
An Orthodontic Approach for Garre’s Sclerosing Osteomyelitis of the Mandible

 , , ,
, , ,  ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Case Presentation
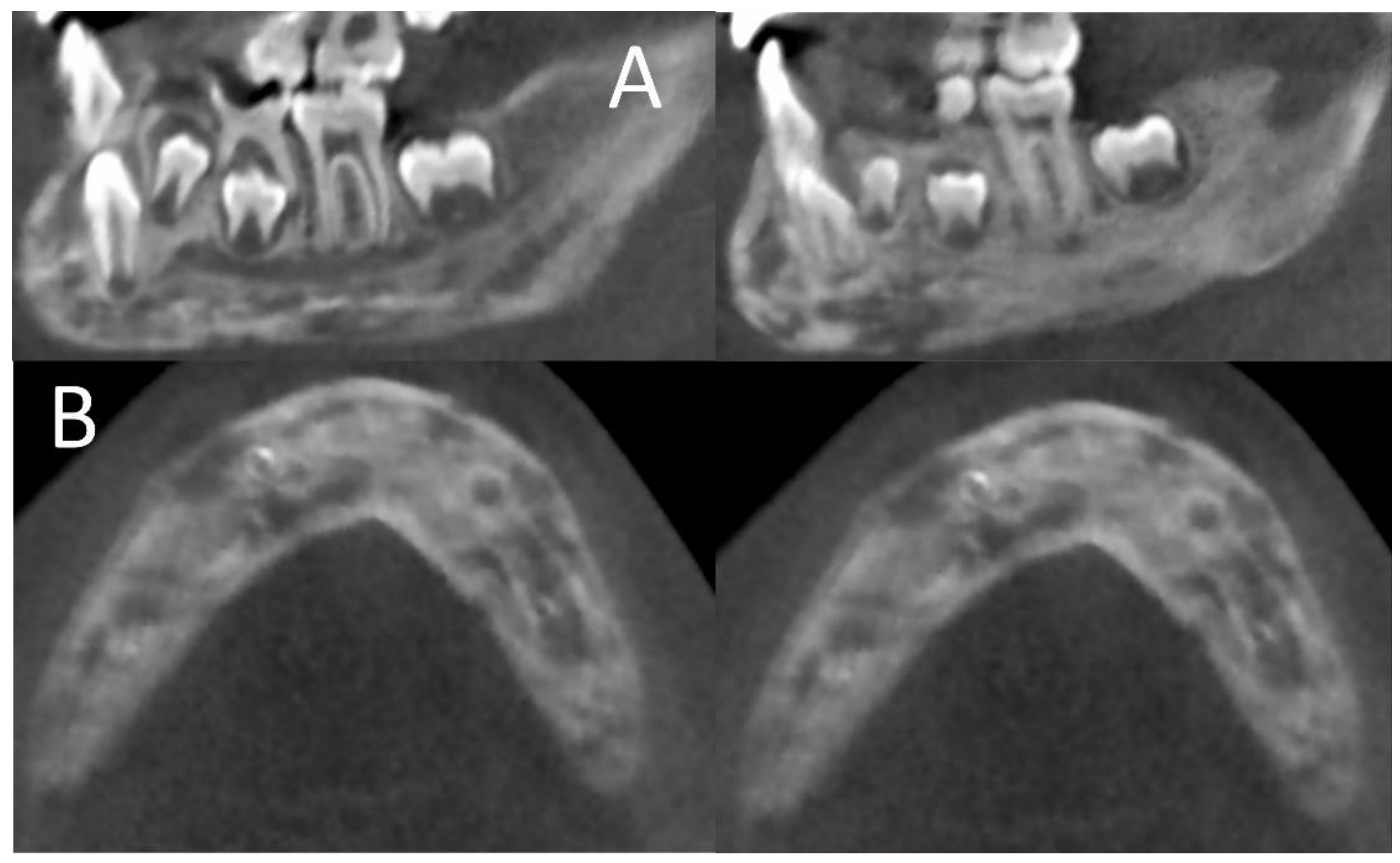
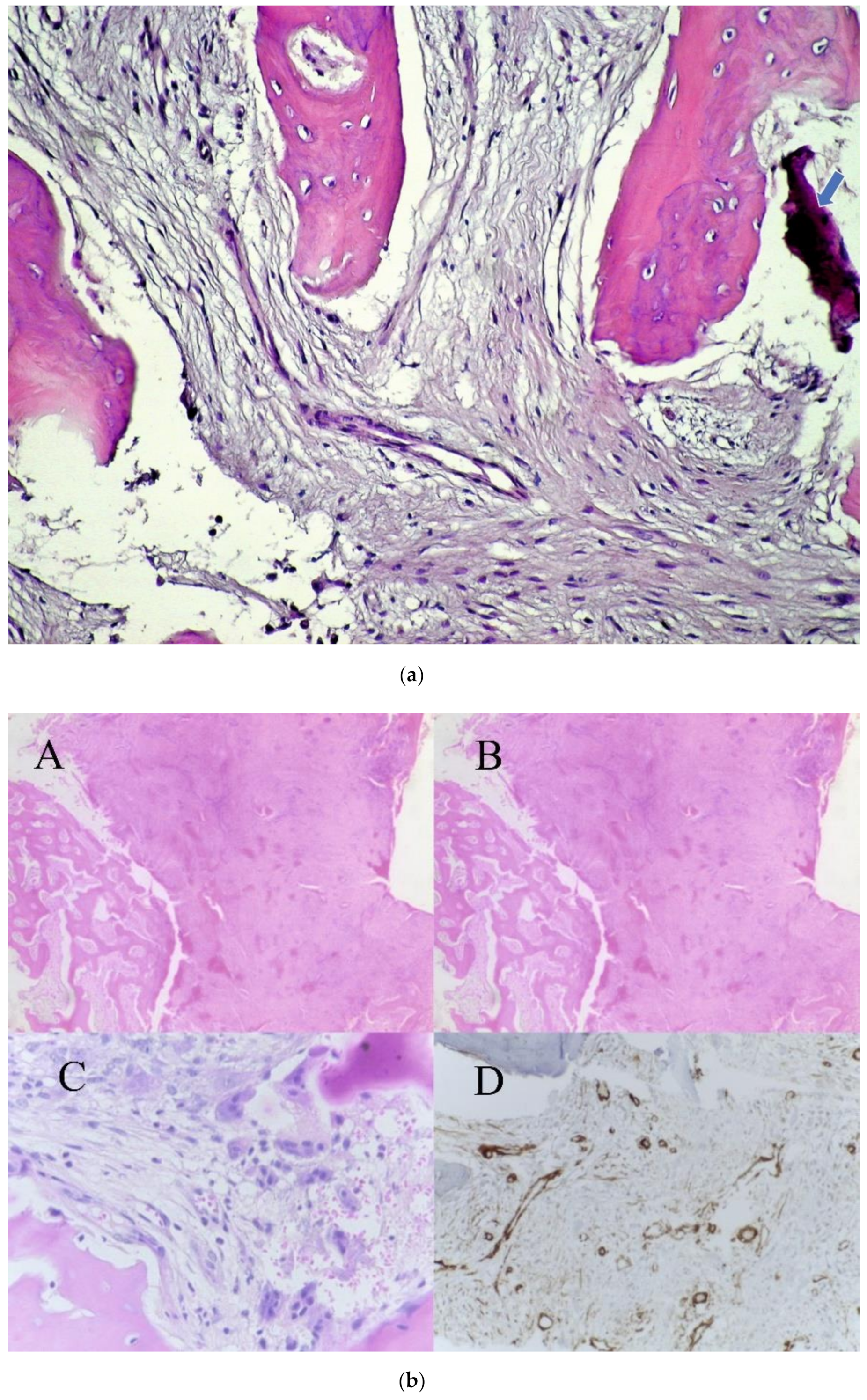
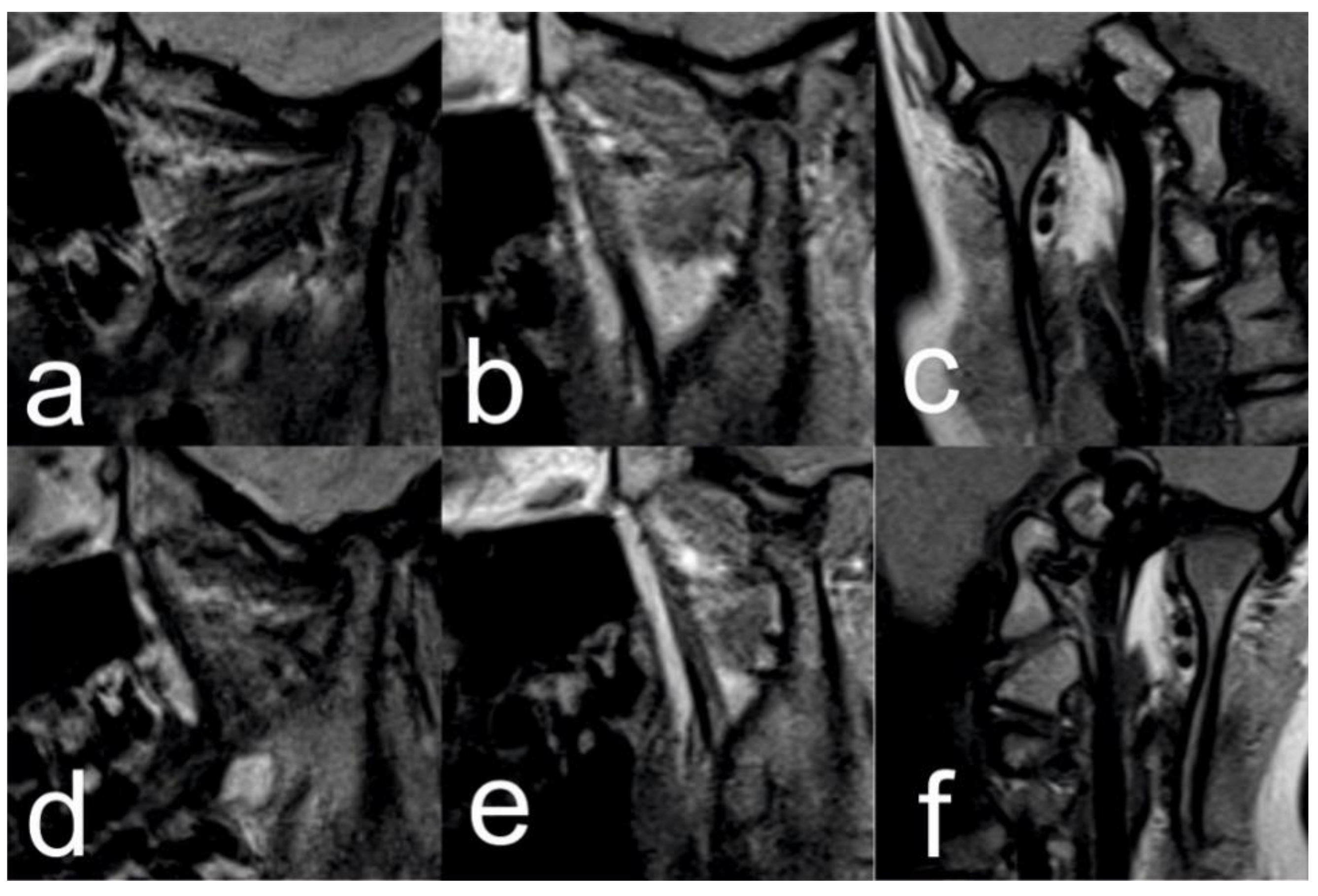
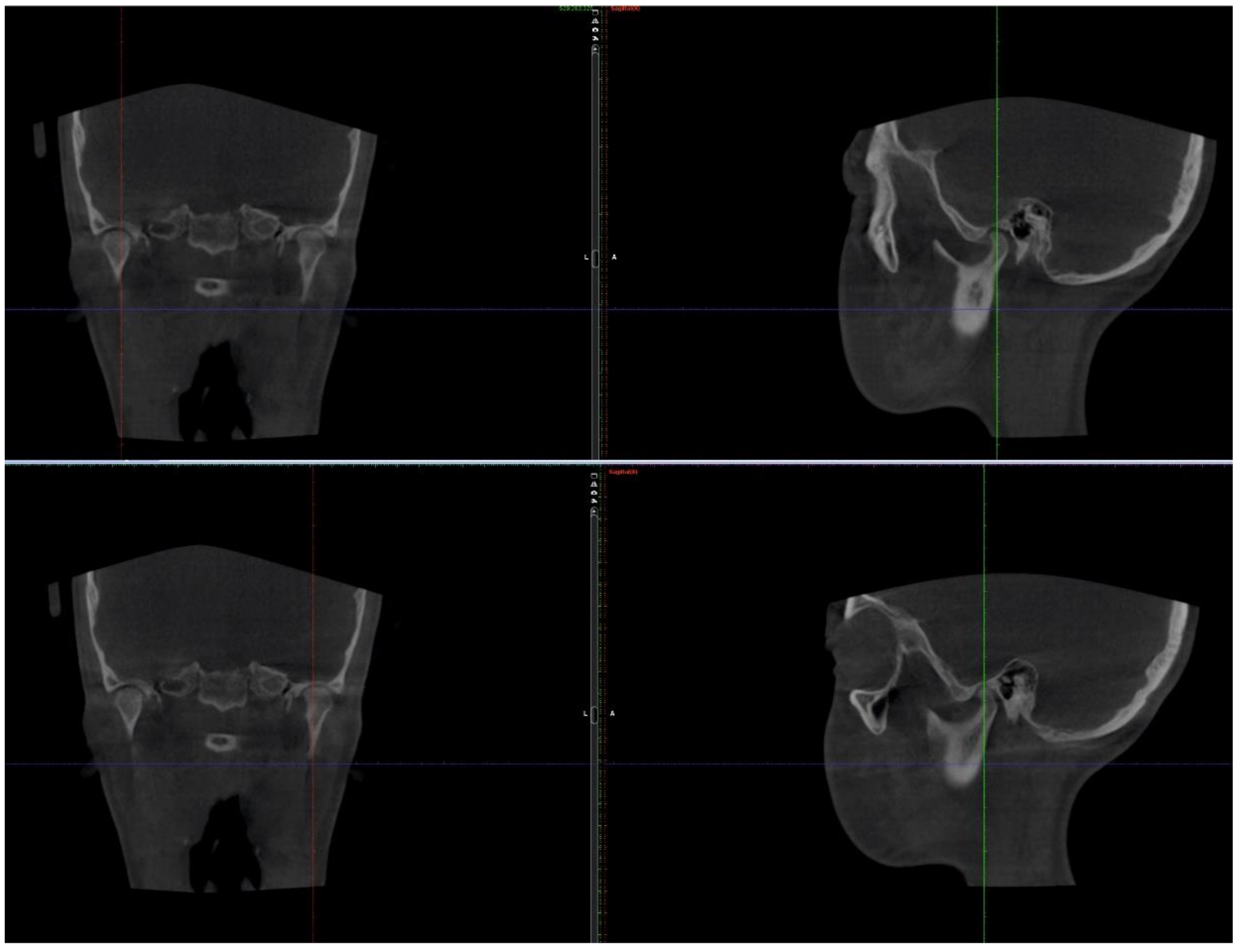
2.1. Initial Diagnosis and Initial Surgical Management
2.2. Orthodontic Treatment
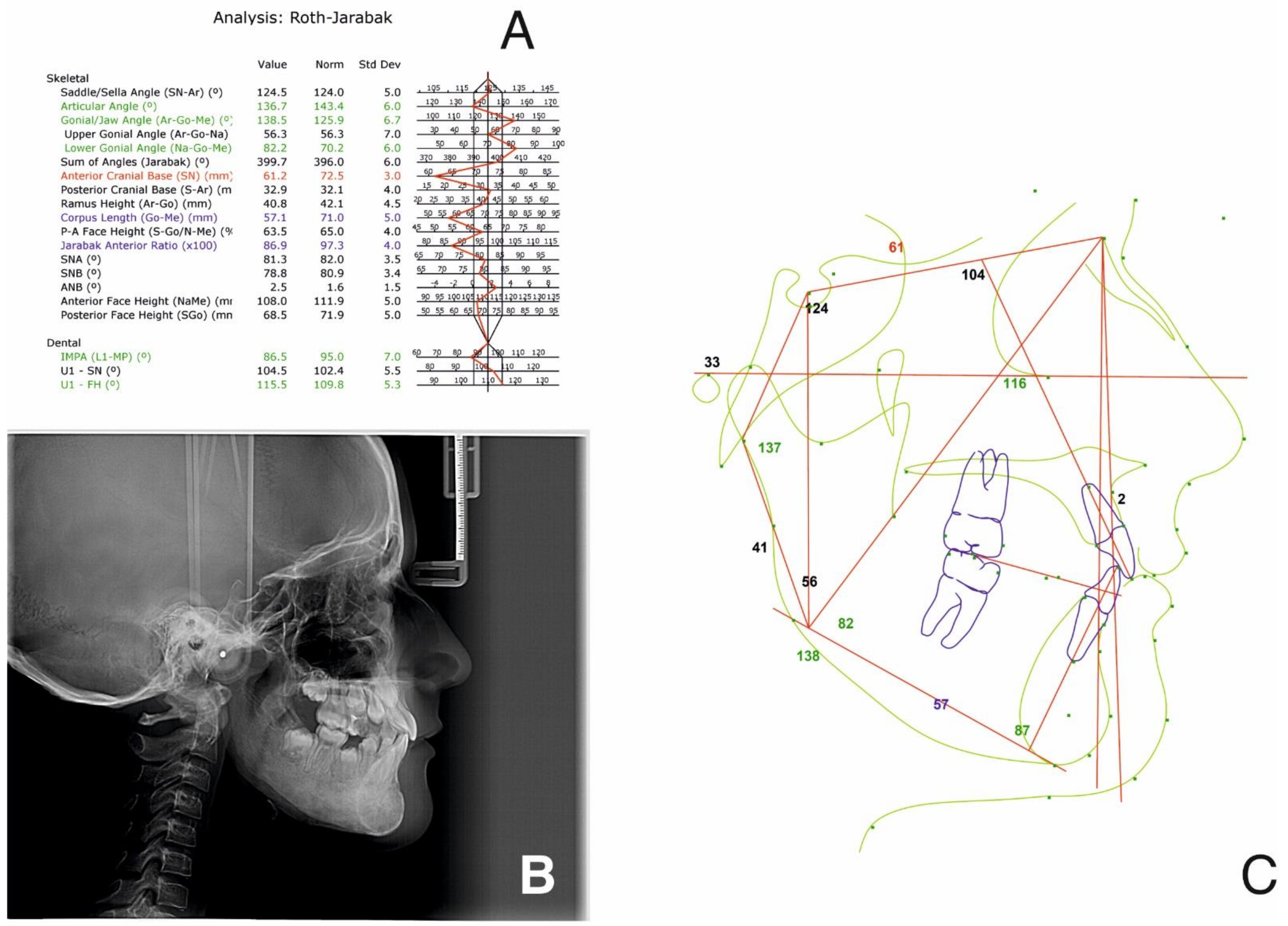
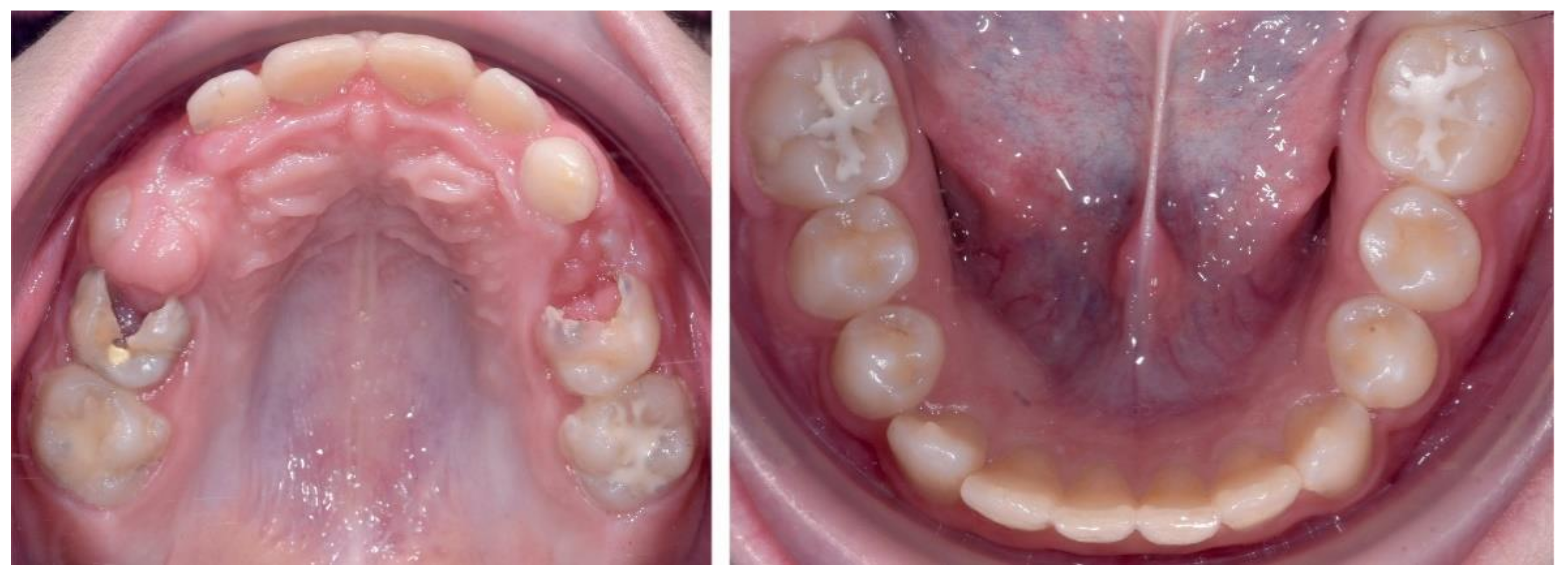
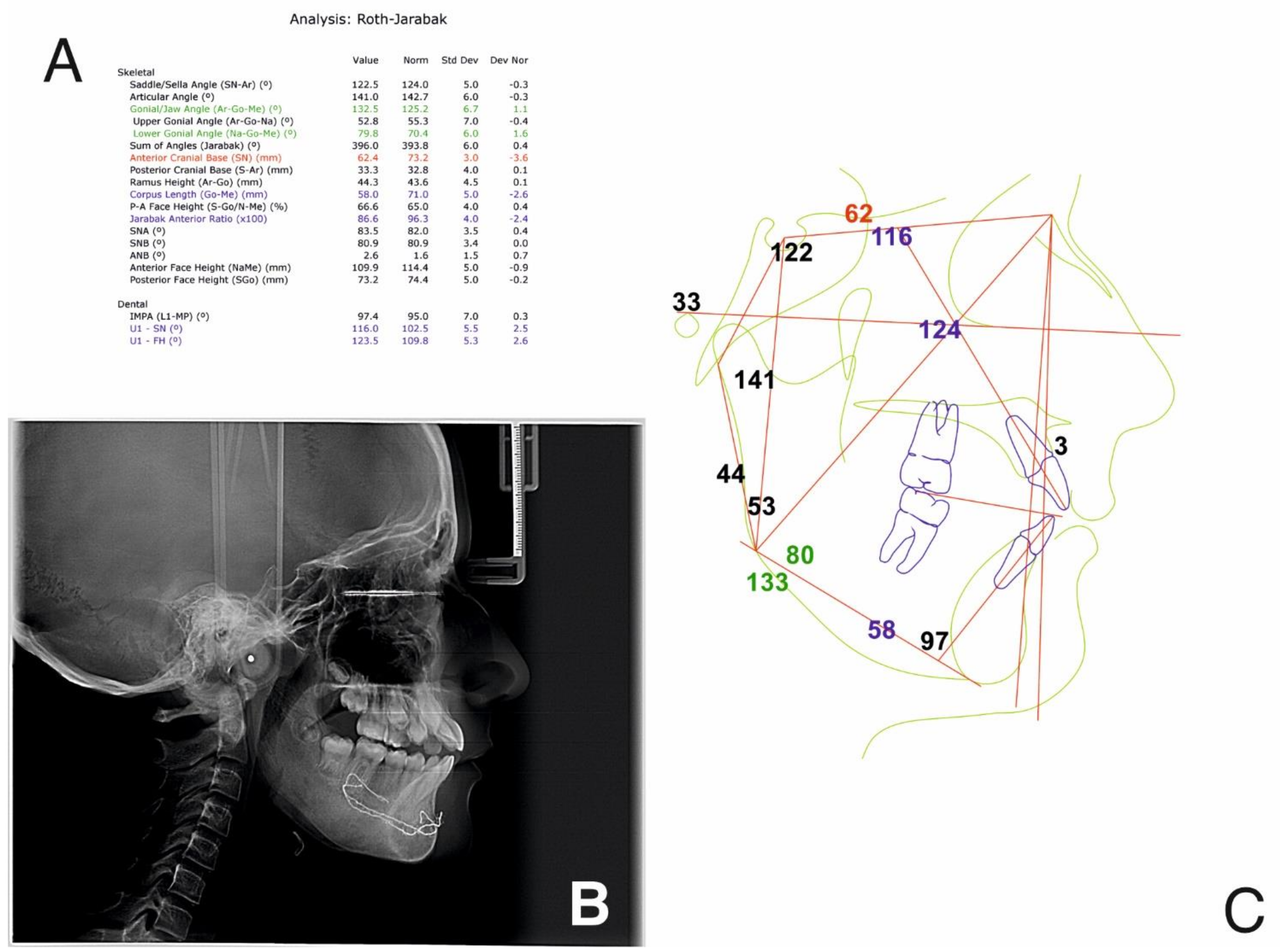
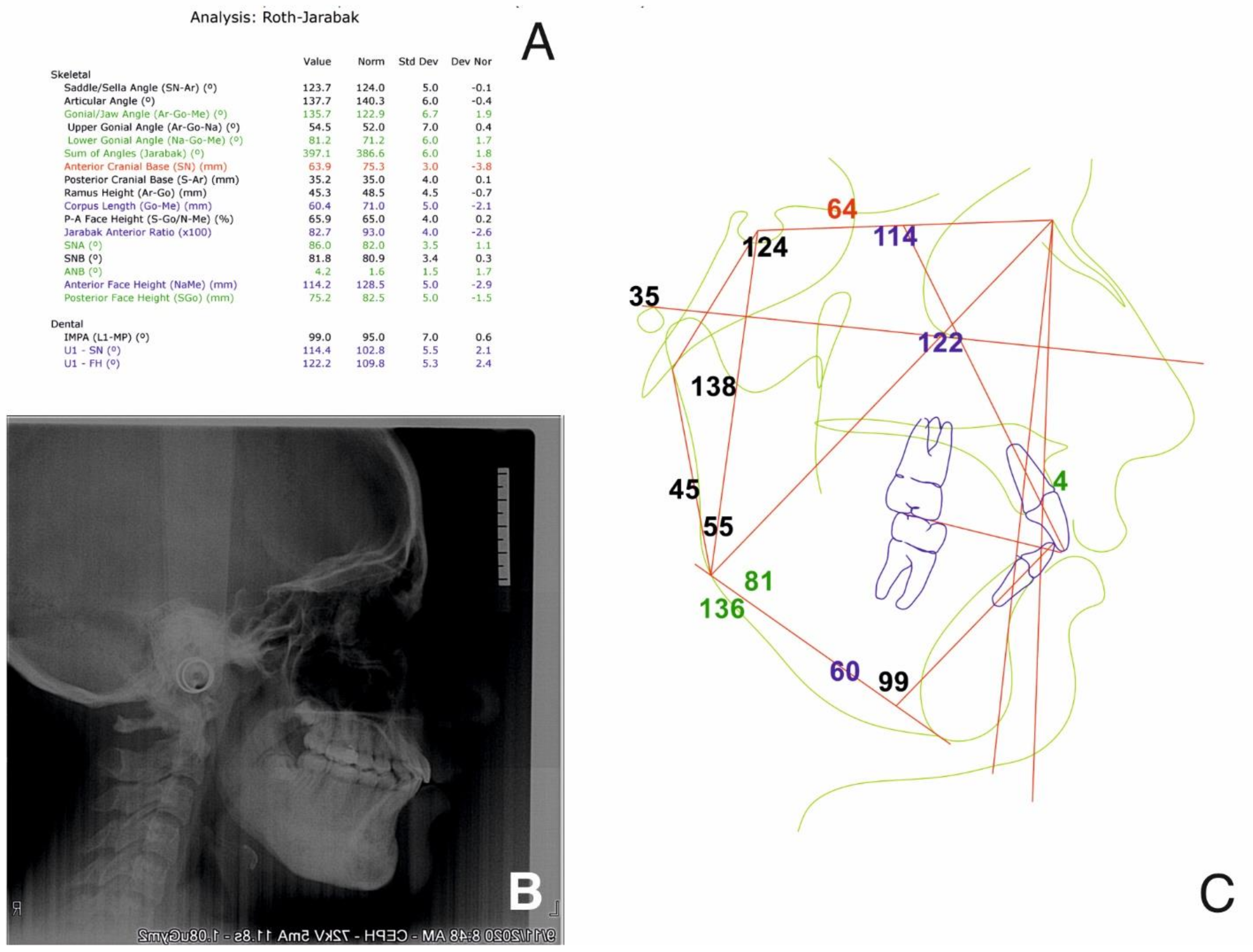
2.2.1. Initial Examination
2.2.2. Treatment Objectives
- Relieve the TMJ pain, stabilize the mandible and muscle relaxation (physiotherapy and splint therapy);
- Orthopedic treatment to ensure a normal growth and development of the maxilla and the mandible, and the correct eruption of the permanent teeth (class I for canine and molar);
- Diminishing the growth of the inferior lower third of the face;
- Limiting the evolution of the osteomyelitis process by preventing further invasive treatment of the patient (braces, skeletal anchorage, any other forces that are beyond physiological which might increase the osteomyelitis process);
- Deconditioning of the tongue trust and nail biting and improving oral hygiene.
2.2.3. Treatment Planning and Treatment Alternatives
2.3. Treatment Progress
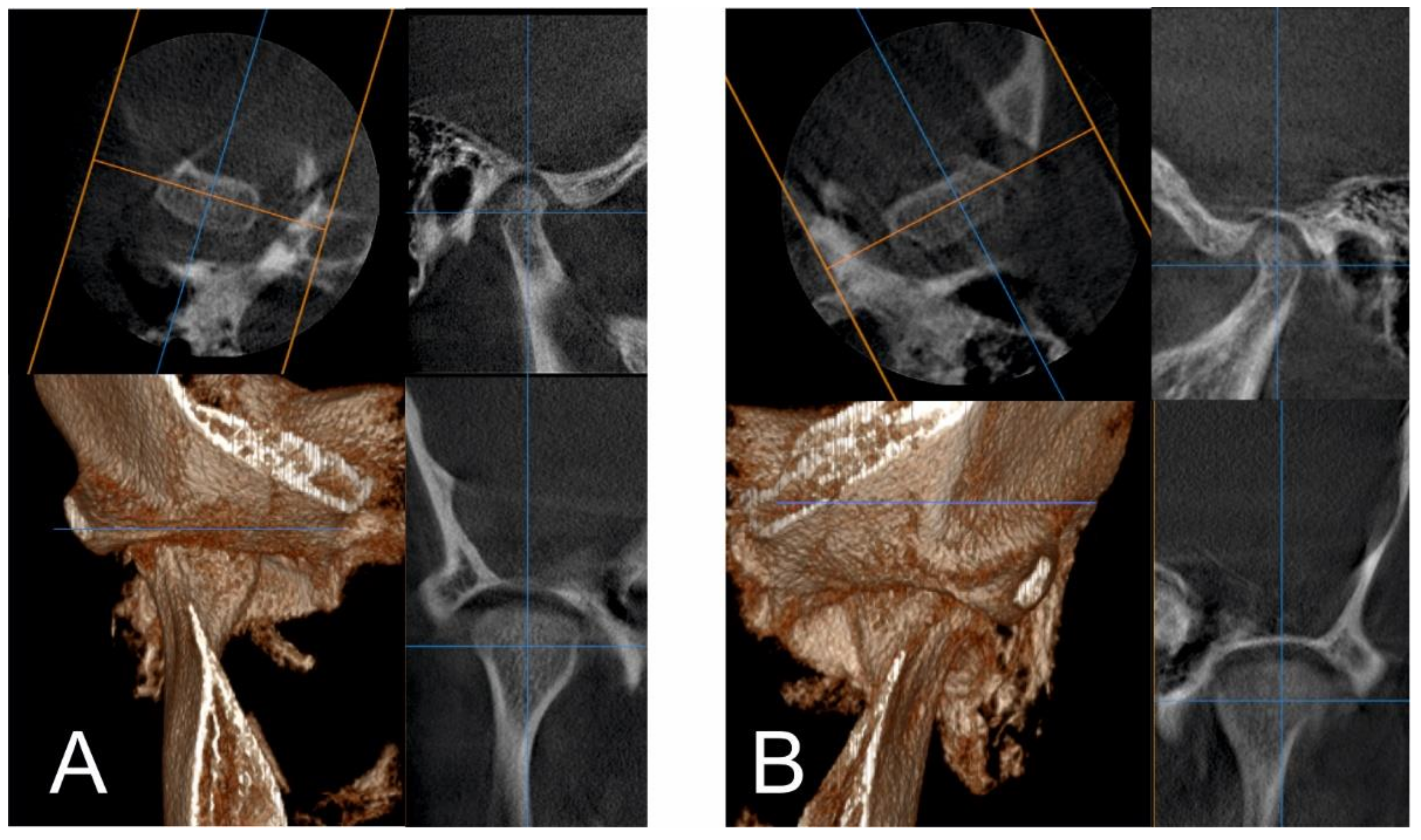
2.3.1. First Treatment Phase—2016—TMJ Splint Therapy
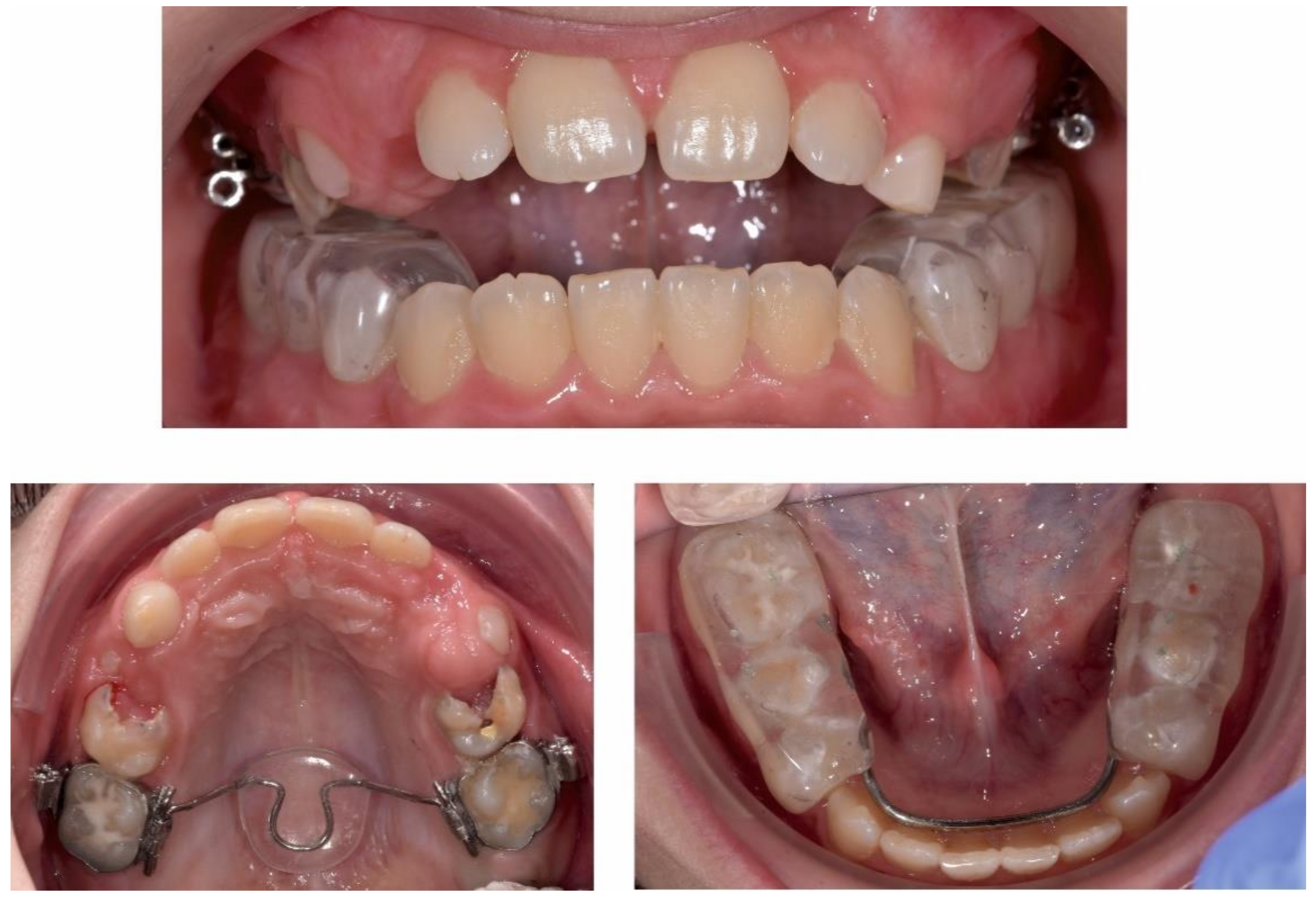
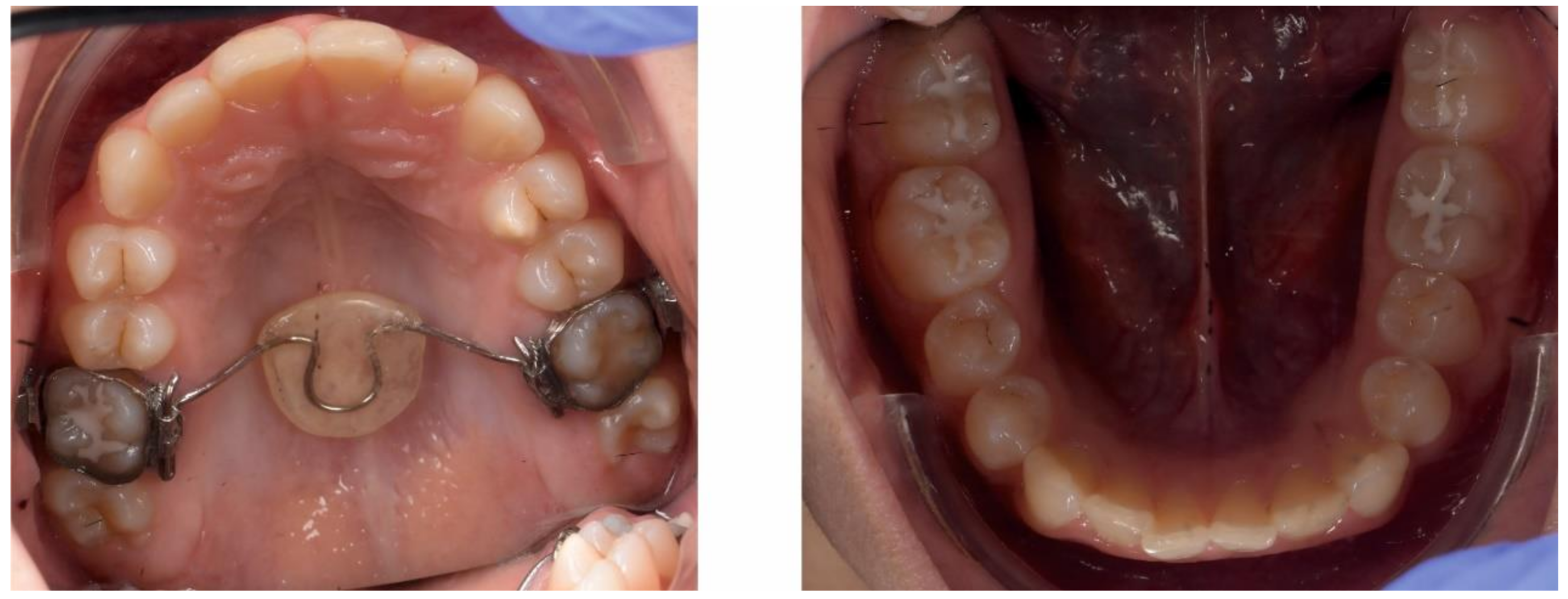
2.3.2. Second Phase of Treatment—2017—Bite-Blocks and Transpalatal Arch
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lew, D.P.; Waldvogel, F.A. Osteomyelitis. Lancet 2004, 364, 369–379. [Google Scholar] [CrossRef]
- Hatzenbuehler, J.; Pulling, T.J. Diagnosis and management of osteomyelitis. Am. Fam. Physician 2011, 84, 1027–1033. [Google Scholar]
- Sia, I.G.; Berbari, E.F. Infection and musculoskeletal conditions: Osteomyelitis. Best Pract. Res. Clin. Rheumatol. 2006, 20, 1065–1081. [Google Scholar] [CrossRef]
- Kremers, H.M.; Nwojo, M.E.; Ransom, J.E.; Wood-Wentz, C.M.; Melton, L.J.; Huddleston, P.M. Trends in the epidemiology of osteomyelitis: A population-based study, 1969 to 2009. J. Bone Joint Surg. Am. 2015, 97, 837–845. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walls, R.M.; Hockberger, R.S.; Gausche-Hill, M. Rosen’s Emergency Medicine: Concepts and Clinical Practice, 9th ed.; Elsevier: Philadelphia, PA, USA, 2018; ISBN 9780323354790. [Google Scholar]
- Berbari, E.F.; Kanj, S.S.; Kowalski, T.J.; Darouiche, R.O.; Widmer, A.F.; Schmitt, S.K.; Hendershot, E.F.; Holtom, P.D.; Huddleston, P.M.; Petermann, G.W.; et al. 2015 Infectious Diseases Society of America (IDSA) Clinical Practice Guidelines for the Diagnosis and Treatment of Native Vertebral Osteomyelitis in Adultsa. Clin. Infect. Dis. 2015, 61, e26–e46. [Google Scholar] [CrossRef] [Green Version]
- Adam, A. Grainger & Allison’s Diagnostic Radiology. A Textbook of Medical Imaging; Elsevier: Philadelphia, PA, USA, 2015; Volume 1, ISBN 9780702061288. [Google Scholar]
- Elsevier. Principles and Practice of Pediatric Infectious Diseases; Elsevier: Philadelphia, PA, USA, 2018; ISBN 9780323401814. [Google Scholar]
- Eversole, L.R.; Leider, A.S.; Corwin, J.O.; Karian, B.K. Proliferative periostitis of Garré: Its differentiation from other neoperiostoses. J. Oral Surg. 1979, 37, 725–731. [Google Scholar] [PubMed]
- Cherry, J.; Demmler-Harrison, G.J.; Kaplan, S.L.; Steinbach, W.J.; Hotez, P.J. Feigin and Cherry’s Textbook of Pediatric Infectious Diseases; Elsevier: Philadelphia, PA, USA, 2019; ISBN 9780323376921. [Google Scholar]
- Watt, E.; Ahmad, A.; Adamji, R.; Katsimpali, A.; Ashley, P.; Noar, J. Space maintainers in the primary and mixed dentition—A clinical guide. Br. Dent. J. 2018, 225, 293–298. [Google Scholar] [CrossRef]
- Liu, D.; Zhang, J.; Li, T.; Li, C.; Liu, X.; Zheng, J.; Su, Z.; Wang, X. Chronic osteomyelitis with proliferative periostitis of the mandibular body: Report of a case and review of the literature. Ann. R. Coll. Surg. Engl. 2019, 101, 328–332. [Google Scholar] [CrossRef] [PubMed]
- Martin-Granizo, R.; Garcia-Gonzalez, D.; Sastre, J.; Diaz, F.J. Mandibular sclerosing osteomyelitis of Garré. Otolaryngol. Head. Neck Surg. 1999, 121, 828–829. [Google Scholar] [CrossRef]
- Mattison, G.D.; Gould, A.R.; George, D.I.; Neb, J.L. Garre’s osteomyelitis of the mandible: The role of endodontic therapy in patient management. J. Endod. 1981, 7, 559–564. [Google Scholar] [CrossRef]
- McWalter, G.M.; Schaberg, S.J. Garre’s osteomyelitis of the mandible resolved by endodontic treatment. J. Am. Dent. Assoc. 1984, 108, 193–195. [Google Scholar] [CrossRef]
- Gonçalves, M.; Pinto Oliveira, D.; Oliveira Oya, E.; Gonçalves, A. Garre’s osteomyelitis associated with a fistula: A case report. J. Clin. Pediatr. Dent. 2002, 26, 311–313. [Google Scholar] [CrossRef] [PubMed]
- Akiyama, K.; Omori, K.; Kondo, H.; Kobayashi, J.; Yoshimura, H.; Tobita, T.; Ueno, T.; Sano, K. Root-end resection for preservation of the causative molar in Garrè’s osteomyelitis of the mandible: A case report. J. Oral Maxillofac. Surg. Med. Pathol. 2013, 25, 139–142. [Google Scholar] [CrossRef]
- Groot, R.H.; Ongerboer de Visser, B.W.; van Merkesteyn, J.P.R.; Speelman, J.D.; Bras, J. Changes in masseter inhibitory reflex responses in patients with diffuse sclerosing osteomyelitis of the mandible. Oral Surg. Oral Med. Oral Pathol. 1992, 74, 727–732. [Google Scholar] [CrossRef]
- Van de Meent, M.M.; Wetselaar-Glas, M.J.M.; Fiocco, M.; Appelman-Dijkstra, N.M.; van Merkesteyn, J.P.R. Non-surgical treatment of adults with chronic diffuse sclerosing osteomyelitis/tendoperiostitis of the mandible. J. Craniomaxillofac. Surg. 2019, 47, 1922–1928. [Google Scholar] [CrossRef] [PubMed]
- Van de Meent, M.M.; Meshkini, H.; Fiocco, M.; Wetselaar-Glas, M.J.M.; Appelman-Dijkstra, N.M.; van Merkesteyn, J.P.R. Conservative treatment of children with chronic diffuse sclerosing osteomyelitis/tendoperiostitis of the mandible. J. Cranio Maxillofac. Surg. 2017, 45, 1938–1943. [Google Scholar] [CrossRef] [PubMed]
- Van de Meent, M.M.; Pichardo, S.E.C.; Appelman-Dijkstra, N.M.; van Merkesteyn, J.P.R. Outcome of different treatments for chronic diffuse sclerosing osteomyelitis of the mandible: A systematic review of published papers. Br. J. Oral Maxillofac. Surg. 2020, 58, 385–395. [Google Scholar] [CrossRef] [PubMed]
- Gurton, A.U.; Akin, E.; Karacay, S. Initial intrusion of the molars in the treatment of anterior open bite malocclusions in growing patients. Angle Orthod. 2004, 74, 454–464. [Google Scholar] [CrossRef] [PubMed]
- Rijpstra, C.; Lisson, J.A. Etiology of anterior open bite: A review. J. Orofac. Orthop. 2016, 77, 281–286. [Google Scholar] [CrossRef] [PubMed]




























Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barbur, I.; Bran, S.; Baciut, M.; Armencea, G.; Aghiorghiesei, A.I.; Suciu, T.-S.; Barbur, A.M.; Opris, H.; Baciut, G.; Dinu, C. An Orthodontic Approach for Garre’s Sclerosing Osteomyelitis of the Mandible. Int. J. Environ. Res. Public Health 2021, 18, 3159. https://doi.org/10.3390/ijerph18063159
Barbur I, Bran S, Baciut M, Armencea G, Aghiorghiesei AI, Suciu T-S, Barbur AM, Opris H, Baciut G, Dinu C. An Orthodontic Approach for Garre’s Sclerosing Osteomyelitis of the Mandible. International Journal of Environmental Research and Public Health. 2021; 18(6):3159. https://doi.org/10.3390/ijerph18063159
Chicago/Turabian StyleBarbur, Ioan, Simion Bran, Mihaela Baciut, Gabriel Armencea, Alexandra Iulia Aghiorghiesei, Tudor-Sergiu Suciu, Adina Maria Barbur, Horia Opris, Grigore Baciut, and Cristian Dinu. 2021. "An Orthodontic Approach for Garre’s Sclerosing Osteomyelitis of the Mandible" International Journal of Environmental Research and Public Health 18, no. 6: 3159. https://doi.org/10.3390/ijerph18063159
APA StyleBarbur, I., Bran, S., Baciut, M., Armencea, G., Aghiorghiesei, A. I., Suciu, T. -S., Barbur, A. M., Opris, H., Baciut, G., & Dinu, C. (2021). An Orthodontic Approach for Garre’s Sclerosing Osteomyelitis of the Mandible. International Journal of Environmental Research and Public Health, 18(6), 3159. https://doi.org/10.3390/ijerph18063159