.; Lloyd, S.W.; Lux, L.; Gartlehner, G.; Hansen, R.A.; Brode, S.; Jonas, D.E.; Evans, T.W.; Viswanathan, M.; Lohr, K.N. Repetitive transcranial magnetic stimulation for treatment-resistant depression: A systematic review and meta-analysis. J. Clin. Psychiatry 2014, 75, 477–489. [Google Scholar] [CrossRef]
- Salehi, I.; Hosseini, S.M.; Haghighi, M.; Jahangard, L.; Bajoghli, H.; Gerber, M.; Pühse, U.; Holsboer-Trachsler, E.; Brand, S. Electroconvulsive therapy (ECT) and aerobic exercise training (AET) increased plasma BDNF and ameliorated depressive symptoms in patients suffering from major depressive disorder. J. Psychiatr. Res. 2016, 76, 1–8. [Google Scholar] [CrossRef]
- Ren, J.; Li, H.; Palaniyappan, L.; Liu, H.; Wang, J.; Li, C.; Rossini, P.M. Repetitive transcranial magnetic stimulation versus electroconvulsive therapy for major depression: A systematic review and meta-analysis. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2014, 51, 181–189. [Google Scholar] [CrossRef]
- Li, J.-M.; Zhang, Y.; Su, W.-J.; Liu, L.-L.; Gong, H.; Peng, W.; Jiang, C.-L. Cognitive behavioral therapy for treatment-resistant depression: A systematic review and meta-analysis. Psychiatry Res. 2018, 268, 243–250. [Google Scholar] [CrossRef] [PubMed]
- Cuijpers, P.; Berking, M.; Andersson, G.; Quigley, L.; Kleiboer, A.; Dobson, K.S. A meta-analysis of cognitive-behavioural therapy for adult depression, alone and in comparison with other treatments. Can. J. Psychiatry 2013, 58, 376–385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schuch, F.; Vancampfort, D.; Firth, J.; Rosenbaum, S.; Ward, P.; Reichert, T.; Bagatini, N.C.; Bgeginski, R.; Stubbs, B. Physical activity and sedentary behavior in people with major depressive disorder: A systematic review and meta-analysis. J. Affect. Disord. 2017, 210, 139–150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schuch, F.B.; Morres, I.D.; Ekkekakis, P.; Rosenbaum, S.; Stubbs, B. A critical review of exercise as a treatment for clinically depressed adults: Time to get pragmatic. Acta Neuropsychiatr. 2017, 29, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Schuch, F.; Vasconcelos-Moreno, M.; Borowsky, C.; Zimmermann, A.; Rocha, N.; Fleck, M. Exercise and severe major depression: Effect on symptom severity and quality of life at discharge in an inpatient cohort. J. Psychiatr. Res. 2015, 61, 25–32. [Google Scholar] [CrossRef]
- Stubbs, B.; Rosenbaum, S.; Vancampfort, D.; Ward, P.B.; Schuch, F.B. Exercise improves cardiorespiratory fitness in people with depression: A meta-analysis of randomized control trials. J. Affect. Disord. 2016, 190, 249–253. [Google Scholar] [CrossRef]
- Netterstrøm, B.; Conrad, N.; Bech, P.; Fink, P.; Olsen, O.; Rugulies, R.; Stansfeld, S. The relation between work-related psychosocial factors and the development of depression. Epidemiol. Rev. 2008, 30, 118–132. [Google Scholar] [CrossRef] [Green Version]
- Stansfeld, S.; Candy, B. Psychosocial work environment and mental health—A meta-analytic review. Scand. J. Work Environ. Health 2006, 32, 443–462. [Google Scholar] [CrossRef]
- Nieuwenhuijsen, K.; Bruinvels, D.; Frings-Dresen, M. Psychosocial work environment and stress-related disorders, a systematic review. Occup. Med. 2010, 60, 277–286. [Google Scholar] [CrossRef] [Green Version]
- Ndjaboué, R.; Brisson, C.; Vézina, M. Organisational justice and mental health: A systematic review of prospective studies. Occup. Environ. Med. 2012, 69, 694–700. [Google Scholar] [CrossRef] [PubMed]
- Virtanen, M.; Nyberg, S.T.; Batty, G.D.; Jokela, M.; Heikkilä, K.; Fransson, E.I.; Alfredsson, L.; Bjorner, J.B.; Borritz, M.; Burr, H.; et al. Perceived job insecurity as a risk factor for incident coronary heart disease: Systematic review and meta-analysis. BMJ 2013, 374, f4746. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stuke, H.; Bermpohl, F. Welche Arbeitsbedingungen begünstigen die Entwicklung einer depressiven Störung? Psychiatr. Prax. 2016, 43, 245–252. [Google Scholar] [CrossRef] [PubMed]
- Lépine, J.-P.; Briley, M. The increasing burden of depression. Neuropsychiatr. Dis. Treat. 2011, 7 (Suppl. 1), 3. [Google Scholar]
- Amos, T.B.; Tandon, N.; Lefebvre, P.; Pilon, D.; Kamstra, R.L.; Pivneva, I.; Greenberg, P.E. Direct and Indirect Cost Burden and Change of Employment Status in Treatment-Resistant Depression: A Matched-Cohort Study Using a US Commercial Claims Database. J. Clin. Psychiatry 2018, 79, 17m11725. [Google Scholar] [CrossRef] [Green Version]
- Lerner, D.; Adler, D.A.; Chang, H.; Lapitsky, L.; Hood, M.Y.; Perissinotto, C.; Reed, J.; McLaughlin, T.J.; Berndt, E.R.; Rogers, W.H. Unemployment, job retention, and productivity loss among employees with depression. Psychiatr. Serv. 2004, 55, 1371–1378. [Google Scholar] [CrossRef]
- Evans-Lacko, S.; Koeser, L.; Knapp, M.; Longhitano, C.; Zohar, J.; Kuhn, K. Evaluating the economic impact of screening and treatment for depression in the workplace. Eur. Neuropsychopharmacol. 2016, 26, 1004–1013. [Google Scholar] [CrossRef] [Green Version]
- McTernan, W.P.; Dollard, M.F.; LaMontagne, A.D. Depression in the workplace: An economic cost analysis of depression-related productivity loss attributable to job strain and bullying. Work Stress 2013, 27, 321–338. [Google Scholar] [CrossRef]
- McCrone, P.; Rost, F.; Koeser, L.; Koutoufa, I.; Stephanou, S.; Knapp, M.; Goldberg, D.; Taylor, D.; Fonagy, P. The economic cost of treatment-resistant depression in patients referred to a specialist service. J. Ment. Health 2018, 27, 567–573. [Google Scholar] [CrossRef]
- Schramm, E.; Berger, M. Interpersonal psychotherapy for work-related stress depressive disorders. Nervenarzt 2013, 84, 813–822. [Google Scholar] [CrossRef]
- Niedermoser, D.W.; Kalak, N.; Kiyhankhadiv, A.; Brand, S.; Walter, C.; Schweinfurth, N.; Lang, U.E. Workplace-Related Interpersonal Group Psychotherapy to Improve Life at Work in Individuals With Major Depressive Disorders: A Randomized Interventional Pilot Study. Front. Psychiatry 2020, 11, 168. [Google Scholar] [CrossRef]
- Cuijpers, P.; van Straten, A.; Hollon, S.; Andersson, G. The contribution of active medication to combined treatments of psychotherapy and pharmacotherapy for adult depression: A meta-analysis. Acta Psychiatr. Scand. 2010, 121, 415–423. [Google Scholar] [CrossRef] [PubMed]
- Brakemeier, E.-L.; Köhler, S.; Sterzer, P. Schulenübergreifende Psychotherapie der chronischen Depression. PID-Psychother. Dialog 2013, 14, 34–38. [Google Scholar] [CrossRef] [Green Version]
- Boesen, K.; Paludan-Müller, A.S.; Munkholm, K. Network meta-analysis of antidepressants. Lancet 2018, 392, 1011–1012. [Google Scholar] [CrossRef] [Green Version]
- Evans-Lacko, S.; Knapp, M. Global patterns of workplace productivity for people with depression: Absenteeism and presenteeism costs across eight diverse countries. Soc. Psychiatry Psychiatr. Epidemiol. 2016, 51, 1525–1537. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Module | Goals |
|---|---|
|
|
|
|
|
|
|
|
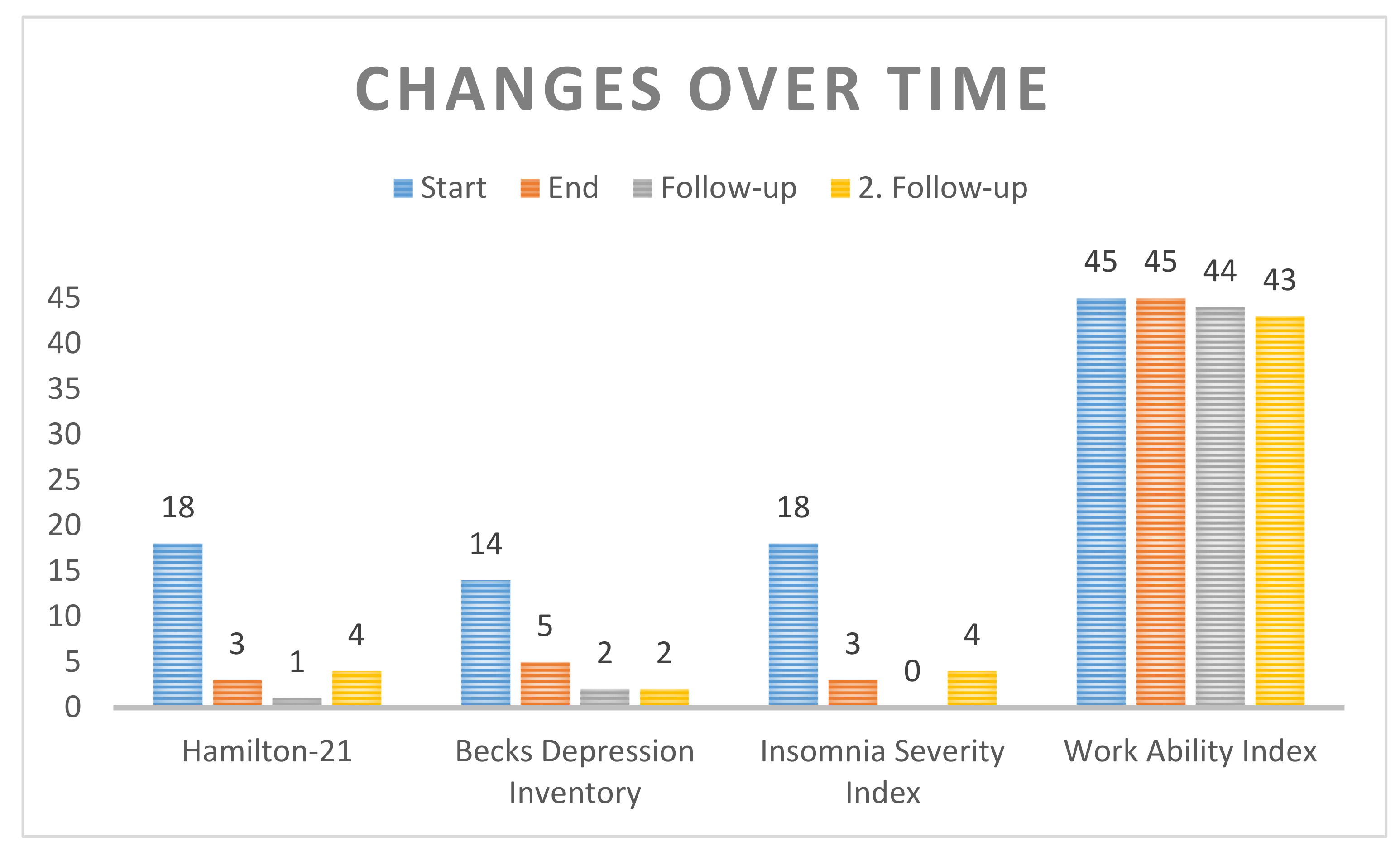
| Start | End | Follow-Up | 2. Follow-Up (15 Months) | |
|---|---|---|---|---|
| Hamilton-21 | 18 | 3 | 1 | 4 |
| Becks Depression Inventory | 14 | 5 | 2 | 2 |
| Insomnia Severity Index | 18 | 3 | 0 | 4 |
| Work Ability Index | 45 | 45 | 44 | 43 |
| Start | End | Follow-Up | 2. Follow-Up (15 Months) | |
|---|---|---|---|---|
| Hamilton-21 | Moderate depression | No depression | No depression | No depression |
| Becks Depression Inventory | Mild depression | No depression | No depression | No depression |
| Insomnia Severity Index | Clinical insomnia, moderate severity | No clinically significant insomnia | No clinically significant insomnia | No clinically significant insomnia |
| Work Ability Index | Very good work ability | Very good work ability | Very good work ability | Good work ability |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Niedermoser, D.W.; Kalak, N.; Meyer, M.; Schweinfurth, N.; Walter, M.; E. Lang, U. How a Depressive Medical Doctor Profited in the Long-Term from a New and Short Psychological Group-Treatment against Major Depressive Disorder. Int. J. Environ. Res. Public Health 2021, 18, 1925. https://doi.org/10.3390/ijerph18041925
Niedermoser DW, Kalak N, Meyer M, Schweinfurth N, Walter M, E. Lang U. How a Depressive Medical Doctor Profited in the Long-Term from a New and Short Psychological Group-Treatment against Major Depressive Disorder. International Journal of Environmental Research and Public Health. 2021; 18(4):1925. https://doi.org/10.3390/ijerph18041925
Chicago/Turabian StyleNiedermoser, Daryl Wayne, Nadeem Kalak, Martin Meyer, Nina Schweinfurth, Marc Walter, and Undine E. Lang. 2021. "How a Depressive Medical Doctor Profited in the Long-Term from a New and Short Psychological Group-Treatment against Major Depressive Disorder" International Journal of Environmental Research and Public Health 18, no. 4: 1925. https://doi.org/10.3390/ijerph18041925
APA StyleNiedermoser, D. W., Kalak, N., Meyer, M., Schweinfurth, N., Walter, M., & E. Lang, U. (2021). How a Depressive Medical Doctor Profited in the Long-Term from a New and Short Psychological Group-Treatment against Major Depressive Disorder. International Journal of Environmental Research and Public Health, 18(4), 1925. https://doi.org/10.3390/ijerph18041925