
A Pandemic within the Pandemic? Physical Activity Levels Substantially Decreased in Countries Affected by COVID-19

 , ,
, ,  , ,
, ,  ,
,  , ,
, ,  , , ,
, , ,  , ,
, ,  ,
,  , ,
, ,  and add
Show full author list
and add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics and Design
2.2. Sample
2.3. Instrument
2.4. Outcomes
2.5. Data Processing and Statistics
3. Results
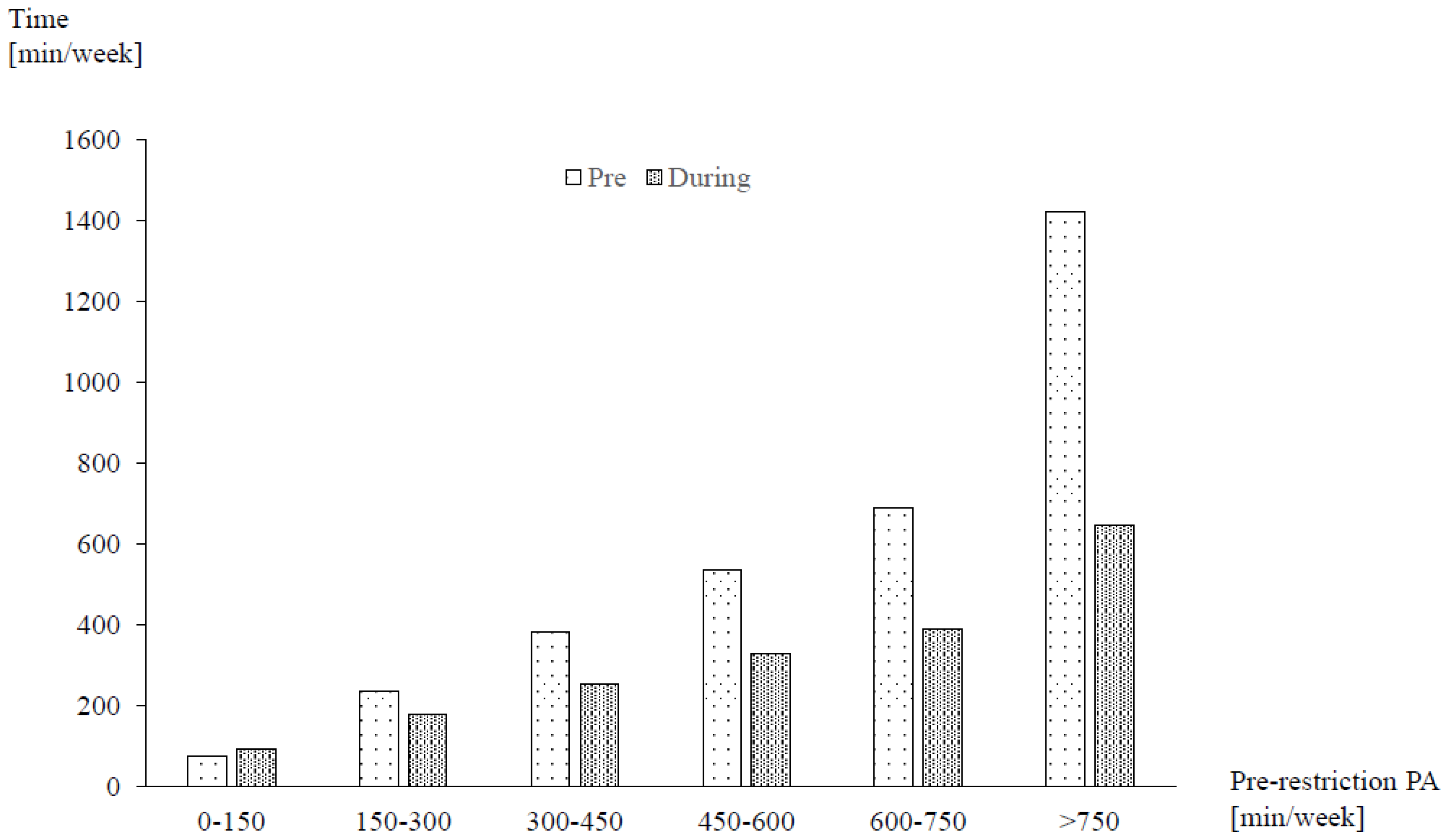
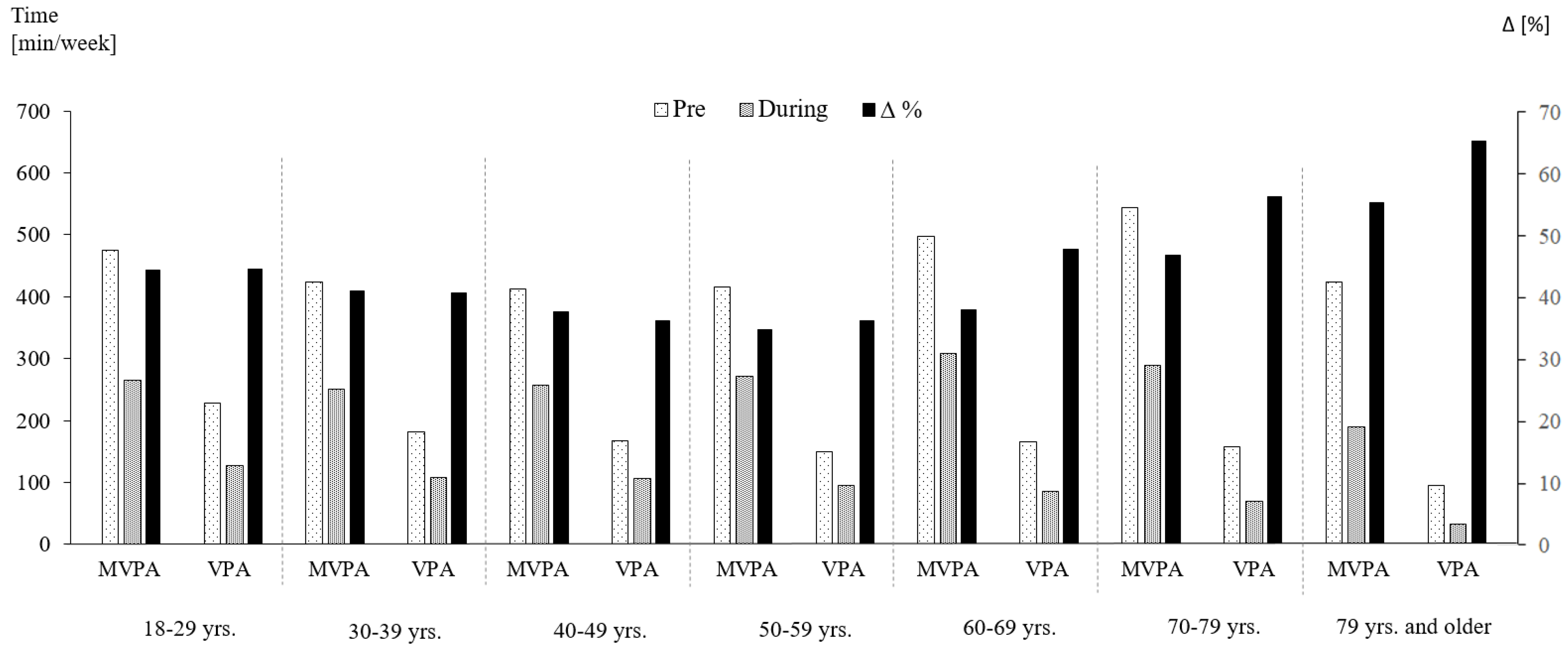
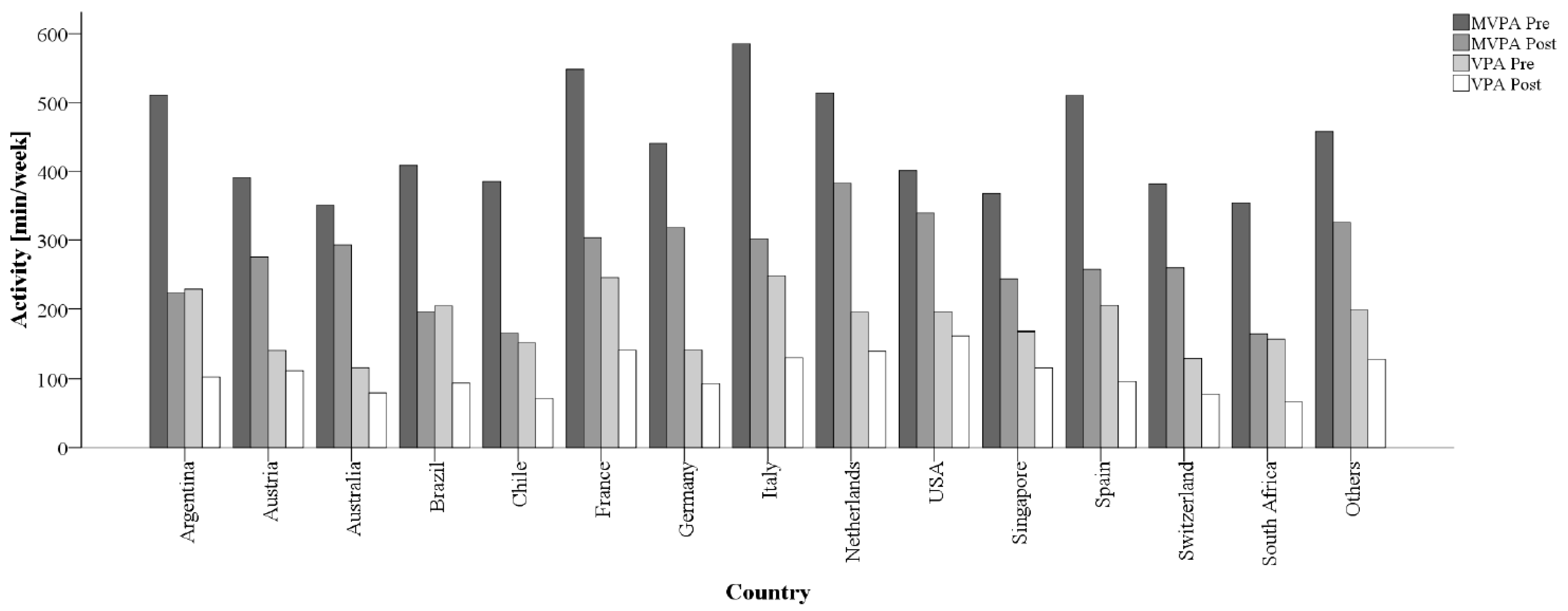
3.1. Changes in Physical Activity
3.2. Changes in Physical Activity Guideline Compliance
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Johns Hopkins University. Johns Hopkins Coronavirus Resource Center. Available online: https://coronavirus.jhu.edu/map.html (accessed on 5 June 2020).
- Lau, H.; Khosrawipour, V.; Kocbach, P.; Mikolajczyk, A.; Schubert, J.; Bania, J.; Khosrawipour, T. The positive impact of lockdown in Wuhan on containing the COVID-19 outbreak in China. J. Travel Med. 2020, 27. [Google Scholar] [CrossRef] [Green Version]
- Tobías, A. Evaluation of the lockdowns for the SARS-CoV-2 epidemic in Italy and Spain after one month follow up. Sci. Total Environ. 2020, 725, 138539. [Google Scholar] [CrossRef]
- Sjödin, H.; Wilder-Smith, A.; Osman, S.; Farooq, Z.; Rocklöv, J. Only strict quarantine measures can curb the coronavirus disease (COVID-19) outbreak in Italy, 2020. Eurosurveillance 2020, 25, 2000280. [Google Scholar] [CrossRef]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quaran-tine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Deelen, I.; Ettema, D.; Kamphuis, C.B.M. Sports participation in sport clubs, gyms or public spaces: How users of different sports settings differ in their motivations, goals, and sports frequency. PLoS ONE 2018, 13, e0205198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, I.-M.; Shiroma, E.J.; Lobelo, F.; Puska, P.; Blair, S.N.; Katzmarzyk, P.T. Effect of physical inactivity on major non-communicable diseases worldwide: An analysis of burden of disease and life expectancy. Lancet 2012, 380, 219–229. [Google Scholar] [CrossRef] [Green Version]
- Pedersen, B.K.; Saltin, B. Exercise as medicine—Evidence for prescribing exercise as therapy in 26 different chronic diseases. Scand. J. Med. Sci. Sports 2015, 25 (Suppl. S3), 1–72. [Google Scholar] [CrossRef] [Green Version]
- Schuch, F.B.; Vancampfort, D.; Firth, J.; Rosenbaum, S.; Ward, P.B.; Silva, E.S.; Hallgren, M.; Ponce De Leon, A.; Dunn, A.L.; Deslandes, A.C.; et al. Physical Activity and Incident Depres-sion: A Meta-Analysis of Prospective Cohort Studies. Am. J. Psychiatry 2018, 175, 631–648. [Google Scholar] [CrossRef]
- Stubbs, B.; Koyanagi, A.; Hallgren, M.; Firth, J.; Richards, J.; Schuch, F.; Rosenbaum, S.; Mugisha, J.; Veronese, N.; Lahti, J.; et al. Physical activity and anxiety: A perspective from the World Health Survey. J. Affect. Disord. 2017, 208, 545–552. [Google Scholar] [CrossRef] [Green Version]
- Arem, H.; Moore, S.C.; Patel, A.; Hartge, P.; De Gonzalez, A.B.; Visvanathan, K.; Campbell, P.T.; Freedman, M.; Weiderpass, E.; Adami, H.O.; et al. Leisure time physical activity and mortality: A detailed pooled analysis of the dose-response relationship. JAMA Intern. Med. 2015, 175, 959–967. [Google Scholar] [CrossRef]
- Stefan, N.; Birkenfeld, A.L.; Schulze, M.B.; Ludwig, D.S. Obesity and impaired metabolic health in patients with COVID-19. Nat. Rev. Endocrinol. 2020, 16, 341–342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simpson, R.J.; Katsanis, E. The immunological case for staying active during the COVID-19 pandemic. Brain Behav. Immun. 2020, 87, 6–7. [Google Scholar] [CrossRef] [PubMed]
- Campbell, J.P.; Turner, J.E. Debunking the Myth of Exercise-Induced Immune Suppression: Redefining the Impact of Exercise on Immunological Health across the Lifespan. Front. Immunol. 2018, 9, 648. [Google Scholar] [CrossRef] [PubMed]
- Fondell, E.; Lagerros, Y.T.; Sundberg, C.J.; Lekander, M.; Bälter, O.; Rothman, K.J.; Bälter, K. Physical Activity, Stress, and Self-Reported Upper Respiratory Tract Infection. Med. Sci. Sports Exerc. 2011, 43, 272–279. [Google Scholar] [CrossRef]
- Fearnbach, S.N.; Flanagan, E.W.; Höchsmann, C.; Beyl, R.A.; Altazan, A.D.; Martin, C.K.; Redman, L.M. Factors Protecting against a Decline in Physical Activity during the COVID-19 Pandemic. Med. Sci. Sports Exerc. 2021. [Google Scholar] [CrossRef]
- Castañeda-Babarro, A.; Arbillaga-Etxarri, A.; Gutiérrez-Santamaría, B.; Coca, A. Physical Activity Change during COVID-19 Confinement. Int. J. Environ. Res. Public Health 2020, 17, 6878. [Google Scholar] [CrossRef]
- Eek, F.; Larsson, C.; Wisén, A.; Hansson, E.E. Self-Perceived Changes in Physical Activity and the Relation to Life Satisfaction and Rated Physical Capacity in Swedish Adults during the COVID-19 Pandemic—A Cross Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 671. [Google Scholar] [CrossRef]
- Meyer, J.; McDowell, C.; Lansing, J.; Brower, C.; Smith, L.; Tully, M.; Herring, M. Changes in Physical Activity and Sedentary Behavior in Response to COVID-19 and Their Associations with Mental Health in 3052 US Adults. Int. J. Environ. Res. Public Health 2020, 17, 6469. [Google Scholar] [CrossRef]
- Giustino, V.; Parroco, A.M.; Gennaro, A.; Musumeci, G.; Palma, A.; Battaglia, G. Physical Activity Levels and Related Energy Expenditure during COVID-19 Quarantine among the Sicilian Active Population: A Cross-Sectional Online Survey Study. Sustainability 2020, 12, 4356. [Google Scholar] [CrossRef]
- Wilke, J.; Mohr, L.; Tenforde, A.S.; Vogel, O.; Hespanhol, L.; Vogt, L.; Verhagen, E.; Hollander, K. Activity and health during the Sars-CoV2 pandemic (ASAP): Study protocol for a multinational network trial. Front. Med. 2020, 7, 302. [Google Scholar] [CrossRef]
- Danquah, I.H.; Petersen, C.B.; Skov, S.S.; Tolstrup, J.S. Validation of the NPAQ-short—A brief questionnaire to monitor physical activity and compliance with the WHO recommendations. BMC Public Health 2018, 18, 601. [Google Scholar] [CrossRef] [PubMed]
- Thomas, H.; Angrist, T.B.; Cameron-Blake, E.; Hallas, L.; Kira, B.; Majumdar, S.; Petherick, A.; Phillips, T.; Tatlow, H.; Web-ster, S. Variation in Government Responses to COVID-19; Version 9.0; Blavatnik School of Government Working Paper; Blavatnik School of Government: Oxford, UK, 2020; Available online: www.bsg.ox.ac.uk/covidtracker (accessed on 15 January 2021).
- Lewis, E.F.; Hardy, M.; Snaith, B. Estimating the Effect of Nonresponse Bias in a Survey of Hospital Organizations. Eval. Health Prof. 2013, 36, 330–351. [Google Scholar] [CrossRef] [PubMed]
- Druss, B.G. Addressing the COVID-19 Pandemic in Populations with Serious Mental Illness. JAMA Psychiatry 2020, 77, 891. [Google Scholar] [CrossRef] [Green Version]
- Jiménez-Pavón, D.; Carbonell-Baeza, A.; Lavie, C.J. Physical exercise as therapy to fight against the mental and physical consequences of COVID-19 quarantine: Special focus in older people. Prog. Cardiovasc. Dis. 2020, 63, 386–388. [Google Scholar] [CrossRef]
- Jakobsson, J.; Malm, C.; Furberg, M.; Ekelund, U.; Svensson, M. Physical Activity during the Coronavirus (COVID-19) Pandemic: Prevention of a Decline in Metabolic and Immunological Functions. Front. Sports Act. Living 2020, 2, 57. [Google Scholar] [CrossRef] [PubMed]
- Davies, K.A.B.; Sprung, V.S.; Norman, J.A.; Thompson, A.; Mitchell, K.L.; Halford, J.C.G.; Harrold, J.A.; Wilding, J.P.H.; Kemp, G.J.; Cuthbertson, D.J. Short-term decreased physical activity with increased sedentary behaviour causes metabolic derangements and altered body composition: Effects in individuals with and without a first-degree relative with type 2 diabetes. Diabetologia 2018, 61, 1282–1294. [Google Scholar] [CrossRef] [Green Version]
- Davies, K.A.B.; Pickles, S.; Sprung, V.S.; Kemp, G.J.; Alam, U.; Moore, D.R.; Tahrani, A.A.; Cuthbertson, D.J. Reduced physical activity in young and older adults: Metabolic and musculoskeletal implications. Ther. Adv. Endocrinol. Metab. 2019, 10. [Google Scholar] [CrossRef]
- Wong, C.-M.; Lai, H.-K.; Ou, C.-Q.; Ho, S.-Y.; Chan, K.-P.; Thach, T.-Q.; Yang, L.; Chau, Y.-K.; Lam, T.-H.; Hedley, A.J.; et al. Is Exercise Protective Against Influenza-Associated Mortality? PLoS ONE 2008, 3, e2108. [Google Scholar] [CrossRef] [Green Version]
- Carlson, S.A.; Fulton, J.E.; Pratt, M.; Yang, Z.; Adams, E.K. Inadequate Physical Activity and Health Care Expenditures in the United States. Prog. Cardiovasc. Dis. 2015, 57, 315–323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swain, D.P.; Franklin, B.A. Comparison of Cardioprotective Benefits of Vigorous Versus Moderate Intensity Aerobic Exercise. Am. J. Cardiol. 2006, 97, 141–147. [Google Scholar] [CrossRef] [PubMed]
- Gebel, K.; Ding, D.; Chey, T.; Stamatakis, E.; Brown, W.J.; Bauman, A.E. Effect of Moderate to Vigorous Physical Activity on All-Cause Mortality in Middle-aged and Older Australians. JAMA Intern. Med. 2015, 175, 970–977. [Google Scholar] [CrossRef] [PubMed]
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Worldwide trends in insufficient physical activity from 2001 to 2016: A pooled analysis of 358 population-based surveys with 1·9 million participants. Lancet Glob. Health 2018, 6, e1077–e1086. [Google Scholar] [CrossRef] [Green Version]
- Valanou, E.M.; Bamia, C.; Trichopoulou, A. Methodology of physical-activity and energy-expenditure assessment: A review. J. Public Health 2006, 14, 58–65. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Physical Activities in Leisure Time We would like to know, how physically active you have been in your free time (including commuting from and to work). We only ask about moderate and vigorous activities—light activities do not need to be reported here. Moderate activities are those where your heartbeat increases and you breathe faster (e.g., brisk walking, cycling as a means of transport or exercise, heavy gardening, running or recreational sports). Vigorous activities as those that get your heart racing, make you sweat and leave you so short of breath that speaking becomes difficult (e.g., swimming, running, cycling at high speeds, intensive cardio training, weight-lifting or team sports such as football). | |
| Physical Activities in the Job While the previous questions addressed free time, the following two focus on work/occupational time. Again, we only ask about moderate and vigorous activities—light activities do not need to be reported here. Remember: Moderate activities are those where your heartbeat increases and you breathe faster (e.g., brisk walking). Vigorous activities are those that get your heart racing, make you sweat and so short of breath that you find it difficult to speak (e.g., repeated lifting of heavy weights). | |
| Moderate and Vigorous Activities On a typical week, how much time in minutes did you spend in total on both moderate and vigorous physical activities? Please sum all activities with a minimal duration of 10 min. Enter 0, if there was not at least one activity of more than 10 min. before lockdown: ___ minutes during lockdown: ___ minutes | Vigorous Activities only How much of that time in minutes you indicated above, did you spend in total on vigorous physical activities only? Please sum all activities with a minimum duration of 10 min. Enter 0, if there was not at least one activity of more than 10 min. before lockdown: ___ minutes during lockdown: ___ minutes |
| Leisure | Work | Total | ||||
|---|---|---|---|---|---|---|
| MVPA (min/wk) | VPA (min/wk) | MVPA (min/wk) | VPA (min/wk) | MVPA (min/wk) | VPA (min/wk) | |
| Pre | 296.0 (290.6 to 301.5) | 134.7 (131.4 to 138.0) | 154.1 (148.0 to 160.2) | 54.4 (51.2 to 57.5) | 450.1 (440.7 to 459.6) | 189.1 (183.6 to 194.5) |
| During | 193.7 (189.6 to 197.7) | 81.9 (79.5 to 84.2) | 72.1 (68.4 to 75.8) | 27.5 (25.5 to 29.5) | 265.8 (259.7 to 271.9) | 109.4 (105.7 to 113.0) |
| ∆ | −102.4 (−107.2 to −97.6) | −52.8 (−55.4 to −50.2) | −82.0 (−86.8 to −77.2) | −26.9 (−29.3 to −24.4) | −184.4 (−192.3 to −176.5) | −79.7 (−84.0 to −75.4) |
| % ∆ | −34.6 | −39.2 | −53.2 | −49.5 | −41.0 | −42.2 |
| Guideline Compliance | ||||
|---|---|---|---|---|
| Pre and During | Pre but Not During | Not Pre but During | Neither Pre nor During | |
| n | 7834 | 3104 | 601 | 1964 |
| Age | 39 ± 15 | 38 ± 15 | 35 ± 13 | 38 ± 16 |
| Sex | Females: 55.1% Males: 62.4% | Females: 22.8% Males: 23.2% | Females: 5.4% Males: 3.2% | Females: 16.8% Males: 11.3% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wilke, J.; Mohr, L.; Tenforde, A.S.; Edouard, P.; Fossati, C.; González-Gross, M.; Sánchez Ramírez, C.; Laiño, F.; Tan, B.; Pillay, J.D.; et al. A Pandemic within the Pandemic? Physical Activity Levels Substantially Decreased in Countries Affected by COVID-19. Int. J. Environ. Res. Public Health 2021, 18, 2235. https://doi.org/10.3390/ijerph18052235
Wilke J, Mohr L, Tenforde AS, Edouard P, Fossati C, González-Gross M, Sánchez Ramírez C, Laiño F, Tan B, Pillay JD, et al. A Pandemic within the Pandemic? Physical Activity Levels Substantially Decreased in Countries Affected by COVID-19. International Journal of Environmental Research and Public Health. 2021; 18(5):2235. https://doi.org/10.3390/ijerph18052235
Chicago/Turabian StyleWilke, Jan, Lisa Mohr, Adam S. Tenforde, Pascal Edouard, Chiara Fossati, Marcela González-Gross, Celso Sánchez Ramírez, Fernando Laiño, Benedict Tan, Julian David Pillay, and et al. 2021. "A Pandemic within the Pandemic? Physical Activity Levels Substantially Decreased in Countries Affected by COVID-19" International Journal of Environmental Research and Public Health 18, no. 5: 2235. https://doi.org/10.3390/ijerph18052235
APA StyleWilke, J., Mohr, L., Tenforde, A. S., Edouard, P., Fossati, C., González-Gross, M., Sánchez Ramírez, C., Laiño, F., Tan, B., Pillay, J. D., Pigozzi, F., Jimenez-Pavon, D., Novak, B., Jaunig, J., Zhang, M., van Poppel, M., Heidt, C., Willwacher, S., Yuki, G., ... Hollander, K. (2021). A Pandemic within the Pandemic? Physical Activity Levels Substantially Decreased in Countries Affected by COVID-19. International Journal of Environmental Research and Public Health, 18(5), 2235. https://doi.org/10.3390/ijerph18052235