
Psychological Approaches for the Integrative Care of Chronic Low Back Pain: A Systematic Review and Metanalysis

 ,
,  ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion Criteria
2.2. Search Methods
- Population: the reference population included not hospitalized patients suffering from chronic low back pain. The patients included should be at least 18 years old, and they did not have to undergo surgery.
- Interventions: Selected psychological approaches
- Comparison Intervention: usual care, education program, supportive care, physical exercise, physiotherapy and waiting list
- Outcomes: pain, disability, fear-avoidance, anxiety and depression reduction and the improvement of quality of life
2.3. Data Collection, Analysis, and Outcomes
2.4. Risk of Bias Assessment
2.5. Statistical Analysis
3. Results
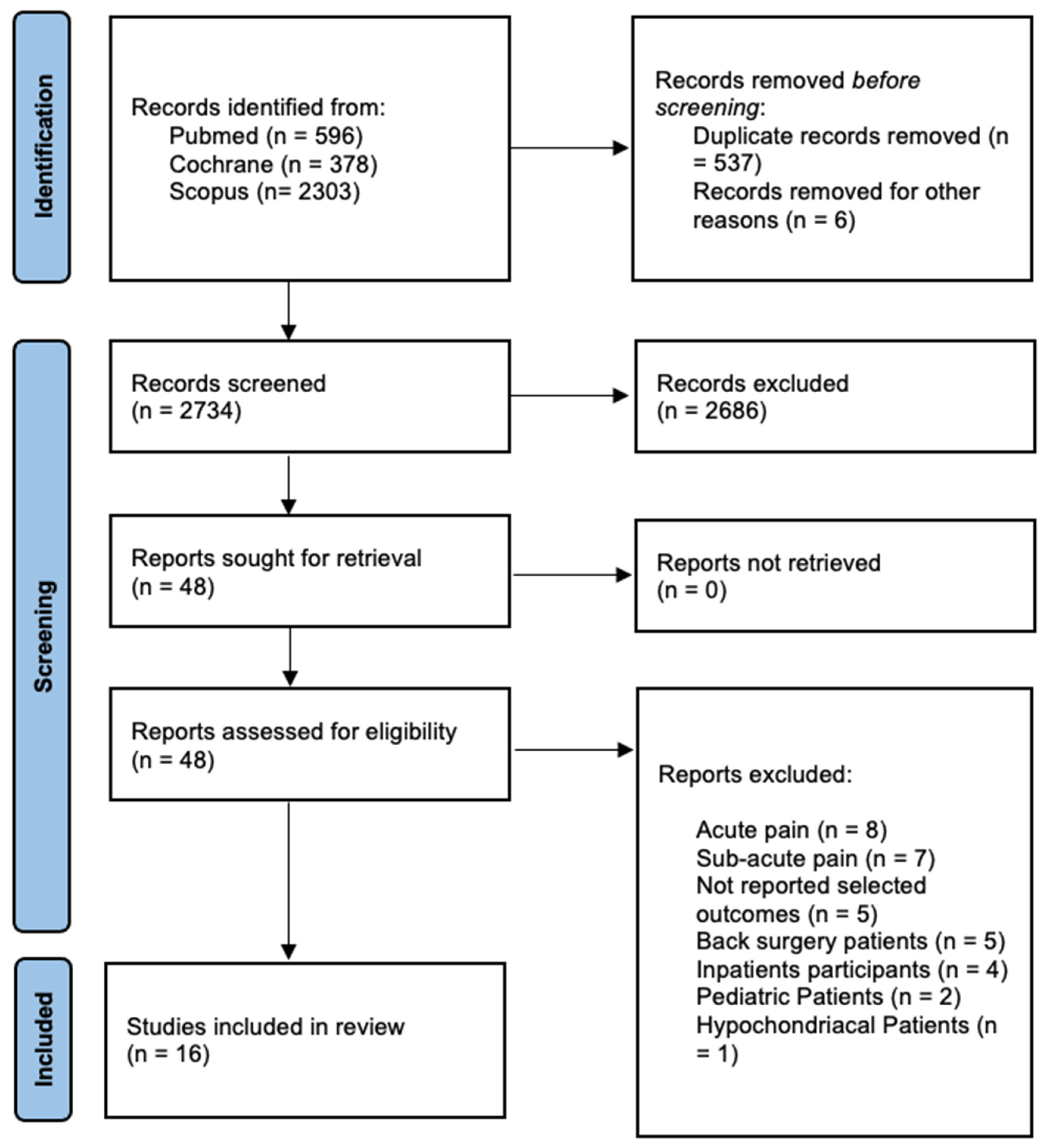
3.1. Results of the Literature Search
3.2. Demographic Data
3.3. Type of Interventions
3.4. Clinical Outcome Data
3.5. Methodological Evaluation
3.6. Effect of Intervention
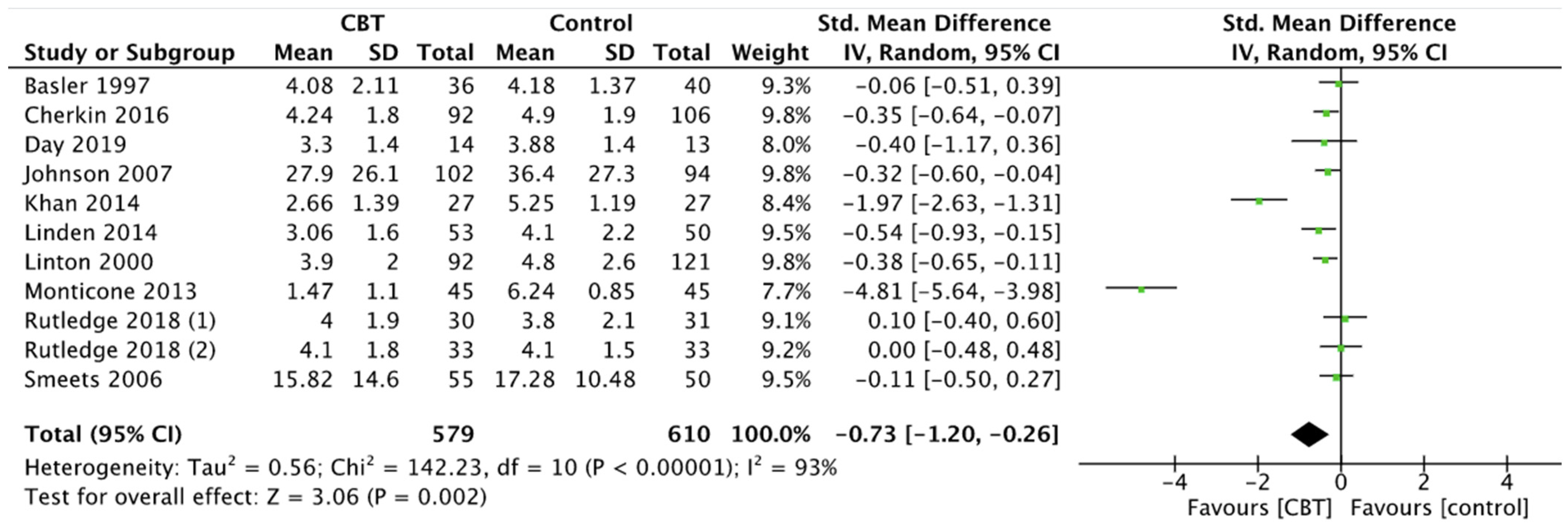
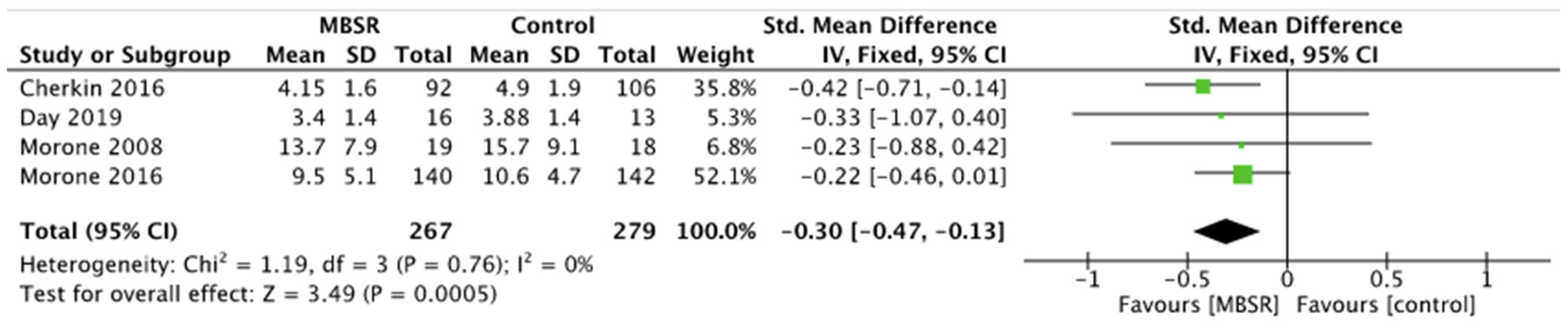
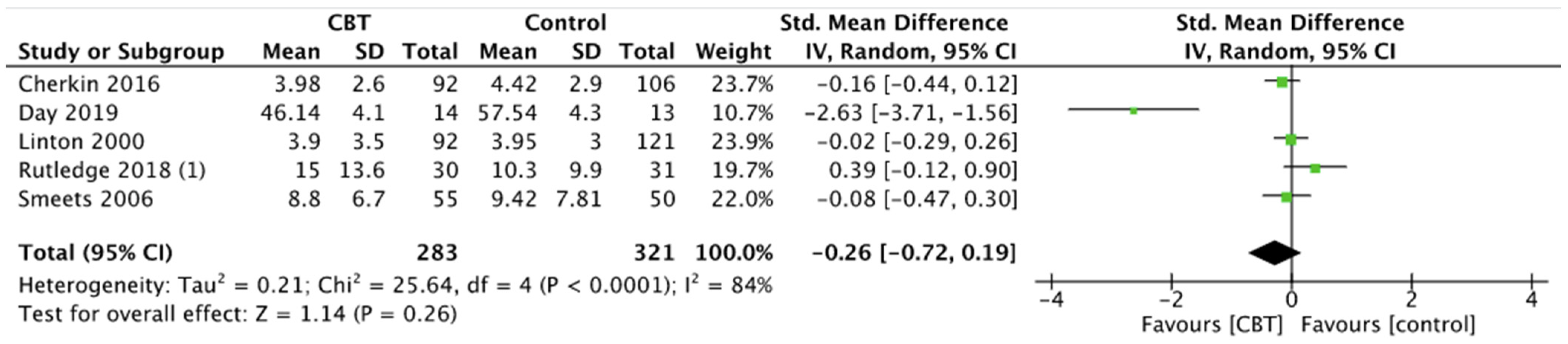
3.6.1. Pain
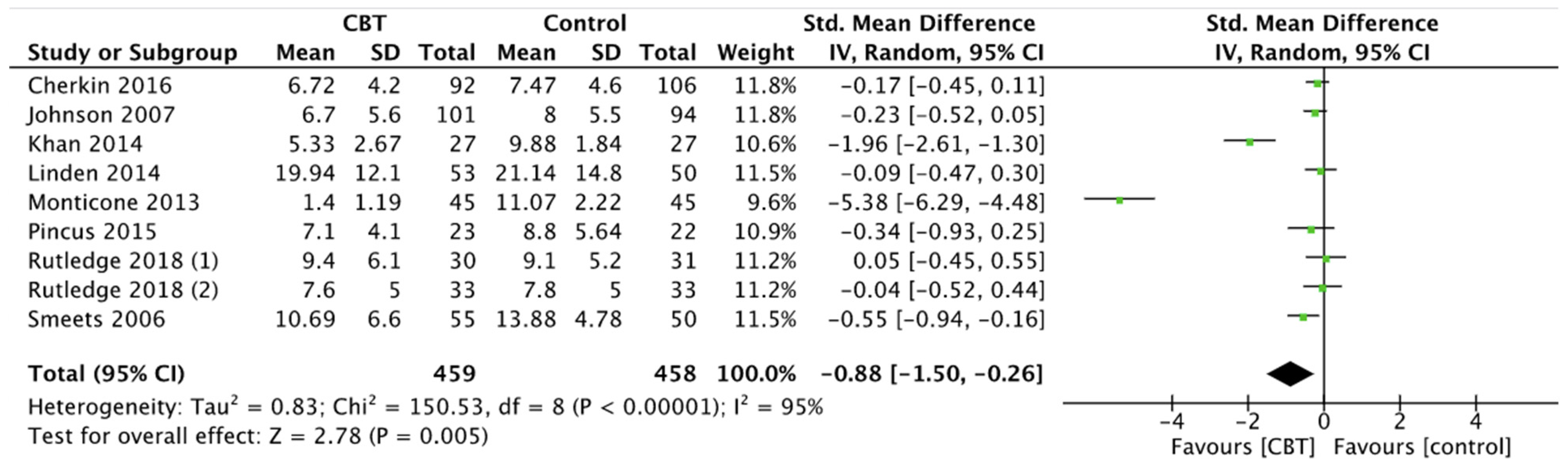
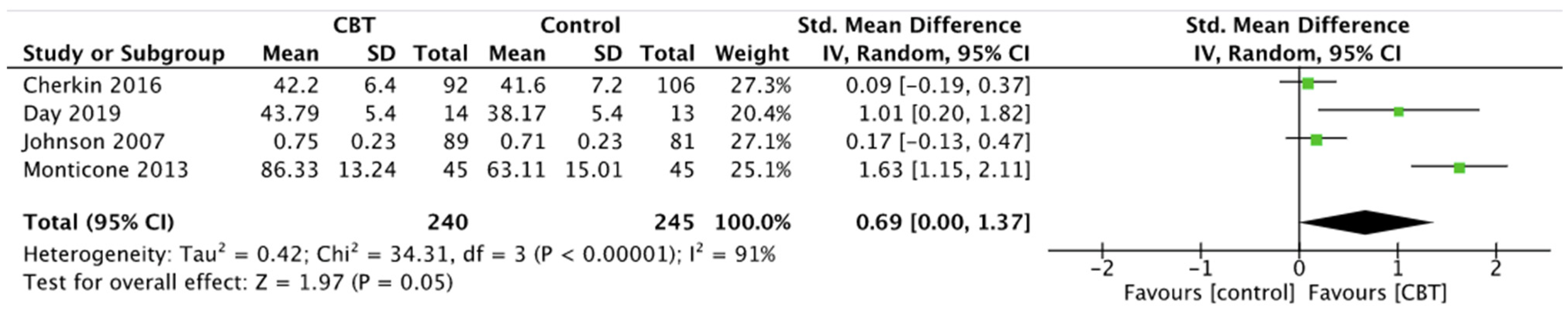
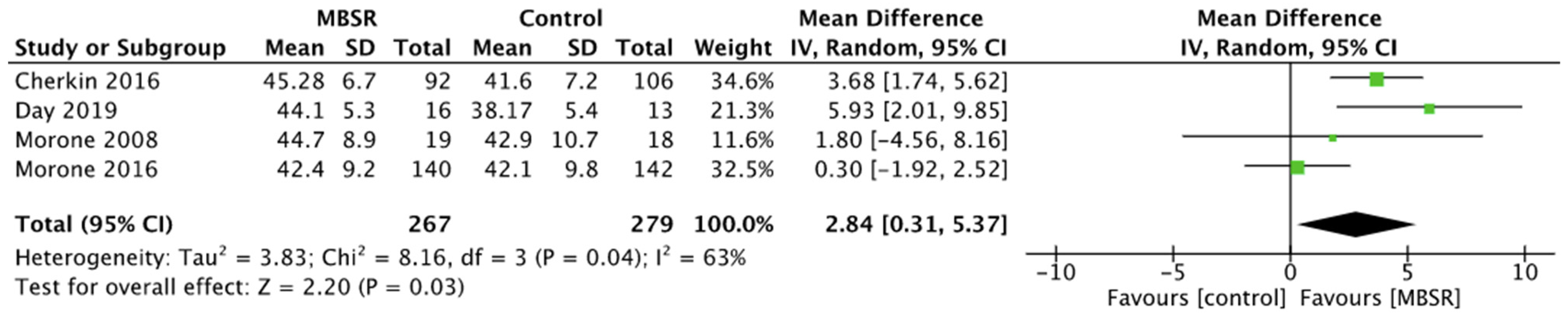
3.6.2. Disability
3.6.3. Quality of Life
3.6.4. Depression
3.6.5. Fear-Avoidance Beliefs
3.6.6. Days without Pain
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Vos, T.; Barber, R.M.; Bell, B.; Bertozzi-Villa, A.; Biryukov, S.; Bolliger, I.; Charlson, F.; Davis, A.; Degenhardt, L.; Dicker, D.; et al. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015, 386, 743–800. [Google Scholar] [CrossRef] [Green Version]
- Russo, F.; Papalia, G.F.; Vadalà, G.; Fontana, L.; Iavicoli, S.; Papalia, R.; Denaro, V. The Effects of Workplace Interventions on Low Back Pain in Workers: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public. Health 2021, 18, 12614. [Google Scholar] [CrossRef] [PubMed]
- Andersson, G.B. Epidemiological features of chronic low-back pain. Lancet 1999, 354, 581–585. [Google Scholar] [CrossRef]
- Deyo, R.A.; Mirza, S.K.; Martin, B.I. Back Pain Prevalence and Visit Rates: Estimates from U.S. National Surveys, 2002. Spine 2006, 31, 2724–2727. [Google Scholar] [CrossRef] [PubMed]
- Rubin, D.I. Epidemiology and Risk Factors for Spine Pain. Neurol. Clin. 2007, 25, 353–371. [Google Scholar] [CrossRef] [PubMed]
- Neugebauer, V.; Galhardo, V.; Maione, S.; Mackey, S. Forebrain pain mechanisms. Brain Res. Rev. 2009, 60, 226–242. [Google Scholar] [CrossRef] [Green Version]
- Williams, A.C.D.C.; Fisher, E.; Hearn, L.; Eccleston, C. Psychological therapies for the management of chronic pain (excluding headache) in adults. Cochrane Database Syst. Rev. 2020, 2021. [Google Scholar] [CrossRef]
- Russo, F.; Ambrosio, L.; Ngo, K.; Vadalà, G.; Denaro, V.; Fan, Y.; Sowa, G.; Kang, J.D.; Vo, N. The Role of Type I Diabetes in Intervertebral Disc Degeneration. Spine 2019, 44, 1177–1185. [Google Scholar] [CrossRef]
- Cherkin, D.C.; Sherman, K.J.; Balderson, B.H.; Cook, A.J.; Anderson, M.L.; Hawkes, R.J.; Hansen, K.E.; Turner, J.A. Effect of Mindfulness-Based Stress Reduction vs. Cognitive Behavioral Therapy or Usual Care on Back Pain and Functional Limitations in Adults With Chronic Low Back Pain: A Randomized Clinical Trial. JAMA 2016, 315, 1240. [Google Scholar] [CrossRef]
- Russo, F.; De Salvatore, S.; Ambrosio, L.; Vadalà, G.; Fontana, L.; Papalia, R.; Rantanen, J.; Iavicoli, S.; Denaro, V. Does Workers’ Compensation Status Affect Outcomes after Lumbar Spine Surgery? A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 6165. [Google Scholar] [CrossRef]
- Gatchel, R.J.; Peng, Y.B.; Peters, M.; Fuchs, P.; Turk, D.C. The biopsychosocial approach to chronic pain: Scientific advances and future directions. Psychol. Bull. 2007, 133, 581–624. [Google Scholar] [CrossRef]
- Keefe, F.J.; Rumble, M.E.; Scipio, C.D.; Giordano, L.A.; Perri, L.M. Psychological aspects of persistent pain: Current state of the science. J. Pain 2004, 5, 195–211. [Google Scholar] [CrossRef] [PubMed]
- Smeets, R.J.; Vlaeyen, J.; Kester, A.D.; Knottnerus, J.A. Reduction of Pain Catastrophizing Mediates the Outcome of Both Physical and Cognitive-Behavioral Treatment in Chronic Low Back Pain. J. Pain 2006, 7, 261–271. [Google Scholar] [CrossRef]
- Sullivan, M.J.L.; Thorn, B.; Haythornthwaite, J.A.; Keefe, F.; Martin, M.; Bradley, L.; Lefebvre, J.C. Theoretical Perspectives on the Relation Between Catastrophizing and Pain. Clin. J. Pain 2001, 17, 52–64. [Google Scholar] [CrossRef] [PubMed]
- Jarvik, J.G.; Hollingworth, W.; Heagerty, P.J.; Haynor, D.R.; Boyko, E.J.; Deyo, R.A. Three-Year Incidence of Low Back Pain in an Initially Asymptomatic Cohort: Clinical and Imaging Risk Factors. Spine 2005, 30, 1541–1548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hajihasani, A.; Rouhani, M.; Salavati, M.; Hedayati, R.; Kahlaee, A.H. The Influence of Cognitive Behavioral Therapy on Pain, Quality of Life, and Depression in Patients Receiving Physical Therapy for Chronic Low Back Pain: A Systematic Review. PM&R 2019, 11, 167–176. [Google Scholar] [CrossRef]
- Vadalà, G.; Russo, F.; De Salvatore, S.; Cortina, G.; Albo, E.; Papalia, R.; Denaro, V. Physical Activity for the Treatment of Chronic Low Back Pain in Elderly Patients: A Systematic Review. J. Clin. Med. 2020, 9, 1023. [Google Scholar] [CrossRef] [Green Version]
- Chou, R.; Loeser, J.D.; Owens, D.K.; Rosenquist, R.W.; Atlas, S.J.; Baisden, J.; Carragee, E.J.; Grabois, M.; Murphy, D.R.; Resnick, D.K.; et al. Interventional Therapies, Surgery, and Interdisciplinary Rehabilitation for Low Back Pain: An Evidence-Based Clinical Practice Guideline from the American Pain Society. Spine 2009, 34, 1066–1077. [Google Scholar] [CrossRef] [Green Version]
- Richmond, H.; Hall, A.M.; Copsey, B.; Hansen, Z.; Williamson, E.; Hoxey-Thomas, N.; Cooper, Z.; Lamb, S.E. The Effectiveness of Cognitive Behavioural Treatment for Non-Specific Low Back Pain: A Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0134192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoffman, B.M.; Papas, R.K.; Chatkoff, D.K.; Kerns, R.D. Meta-analysis of psychological interventions for chronic low back pain. Health Psychol. 2007, 26, 1–9. [Google Scholar] [CrossRef]
- Anheyer, D.; Haller, H.; Barth, J.; Lauche, R.; Dobos, G.; Cramer, H. Mindfulness-Based Stress Reduction for Treating Low Back Pain: A Systematic Review and Meta-Analysis. Ann. Intern. Med. 2017, 166, 799. [Google Scholar] [CrossRef]
- Gotink, R.A.; Chu, P.; Busschbach, J.J.V.; Benson, H.; Fricchione, G.L.; Hunink, M.G.M. Standardised Mindfulness-Based Interventions in Healthcare: An Overview of Systematic Reviews and Meta-Analyses of RCTs. PLoS ONE 2015, 10, e0124344. [Google Scholar] [CrossRef]
- Page, M.J.; Moher, D. Evaluations of the uptake and impact of the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) Statement and extensions: A scoping review. Syst. Rev. 2017, 6, 263. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morone, N.E.; Greco, C.M.; Weiner, D.K. Mindfulness meditation for the treatment of chronic low back pain in older adults: A randomized controlled pilot study. Pain 2008, 134, 310–319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morone, N.E.; Rollman, B.L.; Moore, C.G.; Li, Q.; Weiner, D.K. A Mind–Body Program for Older Adults with Chronic Low Back Pain: Results of a Pilot Study. Pain Med. 2009, 10, 1395–1407. [Google Scholar] [CrossRef] [Green Version]
- Morone, N.E.; Greco, C.M.; Moore, C.G.; Rollman, B.L.; Lane, B.; Morrow, L.A.; Glynn, N.W.; Weiner, D.K. A Mind-Body Program for Older Adults with Chronic Low Back Pain: A Randomized Clinical Trial. JAMA Intern. Med. 2016, 176, 329. [Google Scholar] [CrossRef]
- Day, M.A.; Ward, L.C.; Ehde, D.M.; Thorn, B.E.; Burns, J.; Barnier, A.; Mattingley, J.B.; Jensen, M.P. A Pilot Randomized Controlled Trial Comparing Mindfulness Meditation, Cognitive Therapy, and Mindfulness-Based Cognitive Therapy for Chronic Low Back Pain. Pain Med. 2019, 20, 2134–2148. [Google Scholar] [CrossRef] [Green Version]
- Monticone, M.; Ferrante, S.; Rocca, B.; Baiardi, P.; Farra, F.D.; Foti, C. Effect of a Long-Lasting Multidisciplinary Program on Disability and Fear-Avoidance Behaviors in Patients With Chronic Low Back Pain: Results of a Randomized Controlled Trial. Clin. J. Pain 2013, 29, 929–938. [Google Scholar] [CrossRef]
- Rutledge, T.; Atkinson, J.H.; Chircop-Rollick, T.; D’Andrea, J.; Garfin, S.; Patel, S.; Penzien, D.B.; Wallace, M.; Weickgenant, A.L.; Slater, M. Randomized Controlled Trial of Telephone-delivered Cognitive Behavioral Therapy Versus Supportive Care for Chronic Back Pain. Clin. J. Pain 2018, 34, 322–327. [Google Scholar] [CrossRef]
- Rutledge, T.; Atkinson, J.H.; Holloway, R.; Chircop-Rollick, T.; D’Andrea, J.; Garfin, S.R.; Patel, S.; Penzien, D.B.; Wallace, M.; Weickgenant, A.L.; et al. Randomized Controlled Trial of Nurse-Delivered Cognitive-Behavioral Therapy Versus Supportive Psychotherapy Telehealth Interventions for Chronic Back Pain. J. Pain 2018, 19, 1033–1039. [Google Scholar] [CrossRef] [PubMed]
- Johnson, R.E.; Jones, G.T.; Wiles, N.J.; Chaddock, C.; Potter, R.G.; Roberts, C.; Symmons, D.P.M.; Watson, P.J.; Torgerson, D.J.; Macfarlane, G.J. Active Exercise, Education, and Cognitive Behavioral Therapy for Persistent Disabling Low Back Pain: A Randomized Controlled Trial. Spine 2007, 32, 1578–1585. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.; Akhter, S.; Soomro, R.R.; Ali, S.S. The effectiveness of Cognitive Behavioral Therapy (CBT) with general exercises versus general exercises alone in the management of chronic low back pain. Pak. J. Pharm. Sci. 2014, 27, 1113–1116. [Google Scholar] [PubMed]
- Pincus, T.; Anwar, S.; McCracken, L.M.; McGregor, A.; Graham, L.; Collinson, M.; McBeth, J.; Watson, P.; Morley, S.; on behalf of the OBI Trial Management Team; et al. Delivering an Optimised Behavioural Intervention (OBI) to People with Low Back Pain with High Psychological Risk; Results and Lessons Learnt from a Feasibility Randomised Controlled Trial of Contextual Cognitive Behavioural Therapy (CCBT) vs. Physiotherapy. BMC Musculoskelet. Disord. 2015, 16, 147. [Google Scholar] [CrossRef] [PubMed]
- Zgierska, A.E.; Burzinski, C.A.; Cox, J.; Kloke, J.; Stegner, A.; Cook, D.B.; Singles, J.; Mirgain, S.; Coe, C.L.; Bačkonja, M. Mindfulness Meditation and Cognitive Behavioral Therapy Intervention Reduces Pain Severity and Sensitivity in Opioid-Treated Chronic Low Back Pain: Pilot Findings from a Randomized Controlled Trial. Pain Med. 2016, 17, 1865–1881. [Google Scholar] [CrossRef] [PubMed]
- Linden, M.; Scherbe, S.; Cicholas, B. Randomized controlled trial on the effectiveness of cognitive behavior group therapy in chronic back pain patients. J. Back Musculoskelet. Rehabil. 2014, 27, 563–568. [Google Scholar] [CrossRef] [PubMed]
- Basler, H.-D.; Jäkle, C.; Kröner-Herwig, B. Incorporation of cognitive-behavioral treatment into the medical care of chronic low back patients: A controlled randomized study in German pain treatment centers. Patient Educ. Couns. 1997, 31, 113–124. [Google Scholar] [CrossRef]
- Linton, S.J.; Andersson, T. Can Chronic Disability Be Prevented?: A Randomized Trial of a Cognitive-Behavior Intervention and Two Forms of Information for Patients With Spinal Pain. Spine 2000, 25, 2825–2831. [Google Scholar] [CrossRef]
- Murphy, J.L.; Cordova, M.J.; Dedert, E.A. Cognitive behavioral therapy for chronic pain in veterans: Evidence for clinical effectiveness in a model program. Psychol. Serv. 2020. [Google Scholar] [CrossRef]
- Proulx, K. Integrating Mindfulness-Based Stress Reduction. Holist. Nurs. Pract. 2003, 17, 201–208. [Google Scholar] [CrossRef]
- Majeed, M.H.; Ali, A.A.; Sudak, D.M. Mindfulness-based interventions for chronic pain: Evidence and applications. Asian J. Psychiatry 2018, 32, 79–83. [Google Scholar] [CrossRef] [PubMed]
- Morley, S.; Eccleston, C.; Williams, A. Systematic review and meta-analysis of randomized controlled trials of cognitive behaviour therapy and behaviour therapy for chronic pain in adults, excluding headache. Pain 1999, 80, 1–13. [Google Scholar] [CrossRef]
- Hartvigsen, J.; Hancock, M.; Kongsted, A.; Louw, Q.; Ferreira, M.L.; Genevay, S.; Hoy, D.; Karppinen, J.; Pransky, G.; Sieper, J.; et al. What low back pain is and why we need to pay attention. Lancet 2018, 391, 2356–2367. [Google Scholar] [CrossRef] [Green Version]
- Wertli, M.M.; Eugster, R.; Held, U.; Steurer, J.; Kofmehl, R.; Weiser, S. Catastrophizing—a prognostic factor for outcome in patients with low back pain: A systematic review. Spine J. 2014, 14, 2639–2657. [Google Scholar] [CrossRef] [PubMed]
- Pinheiro, M.B.; Ferreira, M.L.; Refshauge, K.; Maher, C.; Ordoñana, J.R.; Andrade, T.B.; Tsathas, A.; Ferreira, P. Symptoms of depression as a prognostic factor for low back pain: A systematic review. Spine J. 2016, 16, 105–116. [Google Scholar] [CrossRef] [PubMed]
- Crofford, L.J. Psychological aspects of chronic musculoskeletal pain. Best Pract. Res. Clin. Rheumatol. 2015, 29, 147–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tagliaferri, S.D.; Miller, C.T.; Owen, P.J.; Mitchell, U.H.; Brisby, H.; FitzGibbon, B.; Masse-Alarie, H.; Van Oosterwijck, J.; Belavy, D.L. Domains of Chronic Low Back Pain and Assessing Treatment Effectiveness: A Clinical Perspective. Pain Pract. 2020, 20, 211–225. [Google Scholar] [CrossRef]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Year | Country | Study Group | Control Group | ||||
|---|---|---|---|---|---|---|---|---|
| N. | Age | Sex | N. | Age (Years) | Sex | |||
| Cherkin et al. | 2016 | USA | 116 | 50 ± 11.9 | 71% F 29% M | 113 | 48.9 ± 12.5 | 87% F 13% M |
| 112 | 49.1 ± 12.6 | 66% F 34% M | ||||||
| Monticone et al. | 2013 | Italy | 45 | 49 ± 8 | 60% F 40% M | 45 | 49.7 ± 7 | 55% F 45% M |
| Johnson et al. | 2007 | UK | 116 | 47.3 ± 10.9 | 61% F 39% M | 118 | 48.5 ± 11.4 | 58% F 42% M |
| Smeets et al. | 2006 | The Netherlands | 58 | 42.5 ± 9.7 | 58.6% F 41.4% M | 53 | 42.7 ± 9.1 | 41.5% F 58.5% M |
| 61 | 40.7 ± 10.1 | 37.7% F 62.3% M | 51 | 40.5 ± 11.2 | 37.3% F 62.7% M | |||
| Rutledge et al. | 2018 | USA | 30 | 62.5 ± 11.3 | 13% F 87% M | 31 | 64.3 ± 12.7 | 6% F 92% M |
| Rutledge et al. | 2018 | USA | 33 | 54 ± 14.8 | 37.5% F 62.5% M | 33 | 52.6 ± 12.5 | 39.4% F 60.6% M |
| Linden et al. | 2014 | Germany | 53 | 50.4 ± 6.9 | 68% F 32% M | 50 | 49.7 ± 7 | 68% F 32% M |
| Khan et al. | 2016 | Pakistan | 27 | 39.61 ± 5.3 | 54% F 46% M | 27 | 39.61 ± 5.3 | 54% F 46% M |
| Pincus et al. | 2015 | UK | 45 | 43.7 ± 16.3 | 60% F 40% M | 44 | 45.4 ± 15.8 | 38.6% F 61.4% M |
| Basler et al. | 1997 | Germany | 36 | 49.3 ± 9.7 | 75.6% F 24.4% M | 40 | 49.3 ± 9.7 | 75.6% F 24.4%M |
| Linton et al. | 2000 | Sweden | 107 | 44 | 70% F 30% M | 70 | 45 | 71% F 29% M |
| 66 | 44 | 74% F 26% M | ||||||
| Zgierska et al. | 2016 | USA | 21 | 51.8 ± 9.7 | 80% F 20% M | 14 | 51.8 ± 9.7 | 80% F 20% M |
| Morone et al. | .2008 | USA | 19 | 74.1 ± 6.1 | 53% F 47% M | 18 | 75.6 ± 5 | 61% F 39% M |
| Morone et al. | 2009 | USA | 16 | 78 ± 7.1 | 69% F 31% M | 19 | 73 ± 6.2 | 58% F 42% M |
| Morone et al. | 2016 | USA | 140 | 75 ± 7.2 | 66% F 34% M | 142 | 74 ± 6.0 | 66% F 34% M |
| Day et al. | 2019 | USA | 23 | 49.9 ± 11.9 | 61% F 39% M | 23 | 48.1 ± 16.1 | 52% F 48% M |
| 23 | 54.3 ± 14.9 | 44% F 56% M | ||||||
| Study | Intervention (s) | Control | Follow-Up | Outcomes (Tool) | Conclusion |
|---|---|---|---|---|---|
| Cherkin et al., 2016 | Mindfulness: body scan, yoga, meditation, for 8 weeks. CBT: education about chronic pain, relationships between thoughts and emotional and physical reactions, sleep hygiene, setting and working toward behavioral goals, relaxation skills, activity pacing, and pain-coping strategies, for 8 weeks | Usual care (whatever care participants received) | 12 months | Disability (RMDQ) QoL (SF-12) Depression (PHQ-8) Anxiety (GAD-2) | Among adults with CLBP, treatment with MBSR or CBT, compared with usual care, resulted in greater improvement in back pain and functional limitations at 26 weeks, with no significant differences in outcomes between MBSR and CBT |
| Monticone et al., 2013 | CBT: intervention to modify fear of movement beliefs, catastrophizing thinking, and negative feelings, and ensuring gradual reactions to illness behaviors, for 5 weeks | Active and passive mobilizations of the spine, and exercises aimed at stretching and strengthening muscles, and improving postural control, for 5 weeks | 12 months | Disability (RMDQ) Pain (NRS) QOL (SF-36) Fear advoidance behaviours (TSK) | The long-lasting multidisciplinary program was superior to the exercise program in reducing disability, fear- avoidance beliefs and pain, and enhancing the quality of life of patients with chronic low back pain. The effects were clinically tangible and lasted for at least 1 year after the intervention ended. |
| Johnson et al., 2007 | CBT: educational pack containing a booklet and audio-cassette + problem solving, pacing and regulation of activity, challenging distorted cognitions about activity and harm, for 6 week | Educational pack containing a booklet and audio-cassette + usual care for 6 weeks | 15 months | Pain (VAS) Disability (RMDQ) QoL (EQ-5D) | CBT intervention program produces only modest effects in reducing LBP and disability over a 1-year period. |
| Smeets et al., 2006 | CBT: operant behavioral graded activity training and problem solving training Active Physical Treatment (APT): aerobic training, and three dynamic static strengthening exercises for 4 weeks Combined Treatment (CT): CBT + APT | Waiting List (WL) for 10 weeks | 12 months | Disability (RMDQ) Pain (VAS) Depression (BDI) | CBT are as effective in reducing the subjective experienced level of functioning |
| Rutledge et al., 2018 | CBT: to provide core educational information, guide patients’ learning and skills development, and structure self-monitoring exercises for the respective session, for 8 weeks | Supportive Care: - Education by distribution of a standard text - Active Listening by the therapist to participant’s concerns - Supportive care following Rogerian principles | 12 months | Disability (RMDQ) Pain (NRS) Depression (BDI) | No evidence of meaningful effect size differences between the treatments. |
| Rutledgeet al., 2018 | CBT: managing pain, managing stress, thinking differently, assertive communication, setting goals for 8 weeks | Supportive Care: - Education by distribution of a standard text - Active Listening by the therapist to participant’s concerns - Supportive care following Rogerian principles | 12 months | Disability (RMDQ) Pain (NRS) | CBT versus SC therapy demonstrated statistically significant and comparable patterns of improved outcomes on measures of back pain disability, pain severity, and self- rated improvement. |
| Linden et al., 2014 | general orthopedic inpatient treatment + therapy in reference to the GRIP and the pain and illness management program from Geissner at al. with additional cognitive behavior therapy interventions which aim at stress reduction and problem solving, self monitoring, pain management, change in dysfunctional cognitions, reduction of avoidance behavior, and wellbeing therapy for 3 weeks | General orthopedic inpatient treatment | 3 weeks | Fear advoidance behaviours (FABQ) Pain (VAS) Pain related disability (PDI) | CBT can reduce back pain and increase functional coping, and that this is not mediated by an improvement in mental health and a reduction of depression, anxiety or somatization in general or by induc- tion of some general optimistic views. Pain is not identical with mental problems. |
| Khan et al., 2016 | general exercise + CBT aimed to guide patients to achieve their daily life goals. CBT consisted of operant behavioural graded activity and problem solving training, for 12 weeks | General exercise at home 2 times per day and at least 5 times a week (for 12 weeks) | 12 weeks | Disability (RMDQ) Pain (VAS) | This study found that both CBT with General exercises and General exercises alone significantly reduced pain intensity and disability in patients with chronic low back pain. Furthermore, subjects treated with CBT & Exercises showed an additional clinical benefit as compared to General Exercises only. Hence, CBT & Exercises could be a better option in clinical practice. |
| Pincus et al., 2015 | Session content was not structured, and at the discretion of therapists, included any features of Contextual Cognitive-Behavioural Therapy (CCBT) they thought were appropriate at the point with that patient. | Physiotherapy, comprised back to fitness group exercises with at least 60% of content exercise-based. | 3 months | Fear advoidance behaviours (TSK) pain (Brief Pain Inventory) disability (RMDQ) anxiety and depression (HADS) QoL (EQ-5D and SF-36) | CCBT is a credible and acceptable intervention for LBP patients who exhibit psychological obstacles to recovery. |
| Basler et al., 1997 | medical treatment such as pain medication, nerve blocks, TENS, and physical therapy + CBT therapy: education, relaxation, Modifying thoughts and feelings, Pleasant activity scheduling, Training of posture | Medical treatment such as pain medication, nerve blocks, TENS, and physical therapy | 6 months | Pain (NRS) Disability (Dusseldorf disability scale) | Experimental subjects reported less pain, more pleasurable activities and feelings, less avoidance and less catastrophizing, and disability was reduced. The results were maintained at follow-up. Patients who only received medical treatment showed little improvement. Data indicate that the program meets the needs of the patients and should be continued. |
| Linton et al., 2007 | Sessions were organized to activate participants and promote coping. Each session began with a short review, in which homework was covered. The treatment lasts 6 weeks | 1. pamphlet: straightforward advice about the best way to cope with back pain by remaining active and thinking positively. 2. Information package: advice and illustrations showing how the patient might cope with spinal pain or prevent it by such methods as lifting properly and main- taining good posture. | 12 months | Pain (VAS) Depression and anxiety (HAD) Fear Advoidance (FABQ) | This study demonstrates that CBT group intervention can lower the risk of a long-term disability developing. |
| Zgierska et al., 2016 | Usual care and opioid therapy management + manualized training in the meditation-CBT intervention 2 h per week for 8 weeks | Pharmacotherapy, opioid therapy management and physical therapy | 26 weeks | Pain (Brief Pain Inventory) Disability (ODI) | Mindfulness meditation and CBT-based interventions have the potential to safely reduce pain severity and sensitivity in patients with opioid-treated CLBP |
| Morone et al., 2008 | Mindfulness: body scan, sitting practice, walking meditation | Waiting List | 3 months | Pain (McGill pain Questionnaire- Short Form and SF-36 pain scale) Disability (RMDQ) QoL (SF-36) | The mindfulness intervention sustained improvement in physical function and pain acceptance. |
| Morone et al., 2009 | Mindfulness: body scan, sitting practice, walking meditation | Educational program (8 weeks), including lectures, group discussion, and homework assignments based on the health topics discussed | 4 months | Disability (RMDQ) Pain (McGill pain Questionnaire- Short Form and SF-36 pain scale) QoL (SF-36) | A mindfulness meditation program and an education control group both showed improvement at program completion on measures of pain, and physical and psychological function. |
| Morone et al., 2016 | Mindfulness: body scan, sitting practice, walking meditation for 8 weeks | Educational program on a successful aging curriculum known as the 10 Keys to Healthy Aging | 6 months | Disability (RMDQ) Pain (NRS) QoL (SF-36) | A mind-body program for chronic LBP improved short-term function and long-term current and most severe pain. The functional improvement was not sustained. |
| Day et al., 2019 | MBCT for pain protocol integrates cognitive and be- havioral techniques with mindfulness-based strategies | CT techniques delivered: treatment involved traditional Beckian style column technique restructuring exercises Mindufulness: cognitive-behavioral and mindful movement components removed | 6 months | Pain (NRS) Physical function (PROMIS) Depression (PROMIS) | The findings show that MBCT is a feasible, tolerable, acceptable, and potentially efficacious treatment option for CLBP. Further, MBCT, and possibly CT, could have sus- tained benefits that exceed MM on some important CLBP outcomes. |
| Random Sequence Generation | Allocation Concealment | Blinding (Participants and Personnel) | Blinding (Outcome Assessment) | Incomplete Outcome Data | Selective Reporting | Other Bias | Risk of Bias | |
|---|---|---|---|---|---|---|---|---|
| Cherkin et al., 2016 | L | L | H | L | L | L | H | U |
| Monticone et al., 2013 | L | L | H | L | L | L | L | L |
| Johnson et al., 2007 | L | L | H | H | L | L | H | U |
| Smeets et al., 2006 | L | L | H | L | L | L | H | U |
| Rutledge et al., 2018 | L | L | H | L | L | L | H | U |
| Rutledge T et al., 2018 | L | L | H | H | L | L | L | U |
| Linden et al., 2014 | L | U | H | L | L | L | H | U |
| Khan et al., 2016 | L | U | H | L | L | L | H | U |
| Pincus et al., 2015 | L | L | H | U | L | L | H | U |
| Basler et al., 1997 | L | L | H | L | L | L | H | U |
| Linton et al., 2000 | L | U | H | U | L | L | H | H |
| Zgierska et al., 2016 | L | U | H | H | L | L | H | H |
| Morone et al., 2008 | L | U | U | H | L | L | H | H |
| Morone et al., 2009 | L | L | U | L | H | L | L | L |
| Morone et al., 2016 | L | L | U | L | L | U | L | L |
| Day et al., 2019 | L | L | H | L | L | L | L | L |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Petrucci, G.; Papalia, G.F.; Russo, F.; Vadalà, G.; Piredda, M.; De Marinis, M.G.; Papalia, R.; Denaro, V. Psychological Approaches for the Integrative Care of Chronic Low Back Pain: A Systematic Review and Metanalysis. Int. J. Environ. Res. Public Health 2022, 19, 60. https://doi.org/10.3390/ijerph19010060
Petrucci G, Papalia GF, Russo F, Vadalà G, Piredda M, De Marinis MG, Papalia R, Denaro V. Psychological Approaches for the Integrative Care of Chronic Low Back Pain: A Systematic Review and Metanalysis. International Journal of Environmental Research and Public Health. 2022; 19(1):60. https://doi.org/10.3390/ijerph19010060
Chicago/Turabian StylePetrucci, Giorgia, Giuseppe Francesco Papalia, Fabrizio Russo, Gianluca Vadalà, Michela Piredda, Maria Grazia De Marinis, Rocco Papalia, and Vincenzo Denaro. 2022. "Psychological Approaches for the Integrative Care of Chronic Low Back Pain: A Systematic Review and Metanalysis" International Journal of Environmental Research and Public Health 19, no. 1: 60. https://doi.org/10.3390/ijerph19010060
APA StylePetrucci, G., Papalia, G. F., Russo, F., Vadalà, G., Piredda, M., De Marinis, M. G., Papalia, R., & Denaro, V. (2022). Psychological Approaches for the Integrative Care of Chronic Low Back Pain: A Systematic Review and Metanalysis. International Journal of Environmental Research and Public Health, 19(1), 60. https://doi.org/10.3390/ijerph19010060