
Diabetic Mastopathy. Review of Diagnostic Methods and Therapeutic Options

 , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Etiology and Pathogenesis
3. Gross Pathology
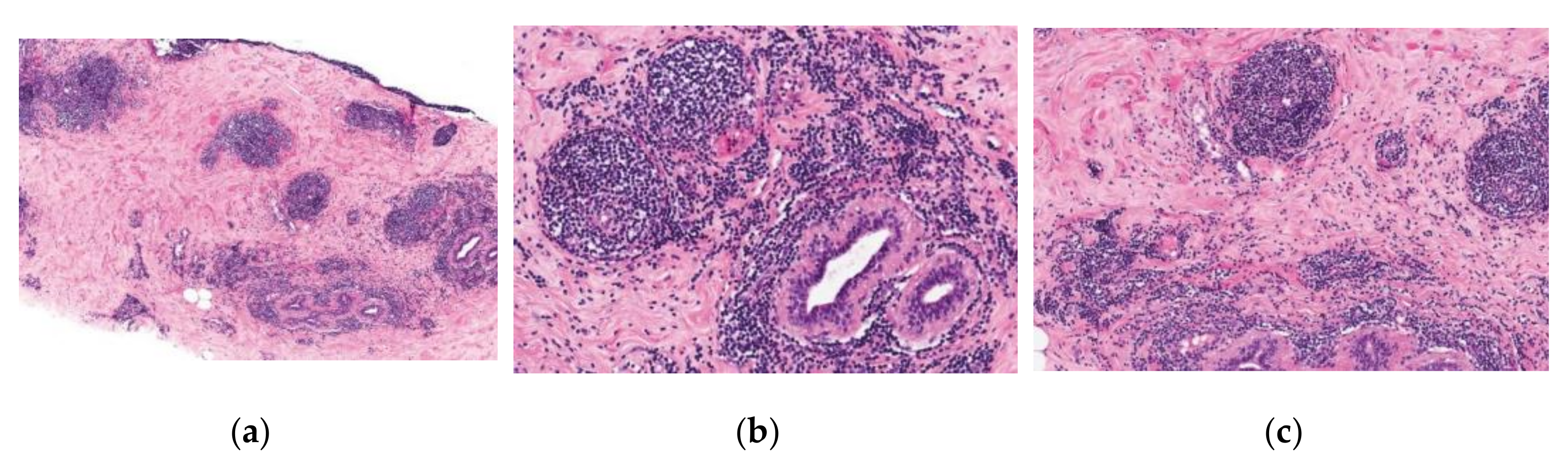
4. Microscopic Pathology
5. Clinical Picture, Diagnostic Criteria
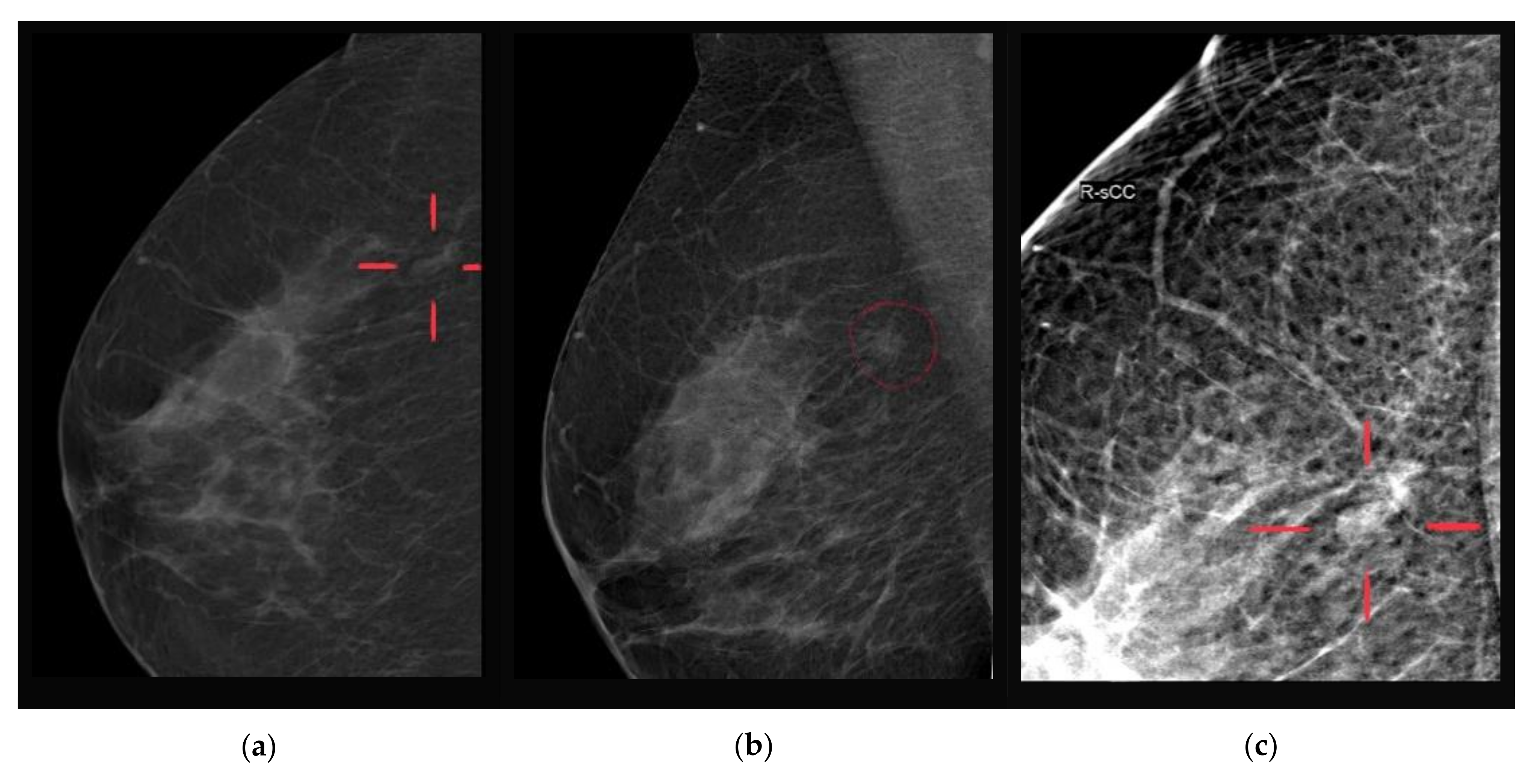
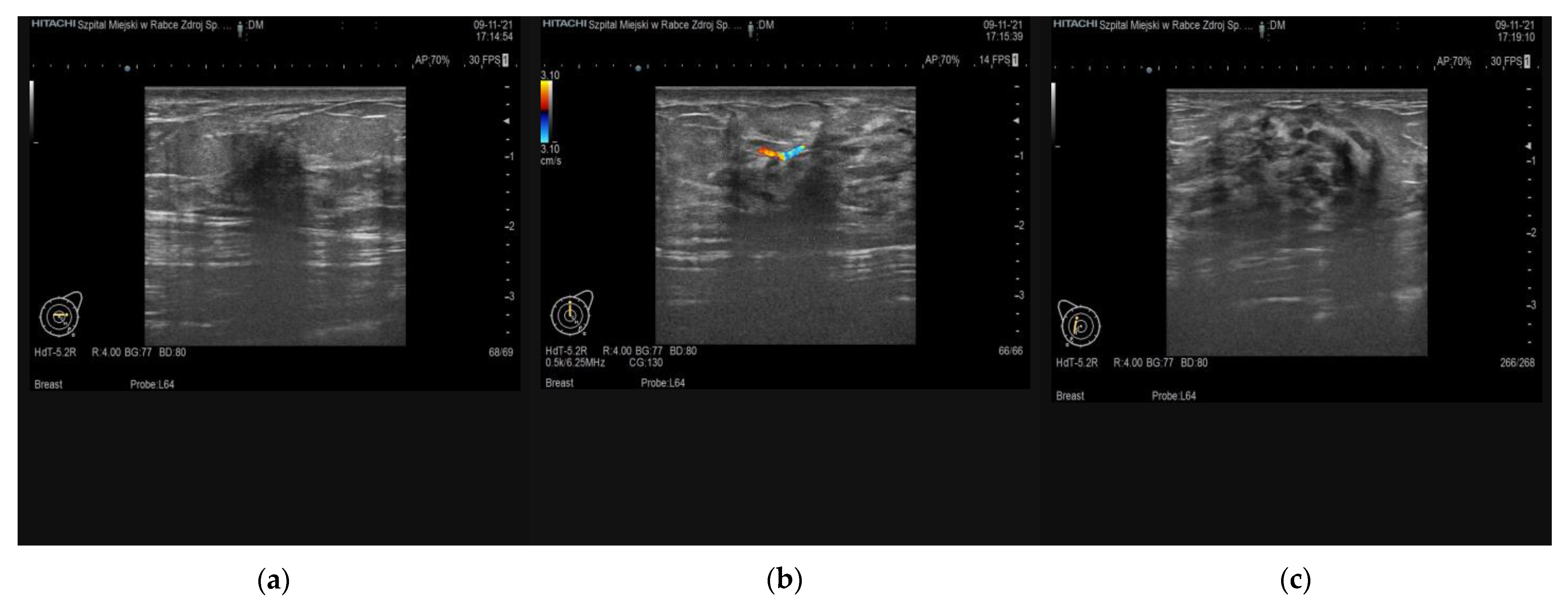
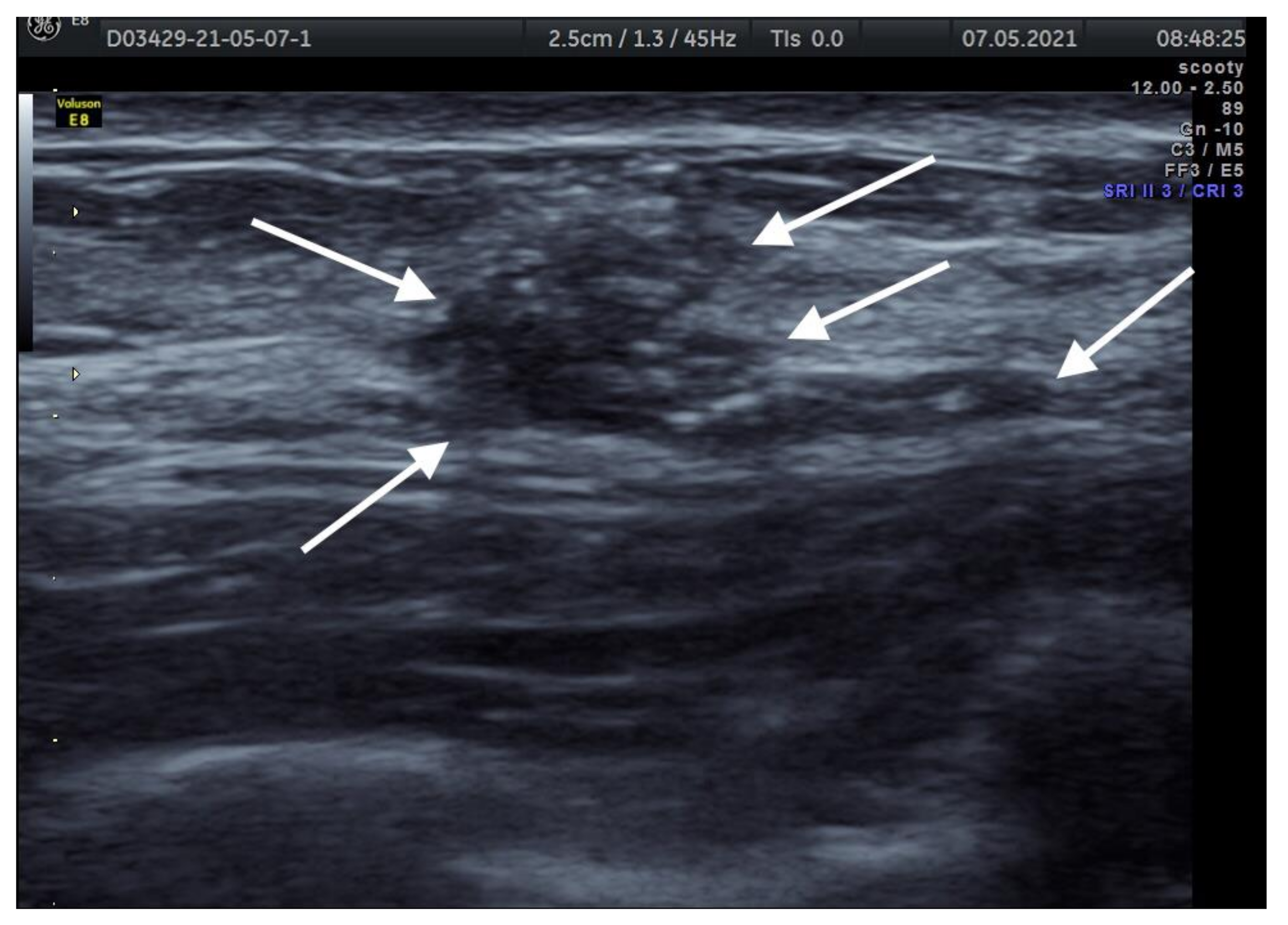
6. Imaging Findings
7. Prognosis and Treatment
8. Conclusions
9. Clinical Key Points
- DM is a rare condition occurring in patients with diabetes mellitus history (both types 1 and 2), may coexist with other diabetic complications such as retinopathy, neuropathy;
- The condition is benign, may affect one or both breasts, be localized in any breast quadrant, may be any size, typically no axillary adenopathy is found;
- Since the differential diagnosis of DM may be difficult, it is important to use multimodal imaging studies, i.e., sonography, mammography, and/or MRI DWI, to estimate the risk of malignant breast lesion;
- Core-needle biopsy and histopathological examination should be performed in all cases for the differential diagnosis;
- In histologically confirmed DM lesions that produce no symptoms conservative approach and observation may be offered to affected women;
- In symptomatic cases, surgery is a treatment of choice; however, the decision to operate and the type of operation (mastectomy with immediate reconstruction vs. lumpectomy) should be carefully planned; however, our experience shows as excisional treatments are barely needed;
- Approximately 30% of cases will recur, and performing wider excision margins may decrease the recurrence rate.
Author Contributions
Funding
Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
Case Presentation



References
- Agochukwu, N.B.; Wong, L. Diabetic Mastopathy: A Systematic Review of Surgical Management of a Rare Breast Disease. Ann. Plast. Surg. 2017, 78, 471–475. [Google Scholar] [CrossRef] [PubMed]
- Miura, K.; Teruya, C.; Hatsuko, N.; Ogura, H. Autoantibody with cross-reactivity between insulin and ductal cells may cause diabetic mastopathy: A case study. Case Rep. Med. 2012, 2012, 1–5. [Google Scholar] [CrossRef]
- Xiao, X.C.; Shi, -J.S.; Hua, W. Diabetic mastopathy in an elderly woman misdiagnosed as breast cancer: A case report and review of the literature. World J. Clin. Cases 2021, 9, 3458–3465. [Google Scholar]
- Lammie, G.A.; Bobrow, L.G.; Staunton, M.D.; Levison, D.A.; Page, G.; Millis, R.R. Sclerosing lymphocytic lobulitis of the breast--evidence for an autoimmune pathogenesis. Histopathology 1991, 19, 13–20. [Google Scholar] [CrossRef]
- Schwartz, I.S.; Strauchen, J.A. Lymphocytic mastopathy. An autoimmune disease of the breast? Am. J. Clin. Pathol. 1990, 93, 725–730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tomaszewski, J.E.; Brooks, J.S.; Hicks, D.; Livolsi, V.A. Diabetic mastopathy: A distinctive clinicopathologic entity. Hum. Pathol. 1992, 23, 780–786. [Google Scholar] [CrossRef]
- Seidman, J.D.; Schnaper, L.A.; Phillips, L.E. Mastopathy in insulin-requiring diabetes mellitus. Hum. Pathol. 1994, 25, 819–824. [Google Scholar] [CrossRef]
- Ely, K.A.; Tse, G.; Simpson, J.F.; Clarfeld, R.; Page, D.L. Diabetic mastopathy. A clinicopathologic review. Am. J. Clin. Pathol. 2000, 113, 541–545. [Google Scholar] [CrossRef]
- Paul, P.R. Rosen’s Breast Pathology, 2nd ed.; Lippincott Williams & Wilkins, Inc.: Philadelphia, PA, USA, 2001; pp. 55–56. [Google Scholar]
- David, G.; Hicks, M.D.; Susan, C. Diagnostic Pathology, Breast, 2nd ed.; Elsevier: Philadelphia, PA, USA, 2016; pp. 530–531. [Google Scholar]
- Chan, C.L.; Ho, R.S.; Shek, T.W.; Kwong, A. Diabetic mastopathy. Breast J. 2013, 19, 533–538. [Google Scholar] [CrossRef]
- Weinstein, S.P.; Conant, E.F.; Orel, S.G.; Lawton, T.J.; Acs, G. Diabetic mastopathy in men: Imaging findings in two patients. Radiology 2001, 219, 797–799. [Google Scholar] [CrossRef]
- Thorncroft, K.; Forsyth, L.; Desmond, S.; Audisio, R.A. The diagnosis and management of diabetic mastopathy. Breast J. 2007, 13, 607–613. [Google Scholar] [CrossRef]
- Rajasundaram, S.; Vijayakumar, V.; Chegu, D.; Uday Prasad, P.V.; Vimalathithan, S.N.; Saravanan, S.; Venkatesan, R. Diabetic mastopathy-An uncommon presentation of a common disease. Breast J. 2020, 26, 1409–1411. [Google Scholar] [CrossRef]
- Nasser, H.A.; Assaf, S.; Aouad, G.; Mouawad, Y.; Elamely, S. Breast manifestations of type I diabetes mellitus. Breast J. 2020, 26, 2079–2080. [Google Scholar] [CrossRef] [PubMed]
- Logan, W.W.; Hoffman, N.Y. Diabetic fibrous breast disease. Radiology 1989, 172, 667–670. [Google Scholar] [CrossRef]
- Camuto, P.M.; Zetrenne, E.; Ponn, T. Diabetic mastopathy: A report of 5 cases and a review of the literature. Arch. Surg. 2000, 135, 1190–1193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moschetta, M.; Telegrafo, M.; Triggiani, V.; Rella, L.; Cornacchia, I.; Serio, G.; Ianora, A.A.; Angelelli, G. Diabetic mastopathy: A diagnostic challenge in breast sonography. J. Clin. Ultrasound. 2015, 43, 113–117. [Google Scholar] [CrossRef]
- Tuncbilek, N.; Karakas, H.M.; Okten, O. Diabetic fibrous mastopathy: Dynamic contrast-enhanced magnetic resonance imaging findings. Breast J. 2004, 10, 359–362. [Google Scholar] [CrossRef] [PubMed]
- Nasu, H.; Ikeda, A.; Ogura, H.; Teruya, C.; Koizumi, K.; Kinoshita, M.; Tsuchida, T.; Baba, S.; Miura, K.; Takehara, Y.; et al. Two cases of diabetic mastopathy: MR imaging and pathological correlation. Breast Cancer 2015, 22, 552–556. [Google Scholar] [CrossRef]
- Guo, Y.; Cai, Y.Q.; Cai, Z.L.; Gao, Y.G.; An, N.Y.; Ma, L.; Mahankali, S.; Gao, J.H. Differentiation of clinically benign and malignant breast lesions using diffusion-weighted imaging. J. Magn. Reson. Imaging 2002, 16, 172–178. [Google Scholar] [CrossRef] [PubMed]
- Tsushima, Y.; Takahashi-Taketomi, A.; Endo, K. Magnetic resonance (MR) differential diagnosis of breast tumors using apparent diffusion coefficient (ADC) on 1.5-T. J. Magn. Reson. Imaging 2009, 30, 249–255. [Google Scholar] [CrossRef]
- Sankaye, S.; Kachewar, S. Diabetic mastopathy. Australas Med. J. 2012, 5, 296–299. [Google Scholar] [CrossRef]
- Radswiki, T.; Hacking, C. Diabetic Mastopathy. Reference Article, Radiopaedia.org. Available online: https://radiopaedia.org/articles/diabetic-mastopathy?lang=us (accessed on 11 November 2021).
- Andrews-Tang, D.; Diamond, A.B.; Rogers, L.; Butler, D. Diabetic Mastopathy: Adjunctive Use of Ultrasound and Utility of Core Biopsy in Diagnosis. Breast J. 2000, 6, 183–188. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Kim, E.K.; Kim, M.J.; Moon, H.J.; Yoon, J.H. Diabetic mastopathy: Imaging features and the role of image-guided biopsy in its diagnosis. Ultrasonography 2016, 35, 140–147. [Google Scholar] [CrossRef] [Green Version]
- Baratelli, G.M.; Riva, C. Diabetic fibrous mastopathy: Sonographic-pathologic correlation. J. Clin. Ultrasound. 2005, 33, 34–37. [Google Scholar] [CrossRef]
- Shrikrishnapalasuriyar, N.; Atkinson, M.; Kalhan, A.; Evans, P. Diabetic mastopathy: A diagnostic challenge. Br. J. Diabetes 2018, 18, 32–34. [Google Scholar] [CrossRef]
- Soler, N.G.; Khardori, R. Fibrous disease of the breast, thyroiditis, and cheiroarthropathy in type I diabetes mellitus. Lancet 1984, 28, 193–195. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guzik, P.; Gęca, T.; Topolewski, P.; Harpula, M.; Pirowski, W.; Koziełek, K.; Żmuda, M.; Śniadecki, M.; Góra, T.; Basta, P.; et al. Diabetic Mastopathy. Review of Diagnostic Methods and Therapeutic Options. Int. J. Environ. Res. Public Health 2022, 19, 448. https://doi.org/10.3390/ijerph19010448
Guzik P, Gęca T, Topolewski P, Harpula M, Pirowski W, Koziełek K, Żmuda M, Śniadecki M, Góra T, Basta P, et al. Diabetic Mastopathy. Review of Diagnostic Methods and Therapeutic Options. International Journal of Environmental Research and Public Health. 2022; 19(1):448. https://doi.org/10.3390/ijerph19010448
Chicago/Turabian StyleGuzik, Paweł, Tomasz Gęca, Paweł Topolewski, Magdalena Harpula, Wojciech Pirowski, Krzysztof Koziełek, Marcin Żmuda, Marcin Śniadecki, Tomasz Góra, Paweł Basta, and et al. 2022. "Diabetic Mastopathy. Review of Diagnostic Methods and Therapeutic Options" International Journal of Environmental Research and Public Health 19, no. 1: 448. https://doi.org/10.3390/ijerph19010448
APA StyleGuzik, P., Gęca, T., Topolewski, P., Harpula, M., Pirowski, W., Koziełek, K., Żmuda, M., Śniadecki, M., Góra, T., Basta, P., & Czekierdowski, A. (2022). Diabetic Mastopathy. Review of Diagnostic Methods and Therapeutic Options. International Journal of Environmental Research and Public Health, 19(1), 448. https://doi.org/10.3390/ijerph19010448