
The Interplay between Public Health, Well-Being and Population Aging in Europe: An Advanced Structural Equation Modelling and Gaussian Network Approach

 ,
,  ,
, 


Abstract
:1. Introduction
2. Brief Literature Review
3. Data and Methodology
3.1. Data
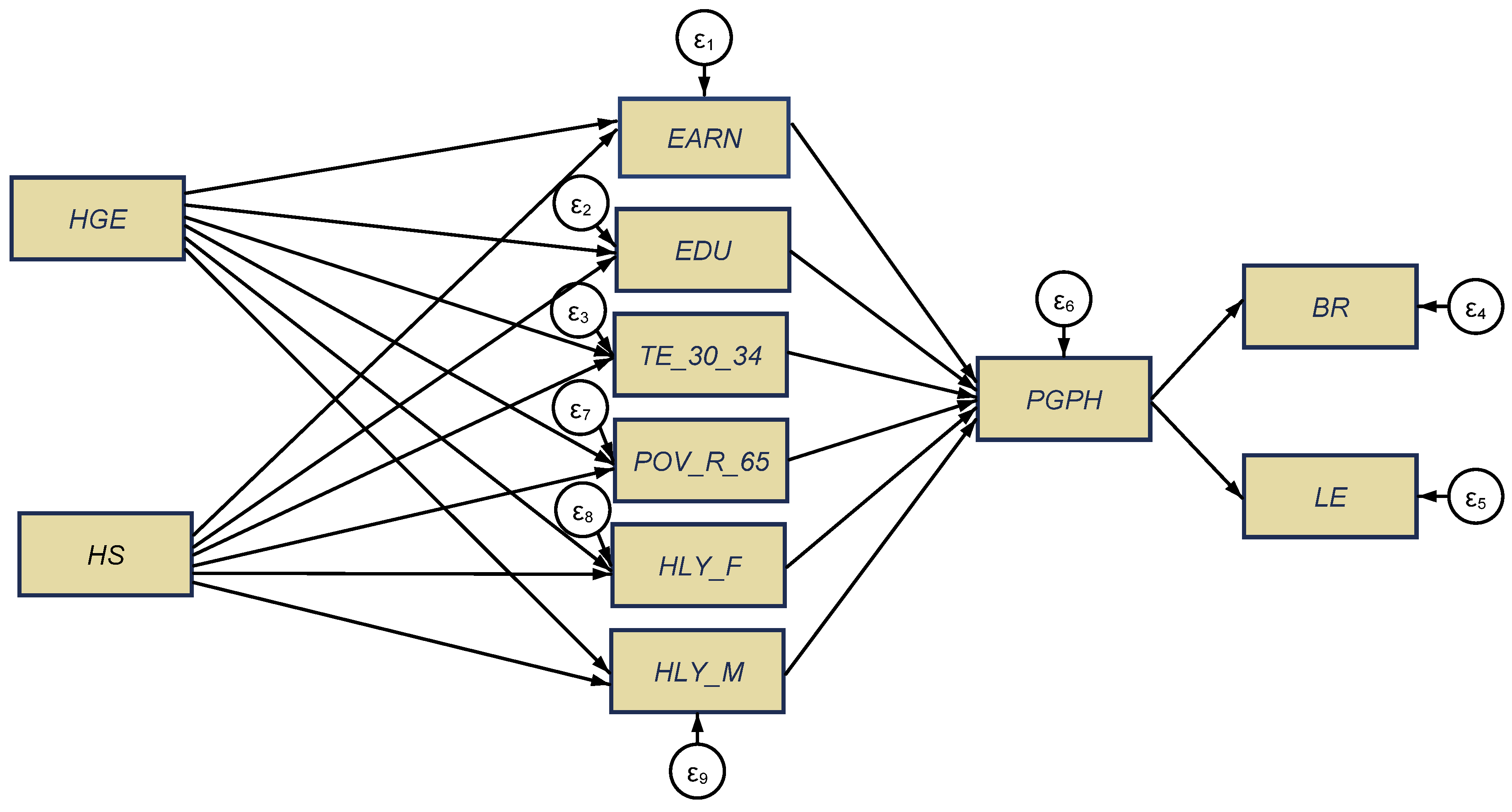
- aging indicators: “Crude birth rate (number of live births per 1000 people)” (BR); “Life expectancy at birth, total population (years)” (LE) (SDG indicator, Goal 3 “Good health and well-being”);
- health indicators: “Health government expenditure” (% of gross domestic product, GDP) (HGE); “Hospital services” (% of GDP) (HS); “Healthy life years in absolute value at 65—females (years)” (HLY_F); “Healthy life years in absolute value at 65—males (years)” (HLY_M); “Share of people aged 16+ with good or very good perceived health” (%) (SDG indicator, Goal 3 “Good health and well-being”) (%) (PGPH);
- other social representative indicators: “Annual net earnings of a two-earner married couple with two children (purchasing power standard)” (EARN); “Population with secondary, upper, post-secondary, and tertiary education (levels 3–8) (% of 15–64 aged years)” (EDU); “Tertiary education level 30–34 age group (% of the population aged 30–34)” (TE_30_34); At-risk-of-poverty-rate of older people, 65+ (%) (POV_R_65).
3.2. Methodology
4. Results and Discussions
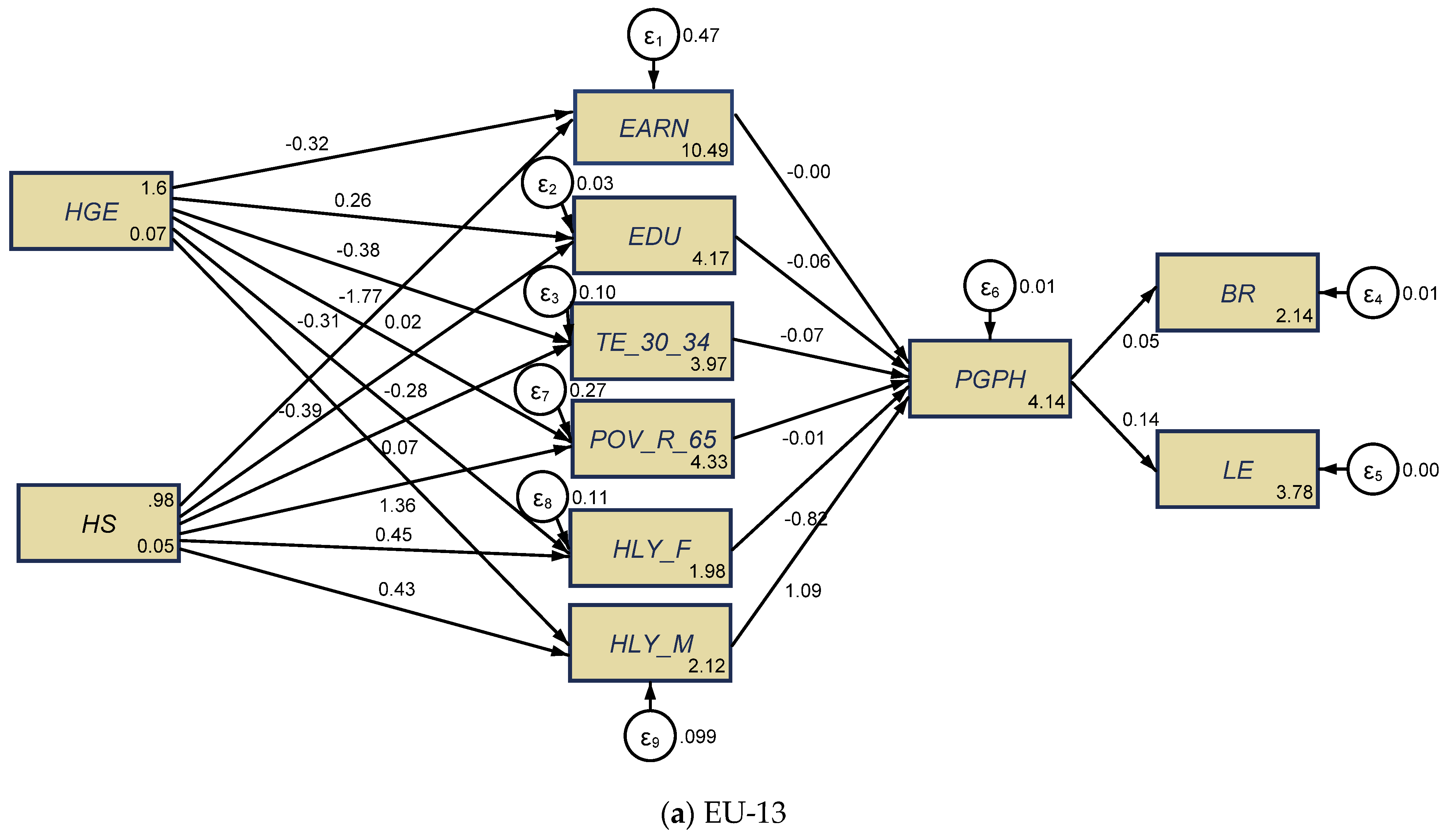
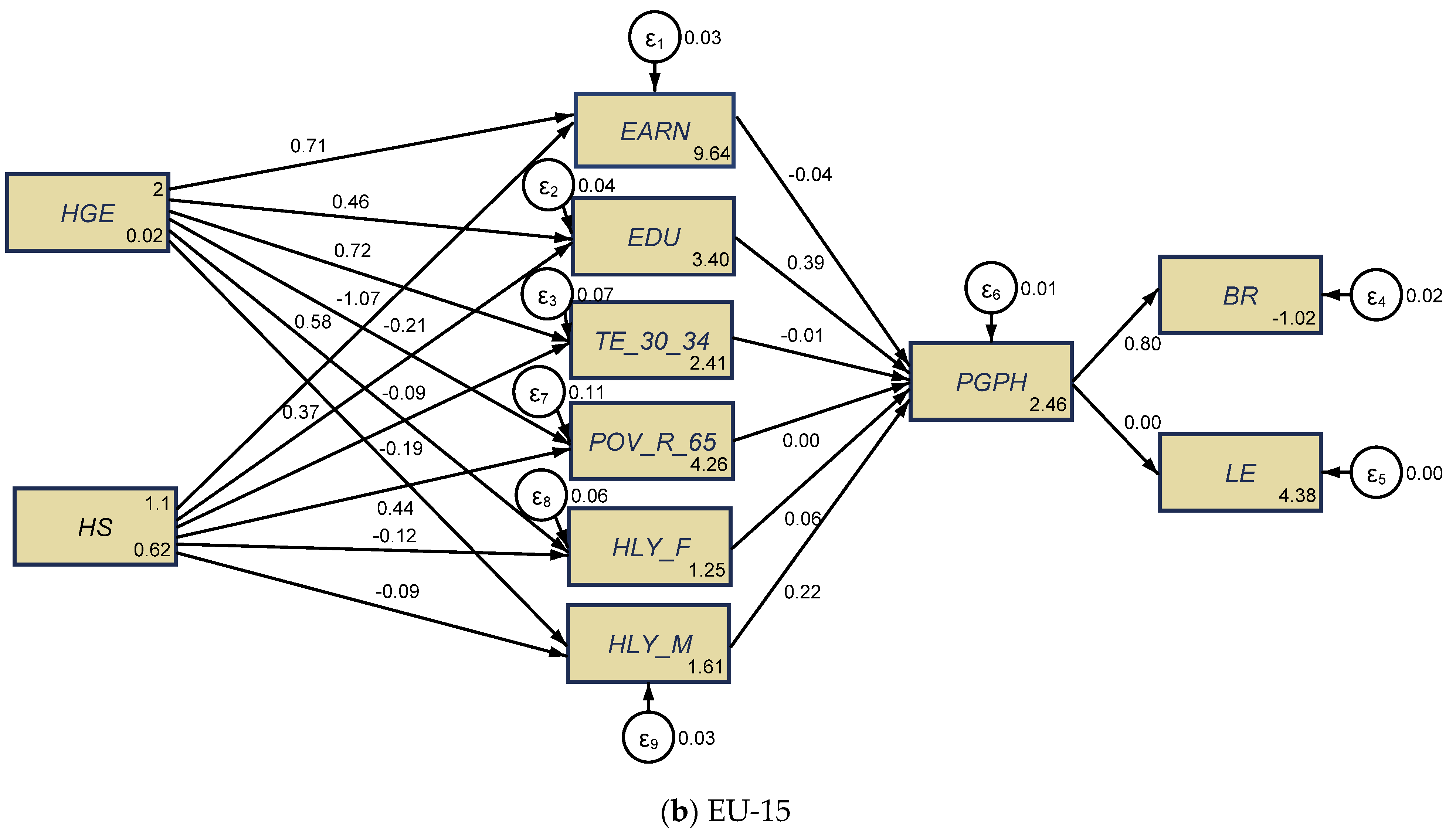
4.1. The Results of Structural Equation Modelling (SEM)
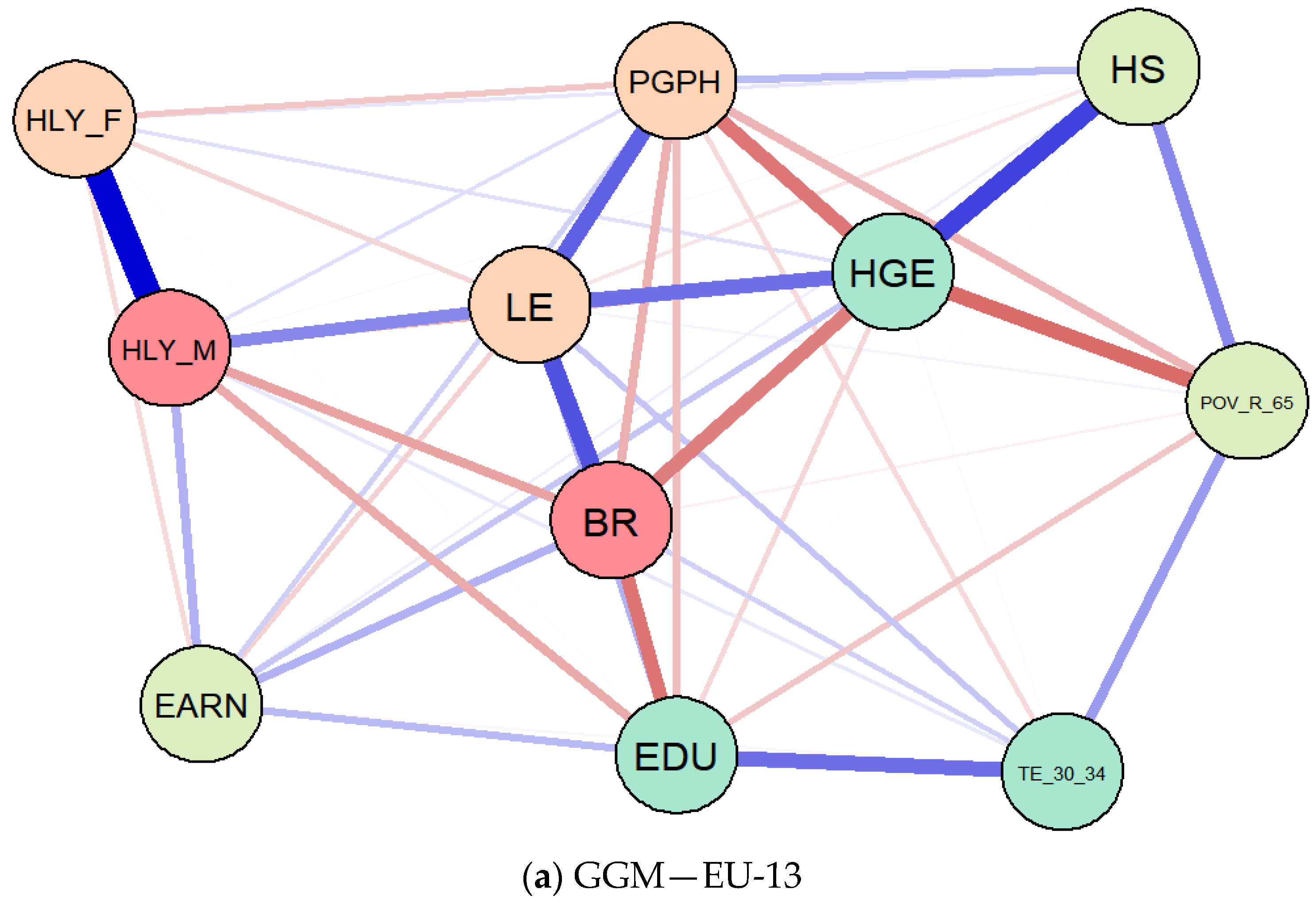
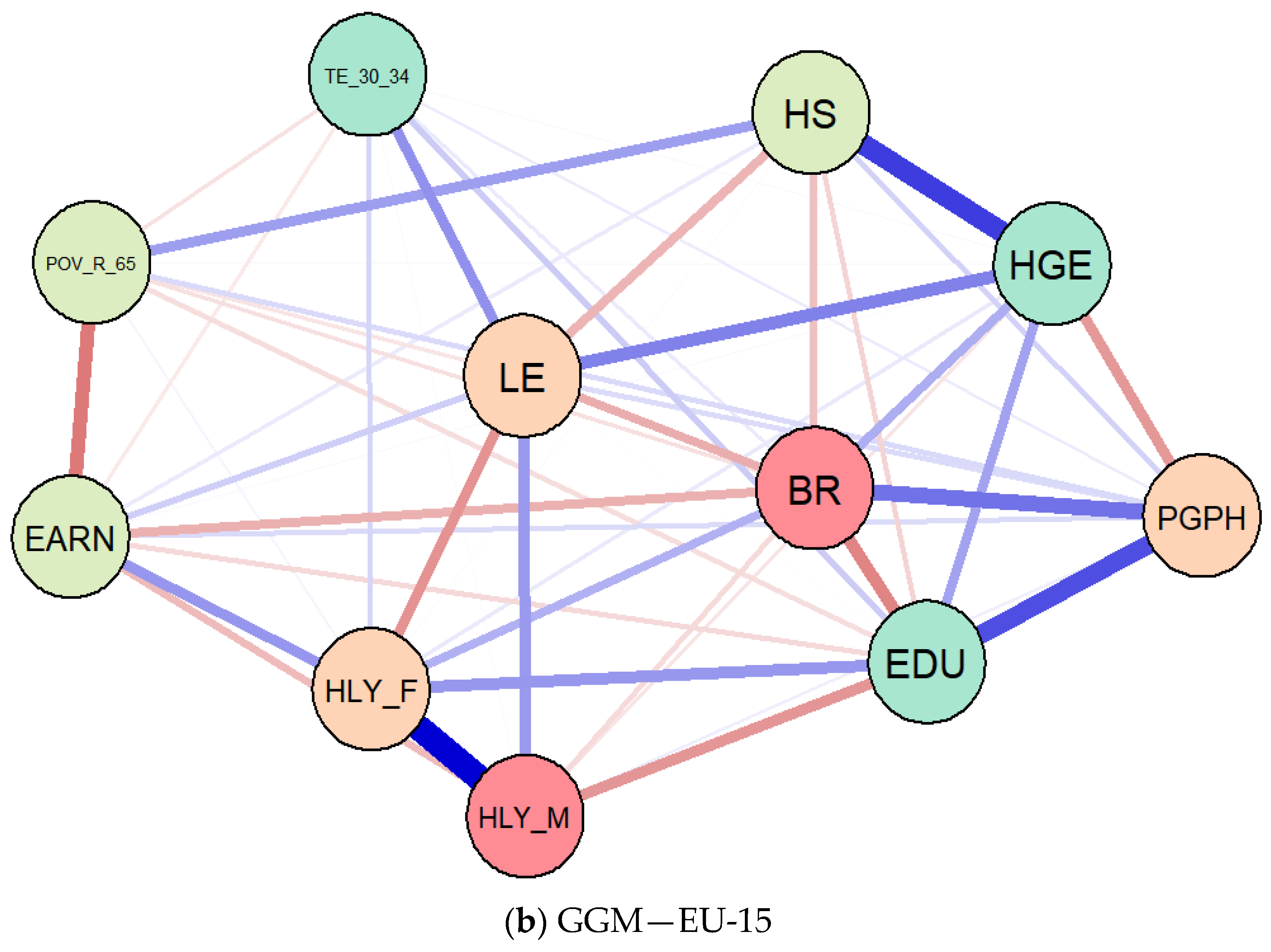
4.2. The Results of Gaussian Graphical Models (GGMs)
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | n | Mean | Standard Deviation | Minimum | Maximum |
|---|---|---|---|---|---|
| EU-13 | |||||
| EDU | 299 | 71.79532 | 14.59404 | 17.1 | 88 |
| EARN | 273 | 35414.8 | 43926.32 | 666.42 | 265212 |
| LE | 273 | 75.16593 | 3.220439 | 67.7 | 82.7 |
| BR | 299 | 10.07358 | 1.053504 | 7.6 | 15.2 |
| TE_30_34 | 299 | 26.13512 | 12.49351 | 1 | 58.7 |
| POV_R_65 | 140 | 19.98786 | 11.30065 | 4.1 | 52 |
| HLY_F | 161 | 7.165217 | 2.504128 | 2.7 | 14.2 |
| HLY_M | 161 | 7.017391 | 2.335047 | 3 | 13.5 |
| HGE | 289 | 4.975779 | 1.415306 | 1.8 | 7.9 |
| HS | 251 | 2.669323 | 0.6839117 | 0.8 | 5.1 |
| PGPH | 164 | 59.72256 | 9.925003 | 35 | 80.3 |
| log_EDU | 299 | 4.24058 | 0.29538 | 2.839078 | 4.477337 |
| log_EARN | 273 | 10.0157 | 0.9378622 | 6.50192 | 12.48829 |
| log_LE | 273 | 4.318788 | 0.0426822 | 4.215086 | 4.41522 |
| log_BR | 299 | 2.304702 | 0.1013955 | 2.028148 | 2.721295 |
| log_TE_30_34 | 299 | 3.129542 | 0.5635107 | 0 | 4.07244 |
| log_POV_R_65 | 140 | 2.811008 | 0.6461677 | 1.410987 | 3.951244 |
| log_HLY_F | 161 | 1.908461 | 0.3540796 | 0.9932518 | 2.653242 |
| log_HLY_M | 161 | 1.894291 | 0.3314473 | 1.098612 | 2.60269 |
| log_HGE | 289 | 1.558653 | 0.3164352 | 0.5877866 | 2.066863 |
| log_HS | 251 | 0.9468871 | 0.272641 | -0.2231435 | 1.629241 |
| log_PGPH | 164 | 4.075466 | 0.1712212 | 3.555348 | 4.38577 |
| N total | 114 | ||||
| EU-15 | |||||
| EDU | 341 | 63.13856 | 13.93617 | 19.3 | 82.3 |
| EARN | 317 | 46101.44 | 27095.49 | 1648.52 | 311052 |
| LE | 330 | 79.63242 | 1.790216 | 75.3 | 83.5 |
| BR | 345 | 11.01391 | 1.720831 | 7.6 | 16.7 |
| TE_30_34 | 345 | 33.01696 | 11.05093 | 8.6 | 54.6 |
| POV_R_65 | 165 | 15.07818 | 5.150729 | 4.7 | 28.3 |
| HLY_F | 192 | 9.878646 | 2.337115 | 5.2 | 16.8 |
| HLY_M | 192 | 9.684375 | 1.839294 | 6.2 | 15.7 |
| HGE | 345 | 6.488696 | 1.085938 | 3.7 | 8.9 |
| HS | 304 | 3.065461 | 1.436566 | 0 | 6.3 |
| PGPH | 196 | 70.79031 | 8.242352 | 45.9 | 84.5 |
| log_EDU | 341 | 4.113025 | 0.2762023 | 2.960105 | 4.410371 |
| log_EARN | 317 | 10.63519 | 0.4655938 | 7.407633 | 12.64772 |
| log_LE | 330 | 4.377168 | 0.0225438 | 4.32148 | 4.424847 |
| log_BR | 345 | 2.387325 | 0.1534143 | 2.028148 | 2.815409 |
| log_TE_30_34 | 345 | 3.428878 | 0.3941481 | 2.151762 | 4.000034 |
| log_POV_R_65 | 165 | 2.645185 | 0.3902959 | 1.547562 | 3.342862 |
| log_HLY_F | 192 | 2.26187 | 0.2422442 | 1.648659 | 2.821379 |
| log_HLY_M | 192 | 2.252649 | 0.1901278 | 1.824549 | 2.753661 |
| log_HGE | 345 | 1.855194 | 0.1758141 | 1.308333 | 2.186051 |
| log_HS | 287 | 1.015284 | 0.7525125 | -2.302585 | 1.84055 |
| log_PGPH | 196 | 4.251958 | 0.1297185 | 3.826465 | 4.436751 |
| n total | 124 | ||||
| Variables | (1) | (2) | Variables | (1) | (2) |
|---|---|---|---|---|---|
| EU-13 | EU-15 | EU-13 | EU-15 | ||
| log_EARN | log_EDU_ATT | ||||
| log_HS | 0.0192 (0.334) | −0.209 *** (0.0313) | log_HS | −0.281 ** (0.0891) | −0.0871 * (0.0349) |
| log_HGE | −0.324 (0.290) | 0.713 *** (0.160) | log_HGE | 0.261 *** (0.0773) | 0.463 ** (0.178) |
| _cons | 10.49 *** (0.404) | 9.635 *** (0.288) | _cons | 4.169 *** (0.108) | 3.398 *** (0.321) |
| log_PGPH | log_TE_30_34 | ||||
| log_EARN | −0.00199 (0.0165) | −0.0410 (0.0618) | log_HS | 0.0663 (0.152) | −0.194 *** (0.0458) |
| log_EDU | −0.0612 (0.0642) | 0.390 *** (0.0607) | log_HGE | −0.383 ** (0.132) | 0.723 ** (0.233) |
| log_TE_30_34 | −0.0732 * (0.0346) | −0.00606 (0.0375) | _cons | 3.973 *** (0.183) | 2.412 *** (0.421) |
| log_POV_R_65 | −0.0131 (0.0164) | 0.00262 (0.0217) | log_POV_R_65 | ||
| log_HLY_F | −0.816 *** (0.0971) | 0.0559 (0.102) | log_HS | 1.357 *** (0.253) | 0.441 *** (0.0579) |
| log_HLY_M | 1.092 *** (0.113) | 0.217 (0.123) | log_HGE | −1.765 *** (0.220) | −1.070 *** (0.295) |
| _cons | 4.139 *** (0.331) | 2.458 *** (0.564) | _cons | 4.331 *** (0.305) | 4.260 *** (0.532) |
| log_HLY_F | log_HLY_M | ||||
| log_HS | 0.447 ** (0.164) | −0.124 ** (0.0415) | log_HS | 0.428 ** (0.153) | −0.0896 ** (0.0320) |
| log_HGE | −0.307 * (0.143) | 0.584 ** (0.211) | log_HGE | −0.391 ** (0.132) | 0.374 * (0.163) |
| _cons | 1.976 *** (0.199) | 1.248 ** (0.381) | _cons | 2.115 *** (0.184) | 1.613 *** (0.294) |
| log_BR | log_LE | ||||
| log_PGPH | 0.0472 (0.0420) | 0.799 *** (0.0920) | log_PGPH | 0.136 *** (0.0173) | 0.00374 (0.00748) |
| _cons | 2.136 *** (0.171) | −1.020 ** (0.392) | _cons | 3.784 *** (0.0706) | 4.378 *** (0.0318) |
| var(e.log_EARN) | var(e.log_PGPH) | ||||
| _cons | 0.473 *** (0.0626) | 0.0326 *** (0.00414) | _cons | 0.00996 *** (0.00132) | 0.00582 *** (0.000739) |
| var(e.log_EDU_ATT) | var(e.log_TE_30_34) | ||||
| _cons | 0.0336 *** (0.00444) | 0.0404 *** (0.00513) | _cons | 0.0973 *** (0.0129) | 0.0696 *** (0.00884) |
| var(e.log_POV_R_65) | var(e.log_HLY_F) | ||||
| _cons | 0.271 *** (0.0359) | 0.111 *** (0.0141) | _cons | 0.114 *** (0.0152) | 0.0570 *** (0.00725) |
| var(e.log_HLY_M) | var(e.log_BR) | ||||
| _cons | 0.0986 *** (0.0131) | 0.0340 *** (0.00432) | _cons | 0.00523 *** (0.000693) | 0.0179 *** (0.00227) |
| var(e.log_LE) | |||||
| _cons | 0.000887 *** (0.000117) | 0.000118 *** (0.0000150) | |||
| n | 114 | 124 |
| Variables | SEM 1—EU-13 | SEM 2—EU-15 | ||||
|---|---|---|---|---|---|---|
| Observation | Sign | Alpha | Observation | Sign | Alpha | |
| Log_EARN | 273 | + | 0.5205 | 317 | + | 0.7413 |
| Log_PGPH | 164 | + | 0.4524 | 196 | + | 0.7120 |
| Log_EDU | 299 | − | 0.5272 | 341 | + | 0.7355 |
| Log_TE_30_34 | 299 | + | 0.5928 | 345 | + | 0.7069 |
| Log_POV_R_65 | 140 | + | 0.5217 | 165 | − | 0.7360 |
| Log_HLY_F | 161 | + | 0.4009 | 192 | + | 0.7079 |
| Log_HLY_M | 161 | + | 0.3722 | 192 | + | 0.7146 |
| Log_BR | 299 | − | 0.6601 | 345 | + | 0.7628 |
| Log_LE | 273 | + | 0.4554 | 330 | + | 0.7763 |
| Log_HS | 251 | + | 0.5603 | 287 | − | 0.7586 |
| Log_HGE | 289 | − | 0.6240 | 345 | − | 0.8098 |
| Total scale | 0.6510 | 0.7618 | ||||
| Variables | SEM 1—EU-13 | SEM 2—EU-15 | ||||
|---|---|---|---|---|---|---|
| Chi2 | df | p-Value | Chi2 | df | p-Value | |
| Log_EARN | 1.71 | 2 | 0.4257 | 45.00 | 2 | ≤0.001 |
| Log_PGPH | 183.94 | 6 | ≤0.001 | 239.38 | 6 | ≤0.001 |
| Log_EDU | 13.75 | 2 | ≤0.001 | 7.43 | 2 | 0.0244 |
| Log_TE_30_34 | 10.53 | 2 | 0.0052 | 18.04 | 2 | ≤0.001 |
| Log_POV_R_65 | 65.79 | 2 | ≤0.001 | 68.43 | 2 | ≤0.001 |
| Log_HLY_F | 7.97 | 2 | 0.0186 | 9.50 | 2 | 0.0086 |
| Log_HLY_M | 10.68 | 2 | 0.0048 | 7.90 | 2 | 0.0192 |
| Log_BR | 1.27 | 1 | 0.2606 | 75.34 | 1 | ≤0.001 |
| Log_LE | 61.61 | 1 | ≤0.001 | 0.25 | 1 | 0.6170 |
| H0: all coefficients excluding the intercepts are 0. We can thus reject the null hypothesis for each equation, with limitations on EARN and BR for EU-13 and LE for EU-15. | ||||||
| Explanations | SEM 1—EU-13 | SEM 2—EU-15 |
|---|---|---|
| Likelihood ratio | ||
| Model vs. saturated chi2_ms (15) | 573.975 | 754.533 |
| p > chi2 | ≤0.001 | ≤0.001 |
| Baseline vs. saturated chi2_bs (24) | 828.606 | 1080.730 |
| p > chi2 | ≤0.001 | ≤0.001 |
| Information criteria | ||
| AIC (Akaike’s information criterion) | −365.186 | −1137.624 |
| BIC (Bayesian information criterion) | −261.210 | −1030.453 |
| Baseline comparison | ||
| CFI (comparative fit index) | 0.803 | 0.898 |
| TLI (Tucker–Lewis index) | 0.407 | 0.515 |
| Size of residuals | ||
| CD (coefficient of determination) | 0.508 | 0.573 |
References
- European Commission. Eurostat-Statistics Explained. Population Structure and Ageing. 2020. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php/Population_structure_and_ageing (accessed on 11 August 2020).
- Lutz, W.; Sanderson, W.C.; Scherbov, S. Global and regional population ageing: How certain are we of its dimensions? J. Popul. Ageing 2008, 1, 75–97. [Google Scholar] [CrossRef] [Green Version]
- Cuaresma, J.C.; Lábaj, M. Pružinský, Prospective ageing and economic growth in Europe. J. Econ. Ageing 2014, 3, 50–57. [Google Scholar] [CrossRef] [Green Version]
- Thalassinos, E.; Cristea, M.; Noja, G.G. Measuring active ageing within the European Union: Implications on economic development. Equilib. Q. J. Econ. Econ. Policy 2019, 14, 591–609. [Google Scholar] [CrossRef]
- Van Groezen, B.; Meijdam, L.; Verbon, H.A. Serving the old: Ageing and economic growth. Oxf. Econ. 2005, 57, 647–663. [Google Scholar] [CrossRef]
- Tinker, A. The social implications of an ageing population. Introduction. Mech. Ageing Dev. 2002, 123, 729–735. [Google Scholar] [CrossRef]
- Beard, J.R.; Officer, A.; Sadana, R.; Pot, A.M.; Michel, J.P.; Lloyd-Sherlock, P.; Epping-Jordan, J.E.; Peeters, G.M.E.E.G.; Mahanani, W.R.; Thiyagarajan, J.A.; et al. The World report on ageing and health: A policy framework for healthy ageing. Lancet 2016, 387, 2145–2154. [Google Scholar] [CrossRef] [Green Version]
- Cristea, M.; Noja, G.G.; Stefea, P.; Sala, A.L. The Impact of Population Aging and Public Health Support on EU Labor Markets. Int. J. Environ. Res. Public Health 2020, 17, 1439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Káčerová, M.; Mládek, J. Population ageing as generation substitutions: Economic and social aspects. Ekon. Cas. 2012, 3, 259–276. [Google Scholar]
- Petretto, D.R.; Pili, R. Ageing and COVID-19: What is the Role for Elderly People? Geriatrics 2020, 5, 25. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Decade of Healthy Ageing (Draft). 2020. Available online: https://www.who.int/docs/default-source/documents/decade-of-health-ageing/decade-ageing-proposal-en.pdf?Status=Temp&sfvrsn=b0a7b5b1_12 (accessed on 12 August 2020).
- World Health Organization (WHO). Active Ageing: A Policy Framework. WHO/NMH/NPH/02.8. 2012. Available online: https://apps.who.int/iris/bitstream/handle/10665/67215/WHO_NMH_NPH_02.8.pdf;jsessionid=29170201D8D99275F7F5024E1C04682A?sequence=1 (accessed on 12 August 2020).
- European Union. The European Year for Active Ageing and Solidarity between Generations; The European Parliament and the Council of the European Union: Brussels, Belgium, 2012. [Google Scholar]
- UNECE/European Commission. 2018 Active Ageing Index: Analytical Report. 2019. Available online: https://www.unece.org/fileadmin/DAM/pau/age/Active_Ageing_Index/Stakeholder_Meeting/ACTIVE_AGEING_INDEX_TRENDS_2008-2016_web_cover_reduced.pdf (accessed on 12 August 2020).
- World Health Organization (WHO). Ageing and Life Course. 2019. Available online: https://www.who.int/ageing/en/ (accessed on 12 August 2020).
- World Health Organization (WHO). 10 Priorities towards a Decade of Healthy Ageing. Department of Ageing and Life Course, WHO/FWC/ALC/17.1. 2017. Available online: https://www.who.int/ageing/WHO-ALC-10-priorities.pdf?ua=1 (accessed on 12 August 2020).
- World Health Organization (WHO). World Report on Ageing and Health. 2015. Available online: https://apps.who.int/iris/bitstream/handle/10665/186463/9789240694811_eng.pdf?sequence=1 (accessed on 12 August 2020).
- European Commission. Eurostat Database. 2020. Available online: https://ec.europa.eu/eurostat/data/database (accessed on 12 August 2020).
- The World Bank. Data. Age Dependency Ratio, Old (% of Working-Age Population). 2020. Available online: https://data.worldbank.org/indicator/SP.POP.DPND.OL (accessed on 10 November 2020).
- Bussolo, M.; Koettl, J.; Sinnott, E. Golden Aging: Prospects for Healthy, Active, and Prosperous Aging in Europe and Central Asia; Europe and Central Asia Studies; The World Bank: Washington DC, USA, 2015; pp. 1–330. [Google Scholar]
- Dustmann, C.; Facchini, G.; Signorotto, C. Population, Migration, Aging and Health: A Survey; Economics without Borders; Economic Research for European Policy Challenges; Cambridge University Press: Cambridge, UK, 2017. [Google Scholar] [CrossRef] [Green Version]
- Gray, A. Population Ageing and Health Care Expenditure; Oxford Institute of Ageing, Ageing Horizons: Oxford, UK, 2015; Available online: https://www.ageing.ox.ac.uk/download/15 (accessed on 28 October 2020).
- Randel, J.; German, T.; Ewing, D. The Ageing and Development Report: Poverty, Independence and the World’s Older People; Routledge: London, UK, 2017. [Google Scholar]
- Sarría-Santamera, A.; Yeskendir, A.; Maulenkul, T.; Orazumbekova, B.; Gaipov, A.; Imaz-Iglesia, I.; Pinilla-Navas, L.; Moreno-Casbas, T.; Corral, T. Population health and health services: Old challenges and new realities in the COVID-19 era. Int. J. Environ. Res. Public Health 2021, 18, 1658. [Google Scholar] [CrossRef]
- Wicks-Lim, J.; Arno, P.S. Improving population health by reducing poverty: New York’s earned income tax credit. SSM-Popul. Health 2017, 3, 373–381. [Google Scholar] [CrossRef]
- Von dem Knesebeck, O.; Vonneilich, N.; Kim, T.J. Public awareness of poverty as a determinant of health: Survey results from 23 countries. Int. J. Public Health 2018, 63, 165–172. [Google Scholar] [CrossRef] [PubMed]
- Arsani, A.M.; Ario, B.; Ramadhan, A.F. Impact of education on poverty and health: Evidence from Indonesia. Econ. Dev. Anal. J. 2020, 9, 87–96. [Google Scholar] [CrossRef]
- Stolz, E.; Mayerl, H.; Waxenegger, A.; Freidl, W. Explaining the impact of poverty on old-age frailty in Europe: Material, psychosocial and behavioural factors. Eur. J. Public Health 2017, 27, 1003–1009. [Google Scholar] [CrossRef]
- Woo, J.; Yu, R.; Cheung, K.; Lai, E.T.C. How much money is enough? Poverty and health in older people. J. Nutr Health Aging 2020, 24, 1111–1115. [Google Scholar] [CrossRef] [PubMed]
- Henseke, G. Good jobs, good pay, better health? The effects of job quality on health among older European workers. Eur. J. Health Econ. 2018, 19, 59–73. Available online: https://link.springer.com/article/10.1007/s10198-017-0867-9 (accessed on 2 November 2020). [CrossRef] [PubMed] [Green Version]
- OECD/EU. Health at a Glance: Europe 2018: State of Health in the EU Cycle; OECD Publishing: Paris, France, 2018. [Google Scholar]
- Brunello, G.; Fort, M.; Schneeweis, N.; Winter-Ebmer, R. The causal effect of education on health: What is the role of health behaviors? Health Econ. 2016, 25, 314–336. [Google Scholar] [CrossRef] [Green Version]
- Cockerham, W.C.; Sharp, K.; Wilcox, J.A. Aging and perceived health status. J. Gerontol. 1983, 38, 349–355. [Google Scholar] [CrossRef]
- Strulik, H. The return to education in terms of wealth and health. J. Econ. Ageing 2018, 12, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Kotschy, R.; Sunde, U. Can education compensate the effect of population ageing on macroeconomic performance? Econ. Policy 2018, 33, 587–634. [Google Scholar] [CrossRef]
- Shields, M.; Shooshtari, S. Determinants of self-perceived health. Health Rep. 2001, 13, 35–52. [Google Scholar]
- Khullar, D.; Chokshi, D.A. Health, income, & poverty: Where we are & what could help? Health Aff. 2018, 4, 1–6. Available online: https://www.healthaffairs.org/do/10.1377/hpb20180817.901935/full/HPB_2017_RWJF_05_W.pdf (accessed on 13 February 2021).
- Kimura, D.; Nakatani, K.; Takeda, T.; Fujita, T.; Sunahara, N.; Inoue, K.; Notoya, M. Analysis of Causal Relationships by Structural Equation Modeling to Determine the Factors Influencing Cognitive Function in Elderly People in Japan. PLoS ONE 2015, 10, e0117554. [Google Scholar] [CrossRef]
- Neufeld, E.; Kristtorn, S. Does non-correlation imply non-causation? Int. J. Approx. Reason. 2007, 46, 257–273. [Google Scholar] [CrossRef] [Green Version]
- Verhulst, B.; Eaves, L. Hatemi, Correlation not Causation: The Relationship between Personality Traits and Political Ideologies. Am. J. Pol. Sci. 2012, 56, 34–51. [Google Scholar] [CrossRef] [Green Version]
- Bullock, H.E.; Harlow, L.L.; Mulaik, S.A. Causation issues in structural equation modeling research. Struct. Equ. Modeling A Multidiscip. J. 1994, 1, 253–267. [Google Scholar] [CrossRef]
- Hitchcock, C. Causal models. Stanf. Encycl. Philos. 2018. Available online: https://plato.stanford.edu/entries/causal-models/ (accessed on 12 February 2021).
- Anyanwu, J.; Erhijakpor, A.E. Health expenditures and health outcomes in Africa. Afr. Dev. Rev. 2009, 21, 400–433. [Google Scholar] [CrossRef]
- Ray, D.; Linden, M. Health expenditure, longevity, and child mortality: Dynamic panel data approach with global data. Int. J. Health Econ. Manag. 2020, 20, 99–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Varvarigos, D.; Zakaria, I.Z. Endogenous fertility in a growth model with public and private health expenditures. J. Popul. Econ. 2013, 26, 67–85. [Google Scholar] [CrossRef] [Green Version]
- Amini, A.A.; Aragam, B.; Zhou, Q. On Perfectness in Gaussian Graphical Models. Cornell University, 2019. Available online: http://arxiv.org/abs/1909.01978 (accessed on 10 November 2020).
- Donald, W. Bayesian estimation for Gaussian Graphical Models: Structure Learning, Predictability, and Network Comparisons. PsyArXiv Preprints. The Society for the Improvement of Psychological Science, 2019. Available online: https://osf.io/x8dpr/download (accessed on 10 November 2020).
- He, H.; Shaolong, C.; Ji-gang, Z.; Hui, S.; Yu-Ping, W.; Hong-wen, D. A statistical test for differential network analysis based on inference of Gaussian Graphical Model. Sci. Rep. 2019, 9, 10863. [Google Scholar] [CrossRef] [PubMed]
- Fitch, K. Learning Directed Graphical Models from Gaussian Data. Cornell University, 2019. Available online: http://arxiv.org/abs/1906.08050 (accessed on 22 November 2020).
- Ha, J.; Kim, J. Ageism and the factors affecting ageism among Korean nursing students: A cross-sectional study. Int. J. Env. Res. Public Health 2021, 18, 1798. [Google Scholar] [CrossRef]
- Pirtea, M.; Nicolescu, C.; Botoc, C. Do Romanian Companies Follow Pecking Order Financing? Econ. Comput. Econ. Cybern. Stud. Res. 2014, 48, 1–15. [Google Scholar]









Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cristea, M.; Noja, G.G.; Jurcuţ, C.-N.; Ponea, C.Ş.; Caragiani, E.S.; Istodor, A.V. The Interplay between Public Health, Well-Being and Population Aging in Europe: An Advanced Structural Equation Modelling and Gaussian Network Approach. Int. J. Environ. Res. Public Health 2021, 18, 2015. https://doi.org/10.3390/ijerph18042015
Cristea M, Noja GG, Jurcuţ C-N, Ponea CŞ, Caragiani ES, Istodor AV. The Interplay between Public Health, Well-Being and Population Aging in Europe: An Advanced Structural Equation Modelling and Gaussian Network Approach. International Journal of Environmental Research and Public Health. 2021; 18(4):2015. https://doi.org/10.3390/ijerph18042015
Chicago/Turabian StyleCristea, Mirela, Graţiela Georgiana Noja, Cecilia-Nicoleta Jurcuţ, Constantin Ştefan Ponea, Elena Sorina Caragiani, and Alin Viorel Istodor. 2021. "The Interplay between Public Health, Well-Being and Population Aging in Europe: An Advanced Structural Equation Modelling and Gaussian Network Approach" International Journal of Environmental Research and Public Health 18, no. 4: 2015. https://doi.org/10.3390/ijerph18042015
APA StyleCristea, M., Noja, G. G., Jurcuţ, C. -N., Ponea, C. Ş., Caragiani, E. S., & Istodor, A. V. (2021). The Interplay between Public Health, Well-Being and Population Aging in Europe: An Advanced Structural Equation Modelling and Gaussian Network Approach. International Journal of Environmental Research and Public Health, 18(4), 2015. https://doi.org/10.3390/ijerph18042015