
Assessing Public Willingness to Wear Face Masks during the COVID-19 Pandemic: Fresh Insights from the Theory of Planned Behavior

 ,
,  ,
,  ,
,  ,
,  ,
, 
Abstract
:1. Introduction
2. Methods
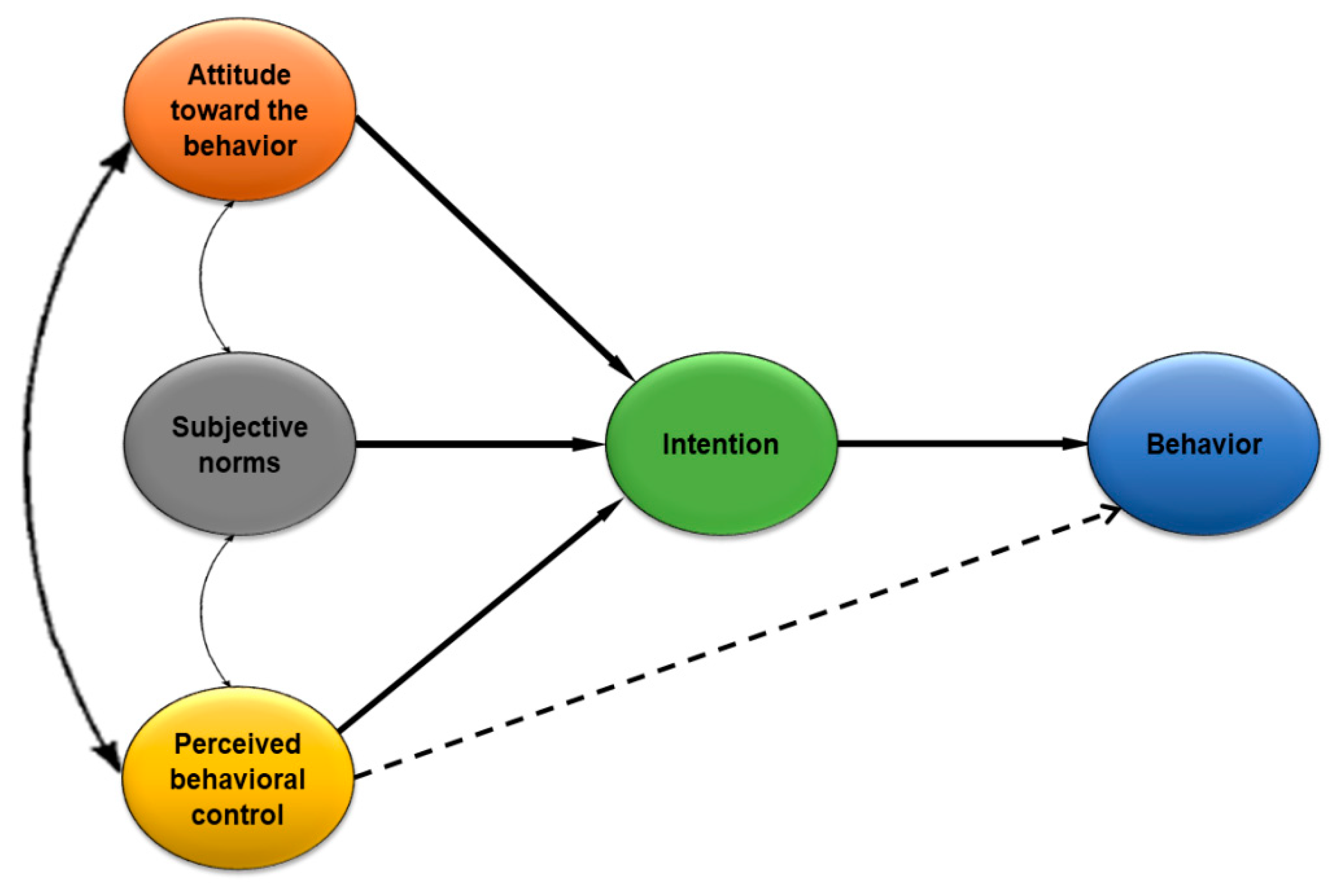
2.1. Theoretical Framework
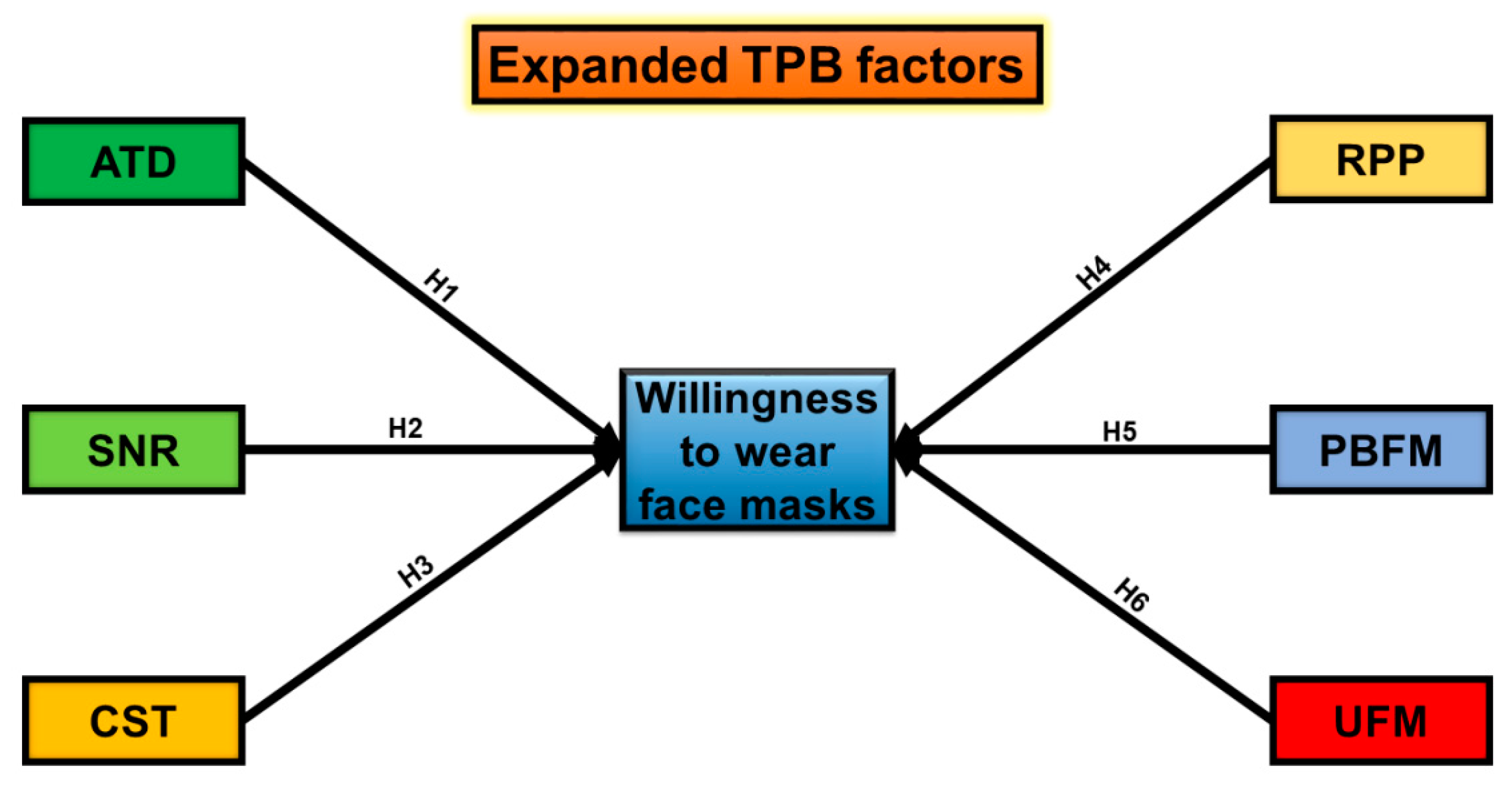
2.2. Formulation of Hypotheses
2.2.1. Attitude
2.2.2. Social Norms
2.2.3. Cost of Face Masks
2.2.4. Risk Perceptions of the Pandemic
2.2.5. Perceived Benefits of Face Masks
2.2.6. Unavailability of Face Masks
3. Research Design
3.1. Survey Site, Sample Size, and Selection of Respondents
3.2. Selection of Variables
3.3. Statistical Analyses
4. Results
4.1. Demographic Features of the Respondents
4.2. Descriptive Statistics and Discriminant Validity Findings
4.3. Testing the Fit of the Model
4.4. Testing of Hypotheses and Structural Equation
4.5. Endogeneity Testing
5. Discussion
5.1. Attitude and WTW Face Masks
5.2. Social Norms and WTW Face Masks
5.3. Cost of Face Masks and WTW Face Masks
5.4. Risk Perceptions of the Pandemic and WTW Face Masks
5.5. Perceived Benefits of Face Masks and WTW Face Masks
5.6. Unavailability of Face Masks and WTW Face Masks
5.7. Demographic Factors and WTW Face Masks
5.8. Summary and Limitations of Research
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Part 1: Demography of Respondents | ||||||
| Gender | ||||||
| Male | Female | |||||
| Age | ||||||
| 18–35 | 36–55 | More than 55 | ||||
| Income (USD) | ||||||
| <100 | 101–200 | 201–300 | 300–400 | >400 | ||
| Education | ||||||
| Uneducated | Primary | High school | College pass | Post-graduation | ||
| Occupation | ||||||
| Government job | Technical worker | Entrepreneur | Other | |||
| Part 2: Influencing Factors of Public WTW Face Masks | ||||||
| Factors | Items | Strongly Disagree | Disagree | Neutral | Agree | Strongly Agree |
| Attitude | ||||||
| ATD1 | I possess a positive attitude towards face masks | |||||
| ATD2 | I possess a positive attitude that wearing a face mask would save me from getting infected | |||||
| ATD3 | I wear a face mask while meeting with people | |||||
| ATD4 | It is wise to wear face mask wear while going out | |||||
| ATD5 | I have a positive attitude that everybody should wear a face mask at public places | |||||
| ATD6 | I believe that wearing face masks during the pandemic is beneficial for society | |||||
| ATD7 | I possess a favourable attitude that wearing face masks has a good influence on society | |||||
| Social norms | ||||||
| SNR1 | People who are dear to me think that I should wear a face mask | |||||
| SNR2 | I will wear a face mask if my family members also wear | |||||
| SNR3 | I will wear a face mask if my relatives also wear | |||||
| SNR4 | I will wear a face mask if my neighbors also wear | |||||
| SNR5 | I will wear a face mask if my friends also wear | |||||
| SNR6 | I will wear a face mask if my colleagues also wear | |||||
| SNR7 | I will wear a face mask if celebrities also wear | |||||
| Cost of face masks | ||||||
| CST1 | PPE is costly to buy | |||||
| CST2 | Price is a big concern for me when buying PPE | |||||
| CST3 | I do not have enough money to buy PPE | |||||
| CST4 | I cannot manage to buy PPE more often | |||||
| CST5 | I think that buying PPE have an extra burden on my expenditures | |||||
| Risk perceptions of the pandemic | ||||||
| RPP1 | COVID-19 is a severe pandemic | |||||
| RPP2 | People without wearing face masks are susceptible to get infection | |||||
| RPP3 | It is risky to go out without wearing a face mask | |||||
| RPP4 | I feel safe after wearing a face mask in the public gatherings | |||||
| RPP5 | One should adopt precautionary measures during the pandemic situations | |||||
| Perceived benefits of face masks | ||||||
| PBFM1 | I believe that wearing face masks is an effective precautionary measure | |||||
| PBFM2 | I believe that wearing face masks will protect my health | |||||
| PBFM3 | I believe that wearing face masks reduces the chances of getting infected | |||||
| PBFM4 | I believe that wearing face masks reduce the chances of inhaling unhealthy air | |||||
| PBFM5 | I believe that wearing a face mask will reduce my exposure to novel SARS-CoV-2 virus | |||||
| PBFM6 | I do not fear going out after wearing a face mask | |||||
| PBFM7 | I believe that society will get protected from viral diseases if people wear face masks | |||||
| Unavailability of face masks | ||||||
| UFM1 | Face masks are unavailable in the market | |||||
| UFM 2 | There is less supply of face masks in the country | |||||
| UFM 3 | I have a difficulty in obtaining face masks | |||||
| UFM 4 | Unavailability of face masks demotivates me to buy face masks | |||||
| Willingness to wear face masks | ||||||
| WTW1 | The pandemic situation encourages me to wear a face mask | |||||
| WTW2 | I am willing to spend extra on face masks | |||||
| WTW3 | Overall, I am willing to wear a face mask | |||||
| WTW4 | I strongly recommend others to wear face masks | |||||
References
- Irfan, M.; Ahmad, M.; Fareed, Z.; Iqbal, N.; Sharif, A.; Wu, H. On the indirect environmental outcomes of COVID-19: Short-term revival with futuristic long-term implications. Int. J. Environ. Health Res. 2021, 15, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Ali, H.; Yilmaz, G.; Fareed, Z.; Shahzad, F.; Ahmad, M. Impact of novel coronavirus (COVID-19) on daily routines and air environment: Evidence from Turkey. Air Qual. Atmos. Health 2020, 14, 1–7. [Google Scholar] [CrossRef]
- Worldometers No Title. Available online: https://www.worldometers.info/coronavirus/countries-where-coronavirus-has-spread/ (accessed on 16 November 2020).
- Elavarasan, R.M.; Pugazhendhi, R.; Shafiullah, G.; Irfan, M.; Anvari-Moghaddam, A. A hover view over effectual approaches on pandemic management for sustainable cities—The endowment of prospective technologies with revitalization strategies. Sustain. Cities Soc. 2021, 68, 102789. [Google Scholar] [CrossRef]
- Shahzad, F.; Shahzad, U.; Fareed, Z.; Iqbal, N.; Hashmi, S.H.; Ahmad, F. Asymmetric nexus between temperature and COVID-19 in the top ten affected provinces of China: A current application of quantile-on-quantile approach. Sci. Total Environ. 2020, 736, 139115. [Google Scholar] [CrossRef]
- Ali, R.; Akram, M.; Haider, M.; Nazir, I.; Manan, A.; Faisal, M. COVID-19 Pandemic and Government Policies to Control its Situation in Pakistan. Acta Sci. Microbiol. 2020, 3, 164–170. [Google Scholar] [CrossRef]
- Shim, E.; Tariq, A.; Choi, W.; Lee, Y.; Chowell, G. Transmission potential and severity of COVID-19 in South Korea. Int. J. Infect. Dis. 2020, 93, 339–344. [Google Scholar] [CrossRef]
- GOP Coronavirus in Pakistan Confirmed Cases (GOP). Available online: http://covid.gov.pk/ (accessed on 14 November 2020).
- Yasir, A.; Hu, X.; Ahmad, M.; Rauf, A.; Shi, J.; Nasir, S.A. Modeling impact of word of mouth and E-Government on online social presence during COVID-19 outbreak: A multi-mediation approach. Int. J. Environ. Res. Public Health 2020, 17, 2954. [Google Scholar] [CrossRef]
- Khan, K.A.; Haq, M.I.; Khan, J.M.; Zahoor, M.; Gohar, U.; Sher, M.H.; Hameed, M.S.; Khaliq, M.A.; Ali, S.; Kamran, A.; et al. Addressing the Impact of Covid-19 Lockdown on Agriculture, Food Security and Livelihoods in Pakistan. Int. J. Agric. Biol. Sci. 2020, 1, 1002. [Google Scholar] [CrossRef]
- Waris, A.; Atta, U.K.; Ali, M.; Asmat, A.; Baset, A. COVID-19 outbreak: Current scenario of Pakistan. NMNI 2020, 35, 100681. [Google Scholar] [CrossRef]
- Yang, Y.; Peng, F.; Wang, R.; Guan, K.; Jiang, T.; Xu, G.; Sun, J.; Chang, C. The Deadly Coronaviruses: The 2003 SARS Pandemic and the 2020 Novel Coronavirus Epidemic in China, The Company’ s Public News and Information. J. Autoimmun. 2020, 109, 102487. [Google Scholar] [CrossRef]
- Zhang, C.-Q.; Chung, P.-K.; Liu, J.-D.; Chan, D.K.C.; Hagger, M.S.; Hamilton, K. Health Beliefs of Wearing Facemasks for Influenza A/H1N1 Prevention: A Qualitative Investigation of Hong Kong Older Adults. Asia Pac. J. Public Health 2019, 31, 246–256. [Google Scholar] [CrossRef] [Green Version]
- Ngonghala, C.N.; Iboi, E.; Eikenberry, S.; Scotch, M.; MacIntyre, C.R.; Bonds, M.H.; Gumel, A.B. Mathematical assessment of the impact of non-pharmaceutical interventions on curtailing the 2019 novel Coronavirus. Math. Biosci. 2020, 325, 108364. [Google Scholar] [CrossRef]
- Zambrano-Monserrate, M.A.; Ruano, M.A.; Sanchez-Alcalde, L. Indirect effects of COVID-19 on the environment. Sci. Total Environ. 2020, 728, 138813. [Google Scholar] [CrossRef]
- Razzaq, A.; Sharif, A.; Aziz, N.; Irfan, M.; Jermsittiparsert, K. Asymmetric link between environmental pollution and COVID-19 in the top ten affected states of US: A novel estimations from quantile-on-quantile approach. Environ. Res. 2020, 191, 110189. [Google Scholar] [CrossRef]
- Shah, S.A.A.; Longsheng, C.; Solangi, Y.A.; Ahmad, M.; Ali, S. Energy trilemma based prioritization of waste-to-energy technologies: Implications for post-COVID-19 green economic recovery in Pakistan. J. Clean. Prod. 2020, 284, 124729. [Google Scholar] [CrossRef]
- Kumaravel, S.K.; Subramani, R.K.; Sivakumar, T.K.; Elavarasan, R.; Manavalanagar, A.; Annam, A.; Subramaniam, U. Investigation on the impacts of COVID-19 quarantine on society and environment: Preventive measures and supportive technologies. 3 Biotech 2020, 10, 393. [Google Scholar] [CrossRef] [PubMed]
- Ajzen, I. From intentions to actions: A theory of planned behavior. In Action Control; Springer: Berlin/Heidelberg, Germany, 1985; pp. 11–39. [Google Scholar]
- Irfan, M.; Elavarasan, R.M.; Hao, Y.; Feng, M.; Sailan, D. An assessment of consumers’ willingness to utilize solar energy in China: End-users’ perspective. J. Clean. Prod. 2021, 292, 126008. [Google Scholar] [CrossRef]
- Gong, X.; Ye, Z.; Liu, K.; Wu, N. The Effects of live platform exterior design on sustainable impulse buying: Exploring the mechanisms of self-effi cacy and psychological ownership. Sustainability 2020, 12, 2406. [Google Scholar] [CrossRef] [Green Version]
- Procter, L.; Angus, D.J.; Blaszczynski, A.; Gainsbury, S.M. Understanding use of consumer protection tools among Internet gambling customers: Utility of the Theory of Planned Behavior and Theory of Reasoned Action. Addict. Behav. 2019, 99. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A. Self-efficacy: Toward aunifying theory of behavioral change. Psychol. Rev. 1977, 84, 191–215. [Google Scholar] [CrossRef]
- Wood, R.; Bandura, A. Social cognitive theory of organizational management. Acad. Manag. Rev. 1989, 14, 361–384. [Google Scholar] [CrossRef]
- Bandura, A. Health promotion from the perspective of social cognitive theory. Psychol. Health 1998, 13, 623–649. [Google Scholar] [CrossRef]
- Martin, F.; Ajzen, I. Belief, Attitude, Intention, and Behavior: An Introduction to Theory and Research; Addison, Wesley: Boston, MA, USA, 1975. [Google Scholar]
- Irfan, M.; Zhao, Z.Y.; Li, H.; Rehman, A. The influence of consumers’ intention factors on willingness to pay for renewable energy: A structural equation modeling approach. Environ. Sci. Pollut. Res. 2020, 27, 21747–21761. [Google Scholar] [CrossRef]
- Ahmad, M.; Iram, K.; Jabeen, G. Perception-based influence factors of intention to adopt COVID-19 epidemic prevention in China. Environ. Res. 2020, 190, 109995. [Google Scholar] [CrossRef] [PubMed]
- Jabeen, G.; Ahmad, M.; Zhang, Q. Perceived critical factors affecting consumers’ intention to purchase renewable generation technologies: Rural-urban heterogeneity. Energy 2021, 218, 119494. [Google Scholar] [CrossRef]
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Ajzen, I. Understanding Attitudes and Predicting Social Behavior; Prentice-Hall: Hoboken, NJ, USA, 1980. [Google Scholar]
- Yan, G.; Peng, Y.; Hao, Y.; Irfan, M.; Wu, H. Household head’s educational level and household education expenditure in China: The mediating effect of social class identification. Int. J. Educ. Dev. 2021, 83, 102400. [Google Scholar] [CrossRef]
- Bang, H.; Ellinger, A.E.; Hadjimarcou, J.; Traichal, P.A. Consumer Concern, Knowledge, Belief, and Attitude toward Renewable Energy: An Application of the Reasoned Action Theory. Psychol. Mark. 2000, 17, 449–468. [Google Scholar] [CrossRef]
- Shakeel, S.R.; Rahman, S. Towards the establishment of renewable energy technologies’ market: An assessment of public acceptance and use in Pakistan. J. Renew. Sustain. Energy 2018, 10, 045907. [Google Scholar] [CrossRef]
- Wüstenhagen, R.; Wolsink, M.; Bürer, M.J. Social acceptance of renewable energy innovation: An introduction to the concept. Energy Policy 2007, 35, 2683–2691. [Google Scholar] [CrossRef] [Green Version]
- Olshavsky, R.W.; Granbois, D.H. “Consumer Decision Making-Fact or Fiction?”. Comment. J. Consum. Res. 1980, 7, 331. [Google Scholar] [CrossRef]
- Jabeen, G.; Yan, Q.; Ahmad, M.; Fatima, N.; Qamar, S. Consumers’ intention-based influence factors of renewable power generation technology utilization: A structural equation modeling approach. J. Clean. Prod. 2019, 237, 117737. [Google Scholar] [CrossRef]
- Walter, D.; Böhmer, M.M.; Reiter, S.; Krause, G.; Wichmann, O. Risk perception and information-seeking behaviour during the 2009/10 influenza a(H1N1)pdm09 pandemic in Germany. Eurosurveillance 2012, 17, 1–8. [Google Scholar] [CrossRef]
- Zhang, J.; Mu, Q. Air pollution and defensive expenditures: Evidence from particulate-filtering facemasks. J. Environ. Econ. Manag. 2018, 92, 517–536. [Google Scholar] [CrossRef]
- Johnson, E.J.; Hariharan, S. Public health awareness: Knowledge, attitude and behaviour of the general public on health risks during the H1N1 influenza pandemic. J. Public Health 2017, 25, 333–337. [Google Scholar] [CrossRef]
- Irfan, M.; Zhao, Z.Y.; Rehman, A.; Ozturk, I.; Li, H. Consumers’ intention-based influence factors of renewable energy adoption in Pakistan: A structural equation modeling approach. Environ. Sci. Pollut. Res. 2020, 28, 432–445. [Google Scholar] [CrossRef]
- Santana, F.N.; Fischer, S.L.; Jaeger, M.O.; Wong-Parodi, G. Responding to simultaneous crises: Communications and social norms of mask behavior during wildfires and COVID-19. Environ. Res. Lett. 2020, 15, 111002. [Google Scholar] [CrossRef]
- Syed, Q.; Sopwith, W.; Regan, M.; Bellis, M.A. Behind the mask. Journey through an epidemic: Some observations of contrasting public health responses to SARS. J. Epidemiol. Community Health 2003, 57, 855–856. [Google Scholar] [CrossRef] [PubMed]
- Taylor, M.; Barr, M.; Agho, K.; Stevens, G.; Jorm, L. Public health measures during an anticipated influenza pandemic: Factors influencing willingness to comply. Risk Manag. Healthc. Policy 2009, 9. [Google Scholar] [CrossRef] [Green Version]
- Burgess, A.; Horii, M. Risk, ritual and health responsibilisation: Japan’s “safety blanket” of surgical face mask-wearing. Sociol. Health Illn. 2012, 34, 1184–1198. [Google Scholar] [CrossRef]
- Al-Marri, W.; Al-Habaibeh, A.; Watkins, M. An investigation into domestic energy consumption behaviour and public awareness of renewable energy in Qatar. Sustain. Cities Soc. 2018, 41, 639–646. [Google Scholar] [CrossRef] [Green Version]
- Weiss, B.D.; Palmer, R. Relationship between health care costs and very low literacy skills in a medically needy and indigent medicaid population. J. Am. Board Fam. Pr. 2004, 17, 44–47. [Google Scholar] [CrossRef]
- Kesselheim, A.S. Rising health care costs and life-cycle management in the pharmaceutical market. Plos Med. 2013, 10, e1001461. [Google Scholar] [CrossRef]
- Irfan, M.; Zhao, Z.Y.; Ahmad, M.; Batool, K.; Jan, A.; Mukeshimana, M.C. Competitive assessment of Indian wind power industry: A five forces model. J. Renew. Sustain. Energy 2019, 11, 063301. [Google Scholar] [CrossRef]
- Irfan, M.; Zhao, Z.Y.; Ahmad, M.; Mukeshimana, M.C. Critical factors influencing wind power industry: A diamond model based study of India. Energy Rep. 2019, 5, 1222–1235. [Google Scholar] [CrossRef]
- MacIntyre, C.R.; Chughtai, A.A. A rapid systematic review of the efficacy of face masks and respirators against coronaviruses and other respiratory transmissible viruses for the community, healthcare workers and sick patients. Int. J. Nurs. Stud. 2020, 108, 103629. [Google Scholar] [CrossRef] [PubMed]
- Barati, M.; Bashirian, S.; Jenabi, E.; Khazaei, S.; Karimi-Shahanjarini, A.; Zareian, S.; Rezapur-Shahkolai, F.; Moeini, B. Factors associated with preventive behaviours of COVID-19 among hospital staff in Iran in 2020: An application of the Protection Motivation Theory. J. Hosp. Infect. 2020, 105, 430–433. [Google Scholar] [CrossRef]
- Maclntyre, C.R.; Cauchemez, S.; Dwyer, D.E.; Seale, H.; Cheung, P.; Browne, G.; Fasher, M.; Wood, J.; Gao, Z.; Booy, R.; et al. Face mask use and control of respiratory virus transmission in households. Emerg. Infect. Dis. 2009, 15, 233–241. [Google Scholar] [CrossRef]
- Hung, Y. A Study of Barriers to the Wearing of Face Masks by Adults in the US to Prevent the Spread of Influenza. Master’s Thesis, Arizona State University, Tucson, AZ, USA, December 2018. [Google Scholar]
- Desai, A.N.; Aronoff, D.M. Masks and Coronavirus Disease 2019 (COVID-19). JAMA 2020, 323, 2103. [Google Scholar] [CrossRef] [PubMed]
- Hansstein, F.V.; Echegaray, F. Exploring motivations behind pollution-mask use in a sample of young adults in urban China. Glob. Health 2018, 14, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Chughtai, A.A.; Khan, W. Use of personal protective equipment to protect against respiratory infections in Pakistan: A systematic review. J. Infect. Public Health 2020, 13, 385–390. [Google Scholar] [CrossRef]
- Carbon, C.-C. The Psychology of Wearing Face Masks in Times of the COVID-19 Pandemic. SSRN Electron. J. 2020, 1–18. [Google Scholar] [CrossRef]
- Tang, C.S.K.; Wong, C.Y. Factors influencing the wearing of facemasks to prevent the severe acute respiratory syndrome among adult Chinese in Hong Kong. Prev. Med. 2004, 39, 1187–1193. [Google Scholar] [CrossRef] [PubMed]
- McDonald, F.; Horwell, C.J.; Wecker, R.; Dominelli, L.; Loh, M.; Kamanyire, R.; Ugarte, C. Facemask use for community protection from air pollution disasters: An ethical overview and framework to guide agency decision making. Int. J. Disaster Risk Reduct. 2020, 43, 101376. [Google Scholar] [CrossRef]
- Reuter, K.E.; Schaefer, M.S. Illegal captive lemurs in Madagascar: Comparing the use of online and in-person data collection methods. Am. J. Primatol. 2017, 79, 22541. [Google Scholar] [CrossRef] [PubMed]
- Shapka, J.D.; Domene, J.F.; Khan, S.; Yang, L.M. Online versus in-person interviews with adolescents: An exploration of data equivalence. Comput. Hum. Behav. 2016, 58, 361–367. [Google Scholar] [CrossRef]
- Woodyatt, C.R.; Finneran, C.A.; Stephenson, R. In-Person versus online focus group discussions: A comparative analysis of data quality. Qual. Health Res. 2016, 26, 741–749. [Google Scholar] [CrossRef] [PubMed]
- Zhou, D.; Shah, T.; Jebran, K.; Ali, S.; Ali, A. Acceptance and willingness to pay for solar home system: Survey evidence from northern area of Pakistan. Energy Rep. 2017, 3, 54–60. [Google Scholar] [CrossRef]
- Etikan, I.; Musa, S.A.; Alkassim, R.S. Comparison of convenience sampling and purposive sampling. Am. J. Appl. Stat. 2016, 5, 1–4. [Google Scholar] [CrossRef] [Green Version]
- Tang, S.F.; Wang, X.; Zhang, Y.; Hou, J.; Ji, L.; Wang, M.L.; Huang, R. Analysis of high alert medication knowledge of medical staff in Tianjin: A convenient sampling survey in China. J. Huazhong Univ. Sci. Technol. Med. Sci. 2015, 35, 176–182. [Google Scholar] [CrossRef]
- Hashiguchi, N.; Sengoku, S.; Kubota, Y.; Kitahara, S.; Lim, Y.; Kodama, K. Age-Dependent influence of intrinsic and extrinsic motivations on construction worker performance. Int. J. Environ. Res. Public Health 2020, 18, 111. [Google Scholar] [CrossRef] [PubMed]
- Hägerhed Engman, L.; Bornehag, C.G.; Sundell, J. How valid are parents’ questionnaire responses regarding building characteristics, mouldy odour, and signs of moisture problems in Swedish homes? Scand. J. Public Health 2007, 35, 125–132. [Google Scholar] [CrossRef]
- Tauni, M.Z.; Fang, H.X.; Rao, Z.R.; Yousaf, S. The influence of investor personality traits on information acquisition and trading behavior: Evidence from Chinese futures exchange. Pers. Individ. Dif. 2015, 87, 248–255. [Google Scholar] [CrossRef]
- Comrey, A.L.; Lee, H.B. A First Course in Factor Analysis, 2nd ed.; Lawrence Erlbaum Associates, Inc.: Hlilsdale, NJ, USA, 1992; ISBN 0805810625. [Google Scholar]
- Mukeshimana, M.C.; Zhao, Z.Y.; Ahmad, M.; Irfan, M. Analysis on barriers to biogas dissemination in Rwanda: AHP approach. Renew. Energy 2020, 163, 1127–1137. [Google Scholar] [CrossRef]
- Jefferson, T.; Del Mar, C.B.; Dooley, L.; Ferroni, E.; Al-Ansary, L.A.; Bawazeer, G.A.; van Driel, M.L.; Nair, S.; Jones, M.A.; Thorning, S.; et al. Physical interventions to interrupt or reduce the spread of respiratory viruses. Cochrane Database Syst. Rev. 2011, 2011. [Google Scholar] [CrossRef] [Green Version]
- Irfan, M.; Hao, Y.; Ikram, M.; Wu, H.; Akram, R.; Rauf, A. Assessment of the public acceptance and utilization of renewable energy in Pakistan. Sustain. Prod. Consum. 2020, 27, 312–324. [Google Scholar] [CrossRef]
- Sardeshmukh, S.R.; Vandenberg, R.J. Integrating moderation and mediation: A structural equation modeling approach. Acad. Manag. 2013, 2013, 443–448. [Google Scholar] [CrossRef]
- Belaïd, F. Untangling the complexity of the direct and indirect determinants of the residential energy consumption in France: Quantitative analysis using a structural equation modeling approach. Energy Policy 2017, 110, 246–256. [Google Scholar] [CrossRef]
- Fornell, C.; Larcker, D.F. Structural equation models with unobuervable variables and measurement error: Algebra and statistics. J. Mark. Res. 1981, 18, 382. [Google Scholar] [CrossRef]
- Wong, K.K.K.-K. Partial Least Squares Structural Equation Modeling (PLS-SEM) Techniques Using SmartPLS. Mark. Bull. 2013, 24, 1–32. [Google Scholar]
- Nunnally, J.C. Psychometric Theory 3E; Tata McGraw-Hill Education: New York, NY, USA, 1994. [Google Scholar]
- Kaiser, H.F. An index of factorial simplicity. Psychometrika 1974, 39, 31–36. [Google Scholar] [CrossRef]
- Cohen, J.E. Statistical Power Analysis for the Behavioral Sciences; Academic Press: Cambridge, MA, USA, 2013; p. 490. [Google Scholar]
- Field, A. Discovering Statistics Using IBM SPSS Statistics; Sage Publication: London, UK, 2013. [Google Scholar]
- Strupeit, L.; Palm, A. Overcoming barriers to renewable energy diffusion: Business models for customer-sited solar photovoltaics in Japan, Germany and the United States. J. Clean. Prod. 2016, 123, 124–136. [Google Scholar] [CrossRef]
- Lucianetti, L.; Chiappetta Jabbour, C.J.; Gunasekaran, A.; Latan, H. Contingency factors and complementary effects of adopting advanced manufacturing tools and managerial practices: Effects on organizational measurement systems and firms’ performance. Int. J. Prod. Econ. 2018, 200, 318–328. [Google Scholar] [CrossRef]
- Huit, G.T.M.; Hair, J.F.; Proksch, D.; Sarstedt, M.; Pinkwart, A.; Ringle, C.M. Addressing endogeneity in international marketing applications of partial least squares structural equation modeling. J. Int. Mark. 2018, 26, 1–21. [Google Scholar] [CrossRef]
- Sim, S.W.; Moey, K.S.P.; Tan, N.C. The use of facemasks to prevent respiratory infection: A literature review in the context of the Health Belief Model. Singap. Med. J. 2014, 55, 160–167. [Google Scholar] [CrossRef] [Green Version]
- Rahim, N.; Iffat, W.; Shakeel, S.; Naeem, M.I.; Qazi, F.; Rizvi, M.; Nasiri, I.; Bashir, L.; Khan, F.M.; Yaseen, H.; et al. Perspectives about pandemic influenza and its prophylactic measures among final year pharmacy students in Karachi, Pakistan. J. Pharm. Bioallied Sci. 2020, 9, 144–151. [Google Scholar] [CrossRef]
- Ahmad, M.; Rehman, A.; Shah, S.A.A.; Solangi, Y.A.; Chandio, A.A.; Jabeen, G. Stylized heterogeneous dynamic links among healthcare expenditures, land urbanization, and CO2 emissions across economic development levels. Sci. Total Environ. 2020, 753, 142228. [Google Scholar] [CrossRef]
- Ahmad, M.; Akram, W.; Ikram, M.; Shah, A.A.; Rehman, A.; Chandio, A.A.; Jabeen, G. Estimating dynamic interactive linkages among urban agglomeration, economic performance, carbon emissions, and health expenditures across developmental disparities. Sustain. Prod. Consum. 2021, 26, 239–255. [Google Scholar] [CrossRef]
- Hamamura, T.; Park, J.H. Regional differences in pathogen prevalence and defensive reactions to the “swine flu” outbreak among East Asians and Westerners. Evol. Psychol. 2010, 8, 506–515. [Google Scholar] [CrossRef] [Green Version]
- Livingston, E.; Desai, A.; Berkwits, M. Sourcing personal protective equipment during the COVID-19 pandemic. JAMA 2020, 323, 1912–1914. [Google Scholar] [CrossRef] [Green Version]
- Wu, J.; Liao, H.; Wang, J.W.; Chen, T. The role of environmental concern in the public acceptance of autonomous electric vehicles: A survey from China. Transp. Res. Part F Traffic Psychol. Behav. 2019, 60, 37–46. [Google Scholar] [CrossRef]
- Elavarasan, R.M.; Pugazhendhi, R. Restructured society and environment: A review on potential technological strategies to control the COVID-19 pandemic. Sci. Total Environ. 2020, 725, 138858. [Google Scholar] [CrossRef]
- Elavarasan, R.M.; Shafiullah, G.M.; Raju, K.; Mudgal, V.; Arif, M.T.; Jamal, T.; Subramanian, S.; Balaguru, V.S.; Reddy, K.S.; Subramaniam, U. COVID-19: Impact analysis and recommendations for power sector operation. Appl. Energy 2020, 279, 115739. [Google Scholar] [CrossRef] [PubMed]
- Bish, A.; Michie, S. Demographic and attitudinal determinants of protective behaviours during a pandemic: A review. Br. J. Health Psychol. 2010, 15, 797–824. [Google Scholar] [CrossRef] [Green Version]
- Condon, B.J.; Sinha, T. Who is that masked person: The use of face masks on Mexico City public transportation during the Influenza A (H1N1) outbreak. Health Policy 2010, 95, 50–56. [Google Scholar] [CrossRef]
- Hashiguchi, N.; Cao, J.; Lim, Y.; Kubota, Y.; Kitahara, S.; Ishida, S.; Kodama, K. The effects of psychological factors on perceptions of productivity in construction sites in Japan by worker age. Int. J. Environ. Res. Public Health 2020, 17, 3517. [Google Scholar] [CrossRef]
- Mwema, F.M.; Nyika, J.M. Challenges in facemasks use and potential solutions: The case study of Kenya. Sci. Afr. 2020, 10, e00563. [Google Scholar] [CrossRef] [PubMed]
- Ji, D.; Fan, L.; Li, X.; Ramakrishna, S. Addressing the worldwide shortages of face masks. BMC Mater. 2020, 2, 1–11. [Google Scholar] [CrossRef]





| Parameters | Value |
|---|---|
| Time frame | August, September, and October (2020) |
| Location of the survey | Lahore, Peshawar, Karachi, Gilgit, and Quetta |
| Size of the sample | 900 |
| Valid responses | 738 |
| Response rate | 82% |
| Features | Options | Frequencies | (%) |
|---|---|---|---|
| Age | 18–35 | 232 | 31.4 |
| 36–55 | 325 | 44 | |
| Above 55 | 181 | 24.5 | |
| Gender | |||
| Male | 387 | 52.4 | |
| Female | 351 | 47.6 | |
| Income (USD) | |||
| <100 | 39 | 5.3 | |
| 101–200 | 218 | 29.5 | |
| 201–300 | 247 | 33.5 | |
| 301–400 | 167 | 22.6 | |
| >400 | 67 | 9.1 | |
| Education | |||
| Uneducated | 32 | 4.3 | |
| Primary | 106 | 14.4 | |
| High school | 192 | 26 | |
| College pass | 270 | 36.6 | |
| Post-graduation | 138 | 18.7 | |
| Occupation | |||
| Government job | 32 | 4.3 | |
| Technical worker | 322 | 43.6 | |
| Entrepreneur | 206 | 27.9 | |
| Other | 178 | 24.1 |
| Factors | UFM | SNR | PBFM | ATD | CST | RPP | WTW |
|---|---|---|---|---|---|---|---|
| UFM | (0.711) | ||||||
| SNR | 0.326 | (0.824) | |||||
| PBFM | 0.267 | 0.491 | (0.822) | ||||
| ATD | 0.354 | 0.375 | 0.523 | (0.753) | |||
| CST | 0.171 | 0.545 | 0.417 | 0.305 | (0.777) | ||
| RPP | 0.341 | 0.256 | 0.181 | 0.329 | 0.224 | (0.836) | |
| WTW | 0.296 | 0.571 | 0.507 | 0.417 | 0.724 | 0.242 | (0.738) |
| Factors | Items | Outer Loadings | AVE | CR | Cronbach-α |
|---|---|---|---|---|---|
| Attitude | 0.567 | 0.901 | 0.903 | ||
| ATD1 | 0.562 | ||||
| ATD2 | 0.834 | ||||
| ATD3 | 0.722 | ||||
| ATD4 | 0.659 | ||||
| ATD5 | 0.898 | ||||
| ATD6 | 0.907 | ||||
| ATD7 | 0.615 | ||||
| Social norms | 0.679 | 0.936 | 0.938 | ||
| SNR1 | 0.774 | ||||
| SNR2 | 0.800 | ||||
| SNR3 | 0.940 | ||||
| SNR4 | 0.969 | ||||
| SNR5 | 0.830 | ||||
| SNR6 | 0.705 | ||||
| SNR7 | 0.651 | ||||
| Cost of face masks | 0.604 | 0.884 | 0.891 | ||
| CST1 | 0.884 | ||||
| CST2 | 0.975 | ||||
| CST3 | 0.688 | ||||
| CST4 | 0.672 | ||||
| CST5 | 0.513 | ||||
| Risk perceptions of the pandemic | 0.699 | 0.921 | 0.918 | ||
| RPP1 | 0.729 | ||||
| RPP 2 | 0.798 | ||||
| RPP 3 | 0.902 | ||||
| RPP 4 | 0.864 | ||||
| RPP 5 | 0.869 | ||||
| Perceived benefits of face masks | 0.675 | 0.936 | 0.937 | ||
| PBFM1 | 0.641 | ||||
| PBFM2 | 0.837 | ||||
| PBFM3 | 0.803 | ||||
| PBFM4 | 0.860 | ||||
| PBFM5 | 0.851 | ||||
| PBFM6 | 0.818 | ||||
| PBFM7 | 0.899 | ||||
| Unavailability of face masks | 0.506 | 0.804 | 0.803 | ||
| UFM1 | 0.729 | ||||
| UFM 2 | 0.747 | ||||
| UFM 3 | 0.681 | ||||
| UFM 4 | 0.674 | ||||
| Willingness to wear face masks | 0.545 | 0.827 | 0.824 | ||
| WTW1 | 0.658 | ||||
| WTW2 | 0.691 | ||||
| WTW3 | 0.662 | ||||
| WTW4 | 0.608 | ||||
| KMO and Bartlett’s Test | ||
|---|---|---|
| Kaiser-Meyer-Olkin Measure of Sampling Adequacy | 0.817 | |
| Bartlett’s Test of Sphericity | Approx. Chi-Square | 9406.783 |
| df | 78 | |
| Sig. | 0.000 | |
| Hypotheses | Structural Paths | b Value | Result | VIF | R2 |
| H1 | ATD ➝ WTW | 0.09 ** | Accepted | 1.631 | 0.74 |
| H2 | SNR ➝ WTW | 0.11 ** | Accepted | 1.811 | |
| H3 | CST ➝ WTW | −0.00 *** | Accepted | 1.281 | |
| H4 | RPP ➝ WTW | 0.65 ** | Accepted | 1.375 | |
| H5 | PBFM ➝ WTW | 0.09 * | Accepted | 1.875 | |
| H6 | UFM ➝ WTW | −0.10 ** | Accepted | 1.785 |
| Term | Value | Recommended Value | Description |
|---|---|---|---|
| CFI | 0.973 | >0.9 good fit | Comparative fit index |
| NFI | 0.966 | >0.9 good fit | Normed fit index |
| IFI | 0.990 | >0.9 good fit | Incremental fit index |
| TLI | 0.978 | >0.9 good fit | Tucker-Lewis index |
| GFI | 0.994 | >0.9 good fit | Goodness of fit index |
| RMSEA | 0.032 | <0.08 good fit | Root mean squared error of approximation |
| X2/df | 1.381 | <3 good fit | Chi-square |
| SRMR | 0.034 | <0.09 good fit | Standardized root mean squared residual |
| Hypotheses | Structural Paths | b Value | t-Value | Description |
|---|---|---|---|---|
| H1 | ATD ➝ WTW | 0.07 ** | 3.036 | Not different |
| H2 | SNR ➝ WTW | 0.13 ** | 0.285 | Not different |
| H3 | CST ➝ WTW | −0.04 *** | −3.445 | Not different |
| H4 | RPP ➝ WTW | 0.08 ** | 4.272 | Not different |
| H5 | PBFM ➝ WTW | 0.05 * | 5.844 | Not different |
| H6 | UFM ➝ WTW | −0.03 ** | −2.758 | Not different |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Irfan, M.; Akhtar, N.; Ahmad, M.; Shahzad, F.; Elavarasan, R.M.; Wu, H.; Yang, C. Assessing Public Willingness to Wear Face Masks during the COVID-19 Pandemic: Fresh Insights from the Theory of Planned Behavior. Int. J. Environ. Res. Public Health 2021, 18, 4577. https://doi.org/10.3390/ijerph18094577
Irfan M, Akhtar N, Ahmad M, Shahzad F, Elavarasan RM, Wu H, Yang C. Assessing Public Willingness to Wear Face Masks during the COVID-19 Pandemic: Fresh Insights from the Theory of Planned Behavior. International Journal of Environmental Research and Public Health. 2021; 18(9):4577. https://doi.org/10.3390/ijerph18094577
Chicago/Turabian StyleIrfan, Muhammad, Nadeem Akhtar, Munir Ahmad, Farrukh Shahzad, Rajvikram Madurai Elavarasan, Haitao Wu, and Chuxiao Yang. 2021. "Assessing Public Willingness to Wear Face Masks during the COVID-19 Pandemic: Fresh Insights from the Theory of Planned Behavior" International Journal of Environmental Research and Public Health 18, no. 9: 4577. https://doi.org/10.3390/ijerph18094577
APA StyleIrfan, M., Akhtar, N., Ahmad, M., Shahzad, F., Elavarasan, R. M., Wu, H., & Yang, C. (2021). Assessing Public Willingness to Wear Face Masks during the COVID-19 Pandemic: Fresh Insights from the Theory of Planned Behavior. International Journal of Environmental Research and Public Health, 18(9), 4577. https://doi.org/10.3390/ijerph18094577