Parameterization of the Models
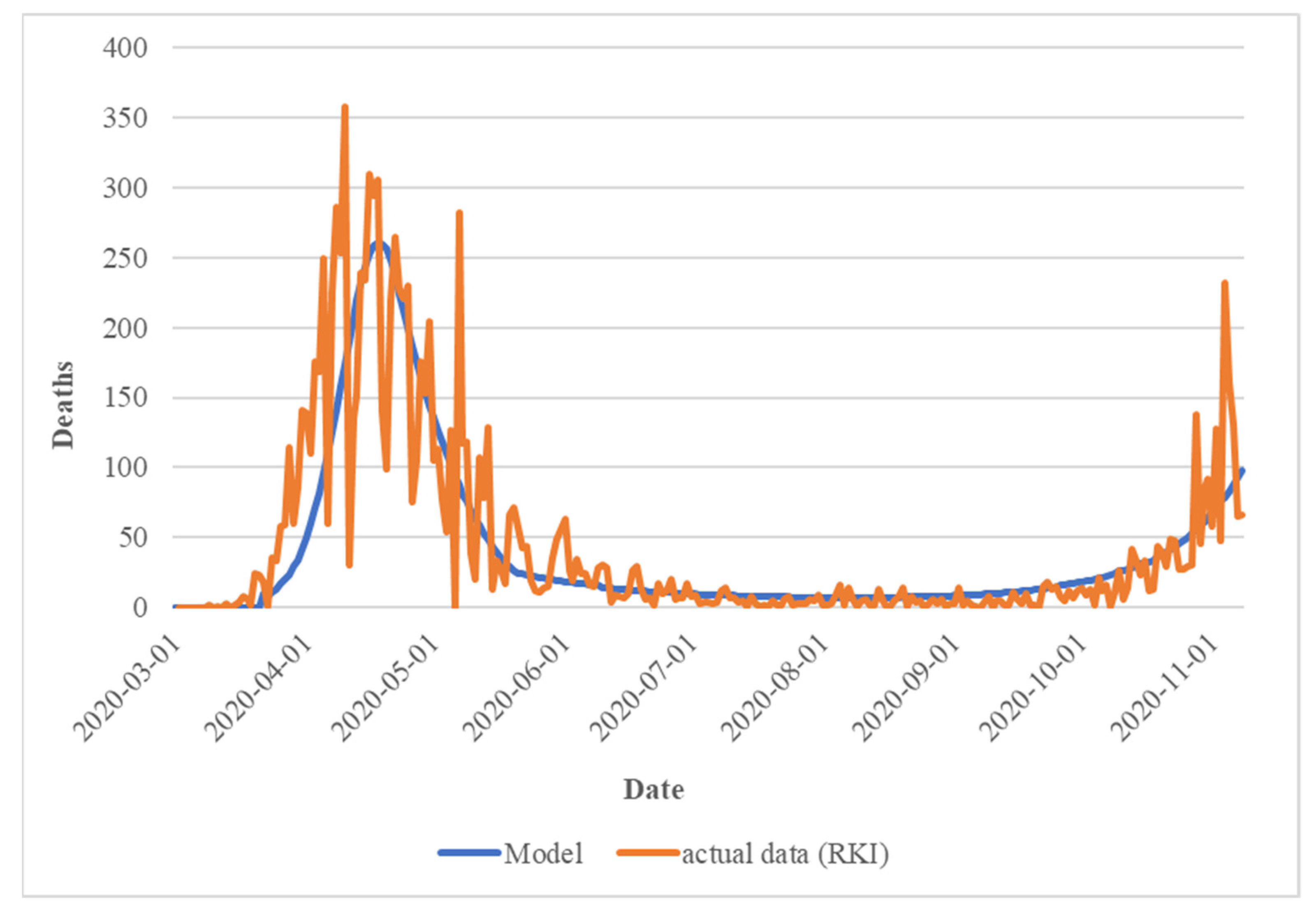
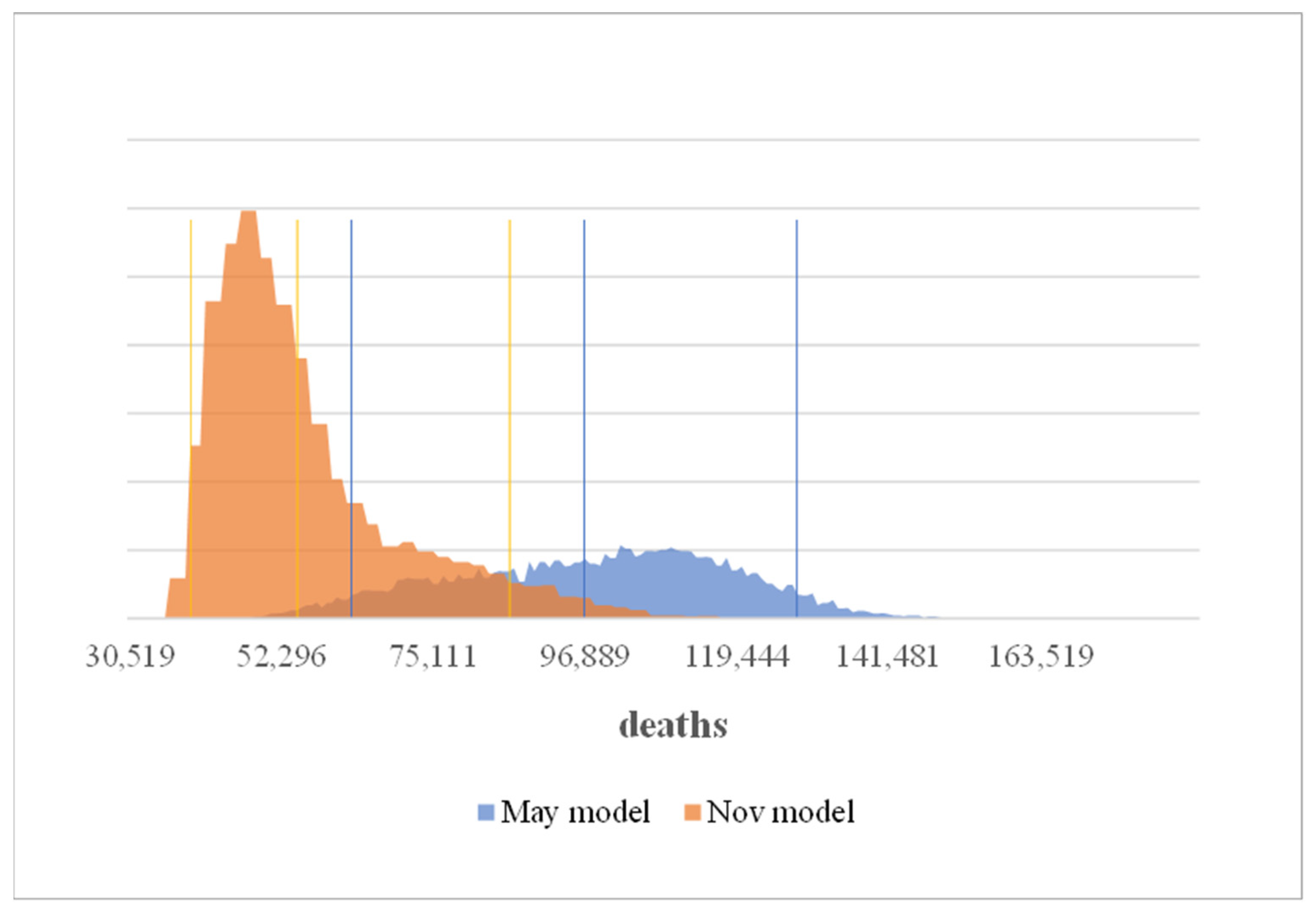
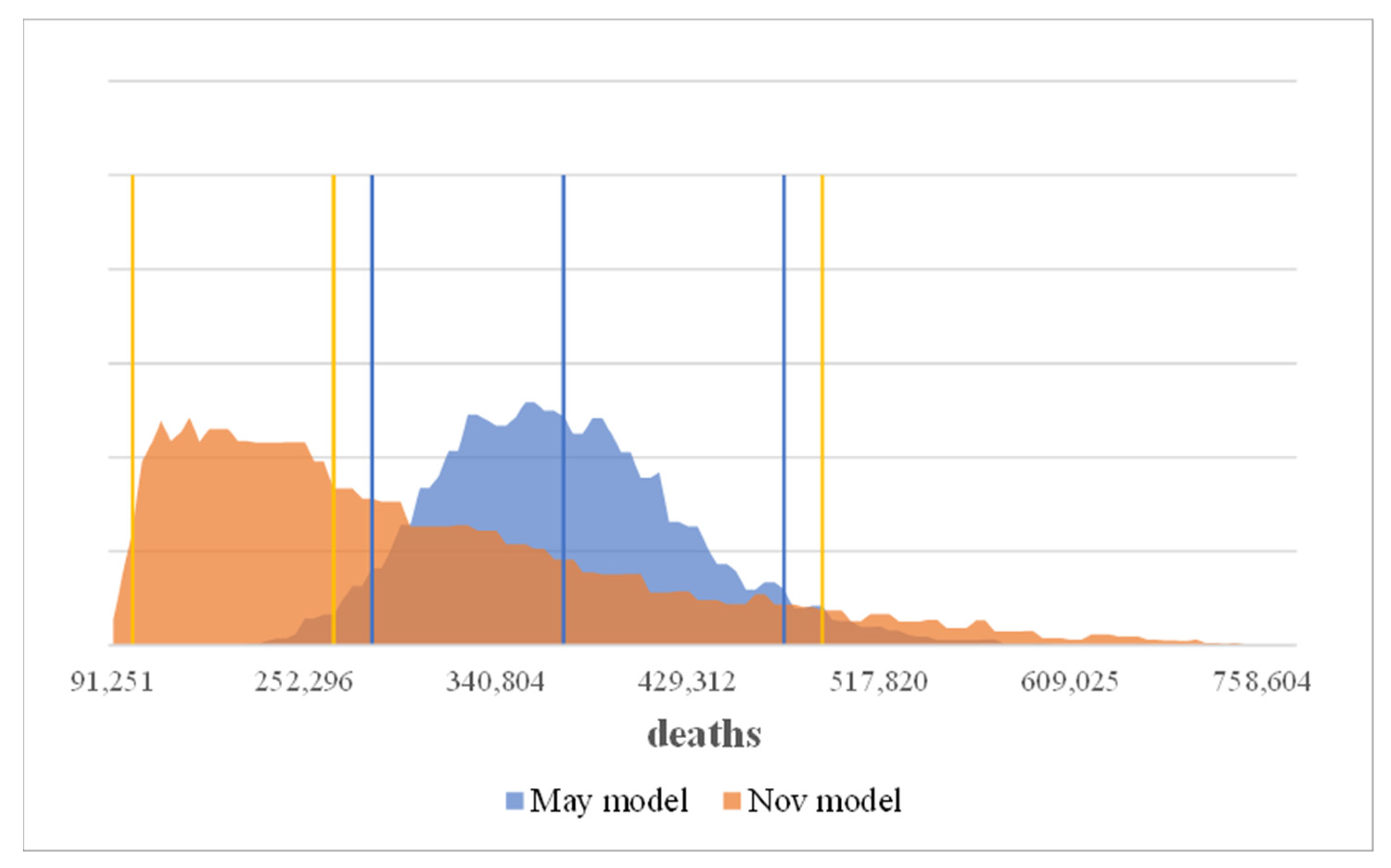
To parameterize the model, a parameter set was developed based on the existing estimates to simulate the course of events in Germany between 1 March 2020 and the respective time of the simulation, until 3 May 2020 (May model) and 10 November 2020 (Nov. model), as closely as possible. These parameters were also fixed for this period of time, but the predicted course—as mentioned above—was provided with bandwidths (uncertainties).
It is important to keep in mind that this parameterization took place at the relative beginning of the pandemic and was based on initial estimates by experts. This also required assumptions to be made about the behavior of politicians. These were also based on the behavior shown up to that point, which changed over time. Thus, from today’s perspective, some of these figures appear to be clearly wrong, but from the perspective of the time, this was the best available information. This also shows, however, that the level of information changes over time and that new parameterizations and remodeling are regularly necessary, and the findings from newer models can very well lead to different decisions. The following
Appendix A Table A1 shows the basic parameters of our models.
Table A1.
Basic parameters of the models.
Table A1.
Basic parameters of the models.
| | May Model | November Model |
|---|
| Starting Point | 1 March 2020 |
| Population (in million) | 82 |
| R0 | 2.03 | 2.07 |
| Number of infected persons at starting point | 380 | 500 |
| Duration of infection time in days (Tinf) | 6 |
| Incubation time * in days (Tinc) | 2 | 1 |
| Recovery after x days | 8 |
| Unreported case factor at the beginning/in the long run ** | 17.5/10 | 7/4 |
| Starting point of uncertainty | 18 January 2020 | 11 October 2020 |
For the factor of the unreported cases for the prognosis period of each model, an additional uncertainty ±10% was used. The starting value of the R-value was redetermined based on the abovementioned estimates in connection with the estimated number of unreported cases at the starting point and was included in the model with a value of 2.03. To parameterize the second model, all input factors were re-estimated based on the development in Germany between 1 March 2020 and 10 November 2020 as well as on the latest expert estimates. The newer RKI estimates show that in the beginning, there was probably a higher R-value. A mean estimate of 2.7 was adopted. The other values—in particular, the number of infected persons at the beginning of March and the length of the incubation period—were adjusted to explain the course of the disease well in the context of the changed effect of the measures.
To simulate the course between 1 March 2020 and the beginning of the model, including measures that have already taken place and are therefore exogenous measures in the model, in terms of the case numbers, death rates and observed
R, the following (safe) effects of the exogenous measures were determined so that the process could be recreated well (fitted). Compared to the status in April in the Nov. model, the relaxation phase and the beginning of the retightening phase were added. In particular, the modeling was extended by a factor that changed the increase in the
R-factor (in a loosening phase) depending on the season. Only this factor can explain the strong decrease in April and May, the low levels in summer, and the strong increase in November (
Appendix A Table A2).
Table A2.
Adapted parameters of the models.
Table A2.
Adapted parameters of the models.
| Parameters | (Static) Value for Calibration |
|---|
| | May Model | Nov. Model |
|---|
Date of first recommendation
(1st exogenous measure) | 11 March 2020 (the 10th day) |
| Max. reduction factor * of the first recommendation | 65% | 60% |
δR of the first recommendation
(per day) | −0.02 | −0.09 |
Date of the “shutdown”
(2nd exogenous measure) | 22 January 2020 (the 22nd day) |
| Max. reduction factor of the “shutdown” | 70% | 71% |
| δRcontain of the “shutdown” (per day) | −0.04 | −0.06 |
| Relaxation from | 20 April 2020 (the 49th day) |
| δRloose “relaxation” (per day) | | |
| between April and July | +0.0027 | +0.0023 |
| between August and March | +0.0027 | +0.0048 |
| “retightening” (mini-lockdown) | ------------- | 6 October 2020 (the 218th day) |
Both the development of
R and the cumulative costs are modeled depending on the uncertain effect of the endogenous measures. In the model, relaxation is endogenously initiated when the reproduction factor is below the given threshold value for a period (different in the two models). The measures are “tightened” again endogenously if the reproduction factor is above another threshold value or if the new infections minus the cured infections exceed its threshold value (
Appendix A Table A3). For these parameters, strong changes were necessary in some cases because the policy changed its behavior strongly. On the one hand, previous limit values were abandoned, and measures were taken much later; on the other hand, these measures themselves were modified or made less restrictive. For example, school closures were al-most completely removed from the catalog of measures for a long time.
Table A3.
Relaxation and retightening of measures.
Table A3.
Relaxation and retightening of measures.
| Initiation of a Phase before the Introduction of a Vaccine | Condition | Period (Consecutive Days) |
|---|
| | May Model | Nov. Model | May Model | Nov. Model |
|---|
| Relaxation phase | R < 0.85 | R < 0.80 | 10 | 14 |
| Retightening of measures after R or | R > 1.3 | 12 |
| Retightening of measures after net new infections (greater than) | 1300 | 10,000 | 12 |
The effects of the measures were reassessed in November. The increasing effect of an easing was overestimated in the first model—as the actual development showed—partly due to the oversimplified model of the mentioned effect of risk homeostasis. Therefore, this effect was weakened. In contrast, the minimum values for
R were increased slightly.
Appendix A Table A4 summarizes the uncertain effect of the measures used for the forecast on
R or on the costs. Regarding the effect on
R, the most likely values without uncertainty were used until the period 3 May 2020. Uncertainties were also considered for the costs for these periods, since the actual costs are still unknown. With the costs instead of the uncertainty in each period, the mean value of uncertainty was considered with the costs.
Table A4.
Uncertain effect of the measures used for the forecast on R or on the costs.
Table A4.
Uncertain effect of the measures used for the forecast on R or on the costs.
| Effect of the Measures on R (Per Day) * | Min | Probable | Max | Minimum Value R |
|---|
| | May | Nov. | May | Nov. | May | Nov. | May | Nov. |
|---|
| Relaxation phase | 0.036 | 0.0019 | 0.04 | 0.002 | 0.044 | 0.0023 | 0.75 |
| Retightening of measures | −0.009 | −0.01 | −0.011 | 0.61 | 0.75 |
| After introduction of a vaccine | −0.009 | −0.01 | −0.011 | 0.5 | 0.7 |
To model the costs, the (first) estimates of the Ifo Institute (including uncertainty ranges [
88]) were used. The cost of the first shutdown is still uncertain, but the estimates changed between May and November. To model the costs in the November model, new estimates of the GDP decline from Statista (before the November lockdown) were used (see
Appendix A Table A5).
Table A5.
Relative uncertainty ranges of costs in EUR bn.
Table A5.
Relative uncertainty ranges of costs in EUR bn.
| Phase | Min | Probable | Max |
|---|
| May | Nov. | May | Nov. | May | Nov. |
|---|
| 1st-month complete shutdown | 255 | 186 | 375 | 207 | 495 | 228 |
| 1st-month complete shutdown per day | 8.5 | 6.21 | 12.5 | 6.9 | 16.5 | 7.59 |
| further complete shutdown per day | 3.57 | 1.97 | 5.86 | 3,23 | 8.14 | 4.49 |
To determine the opportunity costs for an (endogenous) relaxation phase (without a complete return to normality) as well as for a possible renewed (endogenous) tightening of measures after a relaxation, the proportional costs were estimated from the above Ifo data for the May model and were also reconsidered in the November model on the basis of estimates of the costs of the November mini-lockdown (“shutdown light”, such as the mini-lockdown in November) based on DIW estimates of EUR 19 bn (see
https://www.handelsblatt.com/politik/deutschland/coronakrise-diw-zweiter-lockdown-kostet-wirtschaft-19-milliarden-euro/26579632.html?ticket=ST-6458254-MEOkgYN0gDd3PVrHTavQ-ap4 (accessed on 27 December 2021)) for 1 month (0.64 bn per day) of restrictions (see
Appendix A Table A6). The relative uncertainty ranges were taken from the first model. (Concerning the mini-lockdown the costs in the easing phase should probably not exceed the costs of a mini-lockdown. The values for the costs of a relaxation phase without a return to normality were assumed to be half the costs of the November mini-lockdown.
Table A6.
Estimated proportional costs.
Table A6.
Estimated proportional costs.
| Cost Factor (Related to Shutdown Costs) | Min | Probable | Max |
|---|
| | May | Nov. | May | Nov. | May | Nov. |
|---|
| Relaxation phase | 0.225 | 0.29 | 0.25 | 0.32 | 0.275 | 0.35 |
| Retightening | 0.45 | 0.58 | 0.5 | 0.64 | 0.55 | 0.71 |
To reduce complexity, it is assumed that no (direct) costs are incurred in the loosening phase and that there is no difference in the loosening strength.
With testing, unknown cases become known. In the starting period, 3% of already existing but still unknown infections (see the estimation of unreported cases,
Appendix A Table A7) are detected. Per period, this value decreases by 25%.
Table A7.
Estimation of unreported cases.
Table A7.
Estimation of unreported cases.
| | Value |
|---|
| Starting value | 3% |
| Reduction per period (share of previous period) | 25% |
| Minimum value | 0% |
In May 2020, an effective vaccine was still a long way off, accordingly, this period was modeled before the introduction of a vaccine (see
Appendix A Table A8).
Table A8.
Introduction of a vaccine.
Table A8.
Introduction of a vaccine.
| | Earliest | Probable | Latest |
|---|
| | May | Nov. | May | Nov. | May | Nov. |
|---|
| Date of introduction of a vaccine | 1 December 2020 | 9 January 2021 | 2 July 2021 | 8 March 2021 | 3 May 2023 | 8 November 2022 |
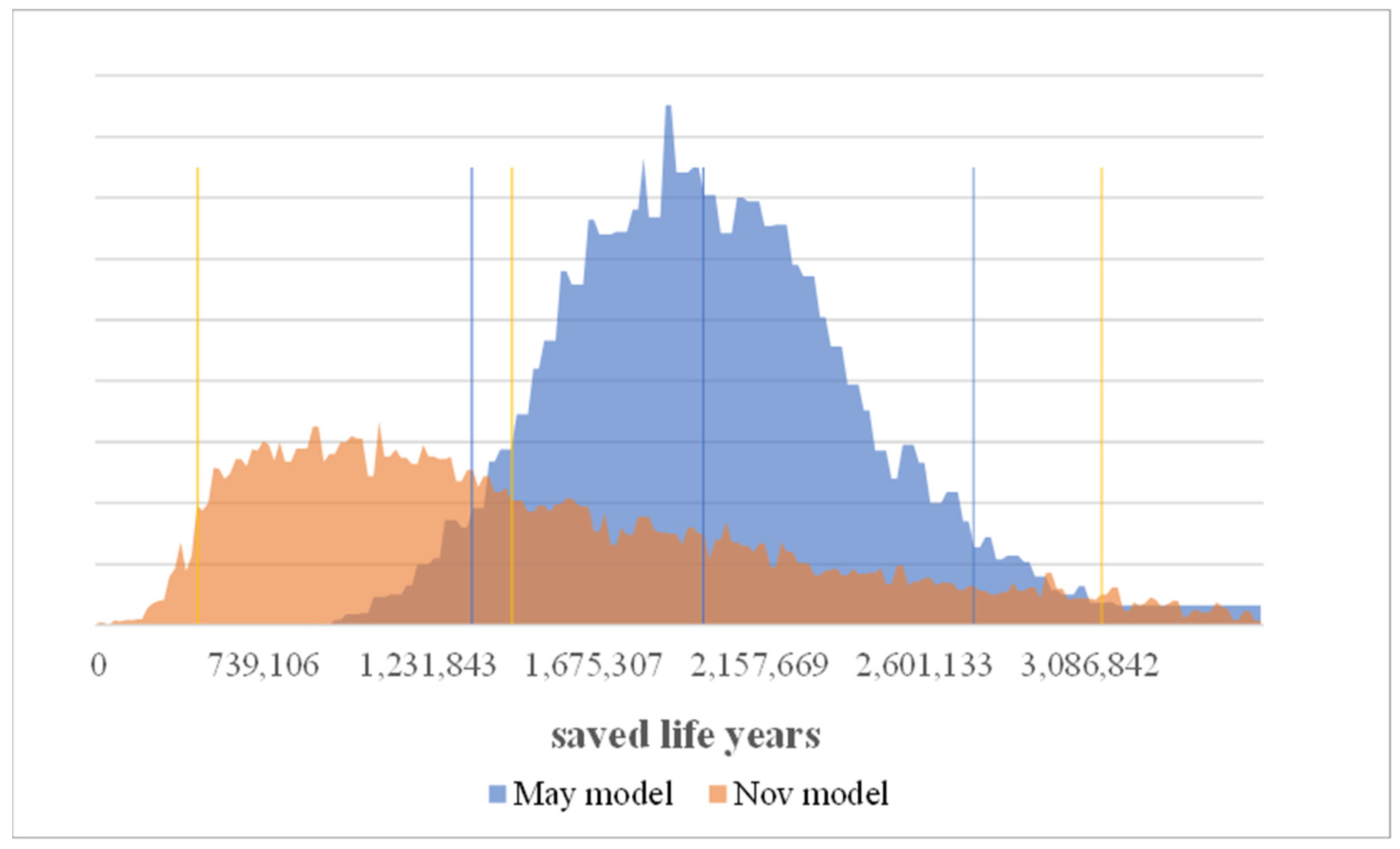
From the data and tables for the shares of the age groups in the previous death statistics, as well as from the expected life expectancy of the individual age groups, the number of deaths can be modeled, and the (sum of) lost years of life or lost years of work can be determined. RKI provided the following data as the known cases of illness by age group (see
Appendix A Table A9):
Table A9.
Known cases of illness by age group.
Table A9.
Known cases of illness by age group.
| Age Group | Infected | Share of Infected |
|---|
| | May | Nov. | May * | Nov. ** |
|---|
| 0–4 | 1224 | 14,591 | 0.82% | 1.90% |
| 5–14 | 3042 | 44,614 | 2.03% | 5.82% |
| 15–34 | 36,548 | 254,811 | 24.40% | 33.27% |
| 35–59 | 63,815 | 296,169 | 42.61% | 38,66% |
| 60–79 | 28,773 | 106,428 | 19.21% | 13.89% |
| 80+ | 16,357 | 49,378 | 10.92% | 6.45% |
| TOTAL | 149,759 | 765,991 | 100% | 100% |
During this period, however, the distribution of deaths was only achievable for a different structure (see
Appendix A Table A10).
Table A10.
Share of death by age group.
Table A10.
Share of death by age group.
| Age Group | Death | Share of Death * |
|---|
| | May | Nov. | May | Nov. |
|---|
| 0–59 | 226 | 566 | 4.44% | 4.92% |
| 60–69 | 457 | 1072 | 8.98% | 9.32% |
| 70–79 | 1197 | 2535 | 23.52% | 22.05% |
| 80–89 | 2308 | 5090 | 45.34% | 44.27% |
| 90+ | 902 | 2235 | 17.72% | 19.44% |
| TOTAL | 5090 | 11,498 | 100% | 100% |
By combining the two tables, assuming that the relative proportions would remain the same if the groups were further divided, the following proportions of age groups were used in terms of deceased and average remaining years of life (see
Appendix A Table A11):
Table A11.
Average remaining years by age group.
Table A11.
Average remaining years by age group.
| Age Group | Proportion of Deceased Patients * | Average Remaining Years ** (Both Models) |
|---|
| | May | Nov. | |
|---|
| 0–14 | 0.03% | 0.04% | 71.0 |
| 14–59 | 4.36% | 4.88% | 43.5 |
| 59–69 | 8.92% | 9.32% | 16.5 |
| 70–79 | 22.66% | 22.05% | 6.5 |
| 80–89 | 45.43% | 44.27% | 3 |
| 90+ | 18.60% | 19.44% | 3 |
At the beginning of April, there were still few data available from Germany. Therefore, we prepared the estimates based on worldwide studies and analyses. The case mortality (of known cases) was approximately 5.4%. We calculated based on data from Johns Hopkins University,
https://coronavirus.jhu.edu/ (accessed on 23 April 2020). These figures were also influenced in particular by the sharp increase in mortality rates in April and May based on the most recent data at the time). Since then, the mortality rate in relation to the number of infected persons has fallen continuously, both in Germany and in other countries, since the beginning of the pandemic. According to the RKI, case mortality (of known cases) was approximately 2.6%. According to the figures published by the RKI since then, a further decrease to approximately 1.7% leaves only approximately one-third of the April figure but is still approximately 15 times as high as for “normal” influenza. Mortality in relation to the number of infected persons is modeled—from the time of the start of the simulation—with the following bandwidths (see
Appendix A Table A12):
Table A12.
Mortality in relation to the number of infected persons.
Table A12.
Mortality in relation to the number of infected persons.
| Mortality | Min | Probable | Max |
|---|
| May | Nov. | May | Nov. | May | Nov. |
|---|
| Known cases | 4.9% | 1.4% | 5.4% | 1.7% | 6.0% | 2.0% |
| Unreported cases | 0.05% |





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}





