
Transient Hyperthyrotropinemia in Outpatient Children with Acute Infections of the Respiratory System

 ,
,  ,
, 

Abstract
:1. Introduction
2. Patients and Methods
- high CRP—according to World Health Organization recommendation-over 10 mg/L [19];
- high white blood cell (WBC) count-above the reference range quoted on the test result, i.e., over 17.500 leukocytes/mm3 for children up to 5 years old, over 15.000 leukocytes/mm3 for children aged 6–12 years, and over 11.000 leukocytes/mm3 for children over 12 years;
- increase in the proportion of lymphocytes (lymphocytosis)-above the reference range quoted on the test result, i.e., over 60% for children up to 5 years old, over 48% for children aged 6–12 years, and over 45% for children over 12 years;
- increase in the proportion of neutrophils (neutrophilia)-above the reference range quoted on the test result, i.e., 51% for children up to 5 years old, over 59% for children aged 6–12 years, and over 55% for children over 12 years.
3. Results
4. Discussions
5. Conclusions
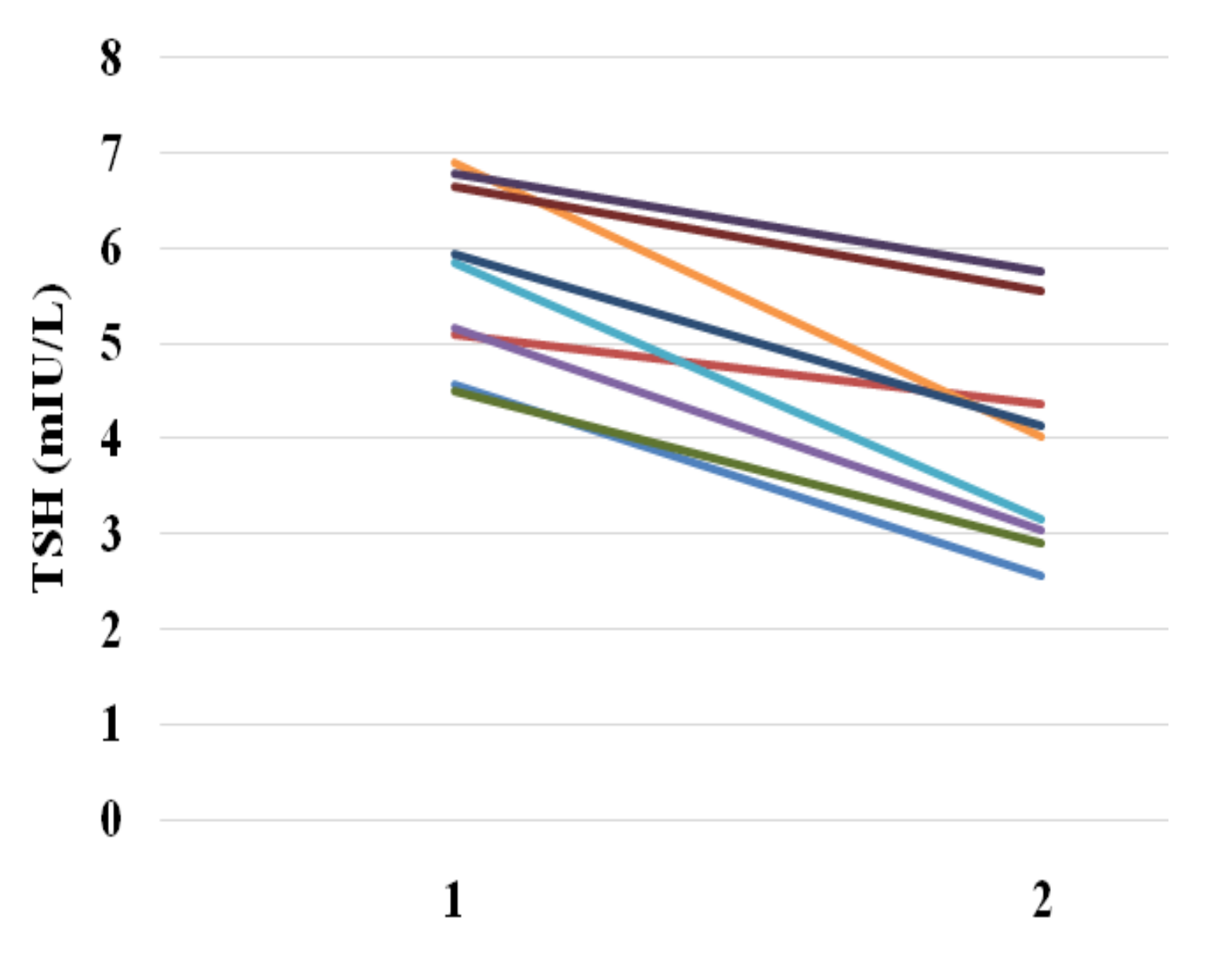
- Transient hyperthyrotropinemia was observed in about 10% of children suffering from an acute respiratory tract infection, regardless of its course, location and severity. The etiology for this finding is unclear.
- If the test is performed during the infection and slightly elevated TSH concentration is noted, the TSH test should be repeated after recovery. Such an approach will allow many patients to avoid expensive diagnostic procedures and unnecessary implementation of treatment.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hanley, P.; Lord, K.; Bauer, A.J. Thyroid disorders in children and adolescents: A review. JAMA Pediatr. 2016, 170, 1008–1019. [Google Scholar] [CrossRef]
- Leung, A.K.C.; Leung, A.A.C. Evaluation and management of the child with hypothyroidism. World J. Pediatr. 2019, 15, 124–134. [Google Scholar] [CrossRef] [PubMed]
- Zygmunt, A.; Adamczewski, Z.; Wojciechowska-Durczynska, K.; Krawczyk-Rusiecka, K.; Bieniek, E.; Stasiak, M.; Zygmunt, A.; Purgat, K.; Zakrzewski, R.; Brzezinski, J.; et al. Evaluation of the effectiveness of iodine prophylaxis in Poland based on over 20 years of observations of iodine supply in school-aged children in the central region of the country. Arch. Med. Sci. 2019, 15, 1468–1474. [Google Scholar] [CrossRef] [PubMed]
- Borowiec, A.; Labochka, D.; Milczarek, M.; Kopiec-Burdecka, M.; Artemniak-Wojtowicz, D.; Pyrżak, B.; Kucharska, A.M. Graves’ disease in children in the two decades following implementation of an iodine prophylaxis programme. Cent. Eur. J. Immunol. 2018, 43, 399–404. [Google Scholar] [CrossRef] [PubMed]
- Gharib, H.; Tuttle, R.M.; Baskin, H.J.; Fish, L.H.; Singer, P.A.; McDermott, M.T.; American Association of Clinical Endocrinologists; American Thyroid Association; Endocrine Society. Consensus Statement #1: Subclinical thyroid dysfunction: A joint statement on management from the American Association of Clinical Endocrinologists, the American Thyroid Association, and The Endocrine Society. Thyroid 2005, 15, 24–28; response 32–33. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, J.; Brown, R.S.; Daumerie, C.; Hubalewska-Dydejczyk, A.; Negro, R.; Vaidya, B. 2014 European thyroid association guidelines for the management of subclinical hypothyroidism in pregnancy and in children. Eur. Thyroid J. 2014, 3, 76–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garber, J.R.; Cobin, R.H.; Gharib, H.; Hennessey, J.V.; Klein, I.; Mechanick, J.I.; Pessah-Pollack, R.; Singer, P.A.; Woeber, K.A.; American Association of Clinical Endocrinologists and American Thyroid Association Taskforce on Hypothyroidism in Adults. Clinical practice guidelines for hypothyroidism in adults: Cosponsored by the American Association of Clinical Endocrinologists and the American Thyroid Association. Endocr. Pract. 2012, 18, 988–1028. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biondi, B.; Cappola, A.R.; Cooper, D.S. Subclinical hypothyroidism: A review. JAMA 2019, 322, 153–160. [Google Scholar] [CrossRef]
- Baloch, Z.; Carayon, P.; Conte-Devolx, B.; Demers, L.M.; Feldt-Rasmussen, U.; Henry, J.F.; LiVosli, V.A.; Niccoli-Sire, P.; John, R.; Ruf, J.; et al. Laboratory medicine practice guidelines. Laboratory support for the diagnosis and monitoring of thyroid disease. Thyroid 2003, 13, 3–126. [Google Scholar] [CrossRef]
- Hoermann, R.; Midgley, J.E.; Larisch, R.; Dietrich, J.W. Homeostatic control of the thyroid-pituitary axis: Perspectives for diagnosis and treatment. Front. Endocrinol. 2015, 6, 177. [Google Scholar] [CrossRef] [Green Version]
- Kapelari, K.; Kirchlechner, C.; Högler, W.; Schweitzer, K.; Virgolini, I.; Moncayo, R. Pediatric reference intervals for thyroid hormone levels from birth to adulthood: A retrospective study. BMC Endocr. Disord. 2008, 8, 15. [Google Scholar] [CrossRef] [Green Version]
- Habib, A.; Molayemat, M.; Habib, A. Elevated serum TSH concentrations are associated with higher BMI Z-scores in southern Iranian children and adolescents. Thyroid Res. 2020, 13, 9. [Google Scholar] [CrossRef]
- Van den Berghe, G.; de Zegher, F.; Bouillon, R. Acute and prolonged critical illness as different neuroendocrine paradigms. J. Clin. Endocrinol. Metab. 1998, 83, 1827–1834. [Google Scholar] [CrossRef]
- Wehmann, R.E.; Gregerman, R.I.; Burns, W.H.; Saral, R.; Santos, G.W. Suppression of thyrotropin in the low-thyroxine state of severe nonthyroidal illness. N. Engl. J. Med. 1985, 312, 546–552. [Google Scholar] [CrossRef]
- Preiser, J.C.; Ichai, C.; Orban, J.C.; Groeneveld, A.B. Metabolic response to the stress of critical illness. Br. J. Anaesth. 2014, 113, 945–954. [Google Scholar] [CrossRef] [Green Version]
- Langouche, L.; Jacobs, A.; Van den Berghe, G. Nonthyroidal illness syndrome across the ages. J. Endocr. Soc. 2019, 3, 2313–2325. [Google Scholar] [CrossRef]
- Jacobs, A.; Derese, I.; Vander Perre, S.; van Puffelen, E.; Verstraete, S.; Pauwels, L.; Verbruggen, S.; Wouters, P.; Langouche, L.; Garcia Guerra, G.; et al. Non-Thyroidal Illness Syndrome in Critically Ill Children: Prognostic Value and Impact of Nutritional Management. Thyroid 2019, 29, 480–492. [Google Scholar] [CrossRef]
- Hamblin, P.S.; Dyer, S.A.; Mohr, V.S.; Le Grand, B.A.; Lim, C.F.; Tuxen, D.V.; Topliss, D.J.; Stockigt, J.R. Relationship between thyrotropin and thyroxine changes during recovery from severe hypothyroxinemia of critical illness. J. Clin. Endocrinol. Metab. 1986, 62, 717–722. [Google Scholar] [CrossRef]
- C-Reactive Protein Concentrations as a Marker of Inflammation or Infection for Interpreting Biomarkers of Micronutrient Status; Vitamin and Mineral Nutrition Information System, WHO/NMH/NHD/EPG/14.7; World Health Organization: Geneva, Switzerland, 2014.
- Raberg, L.; Sim, D.; Read, A.F. Disentangling genetic variation for resistance and tolerance to infectious diseases in animals. Science 2007, 318, 812–814. [Google Scholar] [CrossRef] [Green Version]
- Schneider, D.S.; Ayres, J.S. Two ways to survive infection: What resistance and tolerance can teach us about treating infectious diseases. Nat. Rev. Immunol. 2008, 8, 889–895. [Google Scholar] [CrossRef]
- McEwen, B.S.; Wingfield, J.C. The concept of allostasis in biology and biomedicine. Horm. Behav. 2003, 43, 2–15. [Google Scholar] [CrossRef]
- Chatzitomaris, A.; Hoermann, R.; Midgley, J.E.; Hering, S.; Urban, A.; Dietrich, B.; Abood, A.; Klein, H.H.; Dietrich, J.W. Thyroid allostasis-adaptive responses of thyrotropic feedback control to conditions of strain, stress, and developmental programming. Front. Endocrinol. (Lausanne) 2017, 8, 163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Markanday, A. Acute phase reactants in infections: Evidence-based review and a guide for clinicians. Open Forum Infect. Dis. 2015, 3, 2. [Google Scholar] [CrossRef] [PubMed]
- Sanders, S.; Barnett, A.; Correa-Velez, I.; Coulthard, M.; Doust, J. Systematic review of the diagnostic accuracy of C-reactive protein to detect bacterial infection in nonhospitalized infants and children with fever. J. Pediatr. 2008, 153, 570–574. [Google Scholar] [CrossRef] [PubMed]
- Maturlo, S.J.; Rosenbaum, R.L.; Pan, C.; Surks, M.I. Variable thyrotropin response to thyrotropin-releasing hormone after small decreases in plasma free thyroid hormone concentrations in patients with nonthyroidal diseases. J. Clin. Investig. 1980, 66, 451–456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michalaki, M.; Vagenakis, A.G.; Makri, M.; Kalfarentzos, F.; Kyriazopoulou, V. Dissociation of the early decline in serum T(3) concentration and serum IL-6 rise and TNF alpha in nonthyroidal illness syndrome induced by abdominal surgery. J. Clin. Endocrinol. Metab. 2001, 86, 4198–4205. [Google Scholar] [CrossRef] [PubMed]
- Sawhney, R.C.; Malhotra, A.S.; Nair, C.S.; Bajaj, A.C.; Rajan, K.C.; Pal, K.; Prasad, R.; Basu, M. Thyroid function during a prolonged stay in Antarctica. Eur. J. Appl. Physiol. Occup. Physiol. 1995, 72, 127–133. [Google Scholar] [CrossRef]
- Oka, K.; Hanayama, Y.; Sato, A.; Omura, D.; Yasuda, M.; Hasegawa, K.; Obika, M.; Otsuka, F. Clinical characteristics of febrile outpatients: Possible involvement of thyroid dysfunction in febrile tachycardia. Acta Med. Okayama 2018, 72, 447–456. [Google Scholar] [CrossRef]
- Mustafa, S.; Al-Bader, M.D.; Elgazzar, A.H.; Alshammeri, J.; Gopinath, S.; Essam, H. Effect of hyperthermia on the function of thyroid gland. Eur. J. Appl. Physiol. 2008, 103, 285–288. [Google Scholar] [CrossRef]
- Barington, M.; Brorson, M.M.; Hofman-Bang, J.; Rasmussen, Å.K.; Holst, B.; Feldt-Rasmussen, U. Ghrelin-mediated inhibition of the TSH-stimulated function of differentiated human thyrocytes ex vivo. PLoS ONE 2017, 12, 9. [Google Scholar] [CrossRef] [Green Version]
- Adamczewska, K.; Adamczewski, Z.; Łupińska, A.; Lewiński, A.; Stawerska, R. Strong positive correlation between TSH and ghrelin in euthyroid non-growth hormone-deficient children with short stature. Molecules 2020, 25, 3912. [Google Scholar] [CrossRef]
- Lania, A.; Sandri, M.T.; Cellini, M.; Mirani, M.; Lavezzi, E.; Mazziotti, G. Thyrotoxicosis in patients with COVID-19: The THYRCOV study. Eur. J. Endocrinol. 2020, 183, 381–387. [Google Scholar] [CrossRef]
- Fekete, C.; Gereben, B.; Doleschall, M.; Harney, J.W.; Dora, J.M.; Bianco, A.C.; Sarkar, S.; Liposits, Z.; Rand, W.; Emerson, C.; et al. Lipopolysaccharide induces type 2 iodothyronine deiodinase in the mediobasal hypothalamus: Implications for the nonthyroidal illness syndrome. Endocrinology 2004, 145, 1649–1655. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| ICD-10 | No. | Fever >38 °C | Elevated CRP | Elevated WBC | Neutrophilia | Lymphocytosis | Elevated TSH | |
|---|---|---|---|---|---|---|---|---|
| A88.0 | Enteroviral exanthematous fever (Boston exanthema) | 1 | 1 | 0 | 1 | 0 | 0 | 0 |
| H66.0 | Suppurative otitis media | 2 | 2 | 2 | 1 | 2 | 2 | 2 |
| J00 | Acute nasopharyngitis (cold) | 7 | 1 | 0 | 1 | 1 | 1 | 1 |
| J02 | Streptococcal pharyngitis | 25 | 19 | 10 | 7 | 7 | 7 | 3 |
| J03 | Acute tonsilitis | 2 | 2 | 0 | 0 | 0 | 0 | 0 |
| J04 | Acute laryngitis | 11 | 0 | 3 | 2 | 4 | 4 | 1 |
| J06 | Acute nasopharyngitis | 19 | 5 | 4 | 1 | 5 | 7 | 1 |
| J18 | Pneumonia (unspecified) | 5 | 2 | 3 | 1 | 2 | 1 | 0 |
| J20 | Acute bronchitis | 21 | 9 | 7 | 5 | 6 | 2 | 1 |
| J36 | Peritonsillar abscess | 1 | 1 | 1 | 1 | 1 | 0 | 0 |
| Total | 94 (100%) | 48 (51.1%) | 30 (31.9%) | 20 (23.4%) | 28 (29.8%) | 18 (19.1%) | 9 (9.6%) |
| Initial Visit | Follow-Up Visit | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Gender | Age (years) | Type of Infection | ICD-10 | Fever | CRP mg/L | WBC 109/L | Neu % | Lym % | TSH mIU/L | FT4 ng/dL | Days between Initial and Follow-Up Visits | CRP mg/L | WBC 109/L | Neu % | Lym % | TSH mIU/L | FT4 ng/dL |
| F | 12 | Upper resp. tract | H66 | Yes | 19.81 (↑) | 13.9 (↑) | 74.2 (↑) | 13.9 | 4.57 | 1.33 | 30 | <1 | 7.5 | 42 | 44.1 | 2.56 | 1.27 |
| M | 4 | Upper resp. tract | H66 | Yes | 68.08 (↑) | 10.1 | 52.5 (↑) | 25.7 | 6.9 | 1.25 | 28 | <1 | 8.06 | 37.2 | 49.8 | 4.02 | 1.19 |
| M | 11 | Upper resp. tract | J00 | No | <1 | 6.83 | 42.6 | 42.9 | 5.16 | 0.98 | 35 | <1 | 6.44 | 50.1 | 36 | 3.04 | 1.21 |
| F | 13 | Upper resp. tract | J02 | Yes | 7.03 | 5.34 | 59 (↑) | 29 | 4.51 | 1.34 | 68 | <1 | 4.13 | 49.9 | 39.7 | 2.91 | 1.29 |
| F | 14 | Upper resp. tract | J02 | Yes | 10.51 (↑) | 14.67(↑) | 69.4(↑) | 16.9 | 5.09 | 1.31 | 21 | <1 | 6.85 | 43.9 | 45.0 | 4.36 | 1.23 |
| M | 6 | Upper resp. tract | J02 | No | 3.26 | 11.33 | 32.1 | 55.5 (↑) | 6.78 | 1.27 | 46 | <1 | 5.77 | 56 | 33.8 | 5.77 | 1.33 |
| F | 3 | Upper resp. tract | J04 | No | <1 | 8.5 | 46.7 | 36.4 | 6.64 | 1.12 | 21 | <1 | 7.91 | 29.2 | 58.3 | 5.56 | 1.18 |
| F | 11 | Upper resp. tract | J06 | No | 1.04 | 9.3 | 44.9 | 43.9 | 5.95 | 1.22 | 37 | <1 | 9.43 | 48 | 41.1 | 4.13 | 1.20 |
| M | 4 | Lower resp. tract | J20 | Yes | 33.11 (↑) | 4.21 | 35.9 | 35.9 | 5.85 | 1.44 | 15 | <1 | 8.73 | 51 | 30.8 | 3.15 | 1.37 |
| Normal | Elevated | p = | |
|---|---|---|---|
| body temperature | 2.93 ± 1.27 | 2.85 ± 1.27 | 0.76 |
| CRP | 2.74 ± 1.24 | 3.23 ± 1.27 | 0.08 |
| WBC count | 2.79 ± 1.18 | 3.23 ± 1.48 | 0.15 |
| neutrophils count | 2.83 ± 1.26 | 3.04 ± 1.27 | 0.48 |
| lymphocytes count | 2.90 ± 1.29 | 2.88 ± 1.23 | 0.98 |
| Younger Children n = 76 | Older Children n = 18 | p = | |
|---|---|---|---|
| Girl/boys | 32/44 | 13/5 | |
| Age (years) | 6.79 ±2.75 | 14.5 ±1.53 | <0.000 |
| TSH (mIU/L) | 2.88 ± 1.29 | 2.95 ± 1.16 | NS |
| FT4 (ng/mL) | 1.24 ± 0.08 | 1.24 ± 0.11 | NS |
| Elevated TSH n (%) | 5 (6.6) | 4 (22.2) | 0.06 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adamczewska, K.; Adamczewski, Z.; Stasiak, M.; Lewiński, A.; Stawerska, R. Transient Hyperthyrotropinemia in Outpatient Children with Acute Infections of the Respiratory System. Int. J. Environ. Res. Public Health 2021, 18, 4115. https://doi.org/10.3390/ijerph18084115
Adamczewska K, Adamczewski Z, Stasiak M, Lewiński A, Stawerska R. Transient Hyperthyrotropinemia in Outpatient Children with Acute Infections of the Respiratory System. International Journal of Environmental Research and Public Health. 2021; 18(8):4115. https://doi.org/10.3390/ijerph18084115
Chicago/Turabian StyleAdamczewska, Katarzyna, Zbigniew Adamczewski, Magdalena Stasiak, Andrzej Lewiński, and Renata Stawerska. 2021. "Transient Hyperthyrotropinemia in Outpatient Children with Acute Infections of the Respiratory System" International Journal of Environmental Research and Public Health 18, no. 8: 4115. https://doi.org/10.3390/ijerph18084115
APA StyleAdamczewska, K., Adamczewski, Z., Stasiak, M., Lewiński, A., & Stawerska, R. (2021). Transient Hyperthyrotropinemia in Outpatient Children with Acute Infections of the Respiratory System. International Journal of Environmental Research and Public Health, 18(8), 4115. https://doi.org/10.3390/ijerph18084115