
Linking Health Literacy to Self-Care in Hypertensive Patients with Physical Disabilities: A Path Analysis Using a Multi-Mediation Model


Abstract
:1. Introduction
2. Materials and Methods
2.1. Sampling and Data Collection
2.2. Measurement
2.2.1. Health Literacy
2.2.2. Access to Healthcare
2.2.3. Provider–Patient Interactions
2.2.4. Hypertension Knowledge
2.2.5. Hypertension Control Self-Efficacy
2.2.6. Hypertension Self-Care
2.2.7. Demographic and Health-Related Characteristics
2.3. Data Analysis
3. Results
3.1. Participant Characteristics
3.2. Multi-Collinearity among Research Variables
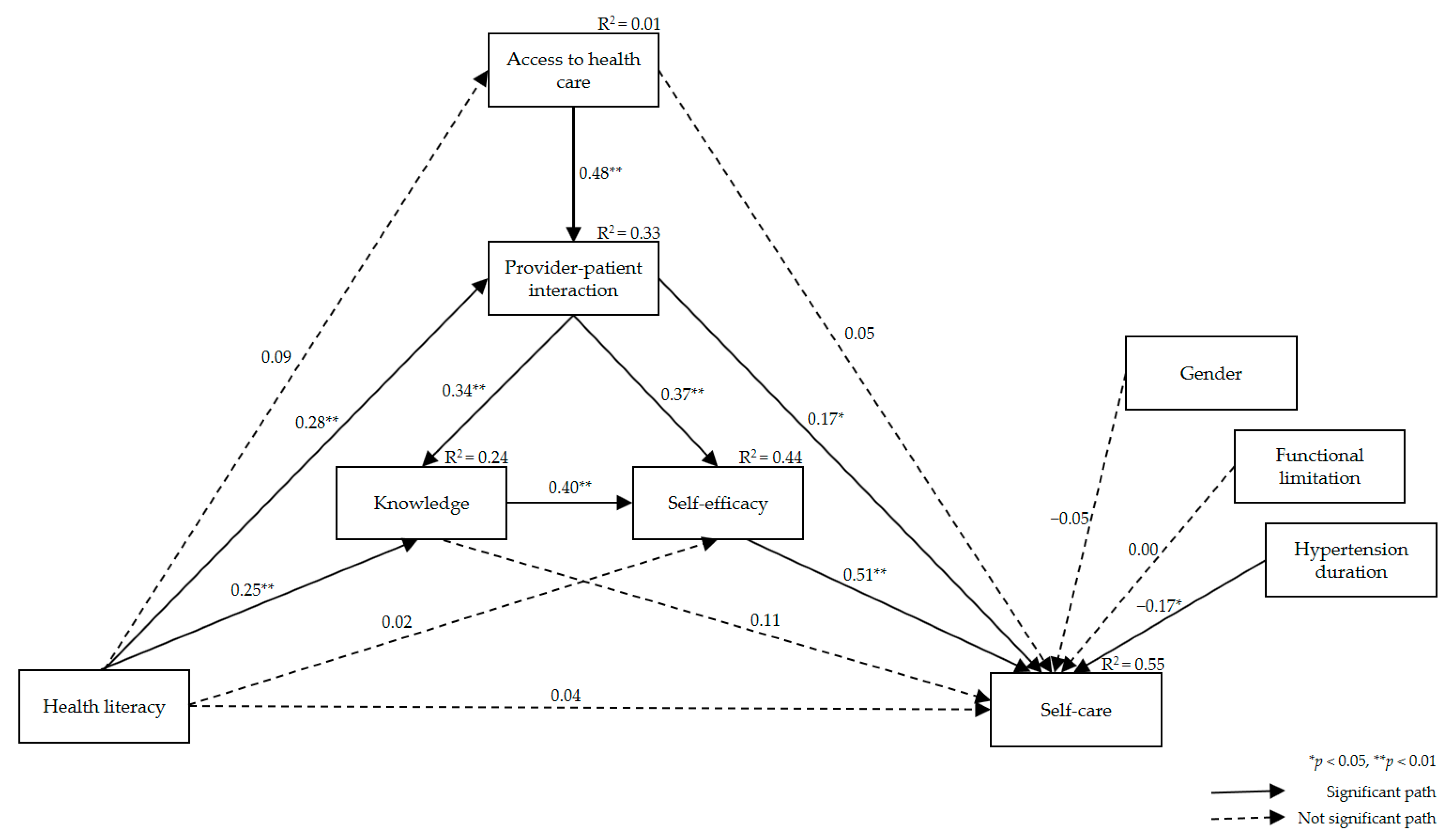
3.3. Fitness of the Hypothetical Path Model
3.4. Effect Analysis of the Multi-Mediation Model
3.5. Indirect Effect Analysis Using Phantom Variables
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- World Health Organization. Disability and Health; WHO Press: Geneva, Switzerland, 2020; Available online: https://www.who.int/news-room/fact-sheets/detail/disability-and-health (accessed on 10 January 2021).
- Krahn, G.L.; Walker, D.K.; Correa-De-Araujo, R. Person with disabilities as an unrecognized health disparity population. Am. J. Public Health 2015, 105, S198–S206. [Google Scholar] [CrossRef]
- Havercamp, S.M.; Scandlin, D.; Roth, M. Health disparities among adults with developmental disabilities, adults with other disabilities, and adults not reporting disability in North Carolina. Public Health Rep. 2004, 119, 418–426. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.; Lee, Y.; Oh, W.; Hwang, J.; Oh, M.; Lee, M.; Lee, N.; Oh, D.; Kang, D.; Kwon, S.; et al. 2017 National Survey of the Disabled Persons; Ministry of Health and Welfare, Korea Institute for Health and Social Affairs: Sejong, Korea, 2017. [Google Scholar]
- Ministry of Health and Welfare. 2020 Statistics of People with Disabilities Lives; Ministry of Health and Welfare: Sejong, Korea, 2020.
- Motlagh, S.F.Z.; Chaman, R.; Sadeghi, E.; Eslami, A.A. Self-care behaviors and related factors in hypertensive patients. Iran. Red. Crescent. Med. J. 2016, 18, e35805. [Google Scholar] [CrossRef] [Green Version]
- Son, Y.; Song, E.K. Impact of health literacy on disease-related knowledge and adherence to self-care in patients with hypertension. J. Korean. Acad. Fundam. Nurs. 2012, 19, 6–15. [Google Scholar] [CrossRef] [Green Version]
- Omisakin, F.D.; Ncama, B.P. Self, self-care and self-management concepts: Implications for self-management education. Edu. Res. 2011, 2, 1733–1737. [Google Scholar]
- Gazmararian, J.A.; Williams, M.V.; Peel, J.; Baker, D.W. Health literacy and knowledge of chronic disease. Patient Educ. Couns. 2003, 51, 267–275. [Google Scholar] [CrossRef]
- Poureslami, I.; Nimmon, L.; Rootman, I.; Fizgerald, M.J. Priorities for action: Recommendations from an international roundtable on health literacy and chronic disease management. Health Promot. Int. 2017, 32, 743–754. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Track 2: Health Literacy and Health Behavior. In Proceedings of the 7th Global Conference on Health Promotion, Nairobi, Kenya, 26–30 October 2009; WHO Press: Geneva, Switzerland. Available online: https://www.who.int/healthpromotion/conferences/7gchp/track2/en/ (accessed on 15 January 2021).
- Berkman, N.D.; Sheridan, S.L.; Donahue, K.E.; Halpern, D.J.; Crotty, K. Low health literacy and health outcomes: An updated systematic review. Ann. Intern. Med. 2011, 155, 97–107. [Google Scholar] [CrossRef] [PubMed]
- Chen, A.M.; Yehle, K.S.; Albert, N.M.; Ferraro, K.F.; Mason, H.L.; Murawski, M.M.; Plake, K.S. Relationships between health literacy and heart failure knowledge, self-efficacy, and self-care adherence. Res. Soc. Adm. Pharm. 2014, 10, 378–386. [Google Scholar] [CrossRef] [Green Version]
- Osborn, C.Y.; Paasche-Orlow, M.K.; Bailey, S.C.; Wolf, M.S. The mechanisms linking health literacy to behavior and health status. Am. J. Health Behav. 2011, 35, 118–128. [Google Scholar] [CrossRef] [Green Version]
- Aboumatar, H.J.; Carson, K.A.; Beach, M.C.; Roter, D.L.; Copper, L.A. The impact of health literacy on desire for participation in healthcare, medical visit communication, and patient reported outcomes among patients with hypertension. J. Gen. Intern. Med. 2013, 28, 1469–1476. [Google Scholar] [CrossRef]
- Hall, E.; Lee, S.; Clark, P.C.; Perilla, J. Social ecology of adherence to hypertension treatment in Latino migrant and seasonal farmworkers. J. Transcult. Nurs. 2014, 27, 33–41. [Google Scholar] [CrossRef] [Green Version]
- Shi, D.; Li, J.; Wang, Y.; Wang, S.; Liu, K.; Shi, R.; Zhang, Q.; Chen, X. Association between health literacy and hypertension management in a Chinese community: A retrospective cohort study. Intern. Emerg. Med. 2017, 12, 765–776. [Google Scholar] [CrossRef]
- Nguyen, J.; Gilbert, L. Health literacy among individuals with disabilities: A health information national trends survey analysis. Perm. J. 2019, 23, 19.034. [Google Scholar] [CrossRef]
- Johnston, M.V.; Diab, M.; Kim, S.S.; Kirshblum, S. Health literacy, morbidity, and quality of life among individuals with spinal cord injury. J. Spinal. Cord. Med. 2005, 28, 230–240. [Google Scholar] [CrossRef]
- Paasche-Orlow, M.K.; Wolf, M.S. The causal pathways linking health literacy to health outcomes. Am. J. Health Behav. 2007, 31, S19–S26. [Google Scholar] [CrossRef] [PubMed]
- Dennison, C.R.; McEntee, M.L.; Samuel, L.; Johnson, B.J.; Rotman, S.; Kielty, A.; Russell, S.D. Adequate health literacy is associated with higher heart failure knowledge and self care confidence in hospitalized patients. J. Cardiovasc. Nurs. 2011, 26, 359–367. [Google Scholar] [CrossRef] [Green Version]
- Macabasco-O’Connell, A.; DeWalt, D.A.; Broucksou, K.A.; Hawk, V.; Baker, D.W.; Schillinger, D.; Ruo, B.; Bibbins-Domingo, K.; Holmes, G.M.; Erman, B.; et al. Relationship between literacy, knowledge, self-care behaviors, and heart failure-related quality of life among patients with heart failure. J. Gen. Intern. Med. 2011, 26, 979–986. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McCleary-Jones, V. Health literacy and its association with diabetes knowledge, self-efficacy and disease self-management among African Americans with diabetes mellitus. ABNF J. 2011, 22, 25–32. [Google Scholar] [PubMed]
- Ministry of Health and Welfare. Policy for People with Disabilities; Ministry of Health and Welfare: Sejong, Korea, 2013. Available online: https://www.mohw.go.kr/react/policy/policy_bd_vw.jsp (accessed on 10 January 2021).
- Hoe, S.L. Issues and procedures in adopting structural equation modelling technique. J. Quant. Methods 2008, 3, 76–83. [Google Scholar]
- Lee, T.W.; Kang, S.J. Development of the short form of the Korean health literacy scale for the elderly. Res. Nurs. Health 2013, 36, 524–534. [Google Scholar] [CrossRef]
- Penchansky, R.; Thomas, J.W. The Concept of Access. Med. Care 1981, 19, 127–140. [Google Scholar] [CrossRef] [PubMed]
- Gil, E.; Oh, H. Testing a middle-range theory of self-care of chronic illness: A validation for Korean adult patients with severe hypertension. J. Korean Acad. Nurs. 2018, 48, 521–533. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.S. Impact of Shared Decision Making on Patient’s Satisfaction in Rheumatic Disease. Master’s Thesis, Hanyang University, Seoul, Korea, 2011. [Google Scholar]
- Lim, J.; Ko, G.P.; Han, E.; Jung, W.; Park, M.J.; Han, J.O. The Effects Assessment of Chronic Care Management Based on Primary Clinics for Hypertension, Diabetes Patients; Korea Health Promotion Institute: Seoul, Korea, 2012. [Google Scholar]
- Viera, A.J.; Cohen, L.W.; Mitchell, C.M.; Sloane, P.D. High blood pressure knowledge among primary care patients with known hypertension: A North Carolina Family Medicine Research Network (NC-FM-RN) study. J. Am. Board. Fam. Med. 2008, 21, 300–308. [Google Scholar] [CrossRef] [Green Version]
- Park, Y. An Effect of the Self-Regulation, Program for Hypertensives, Synthesis & Testing of Orem and Bandura’s Theory. Ph.D. Thesis, Seoul National University, Seoul, Korea, 1994. [Google Scholar]
- Lee, Y.H. A study of the effect of an efficacy expectation promoting program on self-efficacy and self-care. J. Korean Acad. Nurs. 1995, 7, 212–227. [Google Scholar]
- Washington Group on Disability Statistics. The Washington Group on Disability Short Set of Disability Questions; The U.S. National Center for Health Statistics: Hyattsville, MD, USA, 2020.
- Kim, H.Y. Statistical notes for clinical researchers: Assessing normal distribution (2) using skewness and kurtosis. Restor. Dent. Endod. 2013, 38, 52–54. [Google Scholar] [CrossRef]
- Nevitt, J.; Hancock, G.R. Performance of bootstrapping approaches to model test statistics and parameter standard error estimation in structural equation modeling. Structural Equ. Model. 2001, 8, 353–377. [Google Scholar] [CrossRef]
- Bollen, K.A.; Stine, R.A. Bootstrapping goodness-of-fit measures in structural equation models. Sociol. Methods Res. 1992, 21, 205–229. [Google Scholar] [CrossRef]
- Kim, G.S. AMOS Structural Equation Model Analysis; Hannarae: Seoul, Korea, 2013; pp. 120–132. [Google Scholar]
- Macho, S.; Ledermann, T. Estimating, testing, and comparing specific effects in structural equation models: The phantom model approach. Psychol. Methods 2011, 16, 34–43. [Google Scholar] [CrossRef]
- Kim, M.; Song, M. Effects of self-management program applying Dongsasub training on self-efficacy, self-esteem, self-management behavior and blood pressure in older adults with hypertension. J. Korean Acad. Nurs. 2015, 45, 576–586. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministry of Health. Disability and Primary Health: A Review of the Literacy; Te Pou o Te Whakaaro Nui: Wellington, New Zealand, 2013. Available online: https://www.donaldbeasley.org.nz/assets/publications/health/primary-health-and-disability-a-review-of-the-literature.pdf (accessed on 8 February 2021).
- Fisher, W.A.; Fisher, J.D.; Harman, J. The information-motivation-behavioral skills model: A general social psychological approach to understanding and promoting health behavior. Soc. Psychol. Found. Health Illn. 2003, 22, 82–106. [Google Scholar] [CrossRef]
- Schoenthaler, A.; Chaplin, W.F.; Allegrante, J.P.; Fernandez, S.; Diaz-Gloster, M.; Tobin, J.N.; Ogedegbe, G. Provider communication effects medication adherence in hypertensive African Americans. Patient. Educ. Couns. 2009, 75, 185–191. [Google Scholar] [CrossRef] [Green Version]
- Wallace, A. Low health literacy: Overview, assessment, and steps toward providing high-quality diabetes care. Diabetes Spectr. 2010, 23, 220–227. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.Y.; Lin, J.L. The effects of trust in physician on self-efficacy, adherence and diabetes outcomes. Soc. Sci. Med. 2009, 68, 1060–1068. [Google Scholar] [CrossRef] [PubMed]
- McColl, M.A.; Forster, D.; Shortt, S.E.; Hunter, D.; Dorland, J.; Godwin, M.; Rosser, W. Physician experiences providing primary care to people with disabilities. Health Policy 2008, 4, e129. [Google Scholar] [CrossRef] [Green Version]
- Levy, H.; Janke, A. Health literacy and access to care. J. Health Commun. 2016, 21, 43–50. [Google Scholar] [CrossRef]
- Harrington, A.L.; Hirsch, M.A.; Hammond, F.M.; Norton, H.J.; Bockenek, W.L. Assessment of primary care services and perceived barriers to care in persons with disabilities. Am. J. Phys. Med. Rehabil. 2009, 88, 852–863. [Google Scholar] [CrossRef]
- Jeon, B.; Kwon, S.; Kim, H. Health care utilization by people with disabilities: A longitudinal analysis of the Korea Welfare Panel Study (KoWePS). Disabil. Health J. 2015, 8, 353–362. [Google Scholar] [CrossRef]
- Shin, H.I. Strategic Research for Improving the Disabled People’s Health; Ministry of Health and Welfare: Sejong, Korea, 2015.
- Ahn, Y.H.; Ham, O.K. Factors associated with medication adherence among Medical-aid beneficiaries with hypertension. West. J. Nurs. Res. 2016, 38, 1298–1312. [Google Scholar] [CrossRef] [PubMed]
- Rios, D.; Magasi, S.; Novak, C.; Harniss, M. Conducting accessible research: Including people with disabilities in public health, epidemiological, and outcomes studies. Am. J. Public Health 2016, 106, 2137–2144. [Google Scholar] [CrossRef]
- Taber, K.S. The use of Cronbach’s alpha when developing and reporting research instruments in science education. Res. Sci. Educ. 2018, 48, 1273–1296. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Categories | n (%) or Mean ± SD |
|---|---|---|
| Gender | Male | 70 (33.2) |
| Female | 141 (66.8) | |
| Age (year) | 42.09 ± 8.98 | |
| 20~29 | 11 (5.2) | |
| 30~39 | 79 (37.4) | |
| 40~49 | 95 (45.0) | |
| 50~59 | 14 (6.6) | |
| ≥60 | 12 (5.7) | |
| Marital status | With spouse | 123 (58.3) |
| No spouse | 88 (41.7) | |
| Level of education | ≤Middle school | 12 (5.7) |
| High school | 108 (51.2) | |
| ≥College | 91 (43.1) | |
| Monthly household income (KRW 1000) | <100 | 39 (18.5) |
| 100~199 | 62 (29.4) | |
| 200~299 | 70 (33.2) | |
| 300~399 | 32 (15.2) | |
| ≥400 | 8 (3.7) | |
| Disability severity 1 | Mild | 135 (64.0) |
| Severe | 76 (36.0) | |
| Functional limitation | No | 108 (51.2) |
| Yes 2 | 103 (48.8) | |
| Duration of hypertension (month) | 47.03 ± 55.01 | |
| Health literacy | 11.45 ± 0.79 (range 6–12) | |
| Hypertension self-care | 57.23 ± 7.91 (range 33–74) | |
| Access to healthcare | 16.23 ± 2.87 (range 5–25) | |
| Provider–patient interaction | 24.94 ± 4.82 (range 9–35) | |
| Hypertension knowledge | 3.93 ± 1.77 (range 0–7) | |
| Hypertension control self-efficacy | 66.67 ± 14.42 (range 19–100) | |
| Variables | X1 | X2 | X3 | X4 | X5 | X6 | X7 | X8 | X9 |
|---|---|---|---|---|---|---|---|---|---|
| Pearson’s Correlation Coefficient | |||||||||
| Health literacy | 1 | ||||||||
| Access to healthcare | 0.09 | 1 | |||||||
| Provider–patient interaction | 0.32 *** | 0.50 *** | 1 | ||||||
| Knowledge | 0.36 *** | 0.20 ** | 0.43 *** | 1 | |||||
| Self-efficacy | 0.28 *** | 0.33 *** | 0.55 *** | 0.57 *** | 1 | ||||
| Self-care | 0.28 *** | 0.48 *** | 0.33 *** | 0.53 *** | 0.68 *** | 1 | |||
| Gender | −0.14 * | 0.10 | 0.01 | 0.08 | 0.16 * | 0.04 | 1 | ||
| Functional limitation | −0.05 | −0.05 | −0.02 | −0.06 | −0.05 | −0.05 | −0.02 | 1 | |
| Duration of hypertension | 0.06 | −0.02 | 0.09 | 0.13 | 0.10 | −0.09 | 0.01 | 0.01 | 1 |
| Pathways | Estimate | SE | 95% CI 1 | p | ||
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| Health literacy → Access to healthcare → Self-care | 0.05 | 0.10 | −0.07 | 0.36 | 0.394 | |
| Health literacy → Access to healthcare → Provider–patient interaction | → Self-care | 0.07 | 0.08 | −0.04 | 0.30 | 0.206 |
| → Knowledge → Self-care | 0.02 | 0.02 | −0.01 | 0.09 | 0.169 | |
| → Knowledge → Self-efficacy → Self-care | 0.03 | 0.03 | −0.02 | 0.10 | 0.229 | |
| → Self-efficacy → Self-care | 0.08 | 0.09 | −0.06 | 0.29 | 0.284 | |
| Health literacy → Provider–patient interaction | → Self-care | 0.48 | 0.24 | 0.09 | 1.07 | 0.018 |
| → Knowledge → Self-efficacy → Self-care | 0.20 | 0.07 | 0.11 | 0.39 | <0.001 | |
| → Knowledge → Self-care | 0.11 | 0.07 | 0.00 | 0.27 | 0.059 | |
| → Self-efficacy → Self-care | 0.54 | 0.25 | 0.21 | 1.11 | 0.001 | |
| Health literacy → Knowledge | → Self-efficacy → Self-care | 0.53 | 0.29 | 0.16 | 1.24 | 0.001 |
| → Self-care | 0.28 | 0.21 | −0.01 | 0.85 | 0.059 | |
| Health literacy → Self-efficacy → Self-care | 0.09 | 0.40 | −0.80 | 0.76 | 0.818 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nam, H.J.; Yoon, J.Y. Linking Health Literacy to Self-Care in Hypertensive Patients with Physical Disabilities: A Path Analysis Using a Multi-Mediation Model. Int. J. Environ. Res. Public Health 2021, 18, 3363. https://doi.org/10.3390/ijerph18073363
Nam HJ, Yoon JY. Linking Health Literacy to Self-Care in Hypertensive Patients with Physical Disabilities: A Path Analysis Using a Multi-Mediation Model. International Journal of Environmental Research and Public Health. 2021; 18(7):3363. https://doi.org/10.3390/ijerph18073363
Chicago/Turabian StyleNam, Hye Jin, and Ju Young Yoon. 2021. "Linking Health Literacy to Self-Care in Hypertensive Patients with Physical Disabilities: A Path Analysis Using a Multi-Mediation Model" International Journal of Environmental Research and Public Health 18, no. 7: 3363. https://doi.org/10.3390/ijerph18073363
APA StyleNam, H. J., & Yoon, J. Y. (2021). Linking Health Literacy to Self-Care in Hypertensive Patients with Physical Disabilities: A Path Analysis Using a Multi-Mediation Model. International Journal of Environmental Research and Public Health, 18(7), 3363. https://doi.org/10.3390/ijerph18073363