
Water Ski Injuries and Chronic Pain in Collegiate Athletes

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Questionnaire
2.3. Statistical Analyses
3. Results
3.1. Body Region and Type of Injuries in Collegiate Water Ski Athletes
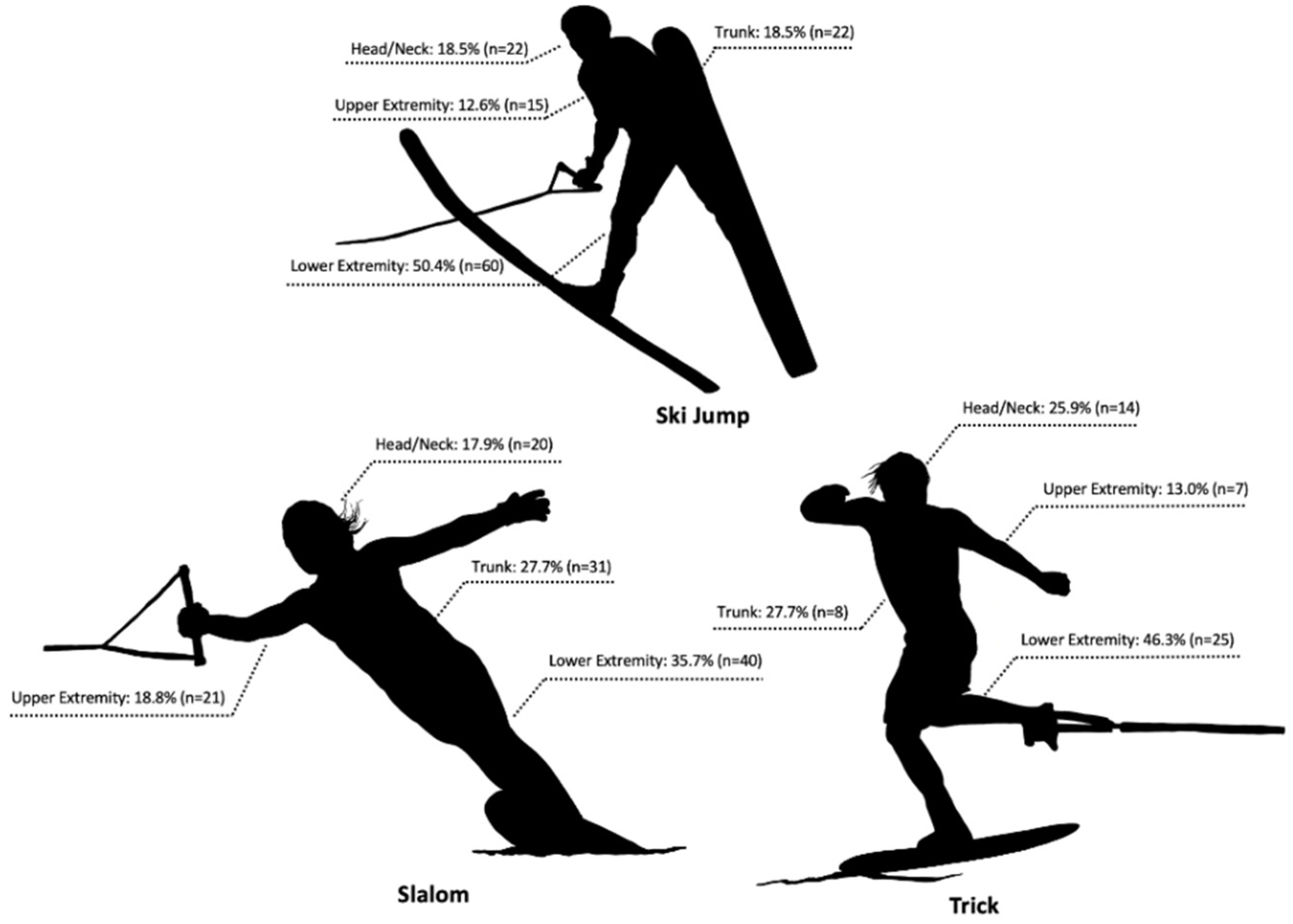
3.2. Distribution of Body Part and Type of Injury Within Disciplines
3.3. Distribution of Type and Location of Injury by the Levels of Water Ski Experiences
3.4. Mechanics and Cause of Injury
3.5. Chronic Pain and Pain Management
4. Discussion
4.1. Body Region and Type of Injuries in Collegiate Water Ski Athletes
4.2. Body Region Injured by Discipline
4.3. Mechanism and Cause of Injury
4.4. Chronic Pain and Pain Management
4.5. Strength and Limitation of the Study
4.6. Practical Application
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Number of Participants in Water Skiing in the United States from 2006 to 2017. Available online: https://www.statista.com/statistics/191986/participants-in-water-skiing-in-the-us-since-2006/ (accessed on 13 February 2020). (In Millions).
- The IWWF Is the World Governing Body for Towed Water Sports Recognized by the International Olympic Committee (IOC). IWWF. Available online: http://iwwfed.com/what-is-the-iwwf/ (accessed on 30 November 2019).
- Mullins, N.M. Slalom water skiing: Physiological Consideration and Specific Conditioning. Strength Cond. J. 2007, 29, 42–54. [Google Scholar] [CrossRef]
- Ota, K.; Tanae, M.; Ishii, K.; Takiyama, K. Optimizing motor decision-making through competition with opponents. Sci. Rep. 2020, 10, 950. [Google Scholar] [CrossRef] [PubMed]
- Leggett, S.H.; Kenney, K.; Eberhardt, T. Applied physiology of water-skiing. Sports Med. 1996, 21, 262–276. [Google Scholar] [CrossRef] [PubMed]
- Loughlin, S. Investigation of injuries occurring within competitive water-skiing in the UK. Int. J. Exer. Sci. 2013, 6, 29–42. [Google Scholar]
- Howe, P.D. Sport, Professionalism and Pain: Ethnographies of Injury and Risk; Routledge: London, UK, 2004. [Google Scholar]
- Bono, C.M. Low-back pain in athletes. J. Bone Jt. Surg. Am. 2004, 86, 382–396. [Google Scholar] [CrossRef]
- Burrus, M.T.; Werner, B.C.; Starman, J.S.; Gwathmey, F.W.; Carson, E.W.; Wilder, R.P.; Diduch, D.R. Chronic leg pain in athletes. Am. J. Sports Med. 2015, 43, 1538–1547. [Google Scholar] [CrossRef]
- Nadler, S.F.; Malanga, G.A.; Bartoli, L.A.; Feinberg, J.H.; Prybicien, M.; Deprince, M. Hip muscle imbalance and low back pain in athletes: Influence of core strengthening. Med. Sci. Sports Exerc. 2002, 34, 9–16. [Google Scholar] [CrossRef] [Green Version]
- Nadler, S.F.; Wu, K.D.; Galski, T.; Feinberg, J.H. Low back pain in college athletes. A prospective study correlating lower extremity overuse or acquired ligamentous laxity with low back pain. Spine 1998, 23, 828–833. [Google Scholar] [CrossRef] [PubMed]
- Perlman, S.E.; Hertweck, S.P.; Wolfe, W.M. Water-ski douche injury in a premenarcheal female. Pediatrics 1995, 96, 782–783. [Google Scholar] [PubMed]
- Blasier, R.B.; Morawa, L.G. Complete rupture of the hamstring origin from a water skiing injury. Am. J. Sports Med. 1990, 18, 435–437. [Google Scholar] [CrossRef] [PubMed]
- Hummel, G.; Gainor, B.J. Waterskiing-related injuries. Am. J. Sports Med. 1982, 10, 215–218. [Google Scholar] [CrossRef]
- Hostetler, S.G.; Hostetler, T.L.; Smith, G.A.; Xiang, H. Characteristics of water skiing-related and wakeboarding-related injuries treated in emergency departments in the United States, 2001–2003. Am. J. Sports Med. 2005, 33, 1065–1070. [Google Scholar] [CrossRef] [PubMed]
- Baker, J.I.; Griffin, R.; Brauneis, P.F.; Rue, L.W.; McGwin, G., Jr. A comparison of wakeboard-, water skiing-, and tubing-related injuries in the United States, 2000–2007. J. Sports Sci. Med. 2010, 9, 92–97. [Google Scholar] [PubMed]
- Furness, J.; Hing, W.; Walsh, J.; Abbott, A.; Sheppard, J.M.; Climstein, M. Acute injuries in recreational and competitive surfers: Incidence, severity, location, type, and mechanism. Am. J. Sports Med. 2015, 43, 1246–1254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jackson, R.A. Musculoskeletal Injuries in California Ocean Lifeguards; California State University-Long Beach: Long Beach, CA, USA, 2017. [Google Scholar]
- Dawson, A.P.; Steele, E.J.; Hodges, P.W.; Stewart, S. Development and test-retest reliability of an extended version of the Nordic Musculoskeletal Questionnaire (NMQ-E): A screening instrument for musculoskeletal pain. J. Pain. 2009, 10, 517–526. [Google Scholar] [CrossRef] [PubMed]
- Taylor, D.M.; Bennett, D.; Carter, M.; Garewal, D.; Finch, C.F. Acute injury and chronic disability resulting from surfboard riding. J. Sci. Med. Sport. 2004, 7, 429–437. [Google Scholar] [CrossRef]
- Zwingenberger, S.; Valladares, R.D.; Walther, A.; Beck, H.; Stiehler, M.; Kirschner, S.; Engelhardt, M.; Kasten, P. An epidemiological investigation of training and injury patterns in triathletes. J. Sports Sci. 2014, 32, 583–590. [Google Scholar] [CrossRef] [PubMed]
- Kotrlik, J.; Williams, H.; Jabor, K. Reporting and Interpreting Effect Size in Quantitative Agricultural Education Research. J. Agric. Edu. 2011, 52, 132–142. [Google Scholar] [CrossRef]
- Sallis, R.E.; Jones, K.; Sunshine, S.; Smith, G.; Simon, L. Comparing sports injuries in men and women. Int. J. Sports Med. 2001, 22, 420–423. [Google Scholar] [CrossRef] [Green Version]
- Weyman, T.G.C.E.; Cole, M.E. Waterskiing injuries. J. Sports Chir. Rehab. 1996, 10, 111–114. [Google Scholar]
- Roberts, S.N.; Roberts, P.M. Tournament water skiing trauma. Br. J. Sports Med. 1996, 30, 90–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grace, N. Water skiing hazards: Nature and prevention. J. Sports Med. 1974, 2, 212–216. [Google Scholar] [CrossRef] [PubMed]
- Banta, J.V. Epidemiology of waterskiing injuries. West J. Med. 1979, 130, 493–497. [Google Scholar] [PubMed]
- Jenkins, P.; Earle-Richardson, G.; Slingerland, D.T.; May, J. Time dependent memory decay. Am. J. Ind. Med. 2002, 41, 98–101. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Athletes’ Physique Information | Total (N = 96) |
|---|---|
| Female participant (%) | 52.1 |
| Age (years) | 21.4 ± 2.23 |
| Body mass (kg) | 69.7 ± 10.72 |
| Height (cm) | 172.6 ± 9.33 |
| Body mass index (kg/m2) | 23.3 ± 2.63 |
| Water Ski Demographics | |
| Career (years) | 11.8 ± 6.29 |
| Training in the off-season (h/wk) | 8.6 ± 5.20 |
| Training in in-season (h/wk) | 6.1 ± 3.94 |
| Muscle/Tendon | Joint/Ligament | Bone | Skin | Nerve | |
|---|---|---|---|---|---|
| Head/Neck 53(30) (15.8%) | 8(4) | 0(0) | 4(3) | 11(5) | 30(18) |
| Shoulder 18(6) (5.4%) | 5(2) | 9(2) | 2(1) | 1(0) | 1(1) |
| Upperback 25(14) (7.4%) | 11(5) | 3(1) | 5(3) | 4(3) | 2(2) |
| Elbow 16(8) (4.8%) | 1(1) | 7(2) | 3(1) | 3(3) | 2(1) |
| Wrist/Hand 30(15) (8.9%) | 6(1) | 5(4) | 11(4) | 7(5) | 1(1) |
| Low back 28(16) (8.3%) | 17(8) | 2(1) | 2(1) | 1(1) | 6(5) |
| Hip/Thigh 21(12) (6.3%) | 11(5) | 8(6) | 1(0) | 0(0) | 1(1) |
| Knees 56(33) (16.7%) | 18(10) | 25(14) | 2(2) | 9(6) | 2(1) |
| Ankle/Feet 89(35) (26.5%) | 35(18) | 18(6) | 19(5) | 16(6) | 1(0) |
| Total 336(169) (100%) | 112(54) (33.3%) | 77(36) (22.9%) | 49(20) (14.6%) | 52(29) (15.5%) | 46(30) * (13.7%) |
| Total | <5 Years (N = 21) | 5–10 Years (N = 17) | 10 Years < (N = 58) | (p-Value) | |
|---|---|---|---|---|---|
| Body Region | |||||
| Head/Neck | 53 (100%) | 4 a (7.5%) | 10 ab (18.9%) | 39 b (73.6%) | 9.20 (0.01) |
| Trunk | 53 (100%) | 7 a (13.2%) | 15 b (23.8%) | 31 ab (58.5%) | 6.12 (0.05) |
| Upper extremity | 64 (100%) | 8 a (12.5%) | 19 b (29.7%) | 37 ab (57.8%) | 6.36 (0.04) |
| Lower extremity | 166 (100%) | 26 (15.7%) | 33 (19.9%) | 107 (64.5%) | 3.65 (.16) |
| Total | 336 | ||||
| Injury Type | |||||
| Muscle/Tendon | 112 (100%) | 26 (23.2%) | 27 (24.1%) | 59 (52.7%) | 0.47 (.79) |
| Joint/Ligament | 77 (100%) | 5 a (6.5%) | 19 b (24.7%) | 53 b (68.8%) | 13.85 (0.001) |
| Bone | 49 (100%) | 3 a (6.1%) | 12 b (24.5%) | 34 b (69.4%) | 9.12 (0.01) |
| Skin | 52 (100%) | 6 (27.3%) | 10 (45.5%) | 36 (50.0%) | 3.52 (0.17) |
| Nerve | 46 (100%) | 5 (23.8%) | 9 (45.0%) | 32 (47.8%) | 3.81 (0.15) |
| Total | 336 |
| Compression | Torsion/Twisting * | Pull | Deceleration | |
|---|---|---|---|---|
| Head/Neck 40(25) (14.8%) | 13(8) | 6(2) | 7(5) | 14(10) |
| Trunk 48(27) (17.7%) | 10(6) | 15(8) | 15(7) | 8(6) |
| Upper Extremity 43(20) (15.9%) | 8(4) | 15(6) | 15(8) | 5(2) |
| Low Extremity 140(71) (51.6%) | 21(11) | 53(27) | 20(12) | 46(21) |
| Total 271(144) (100%) | 52(29) (19.2%) | 89(43) (32.8%) | 57(33) (21.0%) | 73(39) (26.9%) |
| Total | <5 Years (N = 21) | 5–10 Years (N = 17) | 10 Years < (N = 58) | (p-Value) | |
|---|---|---|---|---|---|
| Cause of Injury | |||||
| Insufficient Skill | 24 (100%) | 10 a (41.7) | 3 ab (12.5) | 11 b (45.8) | 7.35 (0.03) |
| Loss of Control | 60 (100%) | 7 a (11.7) | 11 ab (18.3) | 42 b (70.0) | 10.09 (0.01) |
| Weather Condition | 5 (100%) | 0 (0%) | 2 (40.0) | 3 (40.0) | 2.63 (0.27) |
| Low Physical Fitness | 12 (100%) | 2 (16.7) | 3 (25.0) | 7 (58.3) | 0.59 (0.74) |
| Poor Equipment | 13 (100%) | 1 (7.7) | 3 (23.1) | 9 (69.2) | 1.82 (0.40) |
| Others | 16 (100%) | 2 (12.5%) | 2 (12.5%) | 12 (75.0) | 1.74 (0.42) |
| Total | 130 |
| Bone | Muscle | Tendon /Ligament | Others | ||
|---|---|---|---|---|---|
| Body Region | |||||
| Head/Neck | 8 (8.3%) | 2 | 4 | 1 | 1 |
| Trunk | 41 (42.7%) | 6 | 26 | 7 | 2 |
| Upper extremity | 14 (14.6%) | 4 | 4 | 6 | 0 |
| Lower extremity | 33 (34.4%) | 9 | 8 | 14 | 2 |
| Total | 96 (100%) | 21 (21.9%) | 42 (43.8%) | 28 (29.2%) | 5 (5.2%) |
| Pain Management | |||||
| Sauna | 8 (3.4%) | ||||
| Local heat pack | 18 (7.7%) | ||||
| Icing/ice bathing | 32 (13.7%) | ||||
| Massage/Form rolling | 69 (29.6%) | ||||
| Stretching/Exercise | 95 (40.8%) | ||||
| Nutritional Supplement | 11 (4.7%) | ||||
| Total | 233 (100%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jung, H.C.; Straltsova, H.; Woodgate, M.A.; Kim, K.-M.; Lee, J.-M.; Lee, J.-H.; Gann, J.J. Water Ski Injuries and Chronic Pain in Collegiate Athletes. Int. J. Environ. Res. Public Health 2021, 18, 3939. https://doi.org/10.3390/ijerph18083939
Jung HC, Straltsova H, Woodgate MA, Kim K-M, Lee J-M, Lee J-H, Gann JJ. Water Ski Injuries and Chronic Pain in Collegiate Athletes. International Journal of Environmental Research and Public Health. 2021; 18(8):3939. https://doi.org/10.3390/ijerph18083939
Chicago/Turabian StyleJung, Hyun Chul, Hanna Straltsova, Michael A. Woodgate, Kyung-Min Kim, Jung-Min Lee, Joon-Hee Lee, and Joshua J. Gann. 2021. "Water Ski Injuries and Chronic Pain in Collegiate Athletes" International Journal of Environmental Research and Public Health 18, no. 8: 3939. https://doi.org/10.3390/ijerph18083939
APA StyleJung, H. C., Straltsova, H., Woodgate, M. A., Kim, K. -M., Lee, J. -M., Lee, J. -H., & Gann, J. J. (2021). Water Ski Injuries and Chronic Pain in Collegiate Athletes. International Journal of Environmental Research and Public Health, 18(8), 3939. https://doi.org/10.3390/ijerph18083939