
Multiple Unhealthy Behaviors Share Equivalent Profiles of Readiness for Change in Patients with Type 2 Diabetes

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Stages of Readiness for Change
2.1.1. Refined Sugars and Saturated Fats Consumption
2.1.2. Exercise
2.1.3. Tooth Brushing
2.2. Cognitive Factors
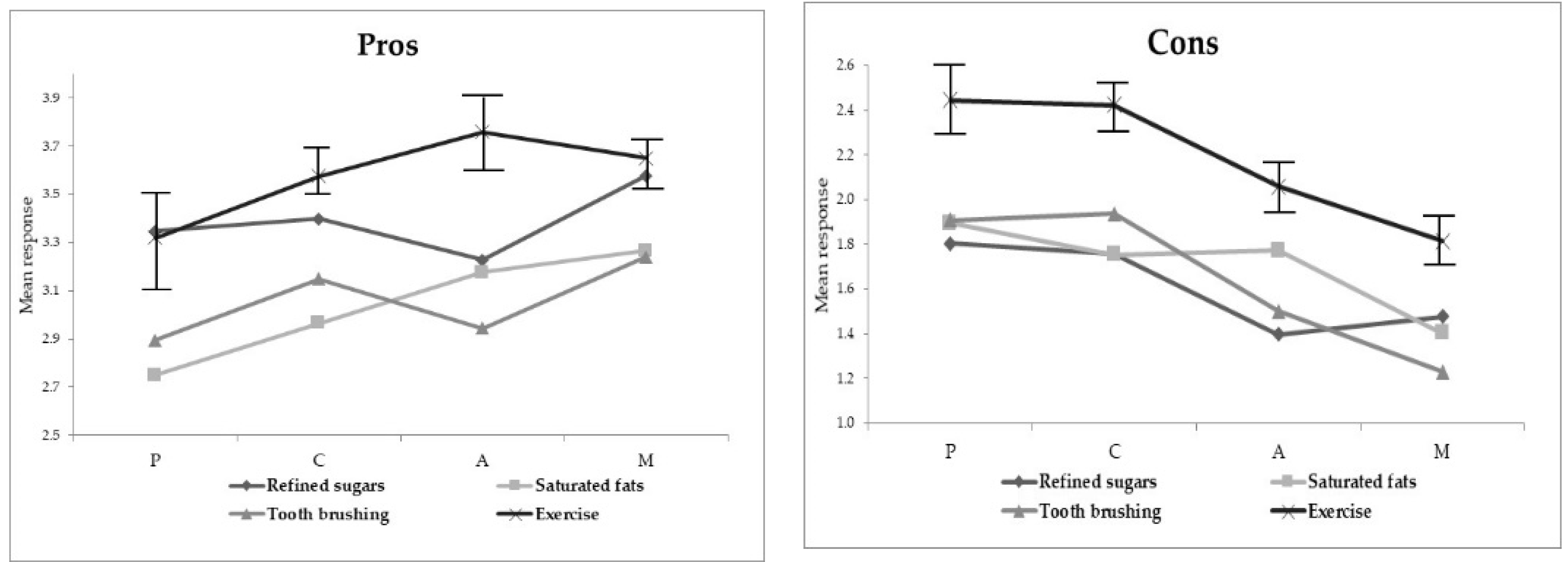
2.2.1. Pros and Cons
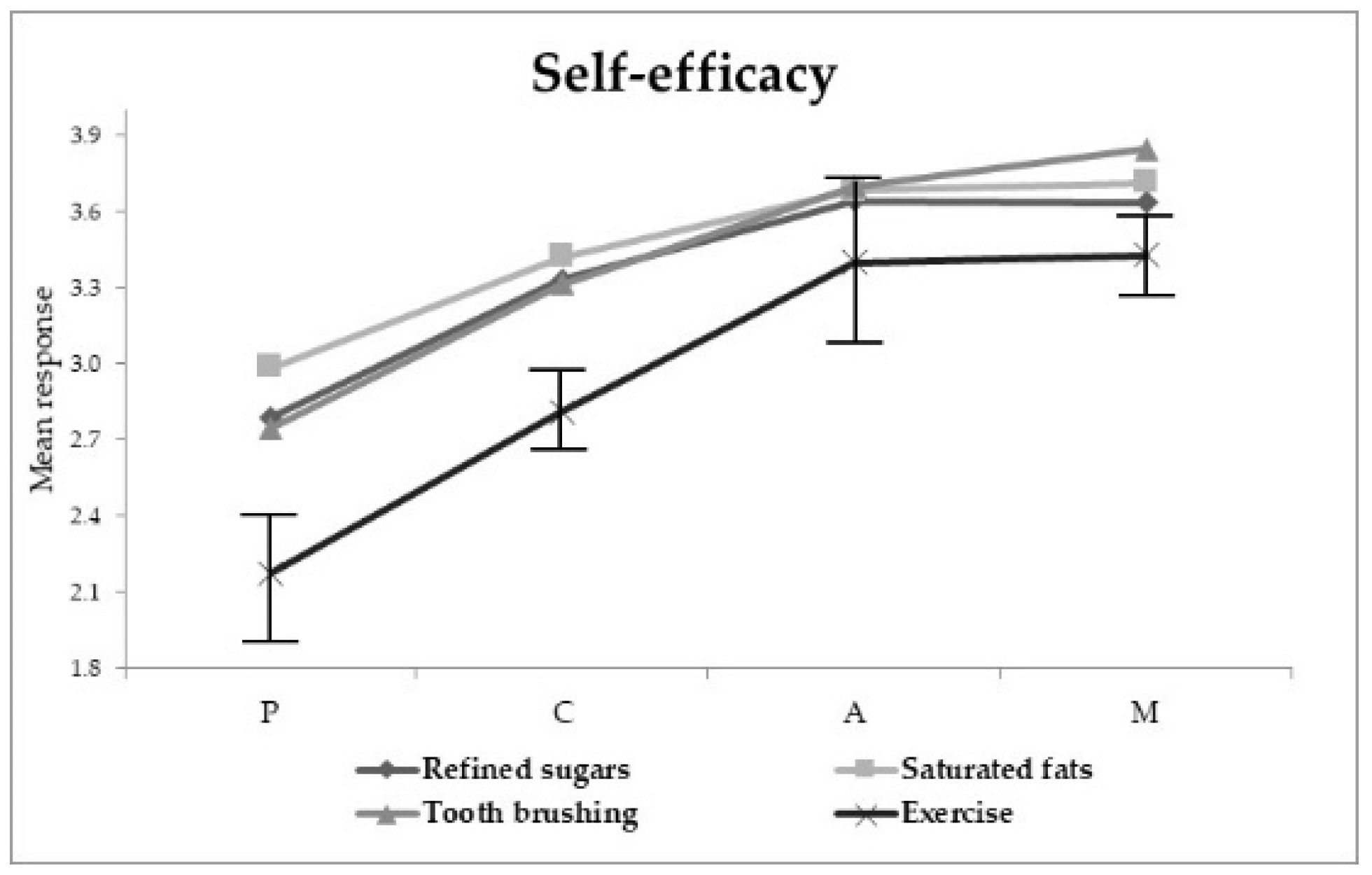
2.2.2. Self-Efficacy
2.2.3. Susceptibility and Severity
2.3. Other Variables
2.4. Statistical Analysis
3. Results
3.1. Distribution and Concurrence of Stages of Readiness for Change
3.2. Cognitive Factors and Stage for Readiness for Change
4. Discussion
Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization Global Report on Diabetes. Available online: https://www.who.int/diabetes/global-report/en/ (accessed on 4 April 2020).
- Instituto Nacional de Salud Pública. Encuesta Nacional de Salud y Nutrición de Medio Camino 2016; Instituto Nacional de Salud Püblica: Cuernavaca, México, 2016. [Google Scholar]
- Shang, J.; Wang, Q.; Zhang, H.; Wang, X.; Wan, J.; Yan, Y.; Gao, Y.; Cheng, J.; Li, Z.; Lin, J. The Relationship Between Diabetes Mellitus and COVID-19 Prognosis: A Retrospective Cohort Study in Wuhan, China. Am. J. Med. 2020, S0002-9343. [Google Scholar] [CrossRef]
- Guo, W.; Li, M.; Dong, Y.; Zhou, H.; Zhang, Z.; Tian, C.; Qin, R.; Wang, H.; Shen, Y.; Du, K.; et al. Diabetes is a risk factor for the progression and prognosis of COVID-19. Diabetes. Metab. Res. Rev. 2020, e3319. [Google Scholar] [CrossRef] [Green Version]
- Prochaska, J.O.; Velicer, W.F. The Transtheoretical Model of Health Behavior Change. Am. J. Health Promot. 1997, 12, 38–48. [Google Scholar] [CrossRef]
- Rosenstock, I.M.; Strecher, V.J.; Becker, M.H. Social Learning Theory and the Health Belief Model. Health Educ. Q. 1988, 15, 175–183. [Google Scholar] [CrossRef]
- American Diabetes Association 5. Lifestyle management: Standards of medical care in diabetesd2019. Diabetes Care 2019, 42, S46–S60. [Google Scholar] [CrossRef] [Green Version]
- Physical Activity Guidelines Advisory Committee. 2018 Physical Activity Guidelines Advisory Committee Scientific Report; US Department of Health and Human Services: Washington, DC, USA, 2018. [Google Scholar]
- Cullinan, M.; Ford, P.; Seymour, G. Periodontal disease and systemic health: Current status. Aust. Dent. J. 2009, 54, S62–S69. [Google Scholar] [CrossRef] [PubMed]
- Vallis, M.; Ruggiero, L.; Greene, G.; Jones, H.; Zinman, B.; Rossi, S.; Edwards, L.; Rossi, J.S.; Prochaska, J.O. Stages of Change for Healthy Eating in Diabetes: Relation to demographic, eating-related, health care utilization, and psychosocial factors. Diabetes Care 2003, 26, 1468–1474. [Google Scholar] [CrossRef] [Green Version]
- Knight, H.; Stetson, B.; Krishnasamy, S.; Mokshagundam, S.P. Diet self-management and readiness to change in underserved adults with type 2 diabetes. Prim. Care Diabetes 2015, 9, 219–225. [Google Scholar] [CrossRef]
- Guicciardi, M.; Lecis, R.; Anziani, C.; Corgiolu, L.; Porru, A.; Pusceddu, M.; Spanu, F. Type 2 diabetes mellitus, physical activity, exercise self-efficacy, and body satisfaction. An application of the transtheoretical model in older adults. Health Psychol. Behav. Med. 2014, 2, 748–758. [Google Scholar] [CrossRef] [Green Version]
- Arafat, Y.; Mohamed Ibrahim, M.I.; Awaisu, A.; Colagiuri, S.; Owusu, Y.; Morisky, D.E.; AlHafiz, M.; Yousif, A. Using the transtheoretical model’s stages of change to predict medication adherence in patients with type 2 diabetes mellitus in a primary health care setting. DARU J. Pharm. Sci. 2019, 27, 91–99. [Google Scholar] [CrossRef]
- Prochaska, J.J.; Nigg, C.R.; Spring, B.; Velicer, W.F.; Prochaska, J.O. The benefits and challenges of multiple health behavior change in research and in practice. Prev. Med. 2010, 50, 26–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parchman, M.L.; Arambula-Solomon, T.G.; Noël, P.H.; Larme, A.C.; Pugh, J.A. Stage of Change Advancement for Diabetes Self-Management Behaviors and Glucose Control. Diabetes Educ. 2003, 29, 128–134. [Google Scholar] [CrossRef]
- Holmen, H.; Wahl, A.; Torbjørnsen, A.; Jenum, A.K.; Småstuen, M.C.; Ribu, L. Stages of change for physical activity and dietary habits in persons with type 2 diabetes included in a mobile health intervention: The Norwegian study in renewing health. BMJ Open Diabetes Res. Care 2016, 4, e000193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bawadi, H.A.; Banks, A.D.; Ammari, F.; Tayyem, R.F.; Jebreen, S. Stage of change of 6 health-related behaviors among patients with type 2 diabetes. Prim. Care Diabetes 2012, 6, 319–327. [Google Scholar] [CrossRef] [PubMed]
- Ndwiga, D.W.; McBride, K.A.; Simmons, D.; MacMillan, F. Diabetes, its risk factors and readiness to change lifestyle behaviours among Australian Samoans living in Sydney: Baseline data for church-wide interventions. Health Promot. J. Aust. 2020, 31, 268–278. [Google Scholar] [CrossRef]
- Mark, A.M. Can diabetes affect my oral health? J. Am. Dent. Assoc. 2018, 149, 328. [Google Scholar] [CrossRef] [Green Version]
- Instituto Nacional de Estadística y Geografía Módulo de Práctica Deportiva y Ejercicio Físico (MOPRADEF). Available online: https://www.inegi.org.mx/programas/mopradef/ (accessed on 28 April 2020).
- Gaona-Pineda, E.B.; Martínez-Tapia, B.; Arango-Angarita, A.; Valenzuela-Bravo, D.; Gómez-Acosta, L.M.; Shamah-Levy, T.; Rodríguez-Ramírez, S. Consumo de grupos de alimentos y factores sociodemográficos en población mexicana. Salud Publica Mex. 2018, 60, 272–282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Munekawa, C.; Hosomi, Y.; Hashimoto, Y.; Okamura, T.; Takahashi, F.; Kawano, R.; Nakajima, H.; Osaka, T.; Okada, H.; Majima, S.; et al. Effect of coronavirus disease 2019 pandemic on the lifestyle and glycemic control in patients with type 2 diabetes: A cross-section and retrospective cohort study. Endocr. J. 2020. [Google Scholar] [CrossRef]
- Grabia, M.; Markiewicz-Żukowska, R.; Puścion-Jakubik, A.; Bielecka, J.; Nowakowski, P.; Gromkowska-Kępka, K.; Mielcarek, K.; Socha, K. The Nutritional and Health Effects of the COVID-19 Pandemic on Patients with Diabetes Mellitus. Nutrients 2020, 12, 3013. [Google Scholar] [CrossRef]
- Emmons, K.M.; Puleo, E.; Greaney, M.L.; Gillman, M.W.; Bennett, G.G.; Haines, J.; Sprunck-Harrild, K.; Viswanath, K. A randomized comparative effectiveness study of Healthy Directions 2—A multiple risk behavior intervention for primary care. Prev. Med. 2014, 64, 96–102. [Google Scholar] [CrossRef] [Green Version]
- Ôunpuu, S.; Woolcott, D.M.; Greene, G.W. Defining stage of change for lower-fat eating. J. Am. Diet. Assoc. 2000, 100, 674–679. [Google Scholar] [CrossRef]
- Plotnikoff, R.C.; Lippke, S.; Johnson, S.T.; Courneya, K.S. Physical Activity and Stages of Change: A Longitudinal Test in Types 1 and 2 Diabetes Samples. Ann. Behav. Med. 2010, 40, 138–149. [Google Scholar] [CrossRef] [PubMed]
- Emani, S.; Thomas, R.; Shah, R.; Mehta, D. Application of transtheoretical model to assess the compliance of chronic periodontitis patients to periodontal therapy. Contemp. Clin. Dent. 2016, 7, 176–181. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.-J.; Kim, B.-T.; Chae, S.-M. Application of the transtheoretical model: Exercise behavior in Korean adults with metabolic syndrome. J. Cardiovasc. Nurs. 2010, 25, 323–331. [Google Scholar] [CrossRef]
- Plotnikoff, R.C.; Brez, S.; Hotz, S.B. Exercise Behavior in a Community Sample with Diabetes: Understanding the Determinants of Exercise Behavioral Change. Diabetes Educ. 2000, 26, 450–459. [Google Scholar] [CrossRef] [PubMed]
- West, G.F.; Cafferty, L.A.; Ledford, C.J.W. Assessing Psychosocial Differences in Stages of Change: An Analysis of Military Healthcare System Patients with Type 2 Diabetes. Mil. Med. 2013, 178, 875–879. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Characteristic | Frequency |
|---|---|
| Sex, female | 65% |
| Highest educational level | |
| None | 3.9% |
| Primary | 35.5% |
| Secondary | 30.3% |
| Preparatory or Technical | 21.2% |
| College or Postgraduate | 9.1% |
| Occupation | |
| Housewife | 49.3% |
| Employee/self-employed | 30.6% |
| Retired | 19.2% |
| Unemployed | 1.0% |
| Marital status, with partner | 76.6% |
| Family background | |
| ≥1 family member has complications of diabetes | 64.8% |
| ≥1 family member tries to avoid foods high in fats or sugars | 71.9% |
| ≥1 family member tries to exercise | 64.8% |
| ≥1 family member visits the dentist annually for revision | 69.5% |
| Stage of Readiness for Change | ||||||
|---|---|---|---|---|---|---|
| P | C | P + C (Early) | A | M | A + M (Late) | |
| Food high in saturated fat | Consumption ≥ once a week | Consumption never or <once a week | ||||
| Interest in reducing frequency, portion size or change to light product | Time with this frequency | |||||
| No | Yes | <6 months | ≥6 months | |||
| Fried or breaded food | 11.9% | 25.4% | 37.3% | 7.7% | 55.1% | 62.8% |
| Whole milk | 10.3% | 23.6% | 33.9% | 4.7% | 61.3% | 66.0% |
| Bacon or menudo (tripe) | 9.9% | 15.1% | 25.0% | 11.4% | 63.7% | 75.1% |
| Whole milk cheese or cream cheese | 9.9% | 17.0% | 26.9% | 10.1% | 63.1% | 73.2% |
| Red meat fat or chicken skin | 5.7% | 12.6% | 18.3% | 10.1% | 71.7% | 81.8% |
| Global, saturated fat | 6.9% | 16.7% | 23.6% | 8.4% | 68.0% | 76.4% |
| Food high in refined sugars | ||||||
| Sugary sodas | 8.6% | 30.0% | 38.6% | 7.9% | 54.0% | 61.9% |
| Pastries | 8.9% | 25.0% | 33.9% | 7.9% | 58.0% | 65.9% |
| Sandwich cookies | 5.2% | 13.0% | 18.2% | 8.9% | 73.0% | 81.9% |
| Coffee or sugary fruit drinks | 4.7% | 14.0% | 18.7% | 3.5% | 78.0% | 81.5% |
| Global refined sugars | 5.7% | 22.4% | 28.1% | 5.4% | 66.5% | 71.9% |
| Tooth brushing | Never or < twice a day | ≥Twice a day | ||||
| Interest in increasing frequency | Time with this frequency | |||||
| No | Yes | <6 months | ≥6 months | |||
| 4.7% | 13.3% | 18.0% | 1.5% | 80.5% | 82.0% | |
| Exercise | Never, moderate <150′ or intense <75′ a week | Moderate ≥150′ or intense ≥ 75′ a week | ||||
| Interest in starting/ increasing the frequency | Time with this frequency | |||||
| No | Yes | <6 months | ≥6 months | |||
| 24.2% | 30.6% | 54.8% | 7.9% | 37.3% | 45.2% | |
| Action or Maintenance | ||||
|---|---|---|---|---|
| Consumption of Refined Sugars | Consumption of Saturated Fats | Exercise | Tooth Brushing | |
| Crude odds ratio (95% confidence interval) | ||||
| Pros | 1.4 (1.1, 1.9) * | 1.7 (1.3, 2.3) *** | 1.6 (1.1, 2.1) *** | n.s. |
| Cons | 0.5 (0.4, 0.7) *** | 0.5 (0.3, 0.7) *** | 0.3 (0.2, 0.4) *** | 0.1 (0.1, 0.2) *** |
| Self-efficacy | 2.3 (1.7, 3.2) *** | 3.1 (2.1, 4.6) *** | 2.4 (1.9, 3.0) *** | 4.5 (3.0, 6.7) *** |
| Adjusted odds ratio (95% confidence interval) | ||||
| Pros | n.s. | 1.4 (1.1, 2.0) *,a,c | n.s. | n.s. |
| Cons | 0.6 (0.4, 0.9) *,a,b | 0.6 (0.4, 0.9) *,a,c | 0.3 (0.2, 0.5) ***,a,d | 0.2 (0.1, 0.3) ***,a,e |
| Self-efficacy | 2.2 (1.6, 3.1) ***,a,b | 2.8 (1.8, 4.4) **,a,c | 2.0 (1.5, 2.5) ***,a,d | 2.4 (1.4, 4.0) **,a,e |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salinas Martínez, A.M.; Gómez Campusano, R.I.; Cordero Franco, H.F.; Chávez Barrón, K.A.; Gutiérrez Sauceda, C.J.; Guzmán de la Garza, F.J.; Núñez Rocha, G.M. Multiple Unhealthy Behaviors Share Equivalent Profiles of Readiness for Change in Patients with Type 2 Diabetes. Int. J. Environ. Res. Public Health 2021, 18, 3631. https://doi.org/10.3390/ijerph18073631
Salinas Martínez AM, Gómez Campusano RI, Cordero Franco HF, Chávez Barrón KA, Gutiérrez Sauceda CJ, Guzmán de la Garza FJ, Núñez Rocha GM. Multiple Unhealthy Behaviors Share Equivalent Profiles of Readiness for Change in Patients with Type 2 Diabetes. International Journal of Environmental Research and Public Health. 2021; 18(7):3631. https://doi.org/10.3390/ijerph18073631
Chicago/Turabian StyleSalinas Martínez, Ana María, Ruth Isabel Gómez Campusano, Hid Felizardo Cordero Franco, Karen Abigail Chávez Barrón, Cecilia Janeth Gutiérrez Sauceda, Francisco Javier Guzmán de la Garza, and Georgina Mayela Núñez Rocha. 2021. "Multiple Unhealthy Behaviors Share Equivalent Profiles of Readiness for Change in Patients with Type 2 Diabetes" International Journal of Environmental Research and Public Health 18, no. 7: 3631. https://doi.org/10.3390/ijerph18073631
APA StyleSalinas Martínez, A. M., Gómez Campusano, R. I., Cordero Franco, H. F., Chávez Barrón, K. A., Gutiérrez Sauceda, C. J., Guzmán de la Garza, F. J., & Núñez Rocha, G. M. (2021). Multiple Unhealthy Behaviors Share Equivalent Profiles of Readiness for Change in Patients with Type 2 Diabetes. International Journal of Environmental Research and Public Health, 18(7), 3631. https://doi.org/10.3390/ijerph18073631