
Effect of Short-Term Exposure to Fine Particulate Matter and Temperature on Acute Myocardial Infarction in Korea


Abstract
:1. Introduction
2. Methods
2.1. Data Source
2.2. Ethic Approval
2.3. AMI Events and Exposure Definition
2.4. Statistical Analysis
3. Results
3.1. Summary Statistics of Air Pollutant and Weather Conditions
3.2. AMI Incidence
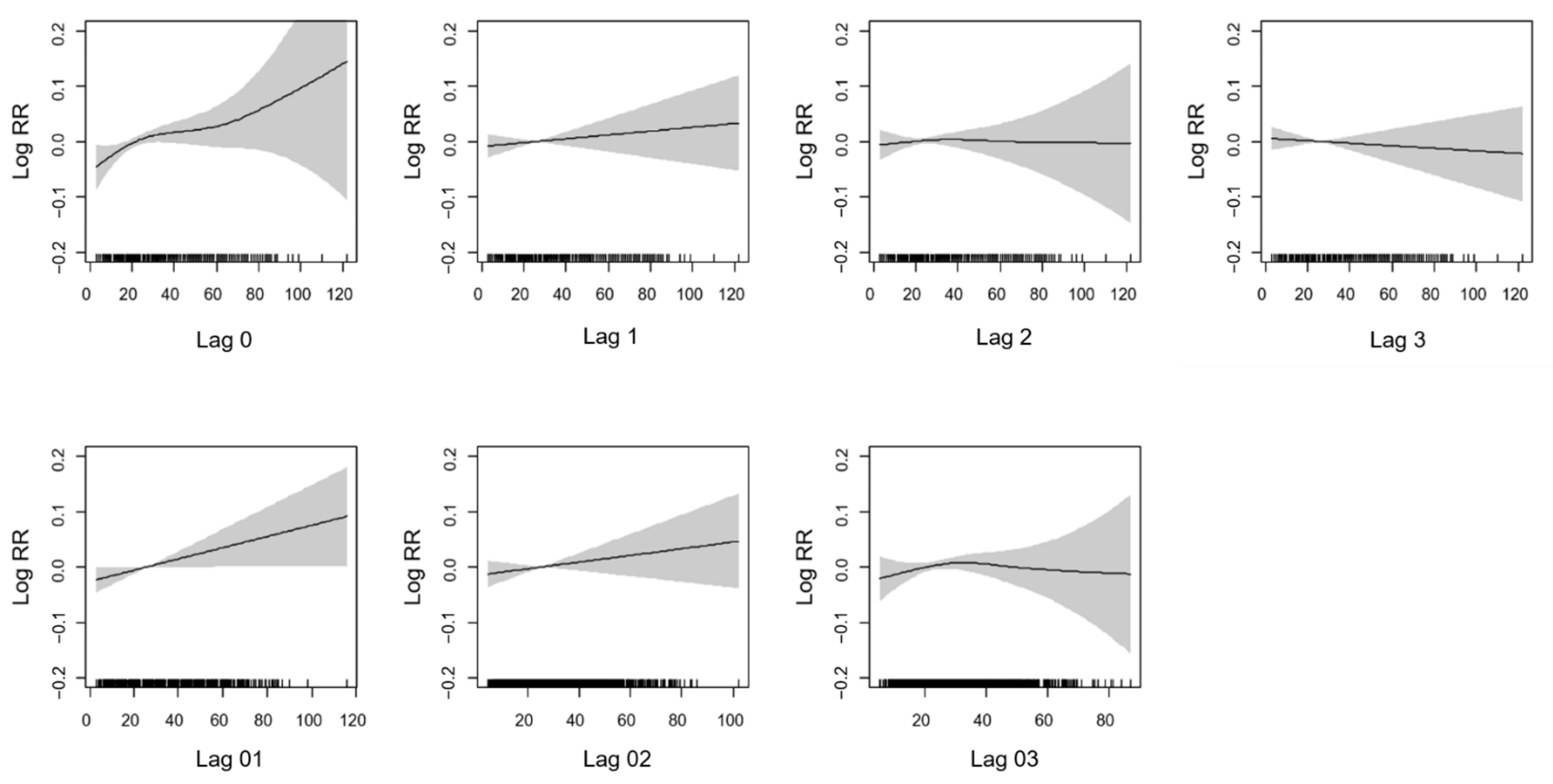
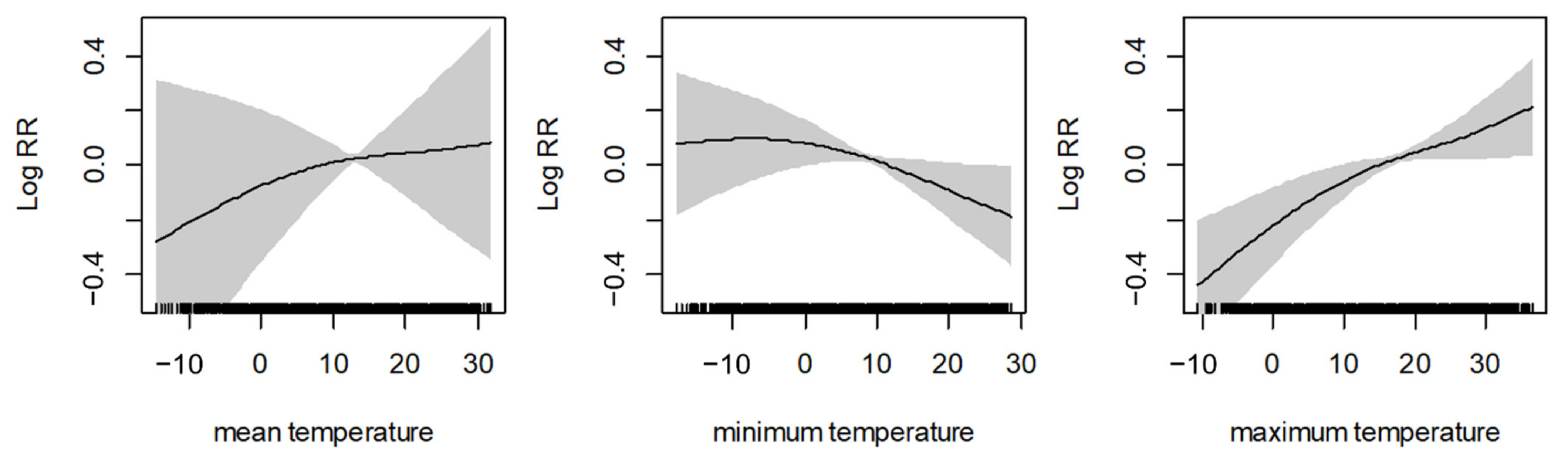
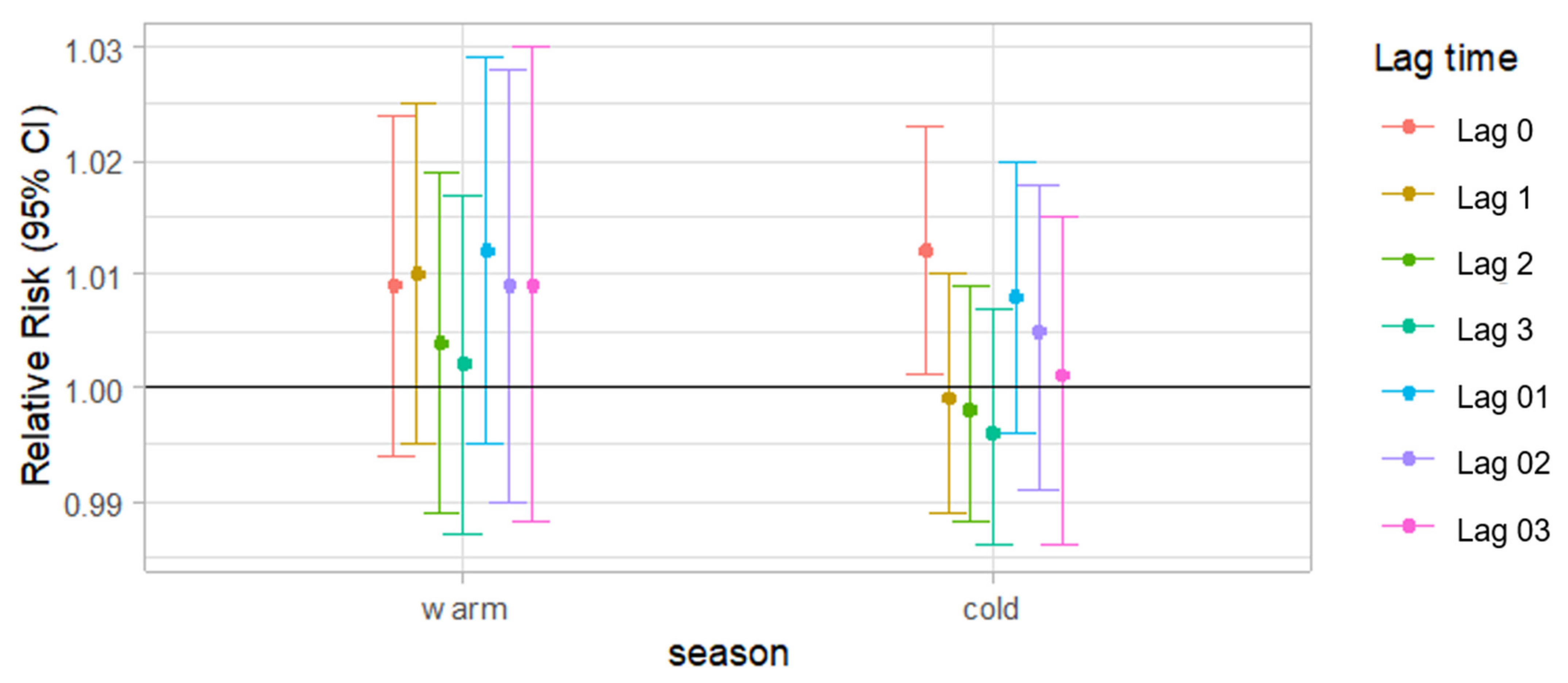
3.3. Relative Risk Estimates for Cases of AMI Events
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lloyd-Jones, D.; Adams, R.J.; Brown, T.M.; Carnethon, M.; Dai, S.; De Simone, G.; Ferguson, T.B.; Ford, E.; Furie, K.; Gillespie, C.; et al. Executive summary: Heart disease and stroke statistics—2015 update: A report from the American Heart Association. Circulation 2015, 131, 434–441. [Google Scholar]
- IIshihara, M.; Fujino, M.; Ogawa, H.; Yasuda, S.; Noguchi, T.; Nakao, K.; Ozaki, Y.; Kimura, K.; Suwa, S.; Fujimoto, K.; et al. Clinical Presentation, Management and Outcome of Japanese Patients with Acute Myocardial Infarction in the Troponin Era–Japanese Registry of Acute Myocardial Infarction Diagnosed by Universal Definition (J-MINUET). Circ. J. 2015, 79, 1255–1262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.H.; Chae, S.-C.; Oh, D.J.; Kim, H.-S.; Kim, Y.J.; Ahn, Y.; Cho, M.C.; Kim, C.J.; Yoon, J.-H.; Park, H.-Y.; et al. Multicenter Cohort Study of Acute Myocardial Infarction in Korea—Interim Analysis of the Korea Acute Myocardial Infarction Registry-National Institutes of Health Registry. Circ. J. 2016, 80, 1427–1436. [Google Scholar] [CrossRef] [Green Version]
- Hong, J.S.; Kang, H.C.; Lee, S.H.; Kim, J. Long-term trend in the incidence of acute myocardial infarction in Korea: 1997-Korean. Circ. J. 2009, 39, 467–476. [Google Scholar]
- Pope, C.A., III; Burnett, R.T.; Thurston, G.D.; Thun, M.J.; Calle, E.E.; Krewski, D.; Godleski, J.J. Cardiovascular mortality and long-term exposure to particulate air pollution: Epidemiological evidence of general pathophysiological pathways of disease. Circulation 2004, 109, 71–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, H.; Atkinson, R.; Bremner, S.; Marston, L. Particulate air pollution and hospital admissions for cardiorespiratory diseases: Are the elderly at greater risk? Eur. Respir. J. 2003, 21, 39–46. [Google Scholar] [CrossRef] [Green Version]
- Ahn, J. Fine Particulate Matter: A Threat to the Heart Rhythm. Korean Circ. J. 2021, 51, 171–173. [Google Scholar] [CrossRef] [PubMed]
- Pope, C.A., III; Dockery, D.W. Health effects of fine particulate air pollution: Lines that connect. J. Air Waste Manag. Assoc. 2006, 56, 709–742. [Google Scholar] [CrossRef] [PubMed]
- Peng, R.D.; Chang, H.H.; Bell, M.L.; McDermott, A.; Zeger, S.L.; Samet, J.M.; Dominici, F. Coarse particulate matter air pollution and hospital admissions for cardiovascular and respiratory diseases among Medicare patients. JAMA 2008, 299, 2172–2179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, H.; Lim, S.; Lee, S.; Mun, D.; Kang, J.; Kim, H.; Park, H.; Kim, C.; Park, S.; Lim, Y.-M.; et al. High Level of Real Urban Air Pollution Promotes Cardiac Arrhythmia in Healthy Mice. Korean Circ. J. 2021, 51, 157–170. [Google Scholar] [CrossRef] [PubMed]
- Miller, M.R.; Shaw, C.A.; Langrish, J.P. From particles to patients: Oxidative stress and the cardiovascular effects of air pollution. Futur. Cardiol. 2012, 8, 577–602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, H.; Tian, Y.; Xiang, X.; Sun, K.; Juan, J.; Song, J.; Cao, Y.; Xu, B.; Hu, Y. Air Pollution and Hospitalization for Acute Myocardial Infarction in China. Am. J. Cardiol. 2017, 120, 753–758. [Google Scholar] [CrossRef] [PubMed]
- Rivero, A.; Bolufé, J.; Ortiz, P.L.; Rodríguez, Y.; Reyes, M.C. Influence of climate variability on acute myocardial infarction mortality in Havana, 2001–2012. MEDICC Rev. 2015, 17, 14–19. [Google Scholar] [PubMed]
- Wichmann, J.; Rosengren, A.; Sjöberg, K.; Barregard, L.; Sallsten, G. Association between Ambient Temperature and Acute Myocardial Infarction Hospitalisations in Gothenburg, Sweden: 1985–2010. PLoS ONE 2013, 8, e62059. [Google Scholar] [CrossRef] [Green Version]
- Madrigano, J.; Mittleman, M.; Baccarelli, A.; Goldberg, R.; Melly, S.; Von Klot, S.; Schwartz, J. Temperature, Myocardial Infarction, and Mortality: Effect Modification by Individual and Area-Level Characteristics. ISEE Conf. Abstr. 2011, 2011. [Google Scholar] [CrossRef]
- Wichmann, J.; Ketzel, M.; Ellermann, T.; Loft, S. Apparent temperature and acute myocardial infarction hospital admissions in Copenhagen, Denmark: A case-crossover study. Environ. Health 2012, 11, 19. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.; Lee, E.; Park, M.S.; Kwon, B.Y.; Kim, H.; Jung, D.H.; Jo, K.H.; Jeong, M.H.; Rha, S.-W. Short-Term Effect of Temperature on Daily Emergency Visits for Acute Myocardial Infarction with Threshold Temperatures. PLoS ONE 2014, 9, e94070. [Google Scholar] [CrossRef]
- Bhaskaran, K.; Hajat, S.; Haines, A.; Herrett, E.; Wilkinson, P.; Smeeth, L. Short term effects of temperature on risk of myocardial infarction in England and Wales: Time series regression analysis of the Myocardial Ischaemia National Audit Project (MINAP) registry. BMJ 2010, 341, c3823. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Z.; Zhang, X.; Gong, D.; Kim, S.-J.; Mao, R.; Zhao, X. Possible influence of atmospheric circulations on winter haze pollution in the Beijing–Tianjin–Hebei region, northern China. Atmos. Chem. Phys. Discuss. 2016, 16, 561–571. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.K.; Sun, Y.; Liu, Z.R.; Ji, D.S.; Hu, B.; Liu, Q.; Wang, Y.S. Characterization of submicron aerosols during a month of serious pollution in Beijing, 2013. Atmos. Chem. Phys. Discuss. 2014, 14, 2887–2903. [Google Scholar] [CrossRef] [Green Version]
- Lee, D.; Lee, Y.-M.; Jang, K.-W.; Yoo, C.; Kang, K.-H.; Lee, J.-H.; Jung, S.-W.; Park, J.-M.; Lee, S.-B.; Han, J.-S.; et al. Korean National Emissions Inventory System and 2007 Air Pollutant Emissions. Asian J. Atmos. Environ. 2011, 5, 278–291. [Google Scholar] [CrossRef] [Green Version]
- Cheol Seong, S.; Kim, Y.Y.; Khang, Y.H.; Heon Park, J.; Kang, H.J.; Lee, H.; Do, C.H.; Song, J.S.; Hyon Bang, J.; Ha, S.; et al. Data resource profile: The national health information database of the National Health Insurance Service in South Korea. Int. J. Epidemiol. 2016, 46, 799–800. [Google Scholar] [CrossRef] [Green Version]
- Song, S.O.; Jung, C.H.; Song, Y.D.; Park, C.-Y.; Kwon, H.-S.; Cha, B.S.; Park, J.-Y.; Lee, K.-U.; Ko, K.S.; Lee, B.-W. Background and Data Configuration Process of a Nationwide Population-Based Study Using the Korean National Health Insurance System. Diabetes Metab. J. 2014, 38, 395–403. [Google Scholar] [CrossRef] [PubMed]
- Lee, M. An analysis on the concentration characteristics of PM2.5 in Seoul, Korea from 2005 to 2012. Asia Pac. J. Atmos. Sci. 2014, 50, 585–594. [Google Scholar] [CrossRef]
- Air Korea. 2018. Available online: http://www.airkorea.or.kr/index (accessed on 28 April 2021).
- Bhaskaran, K.; Gasparrini, A.; Hajat, S.; Smeeth, L.; Armstrong, B. Time series regression studies in environmental epidemiology. Int. J. Epidemiol. 2013, 42, 1187–1195. [Google Scholar] [CrossRef] [PubMed]
- Bell, M.L.; Samet, J.M.; Dominici, F. Time-Series Studies of Particulate Matter. Annu. Rev. Public Health 2004, 25, 247–280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, J.; Liu, Y.; Cui, L.-L.; Liu, S.-Q.; Yin, X.-X.; Li, H.-C. Ambient air pollution, smog episodes and mortality in Jinan, China. Sci. Rep. 2017, 7, 11209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vicedo-Cabrera, A.M.; Olsson, D.; Forsberg, B. Exposure to Seasonal Temperatures during the Last Month of Gestation and the Risk of Preterm Birth in Stockholm. Int. J. Environ. Res. Public Health 2015, 12, 3962–3978. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xie, W.; Li, G.; Zhao, D.; Xie, X.; Wei, Z.; Wang, W.; Wang, M.; Li, G.; Liu, W.; Sun, J.; et al. Relationship between fine particulate air pollution and ischaemic heart disease morbidity and mortality. Heart 2015, 101, 257–263. [Google Scholar] [CrossRef] [PubMed]
- Collart, P.; Dramaix, M.; Levêque, A.; Coppieters, Y. Short-term effects of air pollution on hospitalization for acute myocardial infarction: Age effect on lag pattern. Int. J. Environ. Health Res. 2016, 27, 68–81. [Google Scholar] [CrossRef]
- Hashizume, M.; Kim, Y.; Ng, C.F.S.; Chung, Y.; Madaniyazi, L.; Bell, M.L.; Guo, Y.L.; Kan, H.; Honda, Y.; Yi, S.-M.; et al. Health Effects of Asian Dust: A Systematic Review and Meta-Analysis. Environ. Health Perspect. 2020, 128, 066001. [Google Scholar] [CrossRef]
- Kyobutungi, C.; Grau, A.; Stieglbauer, G.; Becher, H. Absolute Temperature, Temperature Changes and Stroke Risk: A Case-Crossover Study. Eur. J. Epidemiol. 2005, 20, 693–698. [Google Scholar] [CrossRef] [PubMed]
- Neild, P.J.; Syndercombe-Court, D.; Keatinge, W.R.; Donaldson, G.C.; Mattock, M.; Caunce, M. Cold-induced Increases in Erythrocyte Count, Plasma Cholesterol and Plasma Fibrinogen of Elderly People without a Comparable Rise in Protein C or Factor X. Clin. Sci. 1994, 86, 43–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hong, J.-S.; Kang, H.-C. Seasonal variation in case fatality rate in Korean patients with acute myocardial infarction using the 1997-2006 Korean National Health Insurance Claims Database. Acta Cardiol. 2014, 69, 513–521. [Google Scholar] [CrossRef] [PubMed]
- Ye, X.; Peng, L.; Kan, H.; Wang, W.; Geng, F.; Mu, Z.; Zhou, J.; Yang, D. Acute Effects of Particulate Air Pollution on the Incidence of Coronary Heart Disease in Shanghai, China. PLoS ONE 2016, 11, e0151119. [Google Scholar] [CrossRef]
- Nawrot, T.S.; Torfs, R.; Fierens, F.; De Henauw, S.; Hoet, P.H.; Van Kersschaever, G.; De Backer, G.; Nemery, B. Stronger associations between daily mortality and fine particulate air pollution in summer than in winter: Evidence from a heavily polluted region in western Europe. J. Epidemiol. Community Health 2007, 61, 146–149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dai, L.; Zanobetti, A.; Koutrakis, P.; Schwartz, J.D. Associations of fine particulate matter species with mortality in the United States: A multicity time-series analysis. Environ. Health Perspect. 2014, 122, 837–842. [Google Scholar] [CrossRef]
- Milojevic, A.; Wilkinson, P.; Armstrong, B.; Bhaskaran, K.; Smeeth, L.; Hajat, S. Short-term effects of air pollution on a range of car-diovascular events in England and Wales: Case-crossover analysis of the MINAP database, hospital admissions and mortality. Heart 2014, 100, 1093–1098. [Google Scholar] [CrossRef]
- Dominici, F.; Peng, R.D.; Bell, M.L.; Pham, L.; McDermott, A.; Zeger, S.L.; Samet, J.M. Fine Particulate Air Pollution and Hospital Admission for Cardiovascular and Respiratory Diseases. JAMA 2006, 295, 1127–1134. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Ambient air pollution: A global assessment of exposure and burden of disease. Clean Air J. 2016, 26. [Google Scholar] [CrossRef]
- Cao, J.; Chow, J.C.; Lee, F.S.; Watson, J.G. Evolution of PM2. 5 measurements and standards in the US and future perspectives for China. Aerosol Air Qual. Res. 2013, 13, 1197–1211. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Air Pollutants | Mean ± SD | Min | P25 | Median | P75 | Max |
|---|---|---|---|---|---|---|
| PM2.5 a () | 25.7 ± 14.2 | 3.0 | 16.0 | 23.0 | 32.0 | 122 |
| CO (ppb) | 590 ± 241 | 218 | 427 | 529 | 683 | 1835 |
| SO2 (ppb) | 5.46 ± 2.26 | 2.30 | 3.86 | 4.87 | 6.45 | 22.0 |
| NO2 (ppb) | 33.98 ± 12.37 | 6.50 | 24.4 | 32.2 | 42.2 | 89.4 |
| Meteorological indicators | ||||||
| Daily average temperature (°C) | 12.7 ± 10.6 | −14.5 | 3.7 | 14.3 | 22.4 | 31.8 |
| Daily maximum temperature (°C) | 17.1 ± 10.8 | −10.7 | 7.8 | 19.0 | 26.6 | 36.7 |
| Daily minimum temperature (°C) | 8.96 ± 10.7 | −17.8 | −0.2 | 9.9 | 18.7 | 28.7 |
| Relative humidity (%) | 60.6 ± 15.0 | 19.9 | 49.4 | 60.6 | 71.5 | 99.8 |
| Dew point temperature (°C) | 4.55 ± 12.1 | −25.4 | −5.20 | 5.15 | 15.1 | 25.3 |
| Lag Day | RR (95% CI) | |||
|---|---|---|---|---|
| None | +CO | +SO2 | +NO2 | |
| Lag 0 | 1.011 (1.003–1.020) * | 1.018 (1.005–1.031) * | 1.013 (1.000–1.025) * | 1.013 (1.001–1.024) * |
| Lag 1 | 1.004 (0.995–1.012) | 0.998 (0.985–1.011) | 1.005 (0.992–1.017) | 0.993 (0.982–1.004) |
| Lag 2 | 1.000 (0.991–1.009) | 0.999 (0.986–1.012) | 1.000 (0.988–1.013) | 0.995 (0.984–1.006) |
| Lag 3 | 0.997 (0.989–1.006) | 0.999 (0.986–1.012) | 1.003 (0.991–1.015) | 0.996 (0.985–1.007) |
| Lag 01 | 1.010 (1.000–1.020) * | 1.012 (0.997–1.027) | 1.011 (0.997–1.025) | 1.004 (0.991–1.017) |
| Lag 02 | 1.006 (0.995–1.017) | 1.004 (0.987–1.021) | 1.007 (0.991–1.023) | 0.994 (0.979–1.009) |
| Lag 03 | 1.002 (0.990–1.014) | 1.001 (0.982–1.019) | 1.007 (0.989–1.025) | 0.989 (0.972–1.006) |
| Temperature (°C) | Lag 0 | Lag 1 | Lag 2 | Lag 3 | Lag 01 | Lag 02 | Lag 03 |
|---|---|---|---|---|---|---|---|
| <3.70 | 0.983 (0.964–1.002) | 0.988 (0.972–1.005) | 0.989 (0.973–1.005) | 0.992 (0.977–1.008) | 0.985 (0.965–1.004) | 0.980 (0.960–1.001) | 0.977 (0.956–0.999) |
| 3.70–14.30 | 1.030 (1.014–1.046) * | 1.006 (0.990–1.022) | 1.002 (0.986–1.019) | 1.000 (0.983–1.016) | 1.024 (1.006–1.042) * | 1.022 (1.002–1.042) * | 1.018 (0.996–1.041) |
| 14.30–22.40 | 1.017 (0.998–1.037) | 1.007 (0.998–1.025) | 1.011 (0.993–1.031) | 1.002 (0.984–1.020) | 1.015 (0.995–1.036) | 1.019 (0.997–1.042) | 1.018 (0.995–1.043) |
| ≥22.40 | 1.003 (0.984–1.023) | 1.011 (0.992–1.031) | 1.000 (0.981–1.019) | 0.999 (0.979–1.020) | 1.008 (0.986–1.030) | 0.999 (0.975–1.024) | 0.994 (0.967–1.022) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shin, J.; Oh, J.; Kang, I.-S.; Ha, E.; Pyun, W.-B. Effect of Short-Term Exposure to Fine Particulate Matter and Temperature on Acute Myocardial Infarction in Korea. Int. J. Environ. Res. Public Health 2021, 18, 4822. https://doi.org/10.3390/ijerph18094822
Shin J, Oh J, Kang I-S, Ha E, Pyun W-B. Effect of Short-Term Exposure to Fine Particulate Matter and Temperature on Acute Myocardial Infarction in Korea. International Journal of Environmental Research and Public Health. 2021; 18(9):4822. https://doi.org/10.3390/ijerph18094822
Chicago/Turabian StyleShin, Jiyoung, Jongmin Oh, In-Sook Kang, Eunhee Ha, and Wook-Bum Pyun. 2021. "Effect of Short-Term Exposure to Fine Particulate Matter and Temperature on Acute Myocardial Infarction in Korea" International Journal of Environmental Research and Public Health 18, no. 9: 4822. https://doi.org/10.3390/ijerph18094822
APA StyleShin, J., Oh, J., Kang, I. -S., Ha, E., & Pyun, W. -B. (2021). Effect of Short-Term Exposure to Fine Particulate Matter and Temperature on Acute Myocardial Infarction in Korea. International Journal of Environmental Research and Public Health, 18(9), 4822. https://doi.org/10.3390/ijerph18094822