
The Complexity of Decreased Work Ability: Individuals’ Perceptions of Factors That Affect Returning to Work after Sickness Absence


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Qualitative Interviews
2.3. Narrative and Thematic Analysis of the Interviews
3. Results
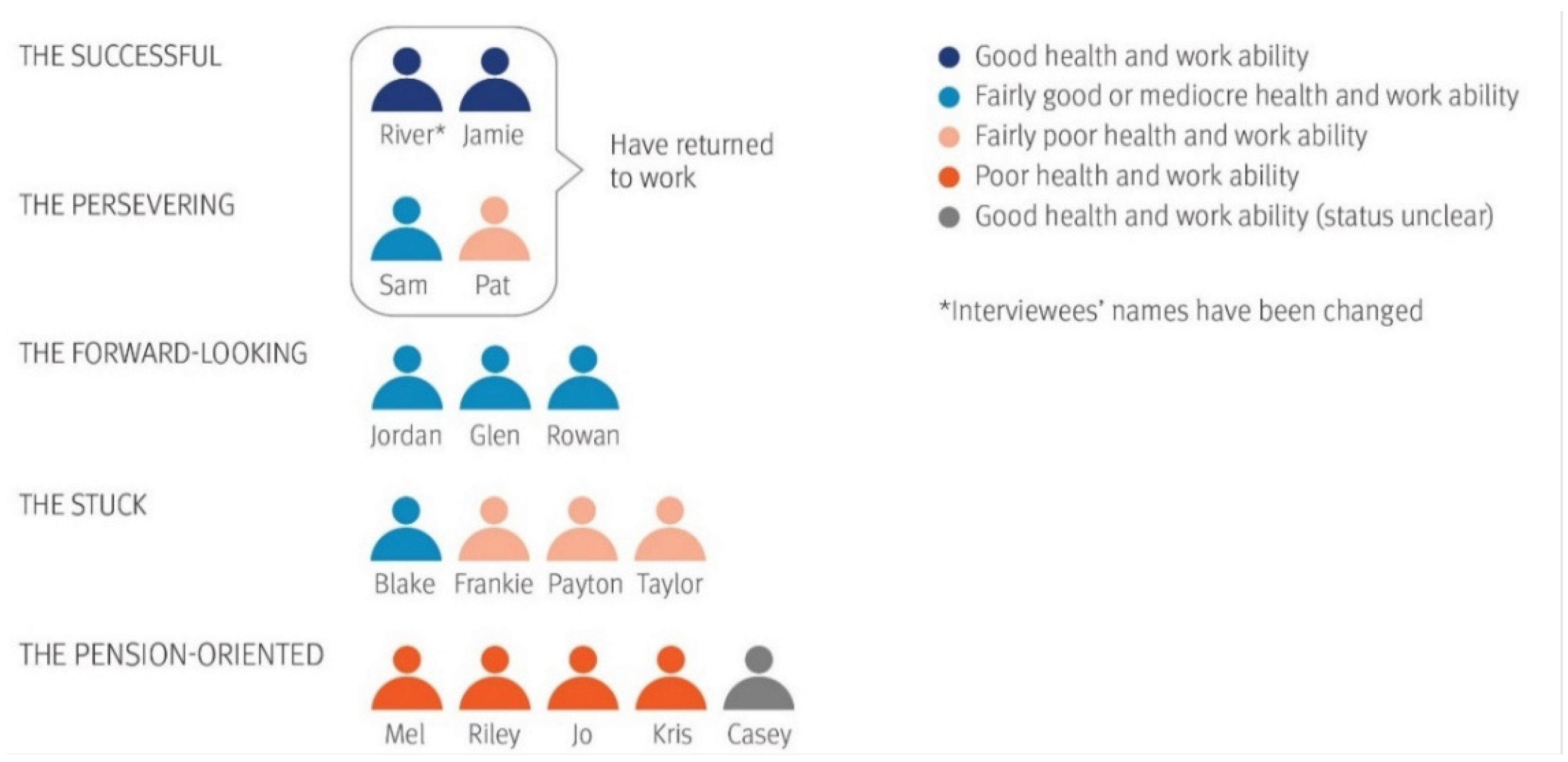
3.1. Perceived Health and Work Ability Predicted Return to Work
- The Successful: work-oriented, returned to work, well-recovered and -motivated: River and Jamie
- The Persevering: somewhat work-oriented, returned to work, not fully recovered, concerned about their work ability: Sam and Pat
- The Forward-looking: work-oriented, have not returned to work, not fully recovered, motivated to find a new job: Jordan, Glen and Rowan
- The Stuck: somewhat pension-oriented, have not returned to work, not recovered, passive: Blake, Frankie, Payton and Taylor
- The Pension-oriented: have not returned to work, not recovered, demotivated: Mel, Riley, Jo, Kris and Casey
3.1.1. The Successful Group: Well-Recovered and Returned to Work
3.1.2. The Persevering: Returned to Work despite Work Ability Concerns
3.1.3. The Forward-Looking: Searching for New Opportunities
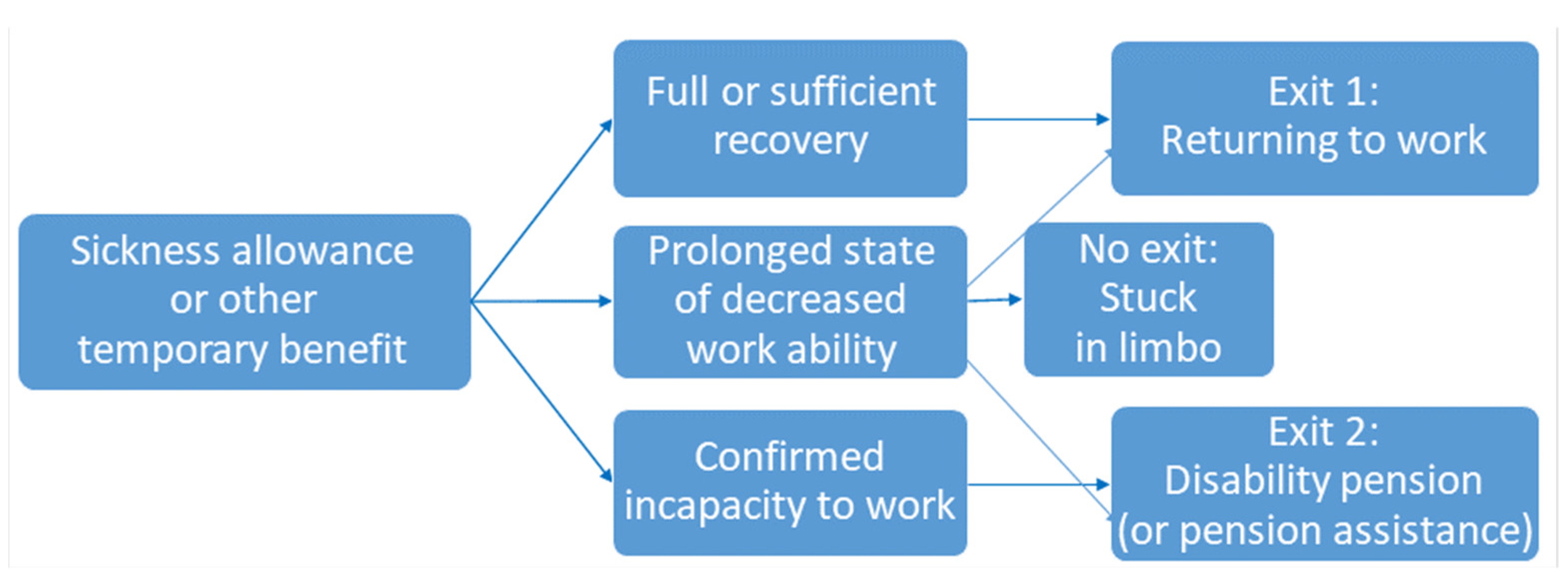
3.1.4. The Stuck: Having No Clear Exit from Temporary Benefits
3.1.5. The Pension-Oriented: Inclination towards Early Retirement
3.2. Supporting Sustainable Work Ability
3.2.1. Age and Skills as Factors Affecting Returning to Work
3.2.2. The Importance of a Coherent Health Care Service System
3.2.3. The Challenges and Potential of Multi-Professional, Holistic Counselling
3.2.4. Exits: Justified Career Orientations
4. Discussion
4.1. Main Findings
4.2. Limitations
4.3. Interpretation and Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Pseudo-nym 1 | Age 2 | Worker/Entrep. 3 | Sector 4 | Health concern 5 | RTW 6 | Situation 7 | Plan 8 | SAH 9 (1–5) | WA 10 (0–10) | Readiness 11(0–10) | TOIKE 12 | Summary 13 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Jamie | ≥51 | Entrep. | Agric. | Shoulder injury | Yes | Recovered, returned-to-work | Continues in old job | 4 | 8 | 10 | No. | Work-oriented, well recovered, motivated |
| River | 40–50 | Worker | Health | Back pain | Yes | Recovered, returned-to-work | Continues in old job | 4 | 9 | 10 | No. | Work-oriented, well recovered, motivated |
| Sam | 40–50 | Worker | Constr. | Back pain and burnout | Yes | Has pain, but returned-to-work | Continues in old job | 3 | 5.5 | ? | Yes. No visit was booked. | Somewhat work- oriented, not fully recovered, work ability concerns |
| Pat | ≤39 | Entrep. | Constr. | Back and leg pain | Yes | Has pain, but returned-to-work | Continues in old job | 2 | 4 | ? | No. | Somewhat work- oriented, not fully recovered, work ability concerns |
| Glen | ≤39 | Worker | Logistics | Shoulder injury | No | Unemployed after sick-leave | Needs a new direction | 3 | 5.5 | 7.5 | No, but considers. | Work-oriented, not fully recovered, hopeful |
| Jordan | ≤39 | Worker | Hosp. | Back and leg pain | No | Sick-leave | Going to re-education | 4 | 4.5 | 2.5 | No. | Work-oriented, not fully recovered, hopeful |
| Rowan | ≤39 | Worker | Transp. | Back pain + other | No | Sick-leave | Needs a new direction. Going to a work tryout | 3 | 3 | 3.5 | No, but considers. | Work-oriented, not fully recovered, hopeful |
| Taylor | ≥51 | Worker | Manuf. | Shoulder injury, dyslexia, memory disorders | No | Prolonged absence: sick-leave/ unemployed | Cannot find work | 2 | 5 | ? | No. | Somewhat pension-oriented, not recovered, hesitant, passive |
| Blake | ≥51 | Worker | Manuf. | Arm injury (+ mental health) | No | Unstable work history | Temporary disability pension | 3 | 5.5 | 6.5 | Yes. No visit was booked. | Somewhat pension-oriented, not recovered, hesitant, passive |
| Frankie | 40–50 | Worker | Agric. | Arm & knee pain, arthritis, dyslexia | No | Prolonged absence: sick-leave/ unemployed | Cannot find work. Applying for partial disability pension | 2 | 4 | 5 | Yes. Has visited. | Somewhat pension-oriented, not recovered, hesitant, passive |
| Peyton | 40–50 | Entrep. | Maint. | Arm pain | No | Rehabilitee/ partial disability pension | May return to work | 1 | 2.5 | 3.5 | No. | Somewhat pension-oriented, not recovered, hesitant, passive |
| Kris | ≥51 | Entrep. | Constr. | Back/leg pain + other | No | Business ceased. Receives sickness allowance | Applying for disability pension | 1 | 0 | 0 | No. | Pension-oriented, disabled, reluctant |
| Mel | ≥51 | Worker | Manuf. | Back pain | No | Cannot return to old job due to sickness | Applying for partial disability pension | 2.5 | 0.5 | ? | Yes. Has visited. | Pension-oriented, disabled, reluctant |
| Jo | ≥51 | Worker | Constr. | Knee pain | No | Attended rehabilitation. Receives sickness allowance | Applying for disability pension | 2 | 2 | 0 | Yes. Has a visit booked. | Pension-oriented, disabled, reluctant |
| Riley | ≥51 | Entrep. | Maint. | Back/ wrist pain + other | No | Business ceased. Receives sickness allowance | Going to rehabilitation. Applying for disability pension | 1 | 2 | 0 | No. | Pension-oriented, disabled, reluctant |
| Casey | ≥51 | Worker | Office | Unclear, reports to be healthy | No | Attended rehabilitation and activation measures | Cannot find work | 4 | 9 | 10 | No. | Pension-oriented, health status unclear, reluctant |
References
- Barnett, K.; Mercer, S.W.; Norbury, M.; Watt, G.; Wyke, S.; Guthrie, B. Epidemiology of multimorbidity and implications for health care, research, and medical education: A cross-sectional study. Lancet 2012, 380, 37–43. [Google Scholar] [CrossRef] [Green Version]
- Riekhoff, A.-J. Retirement Trajectories in the Netherlands and Finland Institutional Change, Inequalities, de-Standardisation and Destabilisation. Doctoral Thesis, Tampere University, Tampere, Finland, 2018. [Google Scholar]
- Vornholt, K.; Villotti, P.; Muschalla, B.; Bauer, J.; Colella, A.; Zijlstra, F.; Van Ruitenbeek, G.; Uitdewilligen, S.; Corbière, M. Disability and employment—Overview and highlights. Eur. J. Work Organ. Psychol. 2018, 27, 40–55. [Google Scholar] [CrossRef] [Green Version]
- Adams, G.A.; Beehr, T.A. Retirement: Reasons, Processes, and Results; Springer Pub: New York, NY, USA, 2003. [Google Scholar]
- Vuori, J.; Blonk, R.; Price, R.H. Sustainable Working Lives: Managing Work Transitions and Health throughout the Life Course; Springer: Dordrecht, The Netherlands, 2015. [Google Scholar]
- Pekkala, J. Occupational Class Differences in Sickness Absence: Changes over Time and Diagnostic Causes. Doctoral Thesis, University of Helsinki, Helsinki, Finland, 2018. [Google Scholar]
- Lmarinen, J.; Gould, R.; Järvikoski, A.; Järvisalo, J. Diversity of work ability. In Dimensions of Work Ability. Results of the Health 2000 Survey; Gould, R., Ilmarinen, J., Järvisalo, J., Koskinen, S., Eds.; Finnish Centre for Pensions: Helsinki, Finland, 2008; pp. 13–24. [Google Scholar]
- United Nations. Transforming Our World: The 2030 Agenda for Sustainable Development. Available online: https://sustainabledevelopment.un.org/post2015/transformingourworld/publication (accessed on 2 November 2021).
- Loisel, P.; Durand, M.-J.; Berthelette, D.; Vézina, N.; Baril, R.; Gagnon, D.; Larivière, C.; Tremblay, C. Disability prevention: New paradigm for the management of occupational back pain. Dis. Manag. Health Outcomes 2001, 9, 351–360. [Google Scholar] [CrossRef]
- Pransky, G.S.; Loisel, P.; Anema, J.R. Work disability prevention research: Current and future prospects. J. Occup. Rehabil. 2011, 21, 287–292. [Google Scholar] [CrossRef] [Green Version]
- Ekberg, K.; Wåhlin, C.; Persson, J.; Bernfort, L.; Öberg, B. Is mobility in the labor market a solution to sustainable return to work for some sick listed persons? J. Occup. Rehabil. 2011, 21, 355–365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gjersøe, H.M. Getting sick and disabled people off temporary benefit receipt: Strategies and dilemmas in the welfare state’s frontline. Nord. J. Work. Life Stud. 2016, 6, 129–145. [Google Scholar] [CrossRef] [Green Version]
- Kerätär, R.; Taanila, A.; Jokelainen, J.; Soukainen, J.; Ala-Mursula, L. Work disabilities and unmet needs for health care and rehabilitation among jobseekers: A community-level investigation using multidimensional work ability assessments. Scand. J. Prim. Health Care 2016, 34, 343–351. [Google Scholar] [CrossRef] [Green Version]
- MacEachen, E.; Kosny, A.; Ferrier, S.; Chambers, L. The “toxic dose” of system problems: Why some injured workers don’t return to work as expected. J. Occup. Rehabil. 2010, 20, 349–366. [Google Scholar] [CrossRef] [PubMed]
- Salonen, L.; Blomgren, J.; Laaksonen, M.; Niemelä, M. Sickness absence as a predictor of disability retirement in different occupational classes: A register-based study of a working-age cohort in Finland in 2007–2014. BMJ Open 2018, 8, e020491. [Google Scholar] [CrossRef]
- Haugli, L.; Maeland, S.; Magnussen, L.H. What facilitates return to work? Patients experiences 3 years after occupational rehabilitation. J. Occup. Rehabil. 2011, 21, 573–581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lydell, M.; Hildingh, C.; Månsson, J.; Marklund, B.; Grahn, B. Thoughts and feelings of future working life as a predictor of return to work: A combined qualitative and quantitative study of sick-listed persons with musculoskeletal disorders. Disabil. Rehabil. 2011, 33, 1262–1271. [Google Scholar] [CrossRef]
- Sanders, T.; Wynne-Jones, G.; Nio Ong, B.; Artus, M.; Foster, N. Acceptability of a vocational advice service for patients consulting in primary care with musculoskeletal pain: A qualitative exploration of the experiences of general practitioners, vocational advisers and patients. Scand. J. Public Health 2019, 47, 78–85. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. International Classification of Functioning, Disability and Health: ICF; World Health Organization: Geneva, Switzerland, 2001; ISBN 978-92-4-154542-6. [Google Scholar]
- Metteri, A. Hyvinvointivaltion Lupaukset, Kohtuuttomat Tapaukset ja Sosiaalityö (Promises of a Welfare state, Non-Fulfilment of These Promises and Social Work). Doctoral Thesis, Tampere University, Tampere, Finland, 2012. [Google Scholar]
- Lahey, P. From Welfare to Work for People with Disabilities in Receipt of Public Income Benefits: A Wicked Problem for Policy Makers. Doctoral Thesis, McMaster University, Hamilton, ON, Canada, 2019. Available online: http://hdl.handle.net/11375/23823 (accessed on 22 December 2021).
- Blackman, T.; Greene, A.; Hunter, D.J.; McKee, L.; Elliott, E.; Harrington, B.; Marks, L.; Williams, G. Performance assessment and wicked problems: The case of health inequalities. Public Policy Adm. 2006, 21, 66–80. [Google Scholar] [CrossRef]
- Saikku, P.; Karjalainen, V. Network governance in activation policy—Health care as an emergent partner. Int. J. Sociol. Soc. Policy 2012, 32, 299–311. [Google Scholar] [CrossRef]
- Mattila-Wiro, P.; Tiainen, R. Involving All in Working Life—Results and Recommendations from OTE Key Project ‘Career Opportunities for People with Partial Work Ability’; Reports and Memorandums of the Ministry of Social Affairs and Health: Helsinki, Finland, 2019; p. 36.
- Määttä, A. Työkyvytön vai työtön? Työkyvyttömyydestä aiheutuva sosiaaliturvan väliinputoaminen elämänkaaren eri vaiheissa (Unfit for work or unemplyed? Falling outside social security schemes due to work disability during different stages of the lifespan). Kuntoutus 2011, 34, 18–28. [Google Scholar]
- Elliott, J. Using Narrative in Social Research: Qualitative and Quantitative Approaches; SAGE: London, UK, 2005. [Google Scholar]
- Silverman, D. Doing Qualitative Research: A Practical Handbook, 3rd ed.; SAGE: London, UK, 2010. [Google Scholar]
- Grant, C.; Osanloo, A. Understanding, selecting, and integrating a theoretical framework in dissertation research: Creating the blueprint for your “house”. Adm. Issues J. Educ. Pract. Res. 2016, 4, 12–16. [Google Scholar] [CrossRef] [Green Version]
- Elo, S.; Kyngäs, H. The qualitative content analysis process. J. Adv. Nurs. 2008, 62, 107–115. [Google Scholar] [CrossRef]
- Heikkinen, V.; Uitti, J. Osatyökykyisille tie työelämään (OTE), Polut hoitoon ja kuntoutukseen, Projekti 7 (Road to Work for Individuals with Decreased Work Ability, Pathways to Healthcare and Rehabilitation, Project 7). Available online: https://docplayer.fi/48361905-Hallituksen-karkihanke-osatyokykyisille-tie-tyoelamaan-ote-polut-hoitoon-ja-kuntoutukseen-projekti-7.html (accessed on 2 November 2021).
- Vuokila-Oikkonen, P.; Janhonen, S.; Nikkonen, M. Kertomukset hoitotieteellisen tiedon tuottamisessa: Narratiivinen lähestymistapa (Stories in producing knowledge for nursing science: A narrative approach). In Laadulliset tutkimusmenetelmät hoitotieteessä (Qualitative Methods in Nursing Science); Janhonen, S., Nikkonen, M., Eds.; WSOY: Juva, Finland, 2001; pp. 81–115. [Google Scholar]
- Green, J.; Thorogood, N. Qualitative Methods for Health Research, 4th ed.; SAGE: Los Angeles, CA, USA, 2018. [Google Scholar]
- Tuomi, K.; Ilmarinen, J.; Jahkola, A.; Katajarinne, L.; Tulkki, A. Work Ability Index, 2nd ed.; Finnish Institute of Occupational Health: Helsinki, Finland, 1998. [Google Scholar]
- Gould, R.; Koskinen, S.; Seitsamo, J.; Tuomi, K.; Polvinen, A.; Sainio, P. Data and Methods. In Dimensions of Work Ability. Results of the Health 2000 Survey; Gould, R., Ilmarinen, J., Järvisalo, J., Koskinen, S., Eds.; Finnish Centre for Pensions: Helsinki, Finland, 2008; pp. 25–32. [Google Scholar]
- Graneheim, U.H.; Lundman, B. Qualitative content analysis in nursing research: Concepts, procedures and measures to achieve trustworthiness. Nurse Educ. Today 2004, 24, 105–112. [Google Scholar] [CrossRef]
- Dwyer, D.S.; Mitchell, O.S. Health problems as determinants of retirement: Are self-rated measures endogenous? J. Health Econ. 1999, 18, 173–193. [Google Scholar] [CrossRef] [Green Version]
- Heikkinen, V. Pitkäaikaistyötön vai pysyvästi työkyvytön: Tyyppitarinoita 2000-luvun teollisuuskaupungista (Long-Term Unemployed or Permanently Disabled—Types and Narratives from an Industrial Town of the 2000s). Ph.D. Thesis, Tampere University, Tampere, Finland, 2016. [Google Scholar]
- Harkonmäki, K. Predictors of Disability Retirement from Early Intentions to Retirement. Doctoral Thesis, University of Helsinki, Helsinki, Finland, 2007. [Google Scholar]
- Jahoda, M. Employment and Unemployment; Cambridge University Press: Cambridge, UK, 1982. [Google Scholar]
- Ministry of Social Affairs and Health. Kuntoutuksen Uudistamiskomitean Ehdotukset Kuntoutusjärjestelmän Uudistamiseksi (Recommendations of the Rehabilitation Reform Committee for Reforming Rehabilitation); Reports and Memorandums of the Ministry of Social Affairs and Health: Helsinki, Finland, 2017; p. 89. [Google Scholar]
- Beehr, T.A. The process of retirement: A review and recommendations for future investigation. Pers. Psychol. 1986, 39, 31–55. [Google Scholar] [CrossRef]
- Kohli, M.; Rein, M.; Guillemard, A.-M.; van Gunsteren, H. (Eds.) Time for Retirement: Comparative Studies of Early Exit from the Labor Force; Cambridge University Press: Cambridge, UK, 1991. [Google Scholar]
- Heslin, P.A.; Keating, L.A.; Ashford, S.J. How being in learning mode may enable a sustainable career across the lifespan. J. Vocat. Behav. 2020, 117, 103324. [Google Scholar] [CrossRef]
- Sen, A. Development as Freedom, 1st ed.; Oxford University Press: Oxford, UK, 1999. [Google Scholar]
- Tamin, J. Occupational Health Ethics: From Theory to Practice; Springer Nature: Cham, Switzerland, 2020; Chapter 5; ISBN 978-3-030-47282-5. [Google Scholar]
- Aalto, A.-M.; Elovainio, M.; Tynkkynen, L.-K.; Reissell, E.; Vehko, T.; Chydenius, M.; Sinervo, T. What patients think about choice in healthcare? A study on primary care services in Finland. Scand. J. Public Health 2018, 46, 463–470. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poutanen, S.; Kovalainen, A.; Rouvinen, P. (Eds.) Digital Work and the Platform Economy: Understanding Tasks, Skills and Capabilities in the New Era, 1st ed.; Routledge: New York, NY, USA, 2019; ISBN 978-0-429-46792-9. [Google Scholar]
- Schoukens, P. Digitalisation and social security in the EU. The case of platform work: From work protection to income protection? Eur. J. Soc. Secur. 2020, 22, 434–451. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Näsi, E.; Perkiö, M.; Kokkinen, L. The Complexity of Decreased Work Ability: Individuals’ Perceptions of Factors That Affect Returning to Work after Sickness Absence. Int. J. Environ. Res. Public Health 2022, 19, 113. https://doi.org/10.3390/ijerph19010113
Näsi E, Perkiö M, Kokkinen L. The Complexity of Decreased Work Ability: Individuals’ Perceptions of Factors That Affect Returning to Work after Sickness Absence. International Journal of Environmental Research and Public Health. 2022; 19(1):113. https://doi.org/10.3390/ijerph19010113
Chicago/Turabian StyleNäsi, Ella, Mikko Perkiö, and Lauri Kokkinen. 2022. "The Complexity of Decreased Work Ability: Individuals’ Perceptions of Factors That Affect Returning to Work after Sickness Absence" International Journal of Environmental Research and Public Health 19, no. 1: 113. https://doi.org/10.3390/ijerph19010113
APA StyleNäsi, E., Perkiö, M., & Kokkinen, L. (2022). The Complexity of Decreased Work Ability: Individuals’ Perceptions of Factors That Affect Returning to Work after Sickness Absence. International Journal of Environmental Research and Public Health, 19(1), 113. https://doi.org/10.3390/ijerph19010113