
Systemic Inflammation (C-Reactive Protein) in Older Chinese Adults Is Associated with Long-Term Exposure to Ambient Air Pollution

 ,
,  ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Popultation
2.2. Exposure Assessment
2.3. Hs-CRP Level Measuremenets
2.4. Covariates
2.5. Statistical Analysis
3. Results
3.1. Study Population
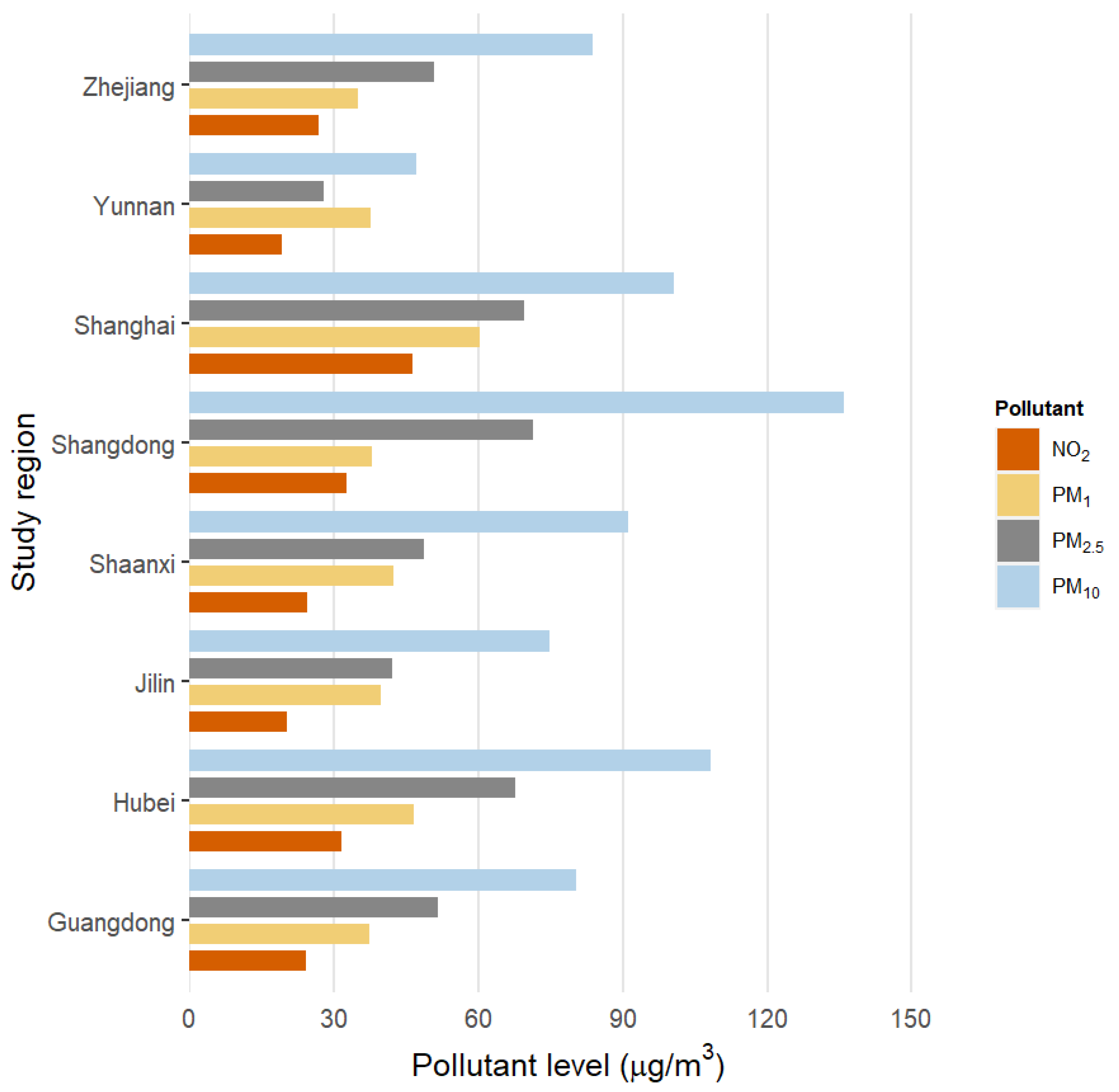
3.2. Air Pollution Exposure
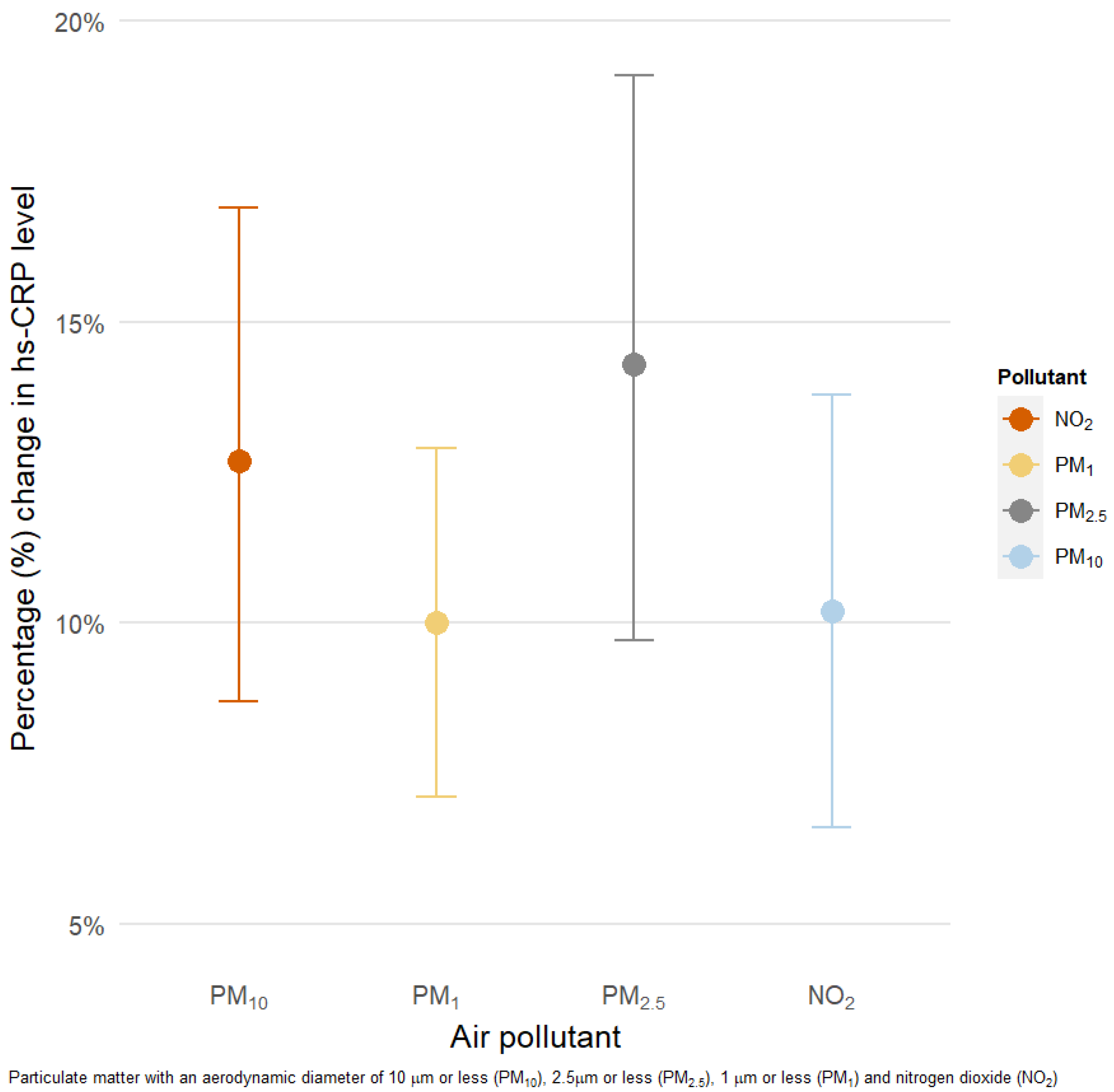
3.3. Association of Exposure to PM and NO2 with hs-CRP Levels
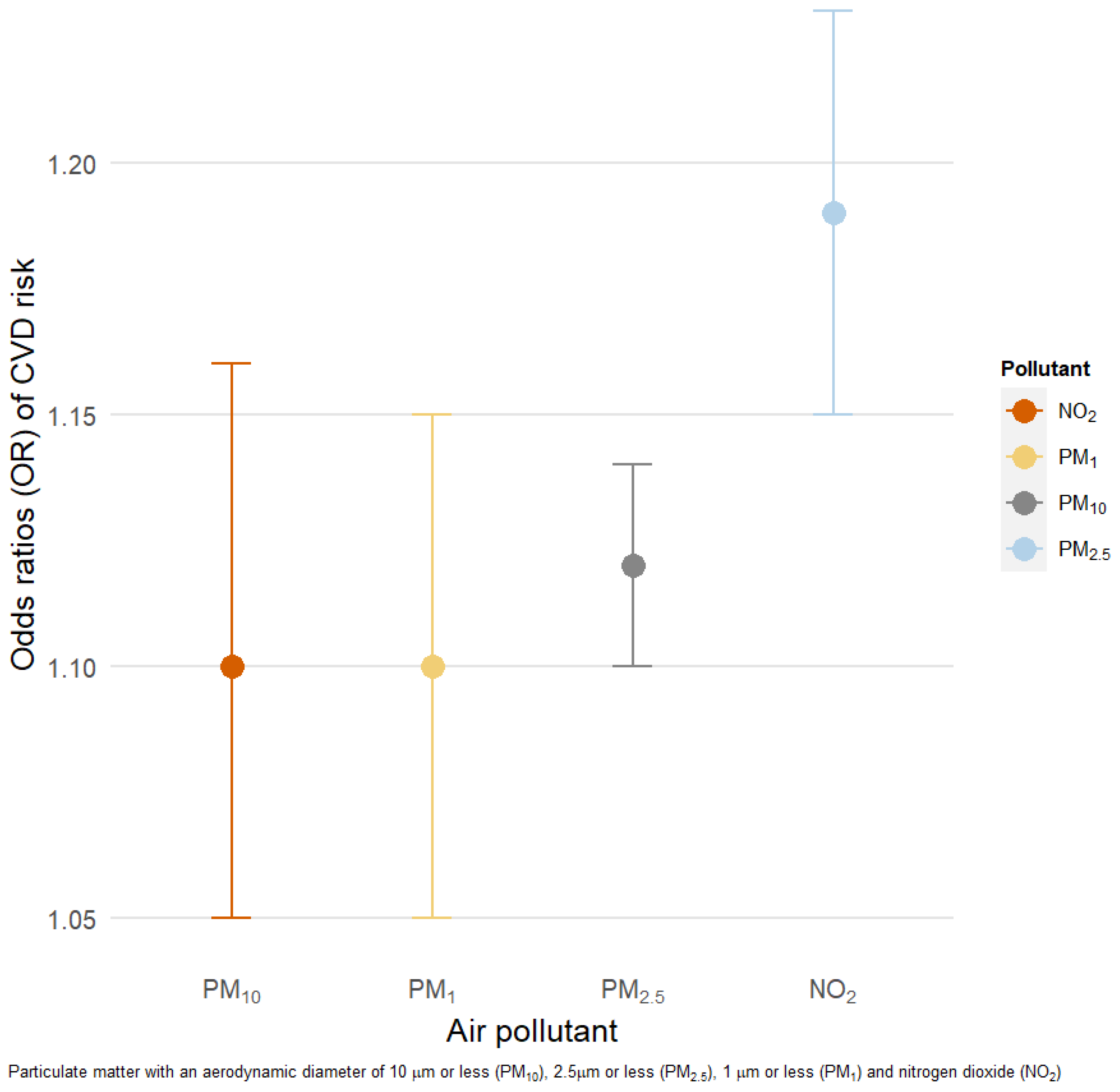
3.4. Odds Ratio of CVD Risk Increase
3.5. Sensitivity Analysis
3.6. Effect Modification
4. Discussion
Strength and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Boogaard, H.; Walker, K.; Cohen, A.J. Air pollution: The emergence of a major global health risk factor. Int. Health 2019, 11, 417–421. [Google Scholar] [CrossRef]
- World Health Organization. Ambient Air Pollution: A Global Assessment of Exposure and Burden of Disease; World Health Organization: Geneva, Switzerland, 2016; pp. 23–50. [Google Scholar]
- Al-Kindi, S.G.; Brook, R.D.; Biswal, S.; Rajagopalan, S. Environmental determinants of cardiovascular disease: Lessons learned from air pollution. Nat. Rev. Cardiol. 2020, 17, 656–672. [Google Scholar] [CrossRef]
- Cohen, A.J.; Anderson, H.R.; Ostro, B.; Pandey, K.D.; Krzyzanowski, M.; Künzli, N.; Gutschmidt, K.; Pope, A.; Romieu, I.; Samet, J.M.; et al. The global burden of disease due to outdoor air pollution. J. Toxicol. Environ. Health Part A 2005, 68, 1301–1307. [Google Scholar] [CrossRef] [PubMed]
- Rückerl, R.; Schneider, A.; Breitner, S.; Cyrys, J.; Peters, A. Health effects of particulate air pollution: A review of epidemiological evidence. Inhal. Toxicol. 2011, 23, 555–592. [Google Scholar] [CrossRef]
- Lu, F.; Xu, D.; Cheng, Y.; Dong, S.; Guo, C.; Jiang, X.; Zheng, X. Systematic review and meta-analysis of the adverse health effects of ambient PM2.5 and PM10 pollution in the Chinese population. Environ. Res. 2015, 136, 196–204. [Google Scholar] [CrossRef] [PubMed]
- Sosa, B.S.; Porta, A.; Colman Lerner, J.E.; Banda Noriega, R.; Massolo, L. Human health risk due to variations in PM10-PM2.5 and associated PAHs levels. Atmos. Environ. 2017, 160, 27–35. [Google Scholar] [CrossRef]
- Cohen, A.J.; Brauer, M.; Burnett, R.; Anderson, H.R.; Frostad, J.; Estep, K.; Balakrishnan, K.; Brunekreef, B.; Dandona, L.; Dandona, R.; et al. Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: An analysis of data from the Global Burden of Diseases Study 2015. Lancet 2017, 389, 1907–1918. [Google Scholar] [CrossRef] [Green Version]
- Roth, G.A.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; et al. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1736–1788. [Google Scholar] [CrossRef] [Green Version]
- Metzger, K.B.; Tolbert, P.E.; Klein, M.; Peel, J.L.; Flanders, W.D.; Todd, K.; Mulholland, J.A.; Ryan, P.B.; Frumkin, H. Ambient air pollution and cardiovascular emergency department visits. Epidemiology 2004, 15, 46–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kan, H.; Huang, W.; Chen, B.; Zhao, N. Impact of outdoor air pollution on cardiovascular health in Mainland China. CVD Prev. Control 2009, 4, 71–78. [Google Scholar] [CrossRef]
- Brook, R.D.; Rajagopalan, S.; Pope, C.A.; Brook, J.R.; Bhatnagar, A.; Diez-Roux, A.V.; Holguin, F.; Hong, Y.; Luepker, R.V.; Mittleman, M.A.; et al. Particulate matter air pollution and cardiovascular disease: An update to the scientific statement from the american heart association. Circulation 2010, 121, 2331–2378. [Google Scholar] [CrossRef] [Green Version]
- Patel, V.; Kantipudi, N.; Jones, G.; Upton, A.; Kamath, M.V. Air pollution and cardiovascular disease: A review. Crit. Rev. Biomed. Eng. 2016, 44, 327–346. [Google Scholar] [CrossRef] [PubMed]
- Van Eeden, S.F.; Tan, W.C.; Suwa, T.; Mukae, H.; Terashima, T.; Fujii, T.; Qui, D.; Vincent, R.; Hogg, J.C. Cytokines involved in the systemic inflammatory response induced by exposure to particulate matter air pollutants (PM10). Am. J. Respir. Crit. Care Med. 2001, 164, 826–830. [Google Scholar] [CrossRef]
- Becker, S.; Mundandhara, S.; Devlin, R.B.; Madden, M. Regulation of cytokine production in human alveolar macrophages and airway epithelial cells in response to ambient air pollution particles: Further mechanistic studies. Toxicol. Appl. Pharmacol. 2005, 207, 269–275. [Google Scholar] [CrossRef]
- Sproston, N.R.; Ashworth, J.J. Role of C-reactive protein at sites of inflammation and infection. Front. Immunol. 2018, 9, 754. [Google Scholar] [CrossRef]
- Cozlea, D.L.; Farcas, D.M.; Nagy, A.; Keresztesi, A.A.; Tifrea, R.; Cozlea, L.; Carașca, E. The impact of C reactive protein on global cardiovascular risk on patients with coronary artery disease. Curr. Health Sci. J. 2013, 39, 225–231. [Google Scholar]
- Hennig, F.; Fuks, K.; Moebus, S.; Weinmayr, G.; Memmesheimer, M.; Jakobs, H.; Bröcker-Preuss, M.; Führer-Sakel, D.; Möhlenkamp, S.; Erbel, R.; et al. Association between source-specific particulate matter air pollution and hs-CRP: Local traffic and industrial emissions. Environ. Health Perspect. 2014, 122, 703–710. [Google Scholar] [CrossRef] [Green Version]
- Hoffmann, B.; Moebus, S.; Dragano, N.; Stang, A.; Möhlenkamp, S.; Schmermund, A.; Memmesheimer, M.; Bröcker-Preuss, M.; Mann, K.; Erbel, R.; et al. Chronic residential exposure to particulate matter air pollution and systemic inflammatory markers. Environ. Health Perspect. 2009, 117, 1302–1308. [Google Scholar] [CrossRef] [Green Version]
- Zeka, A.; Sullivan, J.R.; Vokonas, P.S.; Sparrow, D.; Schwartz, J. Inflammatory markers and particulate air pollution: Characterizing the pathway to disease. Int. J. Epidemiol. 2006, 35, 1347–1354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Q.; Gu, X.; Deng, F.; Mu, L.; Baccarelli, A.A.; Guo, X.; Wu, S. Ambient particulate air pollution and circulating C-reactive protein level: A systematic review and meta-analysis. Int. J. Hyg. Environ. Health 2019, 222, 756–764. [Google Scholar] [CrossRef]
- Mannucci, P.M.; Franchini, M. Health effects of ambient air pollution in developing countries. Int. J. Environ. Res. Public Health 2017, 14, 1048. [Google Scholar] [CrossRef]
- Xue, T.; Liu, J.; Zhang, Q.; Geng, G.; Zheng, Y.; Tong, D.; Liu, Z.; Guan, D.; Bo, Y.; Zhu, T.; et al. Rapid improvement of PM2.5 pollution and associated health benefits in China during 2013–2017. Sci. China Earth Sci. 2019, 62, 1847–1856. [Google Scholar] [CrossRef]
- Dadvand, P.; Nieuwenhuijsen, M.J.; Agustí, À.; De Batlle, J.; Benet, M.; Beelen, R.; Cirach, M.; Martinez, D.; Hoek, G.; Basagaña, X.; et al. Air pollution and biomarkers of systemic inflammation and tissue repair in COPD patients. Eur. Respir. J. 2014, 44, 603–613. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bind, M.A.; Baccarelli, A.; Zanobetti, A.; Tarantini, L.; Suh, H.; Vokonas, P.; Schwartz, J. Air pollution and markers of coagulation, inflammation, and endothelial function: Associations and epigene-environment interactions in an elderly cohort. Epidemiology 2012, 23, 332–340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pilz, V.; Wolf, K.; Breitner, S.; Rückerl, R.; Koenig, W.; Rathmann, W.; Cyrys, J.; Peters, A.; Schneider, A. C-reactive protein (CRP) and long-term air pollution with a focus on ultrafine particles. Int. J. Hyg. Environ. Health 2018, 221, 510–518. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaparro, M.P.; Benzeval, M.; Richardson, E.; Mitchell, R. Neighborhood deprivation and biomarkers of health in Britain: The mediating role of the physical environment. BMC Public Health 2018, 18, 201. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.; Li, S.; Zhang, Y.; Zhang, W.; Li, D.; Wei, X.; He, Y.; Bell, M.L.; Williams, G.; Marks, G.B.; et al. Effects of ambient PM1 air pollution on daily emergency hospital visits in China: An epidemiological study. Lancet Planet. Health 2017, 1, e221–e229. [Google Scholar] [CrossRef]
- Elbarbary, M.; Honda, T.; Morgan, G.; Guo, Y.; Guo, Y.; Kowal, P.; Negin, J. Ambient Air Pollution Exposure Association with Anaemia Prevalence and Haemoglobin Levels in Chinese Older Adults. Int. J. Environ. Res. Public Health 2020, 17, 3209. [Google Scholar] [CrossRef]
- Chen, G.; Knibbs, L.D.; Zhang, W.; Li, S.; Cao, W.; Guo, J.; Ren, H.; Wang, B.; Wang, H.; Williams, G.; et al. Estimating spatiotemporal distribution of PM1 concentrations in China with satellite remote sensing, meteorology, and land use information. Environ. Pollut. 2018, 233, 1086–1094. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.; Li, S.; Knibbs, L.D.; Hamm, N.A.S.; Cao, W.; Li, T.; Guo, J.; Ren, H.; Abramson, M.J.; Guo, Y. A machine learning method to estimate PM2.5 concentrations across China with remote sensing, meteorological and land use information. Sci. Total Environ. 2018, 636, 52–60. [Google Scholar] [CrossRef]
- Krotkov, N.A.; Lamsal, L.N.; Celarier, E.A.; Swartz, W.H.; Marchenko, S.V.; Bucsela, E.J.; Chan, K.L.; Wenig, M.; Zara, M. The version 3 OMI NO2 standard product. Atmos. Meas. Tech. 2017, 10, 3133–3149. [Google Scholar] [CrossRef] [Green Version]
- Zhan, Y.; Luo, Y.; Deng, X.; Zhang, K.; Zhang, M.; Grieneisen, M.L.; Di, B. Satellite-Based Estimates of Daily NO2 Exposure in China Using Hybrid Random Forest and Spatiotemporal Kriging Model. Environ. Sci. Technol. 2018, 52, 4180–4189. [Google Scholar] [CrossRef]
- Skogstrand, K.; Ekelund, C.K.; Thorsen, P.; Vogel, I.; Jacobsson, B.; Nørgaard-Pedersen, B.; Hougaard, D.M. Effects of blood sample handling procedures on measurable inflammatory markers in plasma, serum and dried blood spot samples. J. Immunol. Methods 2008, 336, 78–84. [Google Scholar] [CrossRef] [PubMed]
- McDade, T.W.; Williams, S.; Snodgrass, J.J. What a drop can do: Dried blood spots as a minimally invasive method for integrating biomarkers into population-based research. Demography 2007, 44, 899–925. [Google Scholar] [CrossRef] [Green Version]
- Kamath, D.Y.; Xavier, D.; Sigamani, A.; Pais, P. High sensitivity C-reactive protein (hsCRP) & cardiovascular disease: An Indian perspective. Indian J. Med. Res. 2015, 142, 261–268. [Google Scholar] [CrossRef] [PubMed]
- Pearson, T.A.; Mensah, G.A.; Alexander, R.W.; Anderson, J.L.; Cannon, R.O.; Criqui, M.; Fadl, Y.Y.; Fortmann, S.P.; Hong, Y.; Myers, G.L.; et al. Markers of inflammation and cardiovascular disease: Application to clinical and public health practice: A statement for healthcare professionals from the centers for disease control and prevention and the American Heart Association. Circulation 2003, 107, 499–511. [Google Scholar] [CrossRef]
- Brulle, R.J.; Pellow, D.N. Environmental justice: Human health and environmental inequalities. Annu. Rev. Public Health 2006, 27, 103–124. [Google Scholar] [CrossRef] [Green Version]
- Mohai, P.; Pellow, D.; Roberts, J.T. Environmental justice. Annu. Rev. Environ. Resour. 2009, 34, 405–430. [Google Scholar] [CrossRef]
- Lucht, S.; Hennig, F.; Moebus, S.; Führer-Sakel, D.; Herder, C.; Jöckel, K.H.; Hoffmann, B. Air pollution and diabetes-related biomarkers in non-diabetic adults: A pathway to impaired glucose metabolism? Environ. Int. 2019, 124, 370–392. [Google Scholar] [CrossRef]
- Erqou, S.; Clougherty, J.E.; Olafiranye, O.; Magnani, J.W.; Aiyer, A.; Tripathy, S.; Kinnee, E.; Kip, K.E.; Reis, S.E. Particulate Matter Air Pollution and Racial Differences in Cardiovascular Disease Risk. Arterioscler. Thromb. Vasc. Biol. 2018, 38, 935–942. [Google Scholar] [CrossRef] [Green Version]
- Tsai, D.H.; Riediker, M.; Berchet, A.; Paccaud, F.; Waeber, G.; Vollenweider, P.; Bochud, M. Effects of short- and long-term exposures to particulate matter on inflammatory marker levels in the general population. Environ. Sci. Pollut. Res. 2019, 26, 19697–19704. [Google Scholar] [CrossRef] [PubMed]
- Yang, B.Y.; Guo, Y.; Morawska, L.; Bloom, M.S.; Markevych, I.; Heinrich, J.; Dharmage, S.C.; Knibbs, L.D.; Lin, S.; Yim, S.H.L.; et al. Ambient PM1 air pollution and cardiovascular disease prevalence: Insights from the 33 Communities Chinese Health Study. Environ. Int. 2019, 123, 310–317. [Google Scholar] [CrossRef] [PubMed]
- Zwozdziak, A.; Sówka, I.; Willak-Janc, E.; Zwozdziak, J.; Kwiecińska, K.; Balińska-Miśkiewicz, W. Influence of PM1 and PM2.5 on lung function parameters in healthy schoolchildren—a panel study. Environ. Sci. Pollut. Res. 2016, 23, 23892–23901. [Google Scholar] [CrossRef] [PubMed]
- Yin, P.; Guo, J.; Wang, L.; Fan, W.; Lu, F.; Guo, M.; Moreno, S.B.R.; Wang, Y.; Wang, H.; Zhou, M.; et al. Higher Risk of Cardiovascular Disease Associated with Smaller Size-Fractioned Particulate Matter. Environ. Sci. Technol. Lett. 2020, 7, 95–101. [Google Scholar] [CrossRef]
- Schraufnagel, D.E. The health effects of ultrafine particles. Exp. Mol. Med. 2020, 52, 311–317. [Google Scholar] [CrossRef]
- Midouhas, E.; Kokosi, T.; Flouri, E. Neighbourhood-level air pollution and greenspace and inflammation in adults. Health Place 2019, 58, 102167. [Google Scholar] [CrossRef] [PubMed]
- Forbes, L.J.L.; Patel, M.D.; Rudnicka, A.R.; Cook, D.G.; Bush, T.; Stedman, J.R.; Whincup, P.H.; Strachan, D.P.; Anderson, H.R. Chronic exposure to outdoor air pollution and diagnosed cardiovascular disease: Meta-analysis of three large cross-sectional surveys. Environ. Health 2009, 8, 30. [Google Scholar] [CrossRef] [Green Version]
- Huang, W.H.; Yen, T.H.; Chan, M.J.; Su, Y.J. Environmental carbon monoxide level is associated with the level of high-sensitivity c-reactive protein in peritoneal dialysis patients. Medicine 2014, 93, e181. [Google Scholar] [CrossRef]
- Hajat, A.; Allison, M.; Diez-Roux, A.V.; Jenny, N.S.; Jorgensen, N.W.; Szpiro, A.A.; Vedal, S.; Kaufman, J.D. Long-term exposure to air pollution and markers of inflammation, coagulation, and endothelial activation a repeat-measures analysis in the multi-ethnic study of atherosclerosis (MESA). Epidemiology 2015, 26, 310–320. [Google Scholar] [CrossRef]
- Wolf, K.; Popp, A.; Schneider, A.; Breitner, S.; Hampel, R.; Rathmann, W.; Herder, C.; Roden, M.; Koenig, W.; Meisinger, C.; et al. Association between long-term exposure to air pollution and biomarkers related to insulin resistance, subclinical inflammation, and adipokines. Diabetes 2016, 65, 3314–3326. [Google Scholar] [CrossRef] [Green Version]
- Panasevich, S.; Leander, K.; Rosenlund, M.; Ljungman, P.; Bellander, T.; De Faire, U.; Pershagen, G.; Nyberg, F. Associations of long- and short-term air pollution exposure with markers of inflammation and coagulation in a population sample. Occup. Environ. Med. 2009, 66, 747–753. [Google Scholar] [CrossRef]
- Cai, Y.; Hansell, A.L.; Blangiardo, M.; Burton, P.R.; De Hoogh, K.; Doiron, D.; Fortier, I.; Gulliver, J.; Hveem, K.; Mbatchou, S.; et al. Long-termexposure to road traffic noise, ambient air pollution, and cardiovascular risk factors in the HUNTand lifelines cohorts. Eur. Heart J. 2017, 38, 2290–2296. [Google Scholar] [CrossRef] [Green Version]
- Ostro, B.; Malig, B.; Broadwin, R.; Basu, R.; Gold, E.B.; Bromberger, J.T.; Derby, C.; Feinstein, S.; Greendale, G.A.; Jackson, E.A.; et al. Chronic PM2.5 exposure and inflammation: Determining sensitive subgroups in mid-life women. Environ. Res. 2014, 132, 168–175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viehmann, A.; Hertel, S.; Fuks, K.; Eisele, L.; Moebus, S.; Möhlenkamp, S.; Nonnemacher, M.; Jakobs, H.; Erbel, R.; Jöckel, K.H.; et al. Long-term residential exposure to urban air pollution, and repeated measures of systemic blood markers of inflammation and coagulation. Occup. Environ. Med. 2015, 72, 656–663. [Google Scholar] [CrossRef]
- Rückerl, R.; Peters, A.; Khuseyinova, N.; Andreani, M.; Koenig, W.; Meisinger, C.; Dimakopoulou, K.; Sunyer, J.; Lanki, T.; Nyberg, F.; et al. Determinants of the acute-phase protein C-reactive protein in myocardial infarction survivors: The role of comorbidities and environmental factors. Clin. Chem. 2009, 55, 322–335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Z.; Chang, L.Y.; Lau, A.K.H.; Chan, T.C.; Chuang, Y.C.; Chan, J.; Lin, C.; Jiang, W.K.; Dear, K.; Zee, B.C.Y.; et al. Satellite-based estimates of long-term exposure to fine particulate matter are associated with C-reactive protein in 30 034 Taiwanese adults. Int. J. Epidemiol. 2017, 46, 1126–1136. [Google Scholar] [CrossRef] [PubMed]
- Green, R.; Broadwin, R.; Malig, B.; Basu, R.; Gold, E.B.; Qi, L.; Sternfeld, B.; Bromberger, J.T.; Greendale, G.A.; Kravitz, H.M.; et al. Long- and short-term exposure to air pollution and inflammatory/hemostatic markers in midlife women. Epidemiology 2016, 27, 211–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, W.; Xu, Z.; Yang, T. Health effects of air pollution in china. Int. J. Environ. Res. Public Health 2018, 15, 1471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, D.; Liu, J.; Wang, M.; Zhang, X.; Zhou, M. Epidemiology of cardiovascular disease in China: Current features and implications. Nat. Rev. Cardiol. 2019, 16, 203–212. [Google Scholar] [CrossRef]
- Valiathan, R.; Ashman, M.; Asthana, D. Effects of Ageing on the Immune System: Infants to Elderly. Scand. J. Immunol. 2016, 83, 255–266. [Google Scholar] [CrossRef] [Green Version]
- Cvecka, J.; Tirpakova, V.; Sedliak, M.; Kern, H.; Mayr, W.; Hamar, D. Physical activity in elderly. Eur. J. Transl. Myol. 2015, 25, 249. [Google Scholar] [CrossRef] [PubMed]
- United Nations. World Population Prospects 2019. Available online: https://digitallibrary.un.org/record/3813698 (accessed on 30 July 2019).
- Lelieveld, J.; Klingmüller, K.; Pozzer, A.; Pöschl, U.; Fnais, M.; Daiber, A.; Münzel, T. Cardiovascular disease burden from ambient air pollution in Europe reassessed using novel hazard ratio functions. Eur. Heart J. 2019, 40, 1590–1596. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roth, G.A.; Johnson, C.; Abajobir, A.; Abd-Allah, F.; Abera, S.F.; Abyu, G.; Ahmed, M.; Aksut, B.; Alam, T.; Alam, K.; et al. Global, Regional, and National Burden of Cardiovascular Diseases for 10 Causes, 1990 to 2015. J. Am. Coll. Cardiol. 2017, 70, 1–25. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Mean | SD or % |
|---|---|---|
| PM10 1 year (μg/m3) | 90.23 | 28.80 |
| PM2.5 1 year (μg/m3) | 53.94 | 17.08 |
| PM1 1 year (μg/m3) | 43.67 | 13.04 |
| NO2 1 year (μg/m3) | 30.52 | 12.36 |
| Age (years) | 63.22 | 9.35 |
| BMI (kg/m2) | 24.11 | 4.81 |
| Systolic blood pressure (mmHg) | 148.26 | 24.55 |
| Diastolic blood pressure (mmHg) | 84.64 | 13.55 |
| Total annual household incomes | ||
| • ≤20,000 CNY | 4181 | 52.82 |
| • >20,000 CNY | 3512 | 44.37 |
| Sex (n, %) | ||
| • Male | 3774 | 47.68 |
| • Female | 4141 | 52.32 |
| Smoking status | ||
| • Current tobacco use | 2615 | 33.14 |
| • No current tobacco use | 5275 | 66.86 |
| Alcohol use | ||
| • Current alcohol drinking | 2377 | 30.19 |
| • No current alcohol drinker | 5496 | 69.81 |
| Education | ||
| • No formal education | 1762 | 22.26 |
| • Primary school | 3173 | 40.09 |
| • Middle school | 1521 | 19.22 |
| • High school or higher | 1459 | 18.43 |
| Place of residence | ||
| • Rural | 4276 | 54.02 |
| • Urban | 3639 | 45.98 |
| Physical activity | ||
| • Low level | 2707 | 34.31 |
| • Moderate level | 2243 | 28.43 |
| • High level | 2939 | 37.25 |
| Nutrition | ||
| • Insufficient intake of fruits and vegetables | 3336 | 42.15 |
| • Sufficient intake of fruits and vegetables | 4579 | 57.85 |
| Type of fuel used at home | ||
| • Clean | 4588 | 58.42 |
| • Unclean | 3265 | 41.58 |
| History of Diabetes | ||
| • Yes | 554 | 7.06 |
| • No | 7298 | 92.94 |
| History of Chronic lung diseases | ||
| • Yes | 629 | 8 |
| • No | 7236 | 92 |
| Characteristics | PM10 % (95% CI) | PM2.5 % (95% CI) | PM1 % (95% CI) | NO2 % (95% CI) |
|---|---|---|---|---|
| Sex | p = 0.09 | p = 0.26 | p = 0.25 | p = 0.50 |
| • Male | 11.21 a (6.44, 16.18) | 13.73 (7.21, 20.64) | 9.76 (5.68, 14.01) | 10.16 (4.86, 15.73) |
| • Female | 12.58 a (7.65, 17.75) | 16.06 (9.53, 22.98) | 9.71 (5.73, 13.85) | 11.91 (96.56, 17.52) |
| Smoking | p = 0.11 | p = 0.34 | p = 0.35 | p = 0.52 |
| • Yes | 7.22 b (2.2, 12.67) | 7.81 (0.53, 15.63) | 6.56 (1.86, 11.49) | 3.53 (−2.48, 9.92) |
| • No | 14.29 b (9.75, 19.01) | 17.95 (11.99, 24.24) | 10.76 (7.18, 14.46) | 14.07 (9.29, 19.06) |
| Age | p = 0.02 | p = 0.03 | p = 0.68 | p = 0.34 |
| • ≤65 years | 11.34 c (6.93, 15.93) | 13.41 (7.59, 19.54) | 10.67 (7.13, 14.33) | 11.69 (6.97, 16.63) |
| • >65 years | 13.78 c (8.07, 19.80) | 19.22 (11.26, 27.75) | 9.89 (4.93, 15.08) | 11.70 (5.25, 18.55) |
| Income | p = 0.08 | p = 0.49 | p < 0.001 | p = 0.06 |
| • ≤20,000 CNY | 9.57 d (4.58, 14,80) | 10.35 (3.47, 17.68) | 7.56 (3.62, 11.64) | 5.46 (0.20, 10.99) |
| • >20,000 CNY | 6.33 d (0.59, 12.39) | 9.55 (1.34, 18.42) | 8.38 (3.46, 13.53) | 9.19 (2.37, 16.49) |
| Characteristics | PM10 OR (95% CI) | PM2.5 OR (95% CI) | PM1 OR (95% CI) | NO2 OR (95% CI) |
|---|---|---|---|---|
| Sex | p = 0.93 | p = 0.66 | p = 0.07 | p = 0.309 |
| • Male | 1.11 (1.08, 1.15) a | 1.19 (1.12, 1.26) a | 1.07 (0.99, 1.15) a | 1.11 (1.03, 1.20) a |
| • Female | 1.10 (1.08, 1.13) a | 1.20 (1.15, 1.26) a | 1.11 (1.04, 1.19) a | 1.15 (1.07, 1.23) a |
| Smoking | p = 0.78 | p = 0.58 | p = 0.06 | p = 0.051 |
| • Yes | 1.12 (1.07, 1.16) b | 1.17 (1.09, 1.25) b | 1.00 (0.92, 1.10) b | 1.03 (0.93, 1.13) b |
| • No | 1.10 (1.08, 1.13) b | 1.20 (1.16, 1.25) b | 1.13 (1.07, 1.21) b | 1.18 (1.11, 1.26) b |
| Age | p = 0.06 | p = 0.04 | p = 0.35 | p = 0.08 |
| • ≤65 years | 1.08 (1.06, 1.11) c | 1.14 (1.08, 1.20) c | 1.08 (1.01, 1.15) c | 1.05 (0.98, 1.13) c |
| • >65 years | 1.13 (1.11, 1.16) c | 1.27 (1.20, 1.33) c | 1.13 (1.04, 1.21) c | 1.25 (1.16, 1.36) c |
| Income | p = 0.73 | p = 0.93 | p = 0.05 | p = 0.86 |
| • ≤20,000 CNY | 1.10 (1.07, 1.13) d | 1.15 (1.09, 1.22) d | 1.02 (0.95, 1.09) d | 1.08 (0.99, 1.18) d |
| • >20,000 CNY | 1.10 (1.07, 1.12) d | 1.18 (1.13, 1.24) | 1.08 (1.00, 1.17) d | 1.12 (1.05, 1.20) d |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Elbarbary, M.; Oganesyan, A.; Honda, T.; Morgan, G.; Guo, Y.; Guo, Y.; Negin, J. Systemic Inflammation (C-Reactive Protein) in Older Chinese Adults Is Associated with Long-Term Exposure to Ambient Air Pollution. Int. J. Environ. Res. Public Health 2021, 18, 3258. https://doi.org/10.3390/ijerph18063258
Elbarbary M, Oganesyan A, Honda T, Morgan G, Guo Y, Guo Y, Negin J. Systemic Inflammation (C-Reactive Protein) in Older Chinese Adults Is Associated with Long-Term Exposure to Ambient Air Pollution. International Journal of Environmental Research and Public Health. 2021; 18(6):3258. https://doi.org/10.3390/ijerph18063258
Chicago/Turabian StyleElbarbary, Mona, Artem Oganesyan, Trenton Honda, Geoffrey Morgan, Yuming Guo, Yanfei Guo, and Joel Negin. 2021. "Systemic Inflammation (C-Reactive Protein) in Older Chinese Adults Is Associated with Long-Term Exposure to Ambient Air Pollution" International Journal of Environmental Research and Public Health 18, no. 6: 3258. https://doi.org/10.3390/ijerph18063258
APA StyleElbarbary, M., Oganesyan, A., Honda, T., Morgan, G., Guo, Y., Guo, Y., & Negin, J. (2021). Systemic Inflammation (C-Reactive Protein) in Older Chinese Adults Is Associated with Long-Term Exposure to Ambient Air Pollution. International Journal of Environmental Research and Public Health, 18(6), 3258. https://doi.org/10.3390/ijerph18063258