
Social Telepresence Robots: A Narrative Review of Experiments Involving Older Adults before and during the COVID-19 Pandemic

Abstract
:1. Introduction
1.1. Social Isolation of the Elderly
1.2. Technologies That Help to Reduce Loneliness: Telepresence Robots
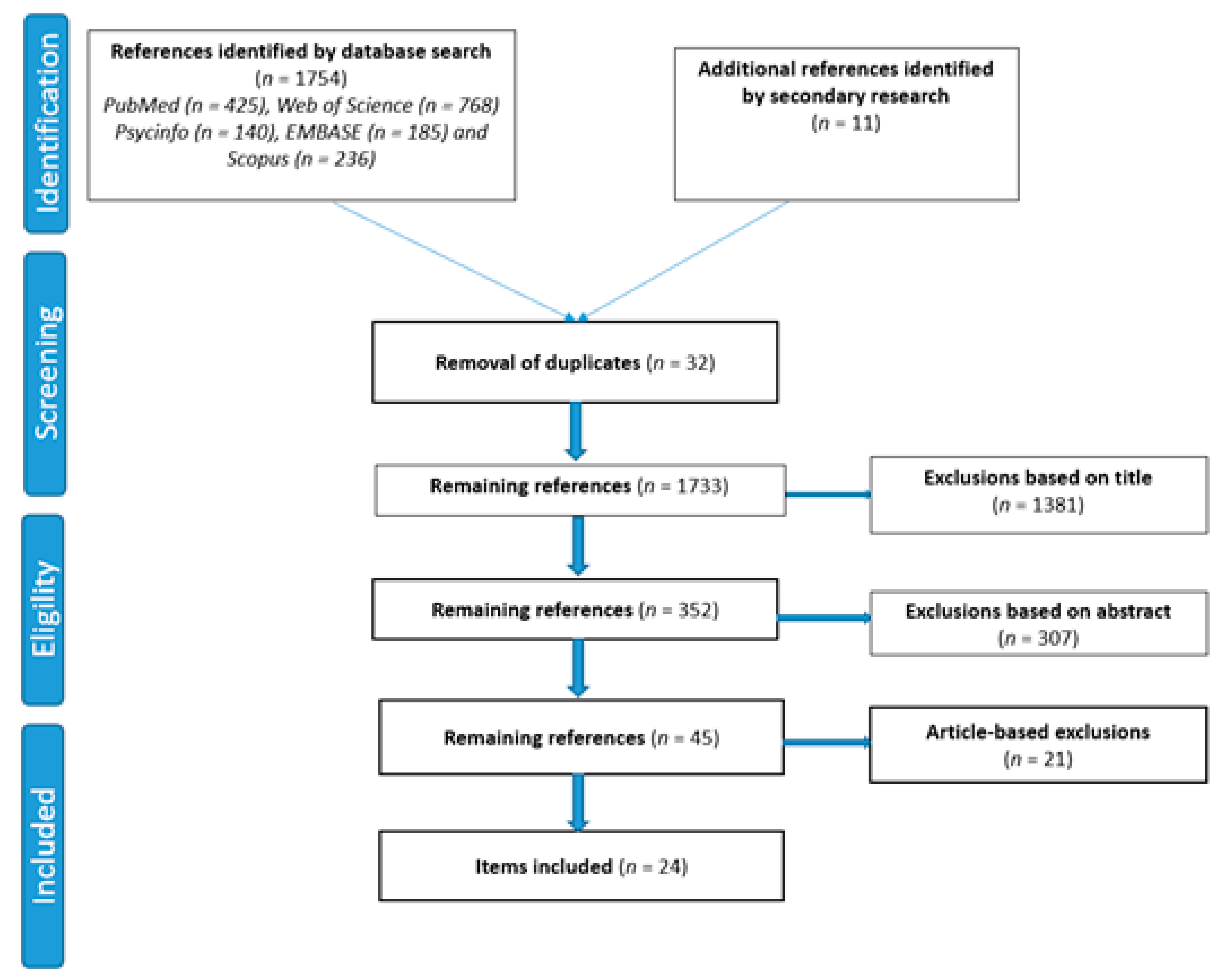
2. Materials and Methods
2.1. Information Sources and Research Method
2.2. Criteria for Inclusion, Exclusion, and Data Extraction
3. Results
3.1. General Data
3.2. Description of Studies Using HTA Dimensions including Topics and Issues When Available
3.2.1. Health Problem and Current Use of the Technology (CUR)
Utilization of MTR
3.2.2. Description and Technical Characteristics of Technology (TEC)
Features of MTR
Training Needed to Use MTR
3.2.3. Safety (SAF)
Patient Safety with MTR
3.2.4. Clinical Effectiveness of Robotic Interventions (EFF)
Patient Satisfaction with MTR
Health-Related Quality of Life and MTR Use
Morbidity and MTR Use
3.2.5. Organizational Aspects (ORG)
Health Delivery Process Using MTR
Culture (Professionals MTR Acceptance)
3.2.6. Medico-Economic Aspects (ECO)
Resource Utilization
3.2.7. Ethical Aspects (ETH)
Benefit–Harm Balance
Autonomy
Respect for Persons
3.2.8. Patients and Social Aspects (SOC)
OAs’ Perspectives on MTR
Communication Aspects on MTR
3.2.9. Legal Aspects (LEG)
4. Discussion
Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Holt-Lunstad, J.; Robles, T.F.; Sbarra, D.A. Advancing social connection as a public health priority in the United States. Am. Psychol. 2017, 72, 517–530. [Google Scholar] [CrossRef] [PubMed]
- Les Petits Frères Des Pauvres. Solitude et Isolement Quand on a Plus de 60 ans en France en 2017. 2017. Available online: https://www.petitsfreresdespauvres.fr/informer/nos-actualites/solitude-et-isolement-quand-on-a-plus-de-60-ans-en-france-en-2017 (accessed on 12 June 2020).
- Ministère des Solidarites et de la Sante. Personnes âgées: Les Chiffres Clés; Ministère des Solidarites et de la Sante: Paris, France, 2018; Available online: https://solidarites-sante.gouv.fr/archives/loi-relative-a-l-adaptation-de-la-societe-au-vieillissement/article/personnes-agees-les-chiffres-cles (accessed on 22 June 2020).
- European Commision. Mental Health. 2018. Available online: https://ec.europa.eu/health/non_communicable_diseases/mental_health_fr (accessed on 7 July 2020).
- Simard, J.; Volicer, L. Loneliness and isolation in long-term care and the COVID-19 pandemic. J. Am. Med. Dir. Assoc. 2020, 21, 966–967. [Google Scholar] [CrossRef] [PubMed]
- Gilmour, H.; Ramage-Morin, P.L. Isolement social et mortalité chez les personnes agées au Canada. Rep. Sante 2020, 31, 29–41. [Google Scholar] [CrossRef]
- Tsuji, T.; Saito, M.; Ikeda, T.; Aida, J.; Cable, N.; Koyama, S.; Kondo, K. Change in the prevalence of social isolation among the older population from 2010 to 2016: A repeated cross-sectional comparative study of Japan and England. Arch. Gerontol. Geriatr. 2020, 91, 104237. [Google Scholar] [CrossRef] [PubMed]
- van Dyck, L.I.; Wilkins, K.M.; Ouellet, J.; Ouellet, G.M.; Conroy, M.L. Combating heightened social isolation of nursing home elders: The telephone outreach in the COVID-19 outbreak program. Am. J. Geriatr. Psychiatry 2020, 28, 989–992. [Google Scholar] [CrossRef] [PubMed]
- Peretti-Watel, P. Lien social et santé en situation de précarité: État de santé, recours aux soins, abus d’alcool et réseau relationnel parmi les usagers des services d’aide. Econ. Stat. 2006, 391, 115–130. [Google Scholar] [CrossRef]
- Holwerda, T.J.; Deeg, D.J.H.; Beekman, A.T.F.; van Tilburg, T.G.; Stek, M.L.; Jonker, C.; Schoevers, R.A. Feelings of loneliness, but not social isolation, predict dementia onset: Results from the Amsterdam Study of the Elderly (AMSTEL). J. Neurol. Neurosurg. Psychiatry 2014, 85, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Hoertel, N.; Crochard, A.; Rouillon, F.; Limosin, F. L’alcool en France et ses conséquences médicales et sociales: Regard de l’entourage et des médecins généralistes. L’ Encéphale 2014, 40, S11–S31. [Google Scholar] [CrossRef]
- Luo, Y.; Hawkley, L.C.; Waite, L.J.; Cacioppo, J.T. Loneliness, health, and mortality in old age: A national longitudinal study. Soc. Sci. Med. 2012, 74, 907–914. [Google Scholar] [CrossRef] [Green Version]
- Patterson, A.C.; Veenstra, G. Loneliness and risk of mortality: A longitudinal investigation in Alameda County, California. Soc. Sci. Med. 2010, 71, 181–186. [Google Scholar] [CrossRef]
- Cacioppo, S.; Grippo, A.J.; London, S.; Goossens, L.; Cacioppo, J.T. Loneliness: Clinical import and interventions. Perspect. Psychol. Sci. 2015, 10, 238–249. [Google Scholar] [CrossRef] [Green Version]
- Khosravi, P.; Rezvani, A.; Wiewiora, A. The impact of technology on older adults’ social isolation. Comput. Hum. Behav. 2016, 63, 594–603. [Google Scholar] [CrossRef]
- Scassellati, B.; Vázquez, M. The potential of socially assistive robots during infectious disease outbreaks. Sci. Robot. 2020, 5, eabc9014. [Google Scholar] [CrossRef]
- Tavakoli, M.; Carriere, J.; Torabi, A. Robotics, smart wearable technologies, and autonomous intelligent systems for healthcare during the COVID-19 pandemic: An analysis of the state of the art and future vision. Adv. Intell. Syst. 2020, 2, 2000071. [Google Scholar] [CrossRef]
- Sheridan, T.B. Musings on Telepresence and Virtual Presence. Presence Teleoper. Virtual Environ. 1992, 1, 120–126. [Google Scholar] [CrossRef]
- Beer, J.M.; Takayama, L. Mobile Remote Presence Systems for Older Adults: Acceptance, Benefits, and Concerns. In Proceedings of the 6th International Conference on Human-Robot Interaction, Lausanne, Switzerland, 6–9 March 2011; pp. 19–26. [Google Scholar]
- Kristoffersson, A.; Coradeschi, S.; Loutfi, A. A Review of mobile robotic telepresence. Adv. Hum. Comput. Interact. 2013, 1–17. [Google Scholar] [CrossRef]
- Robot Beam. AWABOT beyond Robotic. Available online: https://awabot.com (accessed on 19 September 2020).
- Robot Double. Doublerobotics. Available online: https://www.doublerobotics.com (accessed on 19 September 2020).
- Robot Cutii. CareClever. Available online: https://www.cutii.io (accessed on 21 September 2020).
- Robot Kompai. Kompairobotics. Available online: http://kompairobotics.com/fr (accessed on 25 September 2020).
- Shishehgar, M.; Kerr, D.; Blake, J. The effectiveness of various robotic technologies in assisting older adults. Health Inform. J. 2019, 25, 892–918. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cesta, A.; Cortellessa, G.; Orlandini, A.; Tiberio, L. Long-term evaluation of a telepresence robot for the elderly: Methodology and ecological case study. Int. J. Soc. Robot. 2016, 8, 421–441. [Google Scholar] [CrossRef] [Green Version]
- HTAi-INAHTA International. Available online: https://htai.org/ (accessed on 26 January 2021).
- Williams, T.; May, C.; Mair, F.; Mort, M.; Gask, L. Normative models of health technology as-sessment and the social production of evidence about telehealth care. Health Policy 2003, 64, 39–54. [Google Scholar] [CrossRef]
- Moyle, W.; Arnautovska, U.; Ownsworth, T.; Jones, C. Potential of telepresence robots to enhance social connectedness in older adults with dementia: An integrative review of feasibility. Int. Psychogeriatr. 2017, 29, 1951–1964. [Google Scholar] [CrossRef]
- O’Rourke, B.; Oortwijn, W.; Schuller, T. The new definition of health technology assessment: A milestone in international collaboration. Int. J. Technol. Assess. Health Care 2020, 36, 187–901. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Health Technology Assessment of Medical Devices; (WHO Medical Device Technical Series); World Health Organization: Geneva, Switzerland, 2011; Available online: https://apps.who.int/iris/bitstream/handle/10665/44564/9789241501361-eng.pdf (accessed on 26 January 2021).
- EUnetHTA. HTA Core Model ® version 3.0. Available online: www.htacoremodel.info/BrowseModel.aspx (accessed on 26 January 2021).
- European Network of Health Technology Assessment. Available online: www.eunethta.eu (accessed on 12 December 2020).
- Bakas, T.; Sampsel, D.; Israel, J.; Chamnikar, A.; Bodnarik, B.; Clark, J.G.; Vanderelst, D. Using telehealth to optimize healthy independent living for older adults: A feasibility study. Geriatr. Nurs. 2018, 39, 566–573. [Google Scholar] [CrossRef] [PubMed]
- Baisch, S.; Kolling, T.; Schall, A.; Rühl, S.; Selic, S.; Kim, Z.; Knopf, M. Acceptance of social robots by elder people: Does psychosocial functioning matter? Int. J. Soc. Robot. 2017, 9, 293–307. [Google Scholar] [CrossRef]
- Boman, I.L.; Bartfai, A. The first step in using a robot in brain injury rehabilitation: Patients’ and health-care professionals’ perspective. Disabil. Rehabil. Assist. Technol. 2015, 10, 365–370. [Google Scholar] [CrossRef]
- Broadbent, E.; Kerse, N.; Peri, K.; Robinson, H.; Jayawardena, C.; Kuo, T.; Amor, M. Benefits and problems of health-care robots in aged care settings: A comparison trial. Austral. J. Ageing 2016, 35, 23–29. [Google Scholar] [CrossRef]
- Caleb-Solly, P.; Dogramadzi, S.; Huijnen, C.A.; Heuvel, H.V.D. Exploiting ability for human adaptation to facilitate improved human-robot interaction and acceptance. Inf. Soc. 2018, 34, 153–165. [Google Scholar] [CrossRef]
- Cavallo, F.; Esposito, R.; Limosani, R.; Manzi, A.; Bevilacqua, R.; Felici, E.; Dario, P. Robotic services acceptance in smart environments with older adults: User satisfaction and acceptability study. J. Med. Internet Res. 2018, 20, e264. [Google Scholar] [CrossRef] [PubMed]
- Cesta, A.; Cortellessa, G.; Orlandini, A.; Tiberio, L. Addressing the Long-Term Evaluation of a Telepresence Robot for the Elderly. In Proceedings of the 4th International Conference on Agents and Artificial Intelligence (ICAART), Algarve, Portugal, 6–8 March 2012; pp. 652–663. [Google Scholar]
- Gerłowska, J.; Skrobas, U.; Grabowska-Aleksandrowicz, K.; Korchut, A.; Szklener, S.; Szczęśniak-Stańczyk, D.; Rejdak, K. Assessment of perceived attractiveness, usability, and societal impact of a multimodal robotic assistant for aging patients with memory impairments. Front. Neurol. 2018, 9, 392. [Google Scholar] [CrossRef]
- Gonzalez-Jimenez, J.; Galindo, C.; Gutierrez-Castaneda, C. Evaluation of a telepresence robot for the elderly: A spanish experience. In International Work-Conference on the Interplay between Natural and Artificial Computation; Springer: Berlin/Heidelberg, Germany, 2013; pp. 141–150. [Google Scholar]
- Granata, C.; Pino, M.; Legouverneur, G.; Vidal, J.S.; Bidaud, P.; Rigaud, A.S. Robot services for elderly with cognitive impairment: Testing usability of graphical user interfaces. Technol. Health Care 2013, 21, 217–231. [Google Scholar] [CrossRef]
- Hiyama, A.; Kosugi, A.; Fukuda, K.; Kobayashi, M.; Hirose, M. Facilitating remote communication between senior communities with telepresence robots. In International Conference on Human Aspects of IT for the Aged Population; Springer: Cham, Switzerland, 2017; pp. 501–515. [Google Scholar]
- Koceski, S.; Koceska, N. Evaluation of an assistive telepresence robot for elderly healthcare. J. Med. Syst. 2016, 40, 121. [Google Scholar] [CrossRef] [PubMed]
- Kristoffersson, A.; Coradeschi, S.; Loutfi, A.; Severinson-Eklundh, K. Assessment of interaction quality in mobile robotic telepresence: An elderly perspective. Interact. Stud. 2014, 15, 343–357. [Google Scholar] [CrossRef] [Green Version]
- Moyle, W.; Jones, C.; Cooke, M.; O’Dwyer, S.; Sung, B.; Drummond, S. Connecting the person with dementia and family: A feasibility study of a telepresence robot. BMC Geriatr. 2014, 14, 7. [Google Scholar] [CrossRef] [Green Version]
- Niemelä, M.; van Aerschot, L.; Tammela, A.; Aaltonen, I. A telepresence robot in residential care: Family increasingly present, personnel worried about privacy. In International Conference on Social Robotics; Springer: Cham, Switzerland, 2017; pp. 85–94. [Google Scholar]
- Pineau, J.; Montemerlo, M.; Pollack, M.; Roy, N.; Thrun, S. Towards robotic assistants in nursing homes: Challenges and results. Robot. Auton. Syst. 2003, 42, 271–281. [Google Scholar] [CrossRef]
- Schroeter, C.; Mueller, S.; Volkhardt, M.; Einhorn, E.; Huijnen, C.; van den Heuvel, H.; Gross, H.M. Realization and User Evaluation of a Companion Robot for People with Mild Cognitive Impairments. In Proceedings of the 2013 IEEE International Conference on Robotics and Automation, Karlsruhe, Germany, 6–10 March 2003; pp. 1153–1159. [Google Scholar]
- Seelye, A.M.; Wild, K.V.; Larimer, N.; Maxwell, S.; Kearns, P.; Kaye, J.A. Reactions to a remote-controlled video-communication robot in seniors’ homes: A pilot study of feasibility and acceptance. Telemed. E-Health 2012, 18, 755–759. [Google Scholar] [CrossRef] [PubMed]
- Stafford, R.Q.; MacDonald, B.A.; Jayawardena, C.; Wegner, D.M.; Broadbent, E. Does the robot have a mind? Mind perception and attitudes towards robots predict use of an eldercare robot. Int. J. Soc. Robot. 2014, 6, 17–32. [Google Scholar] [CrossRef]
- Tiberio, L.; Cesta, A.; Cortellessa, G.; Padua, L.; Pellegrino, A.R. Assessing Affective Response of Older Users to a Telepresence Robot Using a Combination of Psychophysiological Measures. In Proceedings of the 2012 IEEE RO-MAN: The 21st IEEE International Symposium on Robot and Human Interactive Communication, Paris, France, 9–13 September 2012; pp. 833–838. [Google Scholar]
- Wu, Y.H.; Wrobel, J.; Cornuet, M.; Kerhervé., H.; Damnée, S.; Rigaud, A.S. Acceptance of an assistive robot in older adults: A mixed-method study of human–robot interaction over a 1-month period in the Living Lab setting. Clin. Interv. Aging 2014, 9, 801. [Google Scholar] [CrossRef] [Green Version]
- Zsiga, K.; Tóth, A.; Pilissy, T.; Péter, O.; Dénes, Z.; Fazekas, G. Evaluation of a companion robot based on field tests with single older adults in their homes. Assist. Technol. 2018, 30, 259–266. [Google Scholar] [CrossRef]
- Devillers, L. Des Robots et des Hommes; Plon: Paris, France, 2017. [Google Scholar]
- Young, J.E.; Sung, J.; Voida, A.; Sharlin, E.; Igarashi, T.; Christensen, H.I.; Grinter, R.E. Evaluating human-robot interaction. Int. J. Soc. Robot. 2011, 3, 53–67. [Google Scholar] [CrossRef]
- Mori, M.; MacDorman, K.F.; Kageki, N. The Uncanny Valley. IEEE Robot. Automat. Mag. 2012, 19, 98–100. [Google Scholar] [CrossRef]
- Ono, S.K.; Andraus, W.; Terrabuio, D.R.B.; Cobello-Júnior, V.; Arai, L.; Ducatti, L.; Carrilho, F.J. Technological Innovation in Outpatient Assistance for Chronic Liver Disease and Liver Transplant Patients During the Coronavirus Disease Outbreak: A Method to Minimize Transmission. Clinics 2020, 75. [Google Scholar] [CrossRef]
- AWABOT Téléprésence en EHPAD: Un Dispositif Solidaire Pour Maintenir le lien entre les Familles et les Résidents. Available online: https://awabot.com/ehpad-telepresence-confinement-coronavirus/ (accessed on 5 November 2020).
- Reuters, T. Tommy l’ Infirmière Robot Aide à Protéger les Médecins Italiens du Coronavirus. Available online: https://www.reuters.com/article/us-health-coronavirus-italy-robots/tommy-the-robot-nurse-helps-keep-italy-doctors-safe-from-coronavirus-idUSKBN21J67Y (accessed on 5 November 2020).



{kind=link}
{kind=link}
| Domains | Main Features |
|---|---|
| Health and current use of the technology (CUR) | A description of the condition targeted by the technology, the therapeutic purpose of the intervention, and the current standard treatment to address it. |
| Description and technical characteristics of technology (TEC) | A description of the technical features of the technology, its level of maturity, the resources (material, infrastructural, etc.), and skills required to use it. |
| Safety (SAF) | A description of the risk and unwanted effects caused by the technology, and the way to prevent and manage it. |
| Clinical effectiveness (EFF) | A description of the effects of the intervention on the ability to reach the clinical objectives set for the intervention, on the condition of the quality of life and the autonomy of the users, as well as on the follow up conduct by the professionals who take part in the intervention |
| Costs and economic evaluation (ECO) | A description of the costs, the health-related outcomes, and economic efficiency of the technology. |
| Ethical analysis (ETH) | A description of issues related to ethic and values when using the health technology. |
| Organizational aspects (ORG) | A description of the allocation of resources (material artefacts, skills, knowledge, money, work culture, etc.) required to implement the technology in the organization and the healthcare system. |
| Patients and social aspects (SOC) | A description of the representations conveyed by the intervention at the individual’s and collective’s levels, for the patients, their entourage, the caregivers, and society as a whole. |
| Legal aspects (LEG) | A description of regulations and laws to be considered in evaluating a technological intervention. |
| Study | Country | MTR Model (Manufacturer) | Setting | Time Period | Assessment Objective |
|---|---|---|---|---|---|
| Bakas et al. (2018) [34] | USA | VGO Communications (VGO) | Home | 3 weeks | Study 1: Feasibility Study 2: Clinical impact in a randomized controlled trial (2 groups, with and without robot) |
| Baisch et al. (2017) [35] | Germany | Giraff (GiraffPlus) and Paro (national institute of advanced industrial science and technology) | Laboratory | 1 day | Technology acceptance (investigation of the influence of psychosocial factors) |
| Beer et al. (2011) [19] | USA | MTR Texai project (Willow Garage) | Laboratory | 1 day | Technology acceptance and usability |
| Boman and Bartfai (2014) [36] | Sweden | Giraff (GiraffPlus) | Hospital | 1 day | Usability and user experience |
| Broadbent et al. (2016) [37] | New Zealand | Guide and Cafero | Senior housing | 12 weeks | Clinical impact in a controlled trial (2 groups, with and without robot); technology acceptance; organizational impact |
| Caleb-Solly et al. (2018) [38] | England and the Netherlands | Kompai (Kompai Robotics) | Laboratory | 2 days | Usability and user experience |
| Cavallo et al. (2018) [39] | Italy | Robot ERA-Scitos G5 (MetraLabs) | Laboratory | 1 day | Technology acceptance |
| Cesta et al. (2012) [40] | Italy | Giraff (GiraffPlus) | Laboratory | 1 day | Technology acceptance and usability |
| Cesta et al. (2016) [26] | Italy | Giraff (GiraffPlus) | Laboratory | 12 months | Clinical impact; technology acceptance and user experience |
| Gertowska et al. (2013) [41] | Poland | Robot assistant for MCI patient at home (RAMCIP) | Hospital | 1 day | Technology acceptance and usability; social impact |
| Gonzalez-Jimelez et al. (2013) [42] | Spain | Giraff (GiraffPlus) | Home | 12–18 months | Technology acceptance |
| Granata et al. (2013) [43] | France | Kompai (Kompai Robotics) | Laboratory | 1 day | Usability and user experience |
| Hiyama et al. (2017) [44] | Japan | Double (Double robotics) and Kubi (Xandex In) | Laboratory | 5 days | Technology acceptance and usability |
| Koceski and Koceska (2016) [45] | Macedonia | MTR (academic research) | Nursing home | 1 day | Technology acceptance |
| Kristoffersson et al. (2014) [46] | Sweden | Giraff (GiraffPlus) | Laboratory | 1 day | Usability (positioning of the robot) |
| Moyle et al. (2014) [47] | Australia | Giraff (GiraffPlus) | Long-term care unit | 4 months | Feasibility and technology acceptance |
| Niemela et al. (2019) [48] | Finland | Double (Double robotics) | Nursing home | 12 weeks | Technology acceptance and user experience |
| Pineau et al. (2003) [49] | USA | Nursebot Pearl (academic research) | Nursing home | 1 day | Feasibility and technology acceptance |
| Schroeter et al. (2013) [50] | The Netherlands | Scitos G3 (MetraLabs) | Laboratory | 2 days | Technology acceptance and usability; social impact |
| Seelye et al. (2012) [51] | USA | MTR-VGO system (VGO) | Home | 2 days | Technology acceptance and usability |
| Stafford et al. (2014) [52] | New Zealand | Healthbot (Yujin Robot) | Senior housing | 2 weeks | Feasibility and technology acceptance |
| Tiberio et al. (2012) [53] | Italy | Giraff (GiraffPlus) | Laboratory | 4 days | Clinical impact (psychophysiological responses to the robot) |
| Wu et al. (2014) [54] | France | Kompai (Kompai Robotics) | Laboratory | 4 weeks | Technology acceptance |
| Zsiga et al. (2017) [55] | Hungary | Kompai (Kompai Robotics) | Home | 2–4 months | Technology acceptance and usability |
| Study | Population | Assessment Indicators (Method) | Benefits of MTR Ise | Impact on Social Isolation | If Yes, Which | Barriers to MTR Use | ||
|---|---|---|---|---|---|---|---|---|
| Older Adults (OAs) | Professionals | Family Members | ||||||
| Bakas et al. (2018) [34] | Polypathological OAs Study 1, n = 5 Study 2, n = 22 | Nurses (n = NP) | NA | Number of “bad days”, depression, stress, fatigue, pain, shortness of breath, sleep, quality of life, confidence pre- and post-intervention (scales) | Good feasibility; improvement in the number of “bad days”, depression, sleep, quality of life, confidence in managing one’s own health | No | NA | Training of nurses to handle the robot’s displacement |
| Baisch et al. (2017) [35] | Healthy OAs (n = 29) | NA | NA | Loneliness, depressed mood, life satisfaction, social support (scales) | Regarding Giraff, good acceptability for AOs with limited social support who can control the robot; regarding Paro, no association between acceptability and psychosocial variables. | Yes | Improvement of social contact but reduction of emotional impact compared to personal visit | Regarding Giraff: lack of autonomy (is easily rendered useless if the help of a third party is needed to handle it); it is difficult for the main user to have full control of the robot |
| Beer et al. (2011) [19] | Healthy OAs (n = 12) | NA | NA | Perceived benefits and concerns; suggestions for use cases, recommendations on system design (semi-structured interviews) | Positive feedback from the camera device, helps reduce travel, can provide assistance in health diagnostics; expressed desire to use the robot in the future. | Yes | Reduction of social isolation | OAs concerns: lack of privacy, lack of real contact, ease of use, excessive or inappropriate use; expressed desire to know the capabilities and cost of the device before use |
| Boman and Bartfai (2014) [36] | OAs cognitive impairment (n = 3) | Nurses (n = 38); assistant night nurses (n = 10); occupational therapists (n = 3) | NA | Expectations, usability, and usefulness of the MTR (questionnaire, Likert scale, and open-ended interview) | OAs: very satisfied, easy to use and pleasant system, increases the feeling of security; Pro: positive experience | No | NA | Professionals: a lot of time for training—difficulties in handling the robot and interacting with the OAs at the same time, difficulties in emergency response, privacy concerns |
| Broadbent et al. (2016) [37] | OAs: healthy and with cognitive impairment (n = 52) | Care workers (n= 53) | NA | OAs: Depression, quality of life, mobility, activities of daily living (scales); Pro: job satisfaction, demoralization, attitude towards robots (scales) | OAs: no difference in the scale scores between the two groups; positive, neutral, or negative reactions and opinions of robots; Pro: rather positive opinion of robots | No | NA | Robots difficult to use in OAs with cognitive deficit or motor disability |
| Caleb-Solly et al. (2018) [38] | OAs: healthy and with cognitive impairment (n = 11) | NA | NA | Usability (questionnaire), satisfaction, perceived usefulness, privacy concerns (semi-structured interviews) | Adequate usability and acceptance | No | NA | Need to prepare users for the real capabilities of the robot: many technical constraints, need for realistic expectations towards robot use. |
| Cavallo et al. (2018) [39] | Healthy OAs (n = 45) | NA | NA | Acceptance, perceived robustness (semi-structured interviews), questionnaire of appearance | Good acceptance of robots; appearance and services appreciated, no privacy concerns, no anxiety about using the robot | No | NA | Previous familiarization necessary, importance of combining anthropomorphic and machine features for robots, appropriate robot size (150 cm) |
| Cesta et al. (2012) [40] | Healthy OAs (n = 10) | Nurses (n = 26) | NA | Technology acceptance, usability, satisfaction, positive and negative aspects (focus groups, interviews) | Good engagement with the robot, pleasant to see, satisfactory navigation, gives a feeling of security, interaction with it is spontaneous | No | NA | Concern about size and battery, confidentiality, ability of MTR to avoid obstacles and return to its charging station |
| Cesta et al. (2016) [26] | OAs with health concerns (n = 2, a couple) | NA | Adult child (n = 1) | OAs: loneliness, social support, service satisfaction, depression, emotions, usability, acceptability, psycho-social impact, telepresence dimension, user expectations and attitude towards the robot (scales and questionnaire); family: affects, usability, telepresence dimension, psychosocial impact, expectations and attitude towards the robot (scales and questionnaire) | Good social and functional acceptance by OAs and family; no loss of interest over time; wish to continue the use of the robot beyond 12 months | Yes | MTR appreciated for its ability to create company and alleviate loneliness | Concern about MTR management and maintenance, wish expressed to have more control over the robot |
| Gertowska et al. (2013) [41] | Healthy OAs (n = 10), OAs with MCI (n = 8) | NA | NA | Usability, acceptability, and societal impact (questionnaires) | Satisfactory acceptability and perceived social impact; helps reduce the burden on caregivers; improves the patient’s daily life by facilitating communication; improving safety, mood, and quality of life | No | NA | Necessity of a long-term interaction to evaluate the subjective value of the robot |
| Gonzalez-Jimelez et al. (2013) [42] | OAs (n = 3) | Professional team of a health center (n = NP) | Some relatives (n = NP) | Usability, acceptance, and user experience (interviews and questionnaires) | OAs: good usability and acceptance of the robot; families: feeling of being closer to the OAs; Pro: benefit of being able to follow the health status of patients | No | NA | Concerns about usability, risk of losing “real” contact with OAs; concerns about the size, power consumption, and noise of MTR |
| Granata et al. (2013) [43] | Healthy OAs (n = 11), OAs MCI (n = 11) | NA | NA | Usability (questionnaire and observations) | Better performance for healthy, younger, and IT-experienced OAs | No | NA | NA |
| Hiyama et al. (2017). [44] | Healthy OAs (n = 15) | Lecturers and assistants of a lifelong learning service (n = NP) | NA | Acceptance and usability (questionnaire and observations) | Good acceptance of the robot, easy communication between teachers and OA class during distant class learning | No | NA | NA |
| Koceski and Koceska (2016) [45] | OAs with no severe disability (n = 30) | Professional caregivers (n = 5) | NA | Perceived usefulness and ease of use (questionnaire) | Good acceptability of the basic robot functionalities, willingness to use the robot in the social and medical fields | Yes | The robot helps to reduce loneliness by bridging distances and facilitating communication | Requires training to learn how to manage MTR navigation |
| Kristoffersson et al. (2014) [46] | Healthy OAs (n = 10) | NA | NA | Robot positioning experience with respect to the OAs (Interview and obsevations) | When using MTR, it is important for OAs to have eye-contact with the person embodied, training on the positioning of the robot for pilot users is important | No | NA | NA |
| Moyle et al. (2014) [47] | OAs with dementia (n = 5) | Care workers from a long-term care facility (n= 7) | Family caregivers (n = 6) | Feasibility, emotional state, and engagement while using the robot (semi-structured interviews, observational data) | OAs: Enjoyment and positive emotions when using MTR with a high level of engagement; family and Pro: positive experience, increased contact with family, helps to feel reassured | Yes | Helps to reduce social isolation and increase connection between residents and families, especially for participants who lived some distance away or do not see each other regularly | Technical problems: robot errors, internet connection; ethical issues: confidentiality; need to make a cost analysis. |
| Niemela et al. (2019) [48] | OAs with pathology (n = 1) | Nurses (n = 3) | Adult children (n = 2) | User experience, technology acceptance (pre/post-experimentation interviews, user observations, user journals) | OAs: enjoyment of the family presence; family: satisfaction of seeing the OAs with respect to the only voice calls; Pro: satisfaction when seeing the patient’s enjoyment | Yes | Reduction of social isolation, increased connection between OAs and family | Risk of OA confusion, lack of real physical contact, lack of control over the device, privacy concerns |
| Pineau et al. (2003) [49] | OAs with MCI and other limitations (n = 6) | NA | NA | Feasibility and technology acceptance (observations and post-experimental interviews) | Predominantly positive feedback from OAs, positive conclusion of the robot’s role in assisting nurses | No | NA | Need for technology that adapts to individual differences |
| Schroeter et al. (2013) [50] | OAs with dementia or MCI (n = 6) | NA | Family caregivers (n = 5) | User experience, technology acceptance (post-experimentation interviews, observations, user journals) | Good usability, acceptability, and social impact | No | NA | NA |
| Seelye et al. (2012) [51] | Healthy OAs (n = 8) and MCI OAs (n = 1) | NA | Relatives (n = 8) | Technology acceptance, user experience, usability (interviews) | OAs: positive experience; appreciation of the potential of robots to improve physical health, well-being, social connectedness, and autonomy; family: ease of installation and setup, mobility of the robot appreciated, increased feeling of reassurance | Yes | Good potential to increase OAs’ social connectedness | Operation of the handheld remote confusing for OAs, robot’s wheels not always adapted to handle transitions between different types of flooring; robot not usable by OAs with MCI |
| Stafford et al. (2014) [52] | OAs (n = 25) | NA | NA | Feasibility of robot deployment, feedback on the prototype and services, usability, psychological factors associated with the acceptance of robots (questionnaire) | Feasibility of deploying robots in OAs institutions; OAs having more positive attitudes towards robots, and those that perceived less agency in robot minds were more likely to use them | No | NA | NA |
| Tiberio et al. (2012) [53] | Healthy OAs (n = 9) and MCI OAs (n = 8) | NA | NA | Tolerance towards the robot and effects of the interaction with it (psychophysiological measures, scales, interviews) | Presence of the robot well accepted by healthy and MCI OAs: pleasant experience; good interest, level of attention, and participation | No | NA | Concern about MTR size (too big), real visits preferred to virtual visits |
| Wu et al. (2014) [54] | Healthy OAs (n = 5) and OAs MCI (n = 6) | NA | NA | Technology acceptance (questionnaire, semi-structured interview, focus group) | Robot found easy to use; non-threatening and fun | No | NA | Low intention to use the robot, perceived as not very useful for daily life use, negative image associated with MTR use |
| Zsiga et al. (2017) [55] | OAs with some mobility limitations (n = 8) | NA | NA | Technology acceptance, user behavior and experience (questionnaire, logs collected by the robot) | OAs considered mobility, entertainment, and obstacle detection to be the best robot functionalities. | No | NA | Low reliability of the robot, lack of 24/7 operation time; initial instability of speech recognition, navigation, and self-localization problems |
| HTA Dimension | Benefits of MTR | Barriers to MTR Implementation |
|---|---|---|
| Health problem and current use of the technology | Usable by all the OAs | Lack of recommendations according to health condition |
| Description of the technology | Pleasant design | Complex interfaces, technical problems, fear to fail to use robots |
| Safety | Few side effects (anxiety, confusion) | Limits of current technological capabilities |
| Clinical effectiveness | Satisfying user experience | Insufficient demonstration of real benefit |
| Cost and economic evaluation | Medico-economic evaluation to be developed | |
| Ethical analysis | Potential interest in facilitating contacts | Risk of dehumanization, stigmatization, disappointment |
| Organizational aspects | Potential time saving for families and professionals users | Time required for training and implementation when in use |
| Patients and social aspects | Good user acceptability during the experiments | Different user opinions on long-term use |
| Legal aspects | Legal framework to be developed | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Isabet, B.; Pino, M.; Lewis, M.; Benveniste, S.; Rigaud, A.-S. Social Telepresence Robots: A Narrative Review of Experiments Involving Older Adults before and during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 3597. https://doi.org/10.3390/ijerph18073597
Isabet B, Pino M, Lewis M, Benveniste S, Rigaud A-S. Social Telepresence Robots: A Narrative Review of Experiments Involving Older Adults before and during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2021; 18(7):3597. https://doi.org/10.3390/ijerph18073597
Chicago/Turabian StyleIsabet, Baptiste, Maribel Pino, Manon Lewis, Samuel Benveniste, and Anne-Sophie Rigaud. 2021. "Social Telepresence Robots: A Narrative Review of Experiments Involving Older Adults before and during the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 18, no. 7: 3597. https://doi.org/10.3390/ijerph18073597
APA StyleIsabet, B., Pino, M., Lewis, M., Benveniste, S., & Rigaud, A. -S. (2021). Social Telepresence Robots: A Narrative Review of Experiments Involving Older Adults before and during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health, 18(7), 3597. https://doi.org/10.3390/ijerph18073597