
Gender Differences in Work Status during Early Career of Dentists: An Analysis of National Survey Cohort Data of 10 Years in Japan




Abstract
:1. Introduction
2. Materials and Methods
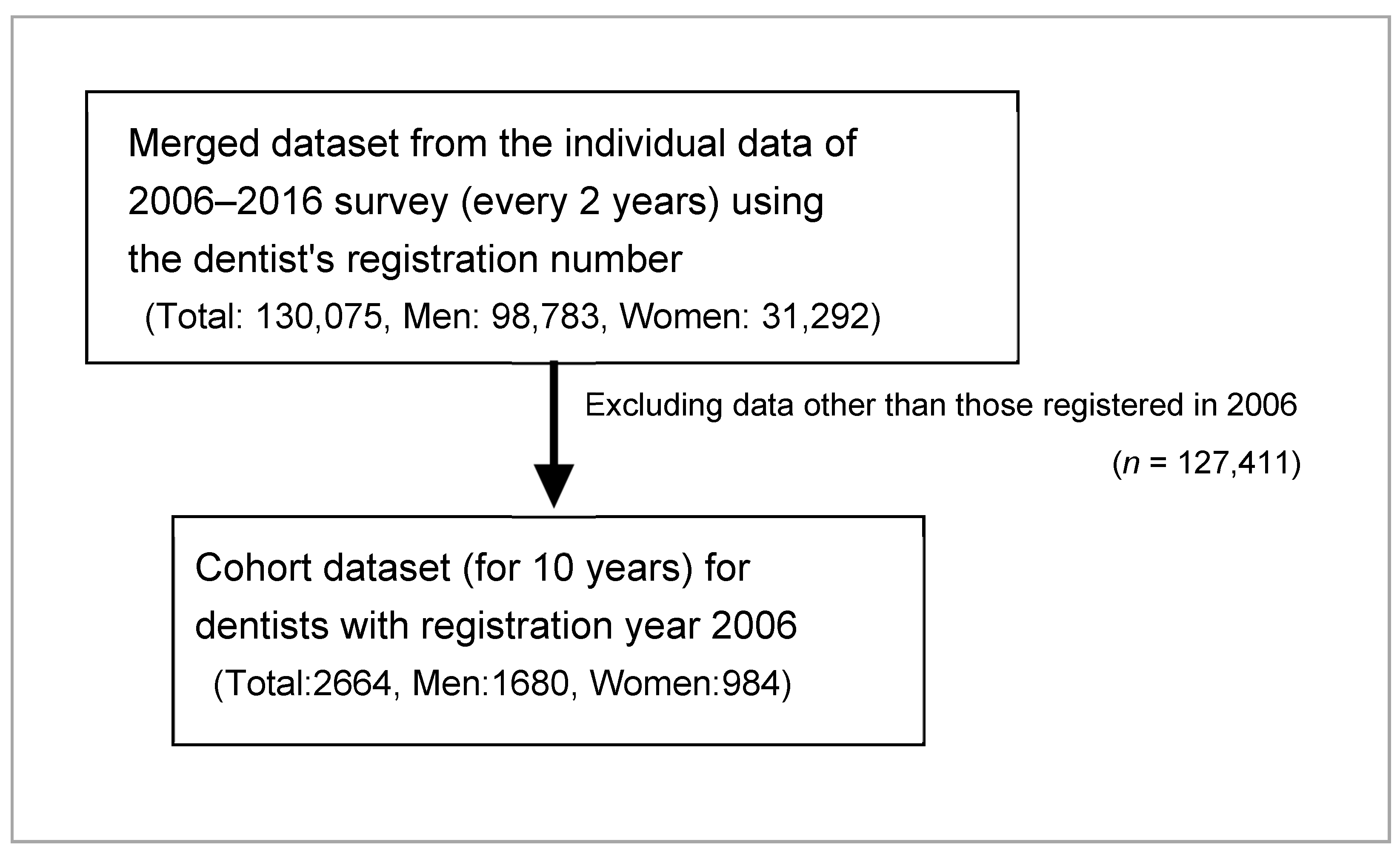
2.1. Data Acquisition and Preparation for Analysis
2.2. Data Analysis
2.3. Ethical Consideration
3. Results
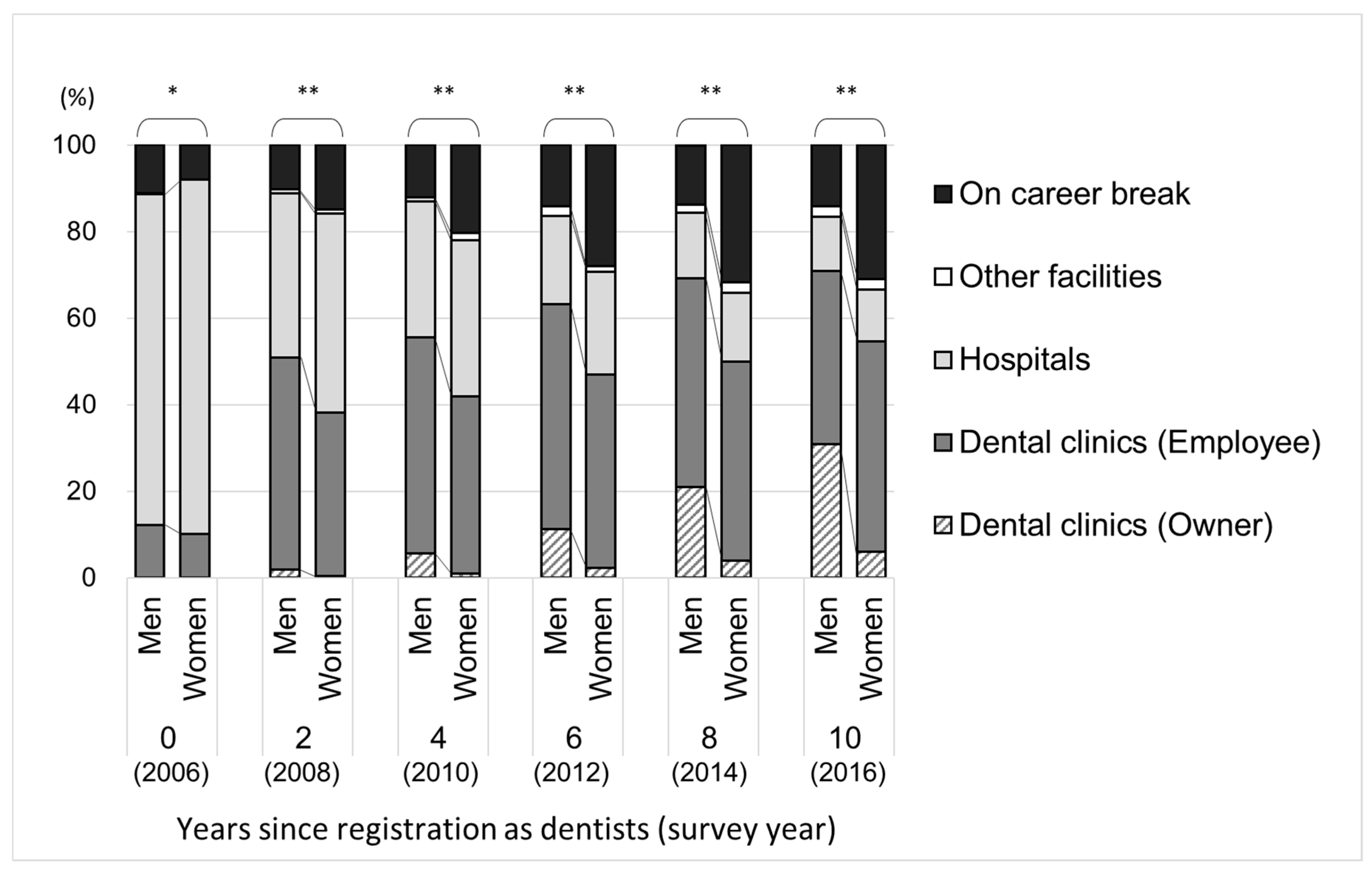
3.1. Changes in Work Status of the Study Participants
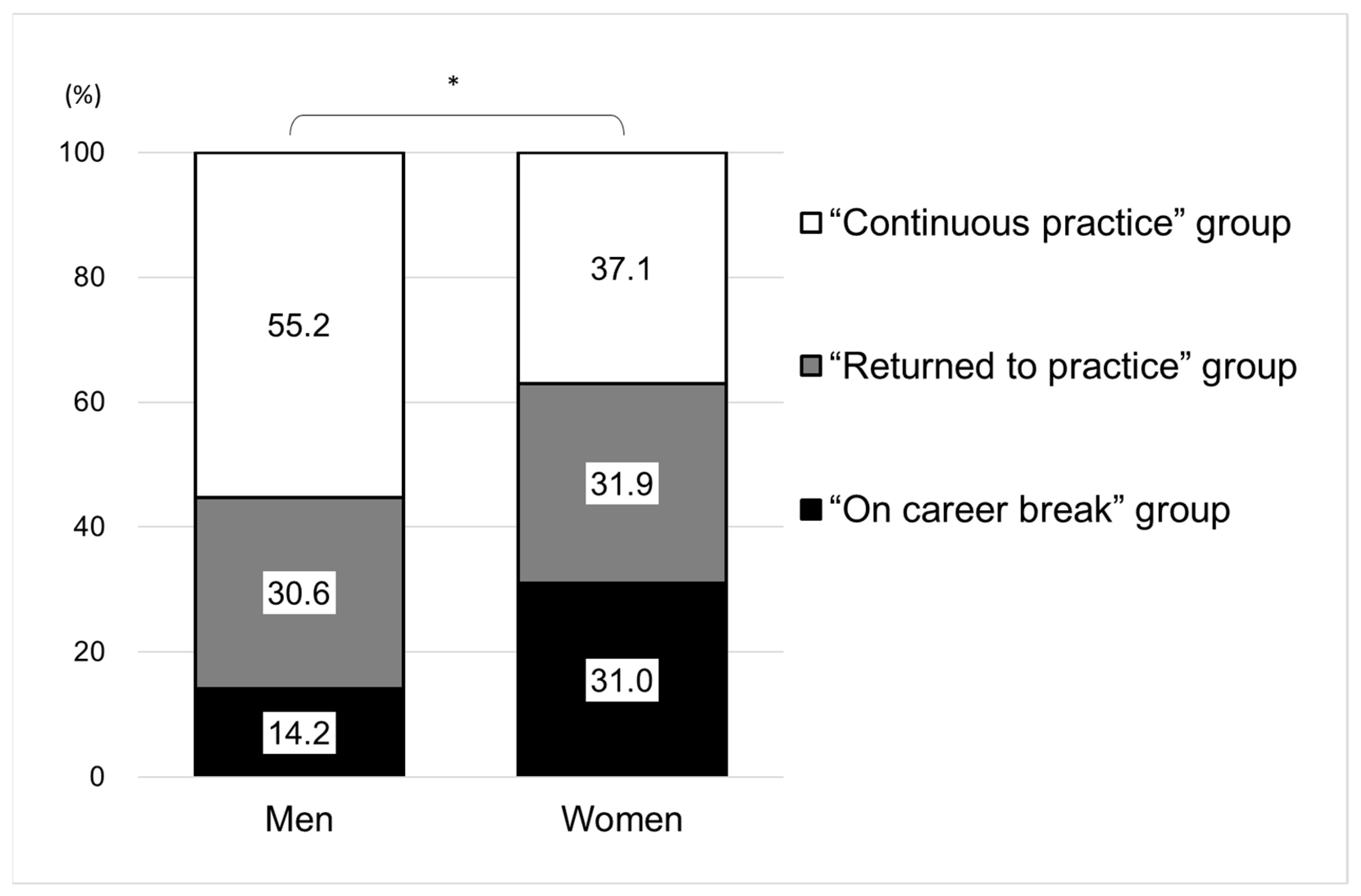
3.2. Gender Differences in Proportion of Those Who Ever Had a Career Break between 2006 and 2016
3.3. Characteristics Associated with the Dentists Who Returned to Practice as of 2016
4. Discussion
4.1. Main Findings
4.2. Gender Differences in Career Break
4.3. Young Dentists Returning to Dental Practice
4.4. Relationship between Geographical Distribution and Young Dentists Returning to Practice
4.5. Increasing Proportion of Female Dentists and the Implications of This Study
4.6. Limitations of This Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- American Dental Association. 2017–2018 Survey of Dental Education—Report 1: Academic Programs, Enrollment, and Graduates; American Dental Association: Chicago, IL, USA, 2018; Available online: https://www.ada.org/en/science-research/health-policy-institute/data-center/dental-education (accessed on 5 January 2021).
- Kravitz, A.; Bullock, A.; Cowpe, J.; Barnes, M. Manual of Dental Practice 2015; 5.1. ed.; Council of European Dentists: Brussels, Belgium, 2016; Available online: https://cedentists.eu/library/eu-manual.html (accessed on 12 December 2020).
- Japan Dental Association. Basic Information on Dental and Oral Health. 2015. Available online: https://www.jda.or.jp/dental_data/pdf/chapter_04.pdf (accessed on 20 December 2020). (In Japanese).
- Tiwari, T.R.; Randall, C.L.; Cohen, L.; Holtzmann, J.; Webster-Cyriaque, J.; Ajiboye, S.A.; Schou, L.; Wandera, M.; Ikeda, K.; Fidela de Lima Navarro, M.; et al. Gender inequalities in the dental workforce: Global perspectives. Adv. Dent. Res. 2019, 30, 60–68. [Google Scholar] [CrossRef] [PubMed]
- Ono, K. Admission of dental students. J. Jpn. Dent. Educ. Assoc. 2017, 10–15. (In Japanese) [Google Scholar]
- Newton, J.T.; Buck, D.; Gibbons, D.E. Workforce planning in dentistry: The impact of shorter and more varied career patterns. Community Dent. Health 2001, 18, 236–241. [Google Scholar]
- del Aguila, M.A.; Leggott, P.J.; Robertson, P.B.; Porterfield, D.L.; Felber, G.D. Practice patterns among male and female general dentists in a Washington State population. J. Am. Dent. Assoc. 2005, 136, 790–796. [Google Scholar] [CrossRef]
- Ayers, K.M.; Thomson, W.M.; Rich, A.M.; Newton, J.T. Gender differences in dentists’ working practices and job satisfaction. J. Dent. 2008, 36, 343–350. [Google Scholar] [CrossRef]
- Pallavi, S.K.; Rajkumar, G.C. Professional practice among woman dentist. J. Int. Soc. Prev. Community Dent. 2011, 1, 14–19. [Google Scholar] [CrossRef] [PubMed]
- McKay, J.C.; Quiñonez, C.R. The feminization of dentistry: Implications for the profession. J. Can. Dent. Assoc. 2012, 78, c1. [Google Scholar] [PubMed]
- McKay, J.C.; Ahmad, A.; Shaw, J.L.; Rashid, F.; Clancy, A.; David, C.; Figueiredo, R.L.F.; Quiñonez, C. Gender differences and predictors of work hours in a sample of Ontario dentists. J. Can. Dent. Assoc. 2016, 82, g26. [Google Scholar] [PubMed]
- Campus, G.; Rusca, P.; Amrhein, C.; Meier, A.; Zeyer, O.; Wolf, T.G. Career Prospects of Young Dentists in Switzerland. Int. J. Environ. Res. Pub. Health 2020, 17, 4310. [Google Scholar] [CrossRef]
- Kulkarni, S.; Dagli, N.; Duraiswamy, P.; Desai, H.; Vyas, H.; Baroudi, K. Stress and professional burnout among newly graduated dentists. J. Int. Soc. Prev. Community Dent. 2016, 6, 535–541. [Google Scholar] [PubMed] [Green Version]
- Ministry of Health, Labour and Welfare. Survey of Physicians, Dentists, and Pharmacists. Available online: https://www.mhlw.go.jp/toukei/list/33-20_old.html (accessed on 15 October 2020). (In Japanese).
- Shimada, N.; Kondo, T. Estimation of actual report rates using data from the survey of physicians, dentists and pharmacists. Nihon Koshu Eisei Zasshi 2004, 51, 117–132. (In Japanese) [Google Scholar] [PubMed]
- Kodama, T.; Koike, S.; Matsumoto, S.; Ide, H.; Yasunaga, H.; Imamura, T. The working status of Japanese female physicians by area of practice: Cohort analysis of taking leave, returning to work, and changing specialties from 1984 to 2004. Health Policy 2012, 105, 214–220. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Labour and Welfare. Current Status of Clinical Training for Dentists. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/0000085959.html (accessed on 30 August 2020).
- Kuthy, R.A.; Jennings, A.D.; McQuistan, M.R.; Marshall, T.A.; Qian, F. Influence of minor children and contribution to household income on work hours of female dentists. J. Public Health Dent. 2013, 73, 245–251. [Google Scholar] [CrossRef]
- Gallagher, J.E.; Clarke, W.; Eaton, K.A.; Wilson, N.H. Dentistry—A professional contained career in healthcare. A qualitative study of Vocational Dental Practitioners’ professional expectations. BMC Oral Health 2007, 7, 16. [Google Scholar] [CrossRef] [Green Version]
- Kodama, T.; Ida, Y.; Miura, H.A. Nationwide Survey on Working Hours and Working Environment among Hospital Dentists in Japan. Int. J. Environ. Res. Public Health 2020, 17, 9048. [Google Scholar] [CrossRef]
- Karube, H.; Suetaka, T. Operation situation of female dentists of about 50 years of age. Jpn. J. Dent. Prac. Admin. 2006, 41, 180–187. (In Japanese) [Google Scholar]
- Riley, J.L., 3rd; Gordan, V.V.; Rouisse, K.M.; McClelland, J.; Gilbert, G.H. Dental Practice-Based Research Network Collaborative Group. Differences in male and female dentists’ practice patterns regarding diagnosis and treatment of dental caries: Findings from The Dental Practice-Based Research Network. J. Am. Dent. Assoc. 2011, 142, 429–440. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, G.M.; MacDonald, J.K. Gender differences in characteristics, infection control practices, knowledge and attitudes related to HIV among Ontario dentists. Community Dent. Oral. Epidemiol. 1996, 24, 412–415. [Google Scholar] [CrossRef] [PubMed]
- Toyokawa, S.; Kobayashi, Y. Increasing supply of dentists induces their geographic diffusion in contrast with physicians in Japan. Soc. Sci. Med. 2010, 71, 2014–2019. [Google Scholar] [CrossRef] [PubMed]
- Morita, T.; Hashimura, T.; Senoo, Y.; Tanimoto, T. Trend in unequal geographical distribution of dentists by age and gender in Japan from 1996—2014. Community Dent. Health 2019, 36, 195–197. [Google Scholar] [PubMed]
- Ishimaru, M.; Ono, S.; Yasunaga, H.; Matsui, H.; Koike, S. Projected future distribution of dentists in Japan. J. Public Health Dent. 2016, 76, 241–248. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | As of Registration (2006) | At 10 Years after Registration (2016) | ||||||
|---|---|---|---|---|---|---|---|---|
| Men (n = 1680) | Women (n = 984) | Men (n = 1680) | Women (n = 984) | |||||
| Age, mean (standard deviation) | 26.9 | (2.7) | 26.1 | (2.3) | ||||
| Age category, n (%) | ||||||||
| 24–26 | 988 | (58.8) | 738 | (75.0) | ||||
| 27–29 | 484 | (28.8) | 185 | (18.8) | ||||
| 30–32 | 122 | (7.3) | 35 | (3.6) | ||||
| ≥33 | 86 | (5.1) | 26 | (2.6) | ||||
| Work setting, n (%) | ||||||||
| Dental clinic (Owner) | 0 | (0.0) | 0 | (0.0) | 518 | (30.8) | 59 | (6.0) |
| Dental clinic (Employee) | 206 | (12.3) | 99 | (10.1) | 672 | (40.0) | 478 | (48.6) |
| Hospitals | 1284 | (76.4) | 807 | (82.0) | 212 | (12.6) | 118 | (12.0) |
| Other facilities | 2 | (0.1) | 0 | (0.0) | 40 | (2.4) | 24 | (2.4) |
| On career break | 188 | (11.2) | 78 | (7.9) | 238 | (14.2) | 305 | (31.0) |
| Municipalities, n (%) | ||||||||
| Metropolis (pop 500,000+) | 741 | (49.7) | 502 | (55.4) | 583 | (40.4) | 303 | (44.6) |
| Cities (pop 50,000+) | 703 | (47.1) | 387 | (42.7) | 781 | (54.2) | 345 | (50.8) |
| Towns and villages | 48 | (3.2) | 17 | (1.9) | 78 | (5.4) | 31 | (4.6) |
| Working hours, n (%) | ||||||||
| Full-time (≥32 h/week) | 1301 | (91.8) | 399 | (59.6) | ||||
| Part-time (<32 h/week) | 117 | (8.2) | 270 | (40.4) | ||||
| Variable | Men | Women | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Continuous Practice Group (n = 928) | Returned to Practice Group (n = 514) | On Career Break Group (n = 238) | p Value | Continuous Practice Group (n = 365) | Returned to Practice Group (n = 314) | On Career Break Group (n = 305) | p Value | |||||||
| n | (%) | n | (%) | n | (%) | n | (%) | n | (%) | n | (%) | |||
| Age category | ||||||||||||||
| 34–36 | 575 | (62.0) | 285 | (55.4) | 128 | (53.8) | 0.041 /0.060 | 284 | (77.8) | 244 | (77.7) | 210 | (68.8) | 0.532 /0.090 |
| 37–39 | 251 | (27.0) | 156 | (30.4) | 77 | (32.4) | 58 | (15.9) | 55 | (17.5) | 72 | (23.6) | ||
| 40–42 | 57 | (6.1) | 48 | (9.3) | 17 | (7.1) | 15 | (4.1) | 7 | (2.2) | 13 | (4.3) | ||
| ≥43 | 45 | (4.9) | 25 | (4.9) | 16 | (6.7) | 8 | (2.2) | 8 | (2.6) | 10 | (3.3) | ||
| Work setting | ||||||||||||||
| Dental clinics (owner) | 315 | (33.9) | 203 | (39.5) | 0.003 | 25 | (6.8) | 34 | (10.8) | <0.001 | ||||
| Dental clinics (employee) | 431 | (46.4) | 241 | (46.9) | 234 | (64.1) | 244 | (77.7) | ||||||
| Hospitals | 159 | (17.1) | 53 | (10.3) | 90 | (24.7) | 28 | (8.9) | ||||||
| Other facilities | 23 | (2.5) | 17 | (3.3) | 16 | (4.4) | 8 | (2.6) | ||||||
| Municipalities | ||||||||||||||
| Metropolis (pop 500,000+) | 363 | (39.1) | 220 | (42.8) | 0.200 | 157 | (43.0) | 146 | (46.5) | 0.477 | ||||
| Cities (pop 50,000+) | 509 | (54.8) | 272 | (52.9) | 193 | (52.9) | 152 | (48.4) | ||||||
| Towns and villages | 56 | (6.0) | 22 | (4.3) | 15 | (4.1) | 16 | (5.1) | ||||||
| Working hours | ||||||||||||||
| Full-time (≥32 h/week) | 845 | (91.9) | 456 | (91.4) | 0.712 | 244 | (67.8) | 155 | (50.2) | <0.001 | ||||
| Part-time (<32 h/week) | 74 | (8.1) | 43 | (8.6) | 116 | (32.2) | 154 | (49.8) | ||||||
| Variable | All (n = 2121) | Men (n = 1442) | Women (n = 679) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| OR | 95%CI | p Value | OR | 95%CI | p Value | OR | 95%CI | p Value | |
| Gender | |||||||||
| Men | 1.00 | Reference | |||||||
| Women | 1.47 | (1.19–1.81) | <0.001 | ||||||
| Age category | |||||||||
| 34–36 | 1.00 | Reference | 1.00 | Reference | 1.00 | Reference | |||
| 37–39 | 1.19 | 0.96–1.47 | 0.116 | 1.24 | (0.96–1.58) | 0.095 | 1.10 | (0.72–1.68) | 0.667 |
| 40–42 | 1.27 | 0.87–1.85 | 0.216 | 1.60 | (1.06–2.41) | 0.027 | 0.53 | (0.20–1.39) | 0.196 |
| ≥43 | 1.03 | 0.65–1.62 | 0.910 | 1.05 | (0.63–1.75) | 0.862 | 0.97 | (0.34–2.77) | 0.959 |
| Work setting | |||||||||
| Dental clinics (Owner) | 2.65 | (1.93–3.62) | <0.001 | 1.94 | (1.34–2.80) | <0.001 | 5.39 | (2.69–10.80) | <0.001 |
| Dental clinics (Employee) | 2.22 | (1.67–2.94) | <0.001 | 1.71 | (1.20–2.43) | 0.003 | 3.10 | (1.93–4.99) | <0.001 |
| Hospitals | 1.00 | Reference | 1.00 | Reference | 1.00 | Reference | |||
| Other facilities | 2.06 | (1.16–3.64) | 0.013 | 2.18 | (1.08–4.43) | 0.031 | 1.88 | (0.72–4.95) | 0.200 |
| Municipalities | |||||||||
| Metropolis (pop 500,000+) | 1.22 | (1.01–1.47) | 0.039 | 1.17 | (0.93–1.48) | 0.167 | 1.33 | (0.96–1.85) | 0.086 |
| Cities (pop 50,000+) | 1.00 | Reference | 1.00 | Reference | 1.00 | Reference | |||
| Towns and villages | 0.89 | (0.58–1.35) | 0.573 | 0.72 | (0.43–1.22) | 0.223 | 1.26 | (0.59–2.69) | 0.548 |
| Working hours | |||||||||
| Full-time (≥32 h/week) | 1.00 | Reference | 1.00 | Reference | 1.00 | Reference | |||
| Part-time (<32 h/week) | 1.64 | (1.28–2.11) | <0.001 | 1.15 | (0.76–1.73) | 0.503 | 2.07 | (1.48–2.88) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oshima, K.; Kodama, T.; Ida, Y.; Miura, H. Gender Differences in Work Status during Early Career of Dentists: An Analysis of National Survey Cohort Data of 10 Years in Japan. Int. J. Environ. Res. Public Health 2021, 18, 2335. https://doi.org/10.3390/ijerph18052335
Oshima K, Kodama T, Ida Y, Miura H. Gender Differences in Work Status during Early Career of Dentists: An Analysis of National Survey Cohort Data of 10 Years in Japan. International Journal of Environmental Research and Public Health. 2021; 18(5):2335. https://doi.org/10.3390/ijerph18052335
Chicago/Turabian StyleOshima, Katsuo, Tomoko Kodama, Yusuke Ida, and Hiroko Miura. 2021. "Gender Differences in Work Status during Early Career of Dentists: An Analysis of National Survey Cohort Data of 10 Years in Japan" International Journal of Environmental Research and Public Health 18, no. 5: 2335. https://doi.org/10.3390/ijerph18052335
APA StyleOshima, K., Kodama, T., Ida, Y., & Miura, H. (2021). Gender Differences in Work Status during Early Career of Dentists: An Analysis of National Survey Cohort Data of 10 Years in Japan. International Journal of Environmental Research and Public Health, 18(5), 2335. https://doi.org/10.3390/ijerph18052335