
Social Media Use and Body Image Disorders: Association between Frequency of Comparing One’s Own Physical Appearance to That of People Being Followed on Social Media and Body Dissatisfaction and Drive for Thinness




Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethics Statements
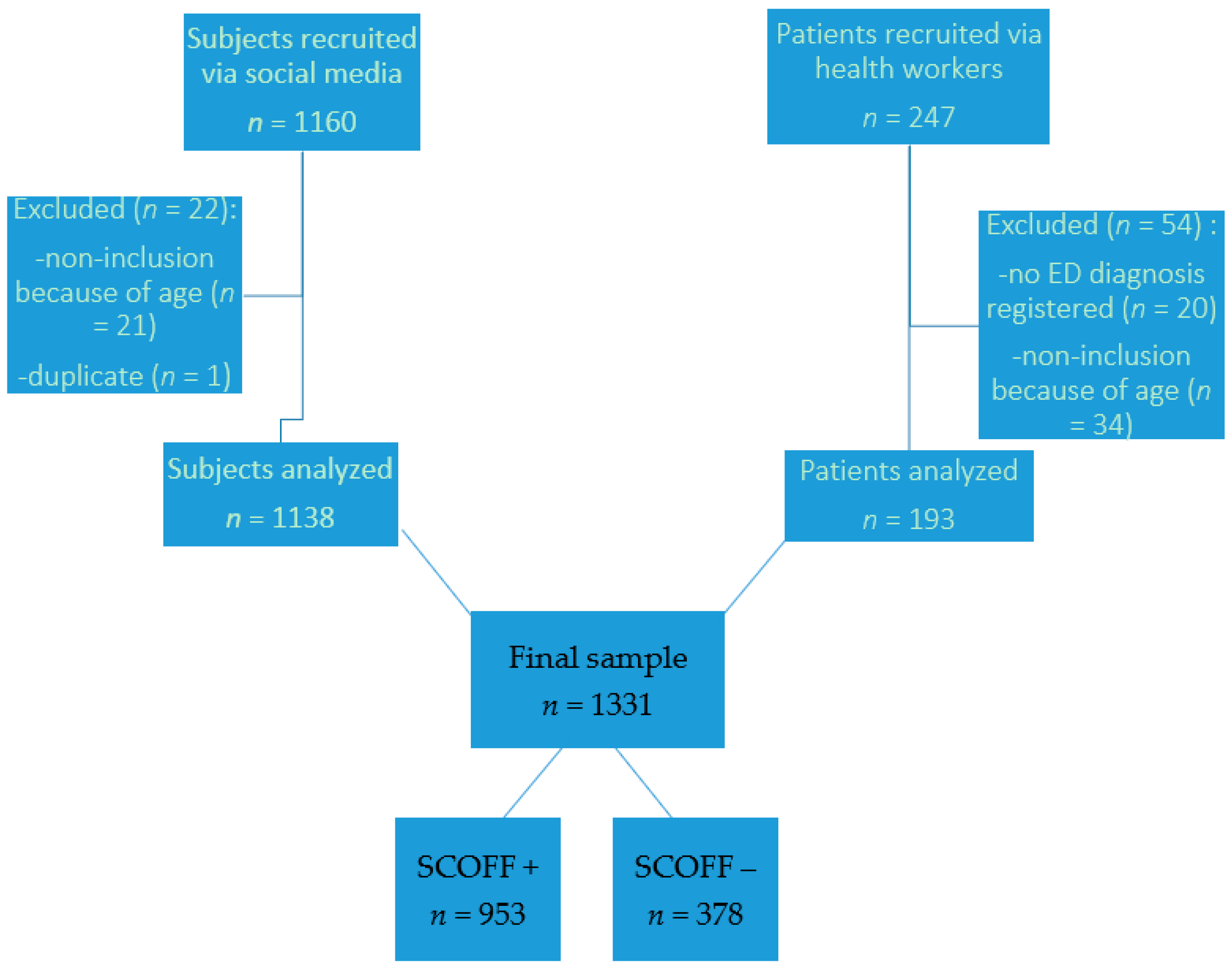
2.2. Participants Recruitment
2.3. Evaluation
2.3.1. General Data
2.3.2. Social Media Use
2.3.3. Body Image
2.3.4. ED Screening
2.4. Statistical Analysis
3. Results
3.1. Population Description
3.2. Comparing Participants Based on Their ED Screening
3.3. Association between the Frequency of Comparing One’s Own Physical Appearance to That of People Followed on Social Media and EDI Body Dissatisfaction and Drive for Thinness
4. Discussion
4.1. Discussing the Main Results
4.2. Study’s Strengths and Weaknesses
4.3. Perspectives
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Blowers, L.C.; Loxton, N.J.; Grady-Flesser, M.; Occhipinti, S.; Dawe, S. The relationship between sociocultural pressure to be thin and body dissatisfaction in preadolescent girls. Eat. Behav. 2003, 4, 229–244. [Google Scholar] [CrossRef]
- Anschutz, D.; van Strien, T.; Engels, R. Exposure to slim images in mass media: Television commercials as reminders of restriction in restrained eaters. Health Psychol. 2008, 27, 401–408. [Google Scholar] [CrossRef] [Green Version]
- Laure, P.; Binsinger, C.; Friser, A.; Ambard, M.; Girault, S. L’estime de soi et l’anxiété sont-elles prédictives de la consommation de substances psychoactives par les préadolescents? Psychotropes 2005, 11, 73–90. [Google Scholar] [CrossRef]
- Stice, E.; Shaw, H.E. Role of body dissatisfaction in the onset and maintenance of eating pathology: A synthesis of research findings. J. Psychosom. Res. 2002, 53, 985–993. [Google Scholar] [CrossRef]
- Gorwood, P.; Blanchet-Collet, C.; Chartrel, N.; Duclos, J.; Dechelotte, P.; Hanachi, M.; Fetissov, S.; Godart, N.; Melchior, J.C.; Ramoz, N.; et al. New insights in anorexia nervosa. Front. Neurosci. 2016, 10, 256. [Google Scholar] [CrossRef] [Green Version]
- Stormer, S.M.; Thompson, J.K. Explanations of body image disturbance: A test of maturational status, negative verbal commentary, social comparison, and sociocultural hypotheses. Int. J. Eat. Disord. 1996, 19, 193–202. [Google Scholar] [CrossRef]
- Jacobi, C.; Hayward, C.; de Zwaan, M.; Kraemer, H.C.; Agras, W.S. Coming to terms with risk factors for eating disorders: Application of risk terminology and suggestions for a general taxonomy. Psychol. Bull. 2004, 130, 19–65. [Google Scholar] [CrossRef] [PubMed]
- Windauer, U.; Lennerts, W.; Talbot, P.; Touyz, S.; Beumont, P.J.V. How well are « cured » anorexia nervosa patients? An investigation of 16 weight-recovered anorexic patients. Br. J. Psychiatry J. Ment. Sci. 1993, 163, 195–200. [Google Scholar] [CrossRef]
- Taylor, C.B.; Bryson, S.; Doyle, A.A.C.; Luce, K.H.; Cunning, D.; Abascal, L.B.; Rockwell, R.; Field, A.E.; Striegel-Moore, R.; Winzelberg, A.J.; et al. The adverse effect of negative comments about weight and shape from family and siblings on women at high risk for eating disorders. Pediatrics 2006, 118, 731–738. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ohring, R.; Graber, J.; Brooks-Gunn, J. Girls’ recurrent and concurrent body dissatisfaction: Correlates and consequences over 8 years. Int. J. Eat. Disord. 2002, 31, 404–415. [Google Scholar] [CrossRef]
- Thompson, J.K.; Heinberg, L.J.; Altabe, M.; Tantleff-Dunn, S. Exacting Beauty: Theory, Assessment, and Treatment of Body Image Disturbance; American Psychological Association: Washington, DC, USA, 1999. [Google Scholar]
- Attie, I.; Brooks-Gunn, J. Development of eating problems in adolescent girls: A longitudinal study. Dev. Psychol. 1989, 25, 70–79. [Google Scholar] [CrossRef]
- Killen, J.D.; Taylor, C.B.; Hayward, C.; Haydel, K.F.; Wilson, D.M.; Hammer, L.; Kraemer, H.; Blair-Greiner, A.; Strachowski, D. Weight concerns influence the development of eating disorders: A 4-year prospective study. J. Consult. Clin. Psychol. 1996, 64, 936–940. [Google Scholar] [CrossRef]
- Ricciardelli, L.A.; McCabe, M.P.; Holt, K.E.; Finemore, J. A biopsychosocial model for understanding body image and body change strategies among children. J. Appl. Dev. Psychol. 2003, 24, 475–495. [Google Scholar] [CrossRef]
- Ricciardelli, L.; McCabe, M.; Lillis, J.; Thomas, K. a longitudinal investigation of the development of weight and muscle concerns among preadolescent boys. J. Youth Adolesc. 2006, 35, 168–178. [Google Scholar] [CrossRef]
- Williamson, D.A.; Cubic, B.A.; Gleaves, D.H. Equivalence of body image disturbances in anorexia and bulimia nervosa. J. Abnorm. Psychol. 1993, 102, 177–180. [Google Scholar] [CrossRef] [PubMed]
- Wilfley, D.E.; Schwartz, M.B.; Spurrell, E.B.; Fairburn, C.G. Using the eating disorder examination to identify the specific psychopathology of binge eating disorder. Int. J. Eat. Disord. 2000, 27, 259–269. [Google Scholar] [CrossRef]
- Stice, E.; Schupak-Neuberg, E.; Shaw, H.E.; Stein, R.I. Relation of media exposure to eating disorder symptomatology: An examination of mediating mechanisms. J. Abnorm. Psychol. 1994, 103, 836–840. [Google Scholar] [CrossRef] [PubMed]
- Stice, E.; Agras, W.S. Predicting onset and cessation of bulimic behaviors during adolescence: A longitudinal grouping analysis. Behav. Ther. 1998, 29, 257–276. [Google Scholar] [CrossRef]
- McKee, S.; Smith, H.J.; Koch, A.; Balzarini, R.; Georges, M.; Callahan, M.P. Looking up and seeing green: Women’s everyday experiences with physical appearance comparisons. Psychol. Women Q. 2013, 37, 351–365. [Google Scholar] [CrossRef]
- Corning, A.; Krumm, A.; Smitham, L. Differential social comparison processes in women with and without eating disorder symptoms. J. Couns. Psychol. 2006, 53, 338–349. [Google Scholar] [CrossRef]
- Dittmar, H.; Howard, S. Thin-ideal internalization and social comparison tendency as moderators of media models’ impact on women’s body-focused anxiety. J. Soc. Clin. Psychol. 2004, 23, 768–791. [Google Scholar] [CrossRef]
- Tiggemann, M.; Polivy, J.; Hargreaves, D. The processing of thin ideals in fashion magazines: A source of social comparison or fantasy? J. Soc. Clin. Psychol. 2009, 28, 73–93. [Google Scholar] [CrossRef] [Green Version]
- Field, A.E.; Camargo, C.A.; Taylor, C.B.; Berkey, C.S.; Colditz, G.A. Relation of peer and media influences to the development of purging behaviors among preadolescent and adolescent girls. Arch. Pediatr. Adolesc. Med. 1999, 153, 1184–1189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Vries, D.A.; Peter, J.; de Graaf, H.; Nikken, P. Adolescents’ social network site use, peer appearance-related feedback, and body dissatisfaction: Testing a mediation model. J. Youth Adolesc. 2016, 45, 211–224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fardouly, J.; Willburger, B.; Vartanian, L.R. Instagram use and young women’s body image concerns and self-objectification: Testing mediational pathways. New Media Soc. 2018, 20, 1380–1395. [Google Scholar] [CrossRef] [Green Version]
- Melioli, T.; Gonzalez, N.; El Jazouli, Y.; Valla, A.; Girard, M.; Chabrol, H.; Rodgers, R.F. Utilisation d’Instagram, aptitude à critiquer les médias et symptômes de troubles du comportement alimentaire chez les adolescentes: Une étude exploratoire. J. Thérapie Comport. Cogn. 2018, 28, 196–203. [Google Scholar] [CrossRef]
- Duggan, M. The Demographics of Social Media Users in 2015; Pew Research Center: Washington, DC, USA, 2015. [Google Scholar]
- Korff-Sausse, S. Selfies: Narcissisme ou autoportrait? Adolescence 2016, 34, 623–632. [Google Scholar] [CrossRef]
- Garner, D.M. Eating Disorder Inventory-2: Professional Manual; Psychological Assessment Resources: Odessa, FL, USA, 1991. [Google Scholar]
- Criquillon-Doublet, S.; Divac, S.; Dardennes, R.; Guelfi, J.D. Le “Eating Disorder Inventory” (EDI); Psychopathologie Quantitative; Masson: Paris, France, 1995; pp. 249–260. [Google Scholar]
- Luck, A.J.; MorganLuck, J.F.; Reid, F.; O’Brien, A.; Brunton, J.; Price, C.; Perry, L.; Lacey, J.H. The SCOFF questionnaire and clinical interview for eating disorders in general practice: Comparative study. BMJ 2002, 325, 755–756. [Google Scholar] [CrossRef] [Green Version]
- Garcia, F.D.; Grigioni, S.; Allais, E.; Houy-Durand, E.; Thibaut, F.; Déchelotte, P. Detection of eating disorders in patients: Validity and reliability of the French version of the SCOFF questionnaire. Clin. Nutr. 2011, 30, 178–181. [Google Scholar] [CrossRef]
- Holland, G.; Tiggemann, M. A systematic review of the impact of the use of social networking sites on body image and disordered eating outcomes. Body Image 2016, 17, 100–110. [Google Scholar] [CrossRef]
- Moscone, A.-L. Troubles de L’image du Corps et Troubles Psychologiques Associés dans L’anorexie Mentale: Mécanismes Sous-jacents et Proposition de Régulation par les Activités Physiques Adaptées. Ph.D. Thesis, Université Paris Sud-Paris, Orsay, France, 2013. [Google Scholar]
- Leahey, T.M.; Crowther, J.H.; Ciesla, J.A. An ecological momentary assessment of the effects of weight and shape social comparisons on women with eating pathology, high body dissatisfaction, and low body dissatisfaction. Behav. Ther. 2011, 42, 197–210. [Google Scholar] [CrossRef] [Green Version]
- Ridgway, J.L.; Clayton, R.B. Instagram unfiltered: Exploring associations of body image satisfaction, instagram #selfie posting, and negative romantic relationship outcomes. Cyberpsychol. Behav. Soc. Netw. 2016, 19, 2–7. [Google Scholar]
- Groesz, L.M.; Levine, M.P.; Murnen, S.K. The effect of experimental presentation of thin media images on body satisfaction: A meta-analytic review. Int. J. Eat. Disord. 2002, 31, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Tiggemann, M.; Slater, A. NetGirls: The Internet, Facebook, and body image concern in adolescent girls. Int. J. Eat. Disord. 2013, 46, 630–633. [Google Scholar] [CrossRef] [PubMed]
- Brown, Z.; Tiggemann, M. Attractive celebrity and peer images on Instagram: Effect on women’s mood and body image. Body Image 2016, 19, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Ho, S.; Lee, E.; Liao, Y. Social network sites, friends, and celebrities: The roles of social comparison and celebrity involvement in adolescents body image dissatisfaction. Soc. Media Soc. 2016, 2. [Google Scholar] [CrossRef] [Green Version]
- Festinger, L. A theory of social comparison processes. Hum. Relat. 1954, 7, 117–140. [Google Scholar] [CrossRef]
- Grogan, S. Body Image: Understanding Body Dissatisfaction in Men, Women and Children; Routledge, Taylor and Francis Group: Abington, UK, 2016. [Google Scholar]
- Boëtsch, G.; Andrieu, B.; Le Breton, D.; Pomarède, N.; Vigarello, G. Corps en Formes; CNRS Editions: Paris, France, 2011; p. 298. [Google Scholar]
- Fredrickson, B.; Roberts, T.-A. Objectification theory: Toward understanding women’s lived experiences and mental health risks. Psychol. Women Q. 1997, 21, 173–206. [Google Scholar] [CrossRef]
- Harper, B.; Tiggemann, M. The effect of thin ideal media images on women’s self-objectification, mood, and body image. Sex Roles 2008, 58, 649–657. [Google Scholar] [CrossRef]
- Haynos, A.F.; Watts, A.W.; Loth, K.A.; Pearson, C.M.; Neumark-Stzainer, D. Factors predicting an escalation of restrictive eating during adolescence. J. Adolesc. Health 2016, 59, 391–396. [Google Scholar] [CrossRef] [Green Version]
- Neumark-Sztainer, D.; Paxton, S.J.; Hannan, P.J.; Haines, J.; Story, M. Does body satisfaction matter? Five-year longitudinal associations between body satisfaction and health behaviors in adolescent females and males. J. Adolesc. Health 2006, 39, 244–251. [Google Scholar] [CrossRef] [PubMed]
- Fisher, M.; Golden, N.H.; Katzman, D.K.; Kreipe, R.E.; Rees, J.; Schebendach, J.; Sigman, G.; Ammerman, S.; Hoberman, H.M. Eating disorders in adolescents: A background paper. J. Adolesc. Health 1995, 16, 420–437. [Google Scholar] [CrossRef]
- Williamson, D.A.; Muller, S.L.; Reas, D.L.; Thaw, J.M. Cognitive bias in eating disorders: Implications for theory and treatment. Behav. Modif. 1999, 23, 556–577. [Google Scholar] [CrossRef] [PubMed]
- Stice, E.; Shaw, H.; Burton, E.; Wade, E. Dissonance and healthy weight eating disorder prevention programs: A randomized efficacy trial. J. Consult. Clin. Psychol. 2006, 74, 263–275. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Drive for Thinness | Always (=3) | Usually (=2) | Often (=1) | Sometimes (=0) | Seldom (=0) | Never (=0) |
|---|---|---|---|---|---|---|
| 1—I eat sweets and carbohydrates without feeling nervous | □ | □ | □ | □ | □ | □ |
| 2—I think about dieting | □ | □ | □ | □ | □ | □ |
| 3—I feel extremely guilty after overeating | □ | □ | □ | □ | □ | □ |
| 4—I am terrified of gaining weight | □ | □ | □ | □ | □ | □ |
| 5—I exaggerate or magnify the importance of weight | □ | □ | □ | □ | □ | □ |
| 6—I am preoccupied with the desire to be thinner | □ | □ | □ | □ | □ | □ |
| 7—If I gain a pound, I worry that I will keep gaining | □ | □ | □ | □ | □ | □ |
| Body Dissatisfaction | Always | Usually | Often | Sometimes | Seldom | Never |
| 1—I think that my stomach is too big (+) | □ | □ | □ | □ | □ | □ |
| 2—I think that my thighs are too large (+) | □ | □ | □ | □ | □ | □ |
| 3—I think that my stomach is just the right size (−) | □ | □ | □ | □ | □ | □ |
| 4—I feel satisfied with the shape of my body (−) | □ | □ | □ | □ | □ | □ |
| 5—I like the shape of my buttocks (−) | □ | □ | □ | □ | □ | □ |
| 6—I think my hips are too big (+) | □ | □ | □ | □ | □ | □ |
| 7—I think that my thighs are just the right size (−) | □ | □ | □ | □ | □ | □ |
| 8—I think my buttocks are too large (+) | □ | □ | □ | □ | □ | □ |
| 9—I think that my hips are just the right size (−) | □ | □ | □ | □ | □ | □ |
| Yes | No | |
|---|---|---|
| 1—Do you make yourself sick because you feel uncomfortably full? | □ | □ |
| 2—Do you worry you have lost control over how much you eat? | □ | □ |
| 3—Have you recently lost over 1 stone (14 lb) in a 3-month period? | □ | □ |
| 4—Do you believe yourself to be fat when others say you are too thin? | □ | □ |
| 5—Would you say that food dominates your life? | □ | □ |
| Final Sample (n = 1331) | SCOFF− (n = 378) | SCOFF+ (n = 953) | p Value | ||||
|---|---|---|---|---|---|---|---|
| Mean or Number of Participants | Standard Deviation or Percentage | Mean or Number of Participants | Standard Deviation or Percentage | Mean or Number of Participants | Standard Deviation or Percentage | ||
| SOCIODEMOGRAPHIC CHARACTERISTICS | |||||||
| Age | 24.2 | 4.2 | 25.1 | 4.2 | 23.9 | 4.2 | <0.001 *** |
| (Student’s t-test) | |||||||
| Sex | 0.012 * | ||||||
| Female | 1300 | 97.7% | 363 | 96.0% | 937 | 98.3% | (Chi-squared test) |
| Male | 31 | 2.3% | 15 | 4.0% | 16 | 1.7% | |
| Studies level | <0.001 *** | ||||||
| Less than Level 12 | 71 | 5.3% | 16 | 4% | 55 | 6% | (Chi-squared test) |
| Level 12 | 229 | 17.2% | 62 | 16% | 167 | 18% | |
| Level 12 + 2 years | 208 | 15.6% | 50 | 13% | 158 | 17% | |
| Level 12 + 3 (Bachelor’s degree) | 320 | 24.0% | 89 | 24% | 231 | 24% | |
| Level 12 + 5 (Master’s degree) | 380 | 0.285 | 96 | 25% | 284 | 30% | |
| Degree over Level 12 + 5 | 123 | 0.092 | 65 | 17% | 58 | 6% | |
| SOCIAL MEDIA USE | |||||||
| Frequency | <0.001 *** | ||||||
| Max. once a day | 64 | 5% | 17 | 4% | 47 | 5% | (Chi-squared test) |
| 2 to 10 times a day | 578 | 43% | 194 | 51% | 384 | 40% | |
| 10 to 20 times a day | 439 | 33% | 115 | 30% | 324 | 34% | |
| Over 20 times a day | 250 | 19% | 52 | 14% | 198 | 21% | |
| Time spent | 0.010 ** | ||||||
| Less than 1 h | 232 | 17% | 81 | 21% | 151 | 16% | (Chi-squared test) |
| Between 1 and 5 h | 1048 | 79% | 289 | 76% | 759 | 80% | |
| Over 5 h | 51 | 4% | 8 | 2% | 43 | 5% | |
| Body comparison | <0.001 *** | ||||||
| Never | 33 | 2% | 18 | 5% | 15 | 2% | (Chi-squared test) |
| Seldom | 114 | 9% | 56 | 15% | 58 | 6% | |
| Sometimes | 317 | 24% | 130 | 34% | 187 | 20% | |
| Often | 523 | 39% | 133 | 35% | 390 | 41% | |
| Always | 344 | 26% | 41 | 11% | 303 | 32% | |
| Posting selfies | <0.001 *** | ||||||
| Never | 457 | 34% | 146 | 39% | 311 | 33% | (Fisher exact test) |
| 1 or 2 times a month | 756 | 57% | 199 | 53% | 557 | 58% | |
| Once a week | 93 | 7% | 24 | 6% | 69 | 7% | |
| 3 to 4 times a week | 18 | 1% | 7 | 2% | 11 | 1% | |
| Daily | 7 | 1% | 2 | 1% | 5 | 1% | |
| EATING DISORDERS | |||||||
| EDI-BD | 12.4 | 7.5 | 7.9 | 6.6 | 14.2 | 7 | <0.001 *** |
| (Student test) | |||||||
| EDI-DT | 8.9 | 6 | 4.1 | 4.2 | 10.8 | 5.5 | <0.001 *** |
| (Student test) | |||||||
| Average BMI | 22.3 | 4.2 | 22.2 | 3.5 | 22.3 | 4.5 | 0.575 |
| (Student test) | |||||||
| Categories of BMI | <0.001 *** | ||||||
| <17.5 | 96 | 7.2% | 9 | 2.4% | 87 | 9.1% | (Chi-squared test) |
| [17.5–25] | 981 | 73.7% | 306 | 81.0% | 675 | 70.8% | |
| ≥25 | 254 | 19.1% | 63 | 16.7% | 191 | 20.0% | |
| Chi-Squared Test | p-Value | |
|---|---|---|
| Frequency of comparing one’s own physical appearance | 38.165 | 0.008 ** |
| Estimates | p-Value | |
|---|---|---|
| Intercept | 13.620 | <2 × 10−16 *** |
| Studies level: Less than level 12 | ||
| Studies level: Level 12 | −0.672 | 0.507 |
| Studies level: Level 12 + 2 years | −0.778 | 0.447 |
| Studies level: Level 12 + 3 (Bachelor’s degree) | −1.560 | 0.110 |
| Studies level: Level 12 + 5 (Master’s degree) | −1.307 | 0.175 |
| Degree over Level 12 + 5 | −2.538 | 0.022 * |
| Estimates | p-Value | |
|---|---|---|
| Intercept | 10.141 | <2 × 10−16 *** |
| Studies level: Less than level 12 | ||
| Studies level: Level 12 | −0.730 | 0.368 |
| Studies level: Level 12 + 2 years | −0.477 | 0.561 |
| Studies level: Level 12 + 3 (Bachelor’s degree) | −1.328 | 0.090 |
| Studies level: Level 12 + 5 (Master’s degree) | −1.451 | 0.061 |
| Degree over Level 12 + 5 | −3.019 | 0.0007 *** |
| Estimates | p-Value | |
|---|---|---|
| Intercept | 21.109 | <2 × 10−16 *** |
| Body comparison: Never | ||
| Body comparison: Seldom | 1.002 | 0.233 |
| Body comparison: Sometimes | 1.049 | 0.177 |
| Body comparison: Often | 1.155 | 0.130 |
| Body comparison: Always | 1.384 | 0.074 |
| Coefficient de Correlation de Pearson Avec son IC à 95% | p-Value | |
|---|---|---|
| EDI-DT | 0.071 [0.017; 0.1239] | 0.0099 ** |
| EDI-BD | 0.253 [0.202; 0.302] | <0.001 *** |
| Estimates | p-Value | |
|---|---|---|
| Intercept | 5.859 | 8.7 × 10−8 *** |
| Body comparison: Never | ||
| Body comparison: Seldom | 0.438 | 0.678 |
| Body comparison: Sometimes | 2.021 | 0.038 * |
| Body comparison: Often | 5.314 | 3.4 × 10−8 *** |
| Body comparison: Always | 8.421 | <2.2 × 10−16 *** |
| Studies level: Less than level 12 | ||
| Studies level: Level 12 | −1.399 | 0.053 |
| Studies level: Level 12 + 2 years | −1.415 | 0.0539 |
| Studies level: Level 12 + 3 (Bachelor’s degree) | −1.723 | 0.0138 * |
| Studies level: Level 12 + 5 (Master’s degree) | −1.999 | 0.0038 ** |
| Degree over Level 12 + 5 | −2.936 | 0.0002 *** |
| Estimates | p-Value | |
|---|---|---|
| Intercept | 9.087 | 1.1 × 10−10 *** |
| Body comparison: Never | ||
| Body comparison: Seldom | 1.225 | 0.365 |
| Body comparison: Sometimes | 1.768 | 0.158 |
| Body comparison: Often | 5.564 | 6.5 × 10−6 *** |
| Body comparison: Always | 9.226 | 2.4 × 10−13 *** |
| Studies level: Less than level 12 | ||
| Studies level: Level 12 | −1.437 | 0.122 |
| Studies level: Level 12 + 2 years | −1.785 | 0.058 |
| Studies level: Level 12 + 3 (Bachelor’s degree) | −1.986 | 0.027 * |
| Studies level: Level 12 + 5 (Master’s degree) | −1.940 | 0.029 * |
| Degree over Level 12 + 5 | −2.471 | 0.016 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiotsa, B.; Naccache, B.; Duval, M.; Rocher, B.; Grall-Bronnec, M. Social Media Use and Body Image Disorders: Association between Frequency of Comparing One’s Own Physical Appearance to That of People Being Followed on Social Media and Body Dissatisfaction and Drive for Thinness. Int. J. Environ. Res. Public Health 2021, 18, 2880. https://doi.org/10.3390/ijerph18062880
Jiotsa B, Naccache B, Duval M, Rocher B, Grall-Bronnec M. Social Media Use and Body Image Disorders: Association between Frequency of Comparing One’s Own Physical Appearance to That of People Being Followed on Social Media and Body Dissatisfaction and Drive for Thinness. International Journal of Environmental Research and Public Health. 2021; 18(6):2880. https://doi.org/10.3390/ijerph18062880
Chicago/Turabian StyleJiotsa, Barbara, Benjamin Naccache, Mélanie Duval, Bruno Rocher, and Marie Grall-Bronnec. 2021. "Social Media Use and Body Image Disorders: Association between Frequency of Comparing One’s Own Physical Appearance to That of People Being Followed on Social Media and Body Dissatisfaction and Drive for Thinness" International Journal of Environmental Research and Public Health 18, no. 6: 2880. https://doi.org/10.3390/ijerph18062880
APA StyleJiotsa, B., Naccache, B., Duval, M., Rocher, B., & Grall-Bronnec, M. (2021). Social Media Use and Body Image Disorders: Association between Frequency of Comparing One’s Own Physical Appearance to That of People Being Followed on Social Media and Body Dissatisfaction and Drive for Thinness. International Journal of Environmental Research and Public Health, 18(6), 2880. https://doi.org/10.3390/ijerph18062880