
A Review of Digital Cognitive Behavioral Therapy for Insomnia (CBT-I Apps): Are They Designed for Engagement?


Abstract
:1. Introduction
1.1. Digital Cognitive Behavioral Therapy for Insomnia
1.2. Study Objectives
- Reviewed the existing full-component dCBT-I platforms and produced a detailed content summary,
- Reviewed and summarized published user studies carried out with dCBT-I platforms.
2. Materials and Methods
3. Results
3.1. App Review
- (1)
- Sleepio: The platform is available in English, and it is a web-based application (mobile version is also available), delivering fully-automated CBT-I support.
- (2)
- Shuti Platform: The platform is available in English, developed as a web platform to deliver fully automated CBT-I support.
- (a)
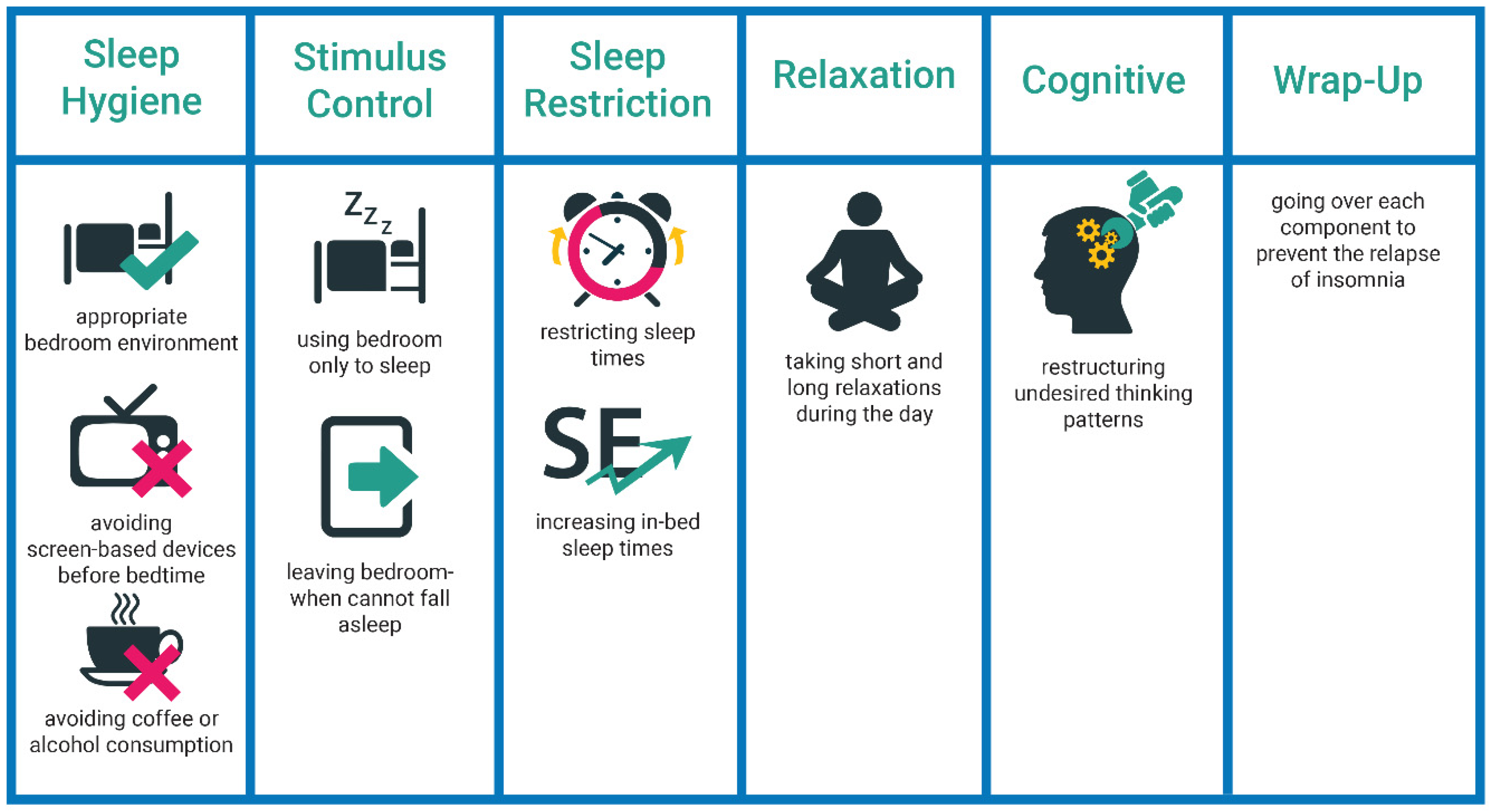
- Sleep Hygiene: CBT-I treatment is introduced through a video presented by an expert, explaining the benefits of the therapy and the prevalence of insomnia. The population at risk is explained, including their gender, emotions, thinking style, medical problems, psychological problems. The impact of insomnia is explained through an interactive checklist about daytime energy, feelings, or mood. Furthermore, there is an interactive sleep hygiene game to spot issues in a hypothetical bedroom; one of such issues, for instance, introducing caffeinated drinks.
- (b)
- Sleep Scheduling: Each module starts with reviewing the sleep diary (total sleep time, total time in bed, and sleep efficiency), and then the user adjusts the arousal time based on preference. The notion of sleep restriction and sleep efficiency and stimulus control are explained in detail. There is also an interactive pop-up panel where the users can adjust the bedtimes and the sleep window to comprehend sleep efficiency. In another pop-up panel, common concerns about sleep restriction therapy and possible negative experiences are interpreted.
- (c)
- Cognitive Therapy: Common thinking errors are explained with interactive exercises, like other peoples’ opinions or personal records of thoughts and beliefs about sleep. Furthermore, strategies to avoid negative thoughts are explained in detail. Additionally, there is an interactive panel that describes the possible reasons for relapse and provides advice on coping with bad nights.
- (3)
- Sleeprate App: The platform is available in English, developed as a mobile app to deliver fully automated CBT-I support.
- (4)
- CBT-I Coach: The platform is available in English, developed as a mobile app to support in-between sessions of traditional CBT-I delivery.
- (5)
- Night Owl: The platform is available in English, developed as a mobile app to deliver fully automated CBT-I support.
- (6)
- Minddistrict: The platform is available in Dutch and Georgian which is also available as a mobile app to deliver fully automated CBT-I support. The platform is also available for clinical monitoring, and user input can be viewed by a personal therapist and the family doctor.
3.2. User Studies
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sateia, M.J. International classification of sleep disorders-third edition highlights and modifications. Chest 2014, 146, 1387–1394. [Google Scholar] [CrossRef]
- Cooper, R. Diagnostic and statistical manual of mental disorders (DSM). Knowl. Organ. 2017, 44, 668–676. [Google Scholar] [CrossRef] [Green Version]
- Morin, C.M.; Drake, C.L.; Harvey, A.G.; Krystal, A.D.; Manber, R.; Riemann, D.; Spiegelhalder, K. Insomnia disorder. Nat. Rev. Dis. Prim. 2015, 1, 15026. [Google Scholar] [CrossRef]
- Espie, C.A. Insomnia: Conceptual Issues in the Development, Persistence, and Treatment of Sleep Disorder in Adults. Annu. Rev. Psychol. 2002, 53, 215–243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Masters, P.A.; Cotton, D.; Rao, J.K.; Taichman, D.; Williams, S. Insomnia. Ann. Intern. Med. 2014, 161. [Google Scholar] [CrossRef]
- Qaseem, A.; Kansagara, D.; Forciea, M.A.; Cooke, M.; Denberg, T.D.; Barry, M.J.; Boyd, C.; Chow, R.D.; Fitterman, N.; Harris, R.P.; et al. Management of chronic insomnia disorder in adults: A clinical practice guideline from the American college of physicians. Ann. Intern. Med. 2016, 165, 125–133. [Google Scholar] [CrossRef]
- Sharma, M.P.; Andrade, C. Behavioral interventions for insomnia: Theory and practice. Indian J. Psychiatry 2012, 54, 359–366. [Google Scholar] [CrossRef] [PubMed]
- Luik, A.I.; Kyle, S.D.; Espie, C.A. Digital Cognitive Behavioral Therapy (dCBT) for Insomnia: A State-of-the-Science Review. Curr. Sleep Med. Rep. 2017, 3, 48–56. [Google Scholar] [CrossRef] [Green Version]
- Bastien, C.H.; Morin, C.M.; Ouellet, M.C.; Blais, F.C.; Bouchard, S. Cognitive-behavioral therapy for insomnia: Comparison of individual therapy, group therapy, and telephone consultations. J. Consult. Clin. Psychol. 2004, 72, 653–659. [Google Scholar] [CrossRef]
- Swift, N.; Stewart, R.; Andiappan, M.; Smith, A.; Espie, C.A.; Brown, J.S.L. The effectiveness of community day-long CBT-I workshops for participants with insomnia symptoms: A randomised controlled trial. J. Sleep Res. 2012, 21, 270–280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bjorvatn, B.; Fiske, E.; Pallesen, S. A self-help book is better than sleep hygiene advice for insomnia: A randomized controlled comparative study. Scand. J. Psychol. 2011, 52, 580–585. [Google Scholar] [CrossRef]
- Espie, C.A.; Hames, P.; McKinstry, B. Use of the internet and mobile media for delivery of cognitive behavioral insomnia therapy. Sleep Med. Clin. 2013, 8, 407–419. [Google Scholar] [CrossRef]
- Gratzer, D.; Khalid-Khan, F.; Balasingham, S. The Internet and CBT: A New Clinical Application of an Effective Therapy. In Cognitive Behavioral Therapy and Clinical Applications; Intechopen: London, UK, 2018. [Google Scholar]
- Zhu, H.; Luo, Y.; Choe, E.K. Making Space for the Quality Care: Opportunities for Technology in Cognitive Behavioral Therapy for Insomnia. In Proceedings of the 2017 CHI Conference on Human Factors in Computing Systems; ACM: New York, 2017; pp. 5773–5786. [Google Scholar]
- Beun, R.J. Persuasive strategies in mobile insomnia therapy: Alignment, adaptation, and motivational support. Pers. Ubiquitous Comput. 2013, 17, 1187–1195. [Google Scholar] [CrossRef] [Green Version]
- Bastien, C.H.; Vallières, A.; Morin, C.M. Validation of the insomnia severity index as an outcome measure for insomnia research. Sleep Med. 2001, 2, 297–307. [Google Scholar] [CrossRef]
- Seyffert, M.; Lagisetty, P.; Landgraf, J.; Chopra, V.; Pfeiffer, P.N.; Conte, M.L.; Rogers, M.A.M. Internet-delivered cognitive behavioral therapy to treat insomnia: A systematic review and meta-analysis. PLoS ONE 2016, 11, e0149139. [Google Scholar] [CrossRef] [PubMed]
- Trauer, J.M.; Qian, M.Y.; Doyle, J.S.; Rajaratnam, S.M.W.; Cunnington, D. Cognitive behavioral therapy for chronic insomnia: A systematic review and meta-analysis. Ann. Intern. Med. 2015, 163, 191–204. [Google Scholar] [CrossRef]
- Meaklim, H.; Abbott, J.A.M.; Kennedy, G.A.; Murray, G.; Klein, B.; Rehm, I. Lessons learned from delivering an internet intervention for insomnia in an Australian public hospital outpatient setting. Aust. Psychol. 2019, 54, 225–234. [Google Scholar] [CrossRef]
- Perski, O.; Blandford, A.; West, R.; Michie, S. Conceptualising engagement with digital behaviour change interventions: A systematic review using principles from critical interpretive synthesis. Transl. Behav. Med. 2017, 7, 254–267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zachariae, R.; Lyby, M.S.; Ritterband, L.M.; O’Toole, M.S. Efficacy of internet-delivered cognitive-behavioral therapy for insomnia—A systematic review and meta-analysis of randomized controlled trials. Sleep Med. Rev. 2016, 30, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuhn, E.; Weiss, B.J.; Taylor, K.L.; Hoffman, J.E.; Ramsey, K.M.; Manber, R.; Gehrman, P.; Crowley, J.J.; Ruzek, J.I.; Trockel, M. CBT-I coach: A description and clinician perceptions of a mobile app for cognitive behavioral therapy for insomnia. J. Clin. Sleep Med. 2016, 12, 597–606. [Google Scholar] [CrossRef] [Green Version]
- Miller, K.E.; Kuhn, E.; Owen, J.E.; Taylor, K.; Yu, J.S.; Weiss, B.J.; Crowley, J.J.; Trockel, M. Clinician Perceptions Related to the Use of the CBT-I Coach Mobile App. Behav. Sleep Med. 2019, 17, 481–491. [Google Scholar] [CrossRef] [PubMed]
- Reilly, E.D.; Robinson, S.A.; Petrakis, B.A.; Kuhn, E.; Pigeon, W.R.; Wiener, R.S.; Keith McInnes, D.; Quigley, K.S. Mobile app use for insomnia self-management: Pilot findings on sleep outcomes in veterans. J. Med. Internet Res. 2019, 8, e12408. [Google Scholar] [CrossRef] [PubMed]
- Chan, C.; West, S.; Glozier, N. Commencing and Persisting with a Web-Based Cognitive Behavioral Intervention for Insomnia: A Qualitative Study of Treatment Completers. J. Med. Internet Res. 2017, 19, e37. [Google Scholar] [CrossRef] [PubMed]
- Espie, C.A.; Kyle, S.D.; Williams, C.; Ong, J.C.; Douglas, N.J.; Hames, P.; Brown, J.S.L. A Randomized, Placebo-Controlled Trial of Online Cognitive Behavioral Therapy for Chronic Insomnia Disorder Delivered via an Automated Media-Rich Web Application. Sleep 2012, 35, 769–781. [Google Scholar] [CrossRef]
- Elison, S.; Ward, J.; Williams, C.; Espie, C.; Davies, G.; Dugdale, S.; Ragan, K.; Chisnall, L.; Lidbetter, N.; Smith, K. Feasibility of a UK community-based, eTherapy mental health service in Greater Manchester: Repeated-measures and between-groups study of “Living Life to the Full Interactive”, “Sleepio” and “Breaking Free Online” “Self Help Services”. BMJ Open 2017, 7, e016392. [Google Scholar] [CrossRef] [PubMed]
- Ritterband, L.M.; Thorndike, F.P.; Gonder-Frederick, L.A.; Magee, J.C.; Bailey, E.T.; Saylor, D.K.; Morin, C.M. Efficacy of an internet-based behavioral intervention for adults with insomnia. Arch. Gen. Psychiatry 2009, 66, 692–698. [Google Scholar] [CrossRef]
- Baharav, A.; Eyal, S. Self-help for insomnia in the mobile era. J. Sleep Res. 2016, 25, 306. [Google Scholar]
- Harbison, B.R.; Cole, J.; Wetzler, R.; Gorzynski, A. Evaluation of a CBT-I self-help program administered by a mobile app. Sleep 2018, 41, A155. [Google Scholar] [CrossRef] [Green Version]
- Okujava, N.; Malashkhia, N.; Shagidze, S.; Tsereteli, A.; Arevadze, B.; Chikhladze, N.; de Weerd, A.; Van Straten, A. Digital cognitive behavioral therapy for insomnia—The first Georgian version. Can we use it in practice? Internet Interv. 2019, 17, 100244. [Google Scholar] [CrossRef]
- Van Straten, A.; Emmelkamp, J.; De Wit, J.; Lancee, J.; Andersson, G.; Van Someren, E.J.W.; Cuijpers, P. Guided Internet-delivered cognitive behavioural treatment for insomnia: A randomized trial. Psychol. Med. 2014, 44, 1521–1532. [Google Scholar] [CrossRef]
- Koffel, E.; Kuhn, E.; Petsoulis, N.; Erbes, C.R.; Anders, S.; Hoffman, J.E.; Ruzek, J.I.; Polusny, M.A. A randomized controlled pilot study of CBT-I Coach: Feasibility, acceptability, and potential impact of a mobile phone application for patients in cognitive behavioral therapy for insomnia. Health Inform. J. 2018, 24, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Ross, P.R.; Wensveen, S.A.G. Designing behavior in interaction: Using aesthetic experience as a mechanism for design. Int. J. Des. 2010, 4, 3–13. [Google Scholar]
- Hassenzahl, M. The interplay of beauty, goodness, and usability in interactive products. Hum. Comput. Interact. 2004, 19, 319–349. [Google Scholar] [CrossRef]
- Deterding, S.; Dixon, D.; Khaled, R.; Nacke, L. From game design elements to gamefulness: Defining “gamification”. In Proceedings of the 15th International Academic MindTrek Conference: Envisioning Future Media Environments, MindTrek 2011, Tampere, Finland, 28–30 September 2011. [Google Scholar]
- Li, J.; Van Der Spek, E.; Hu, J.; Feijs, L. SEE ME ROAR: Self-determination enhanced engagement for math education relying on augmented reality. In Proceedings of the CHI PLAY 2017 Extended Abstracts—Extended Abstracts Publication of the Annual Symposium on Computer-Human Interaction in Play, Amsterdam, The Netherlands, 15–18 October 2017; ACM: New York, NY, USA. [Google Scholar]
- Erten-Uyumaz, B.; Ahuja, M.; Vacaretu, T.; Rama, M.D.; Overeem, S.; Visser, T.; Hu, J.; Feijs, L. Design and evaluation of a negotiation-based sleep scheduler app for insomnia treatment. In Proceedings of the ACM International Conference Proceeding Series; ACM: New York, NY, USA, 2019. [Google Scholar]
- Erten-Uyumaz, B.; Overeem, S.; Feijs, L.; Rama, M.D.; Hu, J. A digital sleep restriction system for insomnia therapy based on sleep window shift negotiation. In Proceedings of the ACM International Conference Proceeding Series; ACM: New York, NY, USA, 2018. [Google Scholar]
- Uyumaz, B.E.; Hendrikx, R.; Quaedackers, L.; Feijs, L.; Rama, M.D.; Overeem, S.; Hu, J. An interactive thought visualization tool for insomnia treatment. In Proceedings of the Procedia Computer Science; Elsevier: Amsterdam, The Netherlands, 2017. [Google Scholar]
- Uyumaz, B.E.; Uyumaz, U.; Rama, M.D.; Overeem, S.; Hu, J.; Feijs, L. The Thought Journal App: Designed to confront thoughts that influence sleep. In Proceedings of the ACM International Conference Proceeding Series, Atlanta, GA, USA, 18–20 May 2020; ACM: New York, NY, USA, 2020. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Published Studies | [26,27] | [25,28] | [29] | [22,23,24,33] | [30] | [31,32] |
|---|---|---|---|---|---|---|
| CBT-I Elements | SHT, SC, SR, RT, CT and RP. | SHT, SC, SR, RT, CT and RP. | SHT, SC, SR, RT and RP. | SHT, SC, SR, RT, CT and RP. | SHT, SC, SR, RT, and CT. | SHT, SC, SR, CT and RP. |
| Presentation style | Textual, graphics, animation videos, interactive quizzes, and list of summaries. | Textual information, visual and interactive pop-up panels, and vignettes. | Interactive and animative videos, visualizations, reminders. | Textual information and graphics organized in tabs. | Textual information and graphics organized in tabs, interactive checklist and videos. | The information is presented as text, picture and videos. There are interactive sections. |
| Support type | Fully automated | Fully automated | Fully automated | Digital CBT-I as support | Fully automated | Guided digital CBT-I |
| Language | English | English | English | English | English | Dutch/Georgian |
| Platform | Sleepio | Shuti | SleepRate | CBT-I Coach | Night Owl | Minddistrict |
| Platform | Advantages | Disadvantages |
|---|---|---|
| Sleepio | The information is divided as modules, there are visually pleasing animative videos, summaries and recaps, competition certificate. | Interactivity is low, content lacking scientific depth |
| Shuti | Available as modules, interactive and playful games, scientifically rich explanations | Too much text |
| Sleeprate | Collects information from multiple sensors (i.e., sleep diary, voice recorder) | Too many reminders, discrepancy between behavioral and cognitive components |
| CBT-I Coach | Rich amount of advices on bedtime and waketime, information is tailored based on a checklist, a rich content is available on relaxation and content training | There is no guidance on sleep restriction, there are technical issues, old fashioned user interface |
| Night Owl | Rich and informative content on sleep education training | The information is too scientific and technically described, lacking user-centered communication |
| Minddistrict | Interactive panels are available on modules, there are relaxation exercises. Diaries for sleep and thoughts are available | Limited in feedback and graphical summaries |
| Article/Platform | Participant Number | Mean Age (SD) | Gender | Mental Health Condition | Treating CBT-I Patients | Benefits |
|---|---|---|---|---|---|---|
| Kuhn et al., 2016 [22]/CBT-I Coach | 138 (VA 1 -Trained CBT-I) clinicians | 47.73 (10.86) | 97 f, 41 m | N/a | 3.36/week | Outcome, compliance, adherence (more) |
| Miller et al., 2019 [23]/CBT-I Coach | 108 (VA Trained CBT-I) clinicians | 48.53 years (SD = 11.56) | 77 f, 31 m | N/a | 5/week | Positive, engagement, compliance |
| Chan et al., 2017 [25]/Shuti | 39 (depressed) patients | 59 years (N/a) | 39 m | 33 major depressive disorder (DSM-5 2 criteria), 13 self-reported cognitive complaints | N/a | Understand factors, challenge misperceptions (more) |
| Meaklim et al., 2018 [19]/Shuti | 10 (sleep) patients | 52.4 years (SD = 13.7) | 4 m, 6 f | Insomnia Severity Scores (ISI) were (M = 17.5, SD = 4.3) | N/a | Sleep diary is informative |
| Espie et al., 2012 [26]/Sleepio | 164 (insomnia) patients | >18 years | 44 m, 120 f. | N/a | N/a | Low dropout rates |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Erten Uyumaz, B.; Feijs, L.; Hu, J. A Review of Digital Cognitive Behavioral Therapy for Insomnia (CBT-I Apps): Are They Designed for Engagement? Int. J. Environ. Res. Public Health 2021, 18, 2929. https://doi.org/10.3390/ijerph18062929
Erten Uyumaz B, Feijs L, Hu J. A Review of Digital Cognitive Behavioral Therapy for Insomnia (CBT-I Apps): Are They Designed for Engagement? International Journal of Environmental Research and Public Health. 2021; 18(6):2929. https://doi.org/10.3390/ijerph18062929
Chicago/Turabian StyleErten Uyumaz, Begum, Loe Feijs, and Jun Hu. 2021. "A Review of Digital Cognitive Behavioral Therapy for Insomnia (CBT-I Apps): Are They Designed for Engagement?" International Journal of Environmental Research and Public Health 18, no. 6: 2929. https://doi.org/10.3390/ijerph18062929
APA StyleErten Uyumaz, B., Feijs, L., & Hu, J. (2021). A Review of Digital Cognitive Behavioral Therapy for Insomnia (CBT-I Apps): Are They Designed for Engagement? International Journal of Environmental Research and Public Health, 18(6), 2929. https://doi.org/10.3390/ijerph18062929