
A Path Model of the Relationship between Mood, Exercise Behavior, Coping, and Mental Health among Malaysians during the COVID-19 Pandemic

 , ,
, , 
Abstract
:1. Introduction
1.1. Effect of Quarantine and Lockdown Measures
1.2. Impact of COVID-19 Pandemic and Its Investigation
2. Materials and Methods
2.1. Participants
2.2. Ethical Considerations
2.3. Questionnaires
2.3.1. Sociodemographic Data
2.3.2. Brunel Mood Scale (BRUMS)
2.3.3. Behavioral Regulation in Exercise (BREQ-3)
2.3.4. Brief Coping Orientation of Problem Experienced (Brief COPE)
2.3.5. Depression, Anxiety, and Stress Scale (DASS-21)
2.4. Sample Size Determination
2.5. Statistical Analyses
3. Results
3.1. Participants’ Characteristics
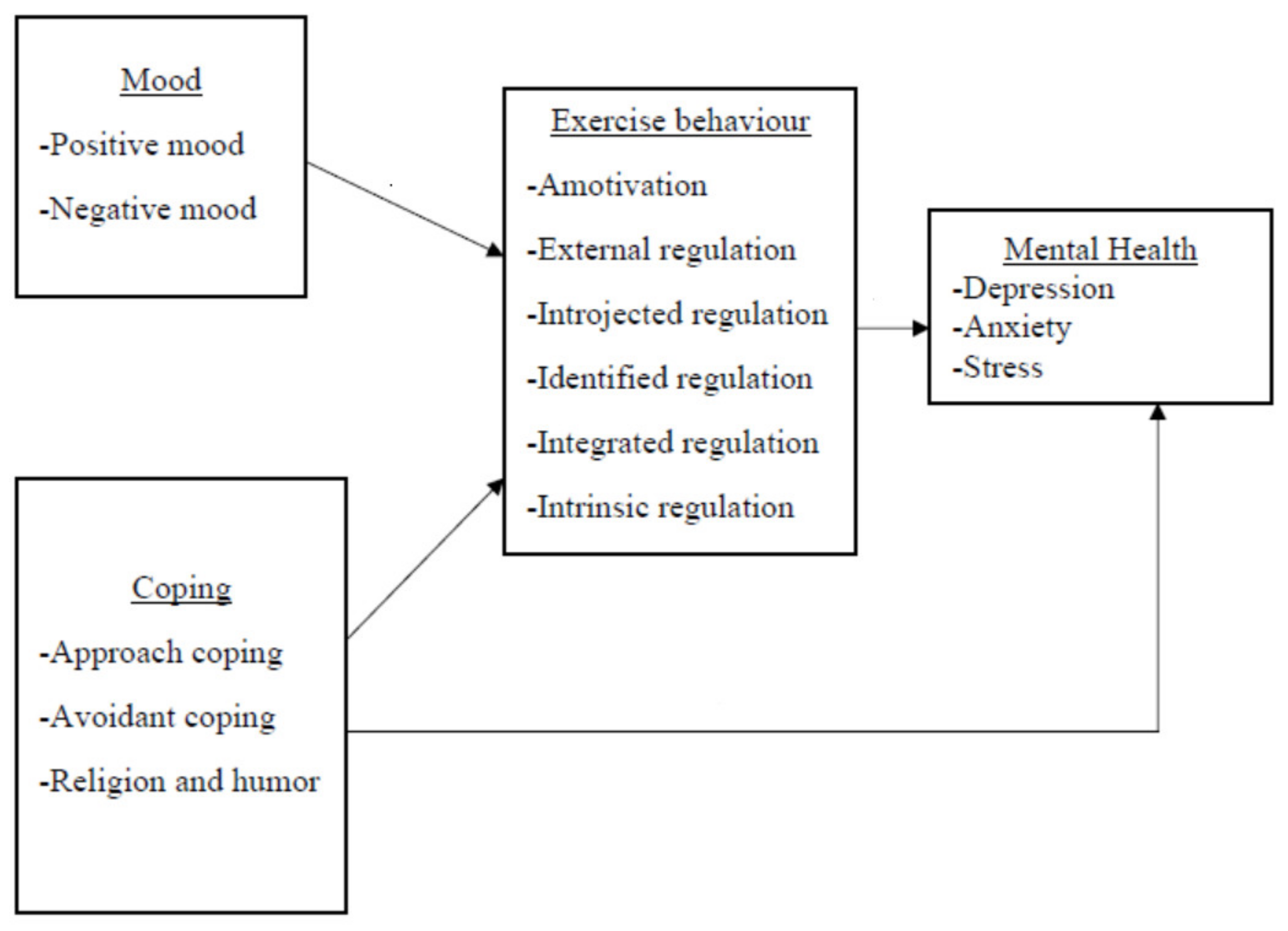
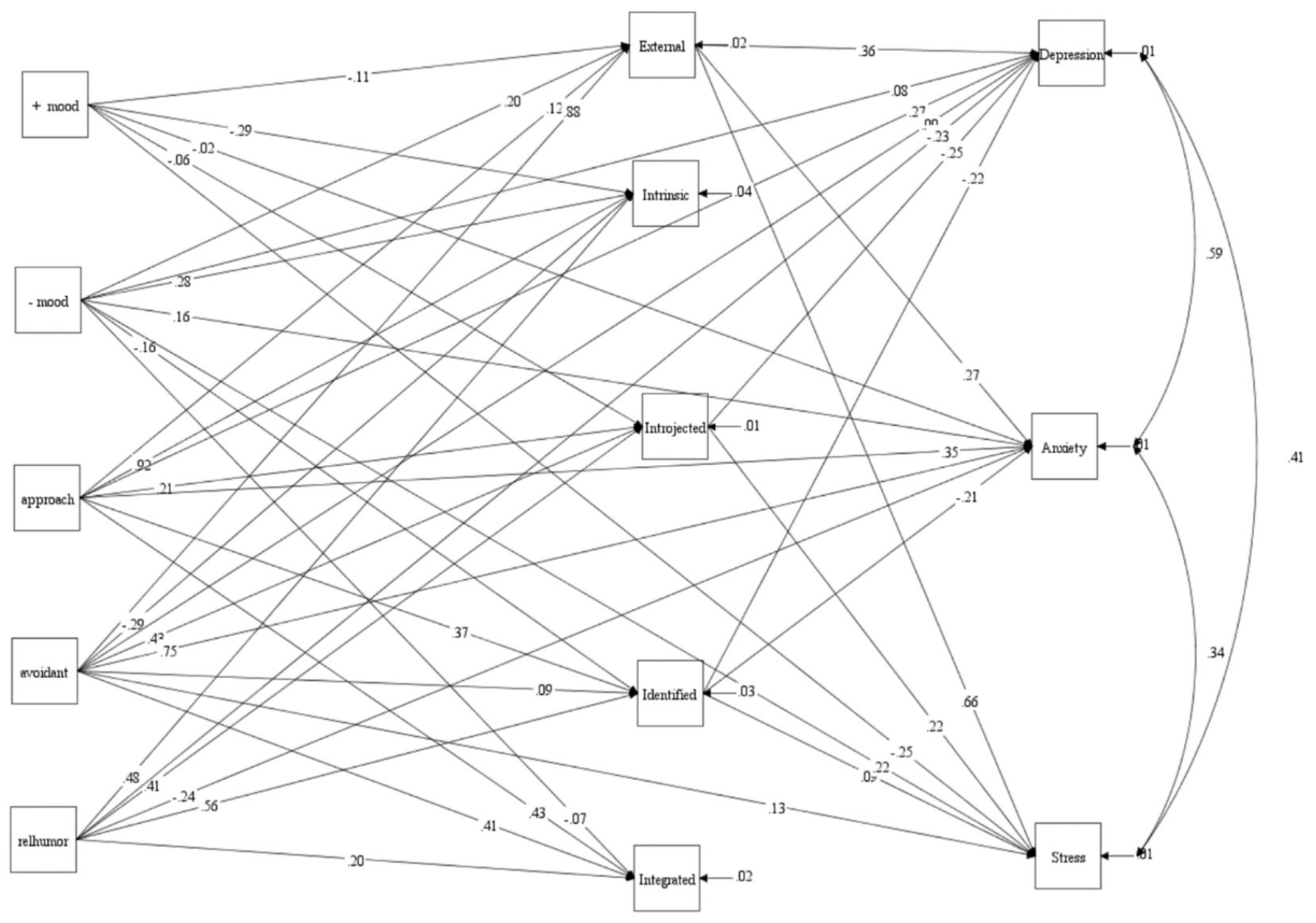
3.2. Path Model
4. Discussion
Strengths, Limitations, and Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- WHO Director-General’s Remarks at the Media Briefing on 2019-nCov on 11 February 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-remarks-at-the-media-briefing-on-2019-ncov-on-11-february-2020 (accessed on 15 March 2022).
- Benzing, V.; Nosrat, S.; Aghababa, A.; Barkoukis, V.; Bondarev, D.; Chang, Y.-K.; Cheval, B.; Çiftçi, M.C.; Elsangedy, H.M.; Guinto, M.L.M.; et al. Staying Active under Restrictions: Changes in Type of Physical Exercise during the Initial COVID-19 Lockdown. Int. J. Environ. Res. Public Health 2021, 18, 12015. [Google Scholar] [CrossRef] [PubMed]
- Ding, K.; Yang, J.; Chin, M.K.; Sullivan, L.; Durstine, L.; Violant-Holz, V.; Demirhan, G.; Oliveira, N.; Popeska, B.; Kuan, G.; et al. Physical Activity among Adults Residing in 11 Countries during the COVID-19 Pandemic Lockdown. Int. J. Environ. Res. Public Health 2021, 18, 7056. [Google Scholar] [CrossRef] [PubMed]
- Prime Minister’s Office of Malaysia. Restriction of Movement Order. 2020. Available online: https://www.pmo.gov.my/2020/03/movement-control-order/ (accessed on 15 March 2022).
- Ding, K.; Yang, J.; Chin, M.-K.; Sullivan, L.; Demirhan, G.; Violant-Holz, V.; Uvinha, R.R.; Dai, J.; Xu, X.; Popeska, B.; et al. Mental Health among Adults during the COVID-19 Pandemic Lockdown: A Cross-Sectional Multi-Country Comparison. Int. J. Environ. Res. Public Health 2021, 18, 2686. [Google Scholar] [CrossRef]
- Friedler, B.; Crapser, J.; McCullough, L. One is the deadliest number: The detrimental effects of social isolation on cerebrovascular diseases and cognition. Acta Neuropathol. 2015, 129, 493–509. [Google Scholar] [CrossRef] [Green Version]
- Huremovic, D. Social distancing, quarantine, and isolation BT—Psychiatry of pandemic: A mental health response to infection outbreak. In Psychiatry of Pandemics; Huremovic, D., Ed.; Spinger: Cham, Switzerland, 2019; pp. 85–94. [Google Scholar]
- Chirico, A.; Lucidi, F.; Mallia, L.; D’Aiuto, M.; Merluzzi, T.V. Indicators of distress in newly diagnosed breast cancer patients. PeerJ 2015, 3, e1107. [Google Scholar] [CrossRef]
- Gutin, B.; Yin, Z.; Humphries, M.C.; Barbeau, P. Relations of moderate and vigorous physical activity to fitness and fatness in adolescents. Am. J. Clin. Nutr. 2005, 81, 746–750. [Google Scholar] [CrossRef]
- Albrecht, J.N.; Werner, H.; Rieger, N.; Widmer, N.; Janisch, D.; Huber, R.; Jenni, O.G. Association between homeschooling and adolescent sleep duration and health during COVID-19 pandemic high school closures. JAMA Netw. Open 2022, 5, e2142100. [Google Scholar] [CrossRef]
- Aghababa, A.; Sani, S.H.Z.; Rohani, H.; Nabilpour, M.; Badicu, G.; Fathirezaie, Z.; Brand, S. No evidence of systematic change of physical activity patterns before and during the Covid-19 pandemic and related mood states among iranian adults attending team sports activities. Front. Psychol. 2021, 12, 641895. [Google Scholar] [CrossRef]
- Asmundson, G.J.; Taylor, S. Garbage in, garbage out: The tenuous state of research on PTSD in the context of the COVID-19 pandemic and infodemic. J. Anxiety Disord. 2021, 78, 102368. [Google Scholar] [CrossRef]
- Santiago, C.D.; Torres, S.A.; Brewer, S.K.; Fuller, A.K.; Lennon, J.M. The effect of cultural factors on daily coping and involuntary responses to stress among low-income Latino adolescents. J. Consum. Psychol. 2016, 44, 872–887. [Google Scholar] [CrossRef]
- Quartiroli, A.; Parsons-Smith, R.L.; Fogarty, G.J.; Kuan, G.; Terry, P.C. Cross-cultural validation of mood profile clusters in a sport and exercise context. Front. Psychol. 2018, 9, 1949. [Google Scholar] [CrossRef]
- Terry, P.C.; Lane, A.M.; Fogarty, G.J. Construct validity of the POMS-A for use with adults. Psychol. Sport Exerc. 2003, 4, 125–139. [Google Scholar] [CrossRef] [Green Version]
- Terry, P.C.; Lane, A.M.; Lane, H.J.; Keohane, L. Development and validation of a mood measure for adolescents. J. Sports Sci. 1999, 17, 861–872. [Google Scholar] [CrossRef] [Green Version]
- Lan, M.F.; Lane, A.M.; Roy, J.; Hanin, N.A. Validity of the Brunel Mood Scale for use with Malaysian athletes. J. Sports Sci. Med. 2012, 11, 131. [Google Scholar]
- Wilson, P.M.; Rodgers, W.M.; Loitz, C.C.; Scime, G. “It’s who I am...really!” the importance of integrated regulation in exercise contexts. J. Appl. Biobehav. Res. 2006, 11, 79–104. [Google Scholar] [CrossRef]
- Chai, S. Structural Relationship of Goal Content, Behavioural Regulation, and Coping Self-Efficacy on Amount of Physical Activity among Undergraduate Students in Health Campus, Universiti Sains Malaysia. Master’s Thesis, Universiti Sains Malaysia, Penang, Malaysia, 2018. [Google Scholar]
- Carver, C.S. You want to measure coping but your protocol’s too long: Consider the brief COPE. Int. J. Behav. Med. 1997, 4, 92–100. [Google Scholar] [CrossRef]
- Yusoff, M.S.B. The validity of the Malay Brief COPE in identifying coping strategies among adolescents in secondary school. Int. Med. J. 2011, 18, 29–33. [Google Scholar]
- Akin, A.; Çetın, B. The Depression Anxiety and Stress Scale (DASS): The study of validity and reliability. Educ. Sci. Theory Pract. 2007, 7, 260–268. [Google Scholar]
- Vaughan, R.S.; Edwards, E.J.; MacIntyre, T.E. Mental health measurement in a post Covid-19 world: Psychometric properties and invariance of the DASS-21 in athletes and non-athletes. Front. Psychol. 2020, 11, 2826. [Google Scholar] [CrossRef]
- Nordin, R.B.; Kaur, A.; Soni, T.; Por, L.K.; Miranda, S. Construct validity and internal consistency reliability of the Malay version of the 21-item depression anxiety stress scale (Malay-DASS-21) among male outpatient clinic attendees in Johor. Med. J. Malays. 2017, 72, 265. [Google Scholar]
- Muthén, L.K.; Muthén, B.O. Mplus User’s Guide, 8th ed.; Muthén & Muthén: Los Angeles, CA, USA, 2017. [Google Scholar]
- Wang, J.; Wang, X. Structural Equation Modeling: Applications Using Mplus; John Wiley & Sons: Chichester, UK, 2019. [Google Scholar]
- Hair, J.F.; Black, W.C.; Babin, B.J.; Anderson, R.E. Multivariate Data Analysis, 7th ed.; Pearson Prentice Hall: Hoboken, NJ, USA, 2010. [Google Scholar]
- Annesi, J.J.; Gorjala, S. Relations of self-regulation and self-efficacy for exercise and eating and BMI change: A field investigation. Biopsychosoc. Med. 2010, 4, 10. [Google Scholar] [CrossRef] [Green Version]
- Kline, R.B. Principles and Practice of Structural Equation Modelling, 3rd ed.; Guilford Publications: New York, NY, USA, 2011. [Google Scholar]
- Muhamad, A.S.; Mohd Puad, N.F.R.; Kuan, G. Effects of carbohydrate mouth rinsing on salivary lysozyme, mood states and running performance among the recreational runners. Malays J. Med. Sci. 2020, 27, 87–96. [Google Scholar] [CrossRef]
- Miller, K.J.; Mesagno, C.; McLaren, S.; Grace, F.; Yates, M.; Gomez, R. Exercise, mood, self-efficacy, and social support as predictors of depressive symptoms in older adults: Direct and interaction effects. Front. Psychol. 2019, 10, 2145. [Google Scholar] [CrossRef] [Green Version]
- Li, M.; Nie, J.; Ren, Y. Effects of exercise dependence on psychological health of Chinese college students. Psychiatr. Danub. 2015, 27, 410–419. [Google Scholar]
- Ogden, J.; Mtandabari, T. Examination stress and changes in mood and health related behaviours. Psychol. Health 1997, 12, 289–299. [Google Scholar] [CrossRef]
- Charles, N.E.; Strong, S.J.; Burns, L.C.; Bullerjahn, M.R.; Serafine, K.M. Increased mood disorder symptoms, perceived stress, and alcohol use among college students during the COVID-19 pandemic. Psychiatry Res. 2021, 296, 113706. [Google Scholar] [CrossRef]
- Terry, P.C.; Parsons-Smith, R.L.; Terry, V.R. Mood responses associated with COVID–19 restrictions. Front. Psychol. 2020, 11, 3090. [Google Scholar] [CrossRef]
- Psederska, E.; Vasilev, G.; DeAngelis, B.; Bozgunov, K.; Nedelchev, D.; Vassileva, J.; al’Absi, M. Resilience, mood, and mental health outcomes during the first wave of the COVID-19 pandemic in Bulgaria. PsyArXic 2021, 1, 20. Available online: https://psyarxiv.com/8nraq/ (accessed on 9 October 2020).
- Vancampfort, D.; De Hert, M.; Skjerven, L.H.; Gyllensten, A.L.; Parker, A.; Mulders, N.; Nyboe, L.; Spencer, F.; Probst, M. International organization of physical therapy in mental health consensus on physical activity within multidisciplinary rehabilitation programmes for minimising cardio-metabolic risk in patients with schizophrenia. Disabil. Rehabil. 2012, 34, 1–12. [Google Scholar] [CrossRef]
- Ryan, R.M.; Deci, E.L. Active human nature: Self-determination theory and the promotion and maintenance of sport, exercise, and health. Intrinsic Motiv. Self-Determ. Exerc. Sport 2007, 1, 19. [Google Scholar]
- Raglin, J.S. Exercise and mental health. Sports Med. 1990, 9, 323–329. [Google Scholar] [CrossRef] [PubMed]
- Khanzada, F.J.; Soomro, N.; Khan, S.Z. Association of physical exercise on anxiety and depression amongst adults. J. Coll. Physicians Surg. Pak. 2015, 25, 546–548. [Google Scholar]
- Blevins, C.E.; Rapoport, M.A.; Battle, C.L.; Stein, M.D.; Abrantes, A.M. Changes in coping, autonomous motivation, and beliefs about exercise among women in early recovery from alcohol participating in a lifestyle physical activity intervention. Ment. Health Phys. Act. 2017, 13, 137–142. [Google Scholar] [CrossRef] [PubMed]
- Dawson, D.L.; Golijani-Moghaddam, N. COVID-19: Psychological flexibility, coping, mental health, and wellbeing in the UK during the pandemic. J. Contextual Behav. Sci. 2020, 17, 126–134. [Google Scholar] [CrossRef]
- Ma, C.; Ma, L.; Helwan, A.; Ma’aitah, M.K.S.; Jami, S.A.; Mobarak, S.A.; Das, N.K.; Haque, M.A. An online survey and review about the awareness, coping style, and exercise behavior during the “COVID-19 pandemic situation” by implementing the cloud-based medical treatment technology system in China among the public. Sci. Prog. 2021, 104, 00368504211000889. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; McKenzie, L.A. The impacts of physical exercise on stress coping and well-being in university students in the context of leisure. Health 2014, 6, 2570–2580. [Google Scholar] [CrossRef] [Green Version]
- Yan, L.; Gan, Y.; Ding, X.; Wu, J.; Duan, H. The relationship between perceived stress and emotional distress during the COVID-19 outbreak: Effects of boredom proneness and coping style. J. Anxiety Disord. 2021, 77, 102328. [Google Scholar] [CrossRef]
- MacIntyre, P.D.; Gregersen, T.; Mercer, S. Language teachers’ coping strategies during the Covid-19 conversion to online teaching: Correlations with stress, wellbeing and negative emotions. System 2020, 94, 102352. [Google Scholar] [CrossRef]
- Agha, S. Mental well-being and association of the four factors coping structure model: A perspective of people living in lockdown during COVID-19. Ethics Med. Public Health 2021, 16, 100605. [Google Scholar] [CrossRef]
- Garcia, F.E.; Barraza-Peña, C.G.; Wlodarczyk, A.; Alvear-Carrasco, M.; Reyes-Reyes, A. Psychometric properties of the Brief-COPE for the evaluation of coping strategies in the Chilean population. Psicol. Reflexão Crítica 2018, 31, 11. [Google Scholar] [CrossRef]
- Dulmus, C.N.; Hilarski, C. When stress constitutes trauma and trauma constitutes crisis: The stress-trauma-crisis continuum. Brief Treat. Crisis Interv. 2003, 3, 27–36. [Google Scholar] [CrossRef]
- Wildman, W.J.; Joseph, B.; Richard, S.; Uffe, S.; Wesley, J.W.; Joseph, B.; Richard, S.; Uffe, S. Religion and the COVID-19 pandemic. Relig. Brain Behav. 2020, 10, 115–117. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Characteristic | Frequency (n) | Percentage (%) | Mean (SD) | Median (IQR) |
|---|---|---|---|---|
| Gender | ||||
| Male | 202 | (24.0) | ||
| Female | 640 | (76.0) | ||
| Age (years) | 22 (6) * | |||
| Ethnicity: | ||||
| Malay | 440 | (52.3) | ||
| Chinese | 308 | (36.6) | ||
| Indian | 48 | (5.7) | ||
| Others | 46 | (5.5) | ||
| Occupation: | ||||
| Employed with wages (full time)/ self-employed | 262 | (31.1) | ||
| A housewife | 7 | (0.8) | ||
| A student | 561 | (66.6) | ||
| Unable to work | 12 | (1.4) | ||
| Household income: | ||||
| I don’t have an income at the moment | 539 | (64.0) | ||
| Below RM 4360 | 147 | (17.5) | ||
| Between RM 4360 to RM 9616 | 109 | (12.9) | ||
| Above RM 9616 | 47 | (5.6) | ||
| Education: | ||||
| No formal education/Primary education/ Secondary education | 24 | (2.9) | ||
| Undergraduate degree | 656 | (77.9) | ||
| Postgraduate degree | 145 | (17.2) | ||
| Others | 17 | (2.0) | ||
| Exercise frequency: | ||||
| Never | 85 | (10.1) | ||
| Once in a while | 325 | (38.6) | ||
| Once a week | 107 | (12.7) | ||
| Two times a week | 88 | (10.5) | ||
| Three times a week | 86 | (10.2) | ||
| Four times a week | 35 | (4.2) | ||
| Five times a week | 29 | (3.4) | ||
| Six times a week | 17 | (2.0) | ||
| Every day | 70 | (8.3) | ||
| Exercise sessions (minutes per sessions): | ||||
| ˂10 min | 234 | (27.8) | ||
| ≥10 min | 608 | (72.2) | ||
| Have you tested positive for COVID-19: | ||||
| Yes | 5 | (0.6) | ||
| No | 837 | (99.4) |
| Model | CFI | TLI | SRMR | RMSEA (90%CI) | RMSEA p-Value |
|---|---|---|---|---|---|
| Model 1 (Initial) | 0.936 | 0.753 | 0.005 | 0.317 (0.305, 0.330) | <0.001 |
| Model 2 | 0.933 | 0.783 | 0.005 | 0.297 (0.286, 0.309) | <0.001 |
| Model 3 | 0.872 | 0.666 | 0.018 | 0.369 (0.359, 0.379) | <0.001 |
| Model 4 | 0.848 | 0.576 | 0.277 | 0.416 (0.405, 0.426) | <0.001 |
| Model 5 (Final) | 0.998 | 0.988 | 0.001 | 0.072 (0.056, 0.088) | 0.012 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yew, J.M.; Kueh, Y.C.; Norsa’adah, B.; Leong, F.W.; Tang, H.Y.; Kuan, G. A Path Model of the Relationship between Mood, Exercise Behavior, Coping, and Mental Health among Malaysians during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 5939. https://doi.org/10.3390/ijerph19105939
Yew JM, Kueh YC, Norsa’adah B, Leong FW, Tang HY, Kuan G. A Path Model of the Relationship between Mood, Exercise Behavior, Coping, and Mental Health among Malaysians during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2022; 19(10):5939. https://doi.org/10.3390/ijerph19105939
Chicago/Turabian StyleYew, Jing Mun, Yee Cheng Kueh, Bachok Norsa’adah, Foo Weng Leong, Heen Yeong Tang, and Garry Kuan. 2022. "A Path Model of the Relationship between Mood, Exercise Behavior, Coping, and Mental Health among Malaysians during the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 19, no. 10: 5939. https://doi.org/10.3390/ijerph19105939
APA StyleYew, J. M., Kueh, Y. C., Norsa’adah, B., Leong, F. W., Tang, H. Y., & Kuan, G. (2022). A Path Model of the Relationship between Mood, Exercise Behavior, Coping, and Mental Health among Malaysians during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health, 19(10), 5939. https://doi.org/10.3390/ijerph19105939