
Endometriosis and Infertility: A Long-Life Approach to Preserve Reproductive Integrity


{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Classification and Histopathology
3. Endometriosis and Infertility
3.1. Does Peritoneal Endometriosis Affect Fertility?
3.2. Does Ovarian Endometrioma per se Affect Fertility?
3.3. Does Deep Endometriosis Affect Fertility?
4. Laparoscopic Surgery
4.1. Should Minimal Mild Endometriotic Lesions Be Surgically Treated?
4.2. Should Ovarian Endometrioma Be Surgically Treated?
5. Ovarian Endometrioma and Infertility: Risk of Expectant Management
Which Are Possible Results and Risks of Surgery for Deep Endometriosis?
6. Deep Endometriosis and Infertility: Risk of Expectant Management in Pregnancy
7. Assisted Reproductive Technology (ART)
7.1. Which ART Procedure Is the Most Appropriate in Patients with Endometriosis?
7.1.1. Peritoneal Endometriosis
7.1.2. Ovarian Endometriomas and/or Deep Infiltrating Endometriosis
7.2. Which Is the Most Suitable Protocol for Ovarian Stimulation in Patients with Endometriosis, Undergoing IVF-ICSI?
8. Endometriosis Is a Chronic Pathology and Involves the Reproductive System: Fertility Preservation
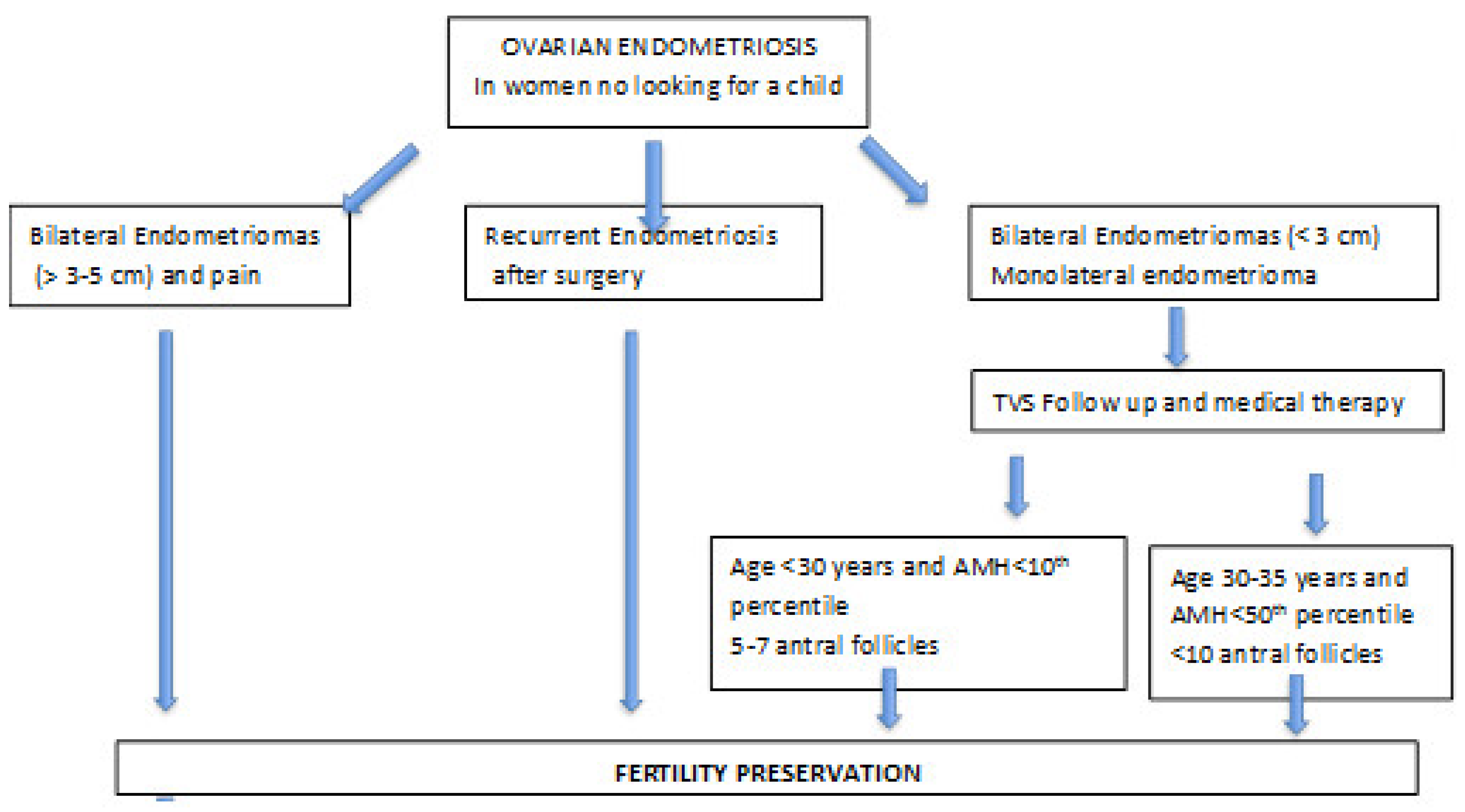
9. Propose an Algorithm
10. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Giudice, L.C. Endometriosis. N. Engl. J. Med. 2010, 362, 2389–2398. [Google Scholar] [CrossRef] [PubMed]
- Gylfason, J.T.; Kristjansson, K.A.; Sverrisdottir, G.; Jonsdottir, K.; Rafnsson, V.; Geirsson, R.T. Pelvic endometriosis diagnosed in an entire nation over 20 years. Am. J. Epidemiol. 2010, 172, 237–243. [Google Scholar] [CrossRef] [PubMed]
- Practice Committee of the American Society for Reproductive Medicine. Endometriosis and infertility: A committee opinion. Fertil. Steril. 2012, 98, 591–598. [Google Scholar] [CrossRef] [PubMed]
- Nisolle, M.; Donnez, J. Peritoneal endometriosis, ovarian endometriosis, and adenomyotic nodules of the rectovaginal septum are three different entities. Fertil. Steril. 1997, 68, 585–596. [Google Scholar] [CrossRef]
- Tuttlies, F.; Keckstein, J.; Ulrich, U.; Possover, M.; Schweppe, K.W.; Wustlich, M.; Buchweitz, O.; Greb, R.; Kandolf, O.; Mangold, R.; et al. ENZIAN-Score, a classification of deep infiltrating endometriosis. Zentralbl. Gynäkol. 2005, 127, 275–281. [Google Scholar] [CrossRef]
- Adamson, G.D.; Pasta, D. Endometriosis fertility index: The new, validated endometriosis staging system. Fertil. Steril. 2010, 94, 1609–1615. [Google Scholar] [CrossRef]
- Tomassetti, C.; Geysenbergh, B.; Meuleman, C.; Timmerman, D.; Fieuws, S.; D’Hooghe, T. External validation of the endometriosis fertility index (EFI) staging system for predicting non-ART pregnancy after endometriosis surgery. Hum. Reprod. 2013, 28, 1280–1288. [Google Scholar] [CrossRef] [Green Version]
- Ferrier, C.; Boujenah, J.; Poncelet, C.; Chabbert-Buffet, N.; D’Argent, E.M.; Carbillon, L.; Grynberg, M.; Darai, E.; Bendifallah, S. Use of the EFI score in endometriosis-associated infertility: A cost-effectiveness study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2020, 253, 296–303. [Google Scholar] [CrossRef]
- Johnson, N.P.; Hummelshoj, L.; Adamson, G.D.; Keckstein, J.; Taylor, H.S.; Abrao, M.S.; Bush, D.; Kiesel, L.; Tamimi, R.; Timms, K.; et al. World Endometriosis Society consensus on the classification of endometriosis. Hum. Reprod. 2017, 32, 315–324. [Google Scholar] [CrossRef]
- Macer, M.L.; Taylor, H.S. Endometriosis and infertility: A review of the pathogenesis and treatment of endometriosis-associatied infertility. Obstet. Gynecol. Clin. N. Am. 2012, 39, 535–549. [Google Scholar] [CrossRef] [Green Version]
- Vercellini, P.; Bocciolone, L.; Crosignani, P.G. Is mild endometriosis always a disease? Hum. Reprod. 1992, 7, 627–629. [Google Scholar] [CrossRef] [PubMed]
- Stratton, P. Diagnostic accuracy of laparoscopy, magnetic resonance imaging, and histopathologic examination for the detection of endometriosis. Fertil. Steril. 2003, 79, 1078–1085. [Google Scholar] [CrossRef]
- Dunselman, G.A.J.; Vermeulen, N.; Becker, C.; Calhaz-Jorge, C.; D’Hooghe, T.; De Bie, B.; Heikinheimo, O.; Horne, A.W.; Kiesel, L.; Nap, A.; et al. ESHRE guideline: Management of women with endometriosis. Hum. Reprod. 2014, 29, 400–412. [Google Scholar] [CrossRef] [PubMed]
- Ramírez-Pavez, T.N.; Martínez-Esparza, M.; Ruiz-Alcaraz, A.J.; Marín-Sánchez, P.; Machado-Linde, F.; García-Peñarrubia, P. The role of peritoneal macrophages in endometriosis. Int. J. Mol. Sci. 2021, 22, 10792. [Google Scholar] [CrossRef]
- Holoch, K.J.; Lessey, B.A. Endometriosis and infertility. Clin. Obstet. Gynecol. 2010, 53, 429–438. [Google Scholar] [CrossRef]
- Ding, G.-L.; Chen, X.-J.; Luo, Q.; Dong, M.-Y.; Wang, N.; Huang, H.-F. Attenuated oocyte fertilization and embryo development associated with altered growth factor/signal transduction induced by endometriotic peritoneal fluid. Fertil. Steril. 2010, 93, 2538–2544. [Google Scholar] [CrossRef]
- Marquardt, R.M.; Kim, T.H.; Shin, J.-H.; Jeong, J.-W. Progesterone and estrogen signaling in the endometrium: What goes wrong in endometriosis? Int. J. Mol. Sci. 2019, 20, 3822. [Google Scholar] [CrossRef] [Green Version]
- Lessey, B.A. The use of integrins for the assessment of uterine receptivity. Fertil. Steril. 1994, 61, 812–814. [Google Scholar] [CrossRef]
- Genbacev, O.D.; Prakobphol, A.; Foulk, R.A.; Krtolica, A.R.; Ilic, D.; Singer, M.S.; Yang, Z.-Q.; Kiessling, L.L.; Rosen, S.D.; Fisher, S.J. Trophoblast L-selectin-mediated adhesion at the maternal-fetal interface. Science 2003, 299, 405–408. [Google Scholar] [CrossRef]
- Coccia, M.E.; Rizzello, F.; Mariani, G.; Bulletti, C.; Palagiano, A.; Scarselli, G. Impact of endometriosis on in vitro fertilization and embryo transfer cycles in young women: A stage-dependent interference. Acta Obstet. Gynecol. Scand. 2011, 90, 1232–1238. [Google Scholar] [CrossRef]
- Guerriero, S.; Condous, G.; van den Bosch, T.; Valentin, L.; Leone, F.P.G.; Van Schoubroeck, D.; Exacoustos, C.; Installé, A.J.F.; Martins, W.P.; Abrao, M.S.; et al. Systematic approach to sonographic evaluation of the pelvis in women with suspected endometriosis, including terms, definitions and measurements: A consensus opinion from the International Deep Endometriosis Analysis (IDEA) group. Ultrasound Obstet. Gynecol. 2016, 48, 318–332. [Google Scholar] [CrossRef] [PubMed]
- Falcone, T.; Flyckt, R. Clinical management of endometriosis. Obstet. Gynecol. 2018, 131, 557–571. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guerriero, S.; Spiga, S.; Ajossa, S.; Peddes, C.; Perniciano, M.; Soggiu, B.; De Cecco, C.N.; Laghi, A.; Melis, G.B.; Saba, L. Role of imaging in the management of endometriosis. Minerva Ginecol. 2013, 65, 143–166. [Google Scholar] [PubMed]
- Vercellini, P.; Cortesi, I.; Giorgi, O.D.; Merlo, D.; Carinelli, S.G.; Crosignani, P.G. Transvaginal ultrasonography versus uterine needle biopsy in the diagnosis of diffuse adenomyosis. Hum. Reprod. 1998, 13, 2884–2887. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prefumo, F.; Serafini, G.; Martinoli, C.; Gandolfo, N.; Gandolfo, N.G.; Derchi, L.E. The sonographic evaluation of tubal pa-tency with stimulated acoustic emission imaging. Ultrasound Obstet. Gynecol. 2002, 20, 386–389. [Google Scholar] [CrossRef] [PubMed]
- Al-Fozan, H. Left lateral predisposition of endometriosis and endometrioma. Obstet. Gynecol. 2003, 101, 164–166. [Google Scholar] [CrossRef]
- Jenkins, S.; Olive, D.L.; Haney, A.F. Endometriosis: Pathogenetic implications of the anatomic distribution. Obstet. Gynecol. 1986, 67, 335–338. [Google Scholar]
- Redwine, D.B. Ovarian endometriosis: A marker for more extensive pelvic and intestinal disease. Fertil. Steril. 1999, 72, 310–315. [Google Scholar] [CrossRef]
- Donnez, J.; Lousse, J.-C.; Jadoul, P.; Donnez, O.; Squifflet, J. Laparoscopic management of endometriomas using a combined technique of excisional (cystectomy) and ablative surgery. Fertil. Steril. 2010, 94, 28–32. [Google Scholar] [CrossRef]
- Moscarini, M.; Milazzo, G.N.; Assorgi, C.; Pacchiarotti, A.; Caserta, D. Ovarian stripping versus cystectomy: Recurrence of endometriosis and pregnancy rate. Arch. Gynecol. Obstet. 2014, 290, 163–167. [Google Scholar] [CrossRef]
- Roman, H.; Auber, M.; Bourdel, N.; Martin, C.; Marpeau, L.; Puscasiu, L. Postoperative recurrence and fertility after endometrioma ablation using plasma energy: Retrospective assessment of a 3-year experience. J. Minim. Invasive Gynecol. 2013, 20, 573–582. [Google Scholar] [CrossRef] [PubMed]
- Roman, H.; Quibel, S.; Auber, M.; Muszynski, H.; Huet, E.; Marpeau, L.; Tuech, J.J. Recurrences and fertility after endometrioma ablation in women with and without colorectal endometriosis: A prospective cohort study. Hum. Reprod. 2015, 30, 558–568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maggiore, U.L.R.; Scala, C.; Venturini, P.; Remorgida, V.; Ferrero, S. Endometriotic ovarian cysts do not negatively affect the rate of spontaneous ovulation. Hum. Reprod. 2015, 30, 299–307. [Google Scholar] [CrossRef] [PubMed]
- Sanchez, A.M.; Viganò, P.; Somigliana, E.; Panina-Bordignon, P.; Vercellini, P.P.; Candiani, M. The distinguishing cellular and molecular features of the endometriotic ovarian cyst: From pathophysiology to the potential endometrioma-mediated damage to the ovary. Hum. Reprod. Updat. 2014, 20, 217–230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iwabuchi, T.; Yoshimoto, C.; Shigetomi, H.; Kobayashi, H. Oxidative stress and antioxidant defense in endometriosis and its malignant transformation. Oxidative Med. Cell. Longev. 2015, 2015, 848595. [Google Scholar] [CrossRef] [Green Version]
- Vercellini, P.; Crosignani, P.; Somigliana, E.; Viganò, P.; Buggio, L.; Bolis, G.; Fedele, L. The ‘incessant menstruation’ hypothesis: A mechanistic ovarian cancer model with implications for prevention. Hum. Reprod. 2011, 26, 2262–2273. [Google Scholar] [CrossRef] [Green Version]
- Becatti, M.; Fucci, R.; Mannucci, A.; Barygina, V.; Mugnaini, M.; Criscuoli, L.; Giachini, C.; Bertocci, F.; Picone, R.; Emmi, G.; et al. A Biochemical approach to detect oxidative stress in infertile women undergoing assisted reproductive technology procedures. Int. J. Mol. Sci. 2018, 19, 592. [Google Scholar] [CrossRef] [Green Version]
- Agarwal, A.; Aponte-Mellado, A.; Premkumar, B.J.; Shaman, A.; Gupta, S. The effects of oxidative stress on female reproduction: A review. Reprod. Biol. Endocrinol. 2012, 10, 49. [Google Scholar] [CrossRef] [Green Version]
- Kitajima, M.; Khan, K.N.; Harada, A.; Taniguchi, K.; Inoue, T.; Kaneuchi, M.; Miura, K.; Masuzaki, H. Association between ovarian endometrioma and ovarian reserve. Front. Biosci. 2018, 10, 92–102. [Google Scholar] [CrossRef] [Green Version]
- Lee, D.; Kim, S.K.; Lee, J.R.; Jee, B.C. Management of endometriosis-related infertility: Considerations and treatment options. Clin. Exp. Reprod. Med. 2020, 47, 1–11, Erratum in: Clin. Exp. Reprod. Med. 2020, 47, 153. [Google Scholar] [CrossRef]
- Cornillie, F.J.; Oosterlynck, D.; Lauweryns, J.M.; Koninckx, P.R. Deeply infiltrating pelvic endometriosis: Histology and clinical significance. Fertil. Steril. 1990, 53, 978–983. [Google Scholar] [CrossRef]
- Fauconnier, A.; Chapron, C.; Dubuisson, J.-B.; Vieira, M.; Dousset, B.; Breart, G. Relation between pain symptoms and the anatomic location of deep infiltrating endometriosis. Fertil. Steril. 2002, 78, 719–726. [Google Scholar] [CrossRef]
- Somigliana, E.; Infantino, M.; Candiani, M.; Vignali, M.; Chiodini, A.; Busacca, M.; Vignali, M. Association rate between deep peritoneal endometriosis and other forms of the disease: Pathogenetic implications. Hum. Reprod. 2004, 19, 168–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wahl, K.J.; Orr, N.L.; Lisonek, M.; Noga, H.; Bedaiwy, M.A.; Williams, C.; Allaire, C.; Albert, A.Y.; Smith, K.B.; Cox, S.; et al. Deep dyspareunia, superficial dyspareunia, and infertility concerns among women with endometriosis: A cross-sectional study. Sex. Med. 2020, 8, 274–281. [Google Scholar] [CrossRef] [Green Version]
- Vercellini, P.; Consonni, D.; Barbara, G.; Buggio, L.; Frattaruolo, M.P.; Somigliana, E. Adenomyosis and reproductive performance after surgery for rectovaginal and colorectal endometriosis: A systematic review and meta-analysis. Reprod. Biomed. Online 2014, 28, 704–713. [Google Scholar] [CrossRef] [Green Version]
- Tanbo, T.; Fedorcsak, P. Endometriosis-associated infertility: Aspects of pathophysiological mechanisms and treatment options. Acta Obstet. Gynecol. Scand. 2017, 96, 659–667. [Google Scholar] [CrossRef]
- Olive, D.L.; Stohs, G.F.; Metzger, D.A.; Franklin, R.R. Expectant management and hydrotubations in the treatment of endometriosis-associated infertility. Fertil. Steril. 1985, 44, 35–41. [Google Scholar] [CrossRef]
- Bérubé, S.; Marcoux, S.; Langevin, M.; Maheux, R. Fecundity of infertile women with minimal or mild endometriosis and women with unexplained infertility. The Canadian Collaborative Group on Endometriosis. Fertil. Steril. 1998, 69, 1034–1041. [Google Scholar] [CrossRef]
- Jacobson, T.Z.; Duffy, J.M.; Barlow, D.; Farquhar, C.; Koninckx, P.R.; Olive, D. Laparoscopic surgery for subfertility associated with endometriosis. Cochrane Database Syst. Rev. 2010, CD001398, Erratum in Cochrane Database Syst. Rev. 2014, 8, CD001398. [Google Scholar] [CrossRef] [Green Version]
- Bafort, C.; Beebeejaun, Y.; Tomassetti, C.; Bosteels, J.; Duffy, J.M.N. Laparoscopic surgery for endometriosis. Cochrane Database Syst. Rev. 2020, 2020, CD011031. [Google Scholar] [CrossRef]
- Benschop, L.; Farquhar, C.; Van Der Poel, N.; Heineman, M.J. Interventions for women with endometrioma prior to assisted reproductive technology. Cochrane Database Syst. Rev. 2010, CD008571. [Google Scholar] [CrossRef] [PubMed]
- Nama, V.; Kalu, E. Management of endometrioma in women embarking on IVF: Paucity of good quality evidence. Fertil. Steril. 2009, 92, e63. [Google Scholar] [CrossRef] [PubMed]
- Coccia, M.E.; Rizzello, F.; Cammilli, F.; Bracco, G.L.; Scarselli, G. Endometriosis and infertility: Surgery and ART: An integrated approach for successful management. Eur. J. Obstet. Gynecol. Reprod. Biol. 2008, 138, 54–59. [Google Scholar] [CrossRef]
- Donnez, J.; Pirard, C.; Smets, M.; Jadoul, P.; Squifflet, J. Surgical management of endometriosis. Best Pract. Res. Clin. Obstet. Gynaecol. 2004, 18, 329–348. [Google Scholar] [CrossRef] [PubMed]
- Coccia, M.E.; Rizzello, F.; Palagiano, A.; Scarselli, G. Long-term follow-up after laparoscopic treatment for endometriosis: Multivariate analysis of predictive factors for recurrence of endometriotic lesions and pain. Eur. J. Obstet. Gynecol. Reprod. Biol. 2011, 157, 78–83. [Google Scholar] [CrossRef] [PubMed]
- Coccia, M.E.; Rizzello, F.; Mariani, G.; Bulletti, C.; Palagiano, A.; Scarselli, G. Ovarian surgery for bilateral endometriomas influences age at menopause. Hum. Reprod. 2011, 26, 3000–3007. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Ziegler, D.; Borghese, B.; Chapron, C. Endometriosis and infertility: Pathophysiology and management. Lancet 2010, 376, 730–738. [Google Scholar] [CrossRef]
- Garcia-Velasco, J.A.; Somigliana, E. Management of endometriomas in women requiring IVF: To touch or not to touch. Hum. Reprod. 2009, 24, 496–501. [Google Scholar] [CrossRef] [Green Version]
- Busacca, M.; Bianchi, S.; Agnoli, B.; Candiani, M.; Calia, C.; De Marinis, S.; Vignali, M. Follow-up of laparoscopic treatment of stage III–IV endometriosis. J. Am. Assoc. Gynecol. Laparosc. 1999, 6, 55–58. [Google Scholar] [CrossRef]
- Busacca, M.; Chiaffarino, F.; Candiani, M.; Vignali, M.; Bertulessi, C.; Oggioni, G.; Parazzini, F. Determinants of long-term clinically detected recurrence rates of deep, ovarian, and pelvic endometriosis. Am. J. Obstet. Gynecol. 2006, 195, 426–432. [Google Scholar] [CrossRef]
- Koga, K.; Takemura, Y.; Osuga, Y.; Yoshino, O.; Hirota, Y.; Hirata, T.; Morimoto, C.; Harada, M.; Yano, T.; Taketani, Y. Recurrence of ovarian endometrioma after laparoscopic excision. Hum. Reprod. 2006, 21, 2171–2174. [Google Scholar] [CrossRef] [PubMed]
- Saleh, A.; Tulandi, T. Reoperation after laparoscopic treatment of ovarian endometriomas by excision and by fenestration. Fertil. Steril. 1999, 72, 322–324. [Google Scholar] [CrossRef]
- Tsoumpou, I.; Kyrgiou, M.; Gelbaya, T.A.; Nardo, L.G. The effect of surgical treatment for endometrioma on in vitro fertilization outcomes: A systematic review and meta-analysis. Fertil. Steril. 2009, 92, 75–87. [Google Scholar] [CrossRef] [PubMed]
- Coccia, M.E.; Rizzello, F.; Capezzuoli, T.; Evangelisti, P.; Cozzi, C.; Petraglia, F. Bilateral endometrioma excision: Surgery-related damage to ovarian reserve. Reprod. Sci. 2019, 26, 543–550. [Google Scholar] [CrossRef]
- Parazzini, F.; Progetto Menopausa Italia Study Group. Determinants of age at menopause in women attending menopause clinics in Italy. Maturitas 2007, 56, 280–287. [Google Scholar] [CrossRef] [PubMed]
- Coccia, M.E.; Rizzello, F.; Barone, S.; Pinelli, S.; Rapalini, E.; Parri, C.; Caracciolo, D.; Papageorgiou, S.; Cima, G.; Gandini, L. Is there a critical endometrioma size associated with reduced ovarian responsiveness in assisted reproduction techniques? Reprod. Biomed. Online 2014, 29, 259–266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferrero, S.; Scala, C.; Tafi, E.; Racca, A.; Venturini, P.L.; Maggiore, U.L.R. Impact of large ovarian endometriomas on the response to superovulation for in vitro fertilization: A retrospective study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2017, 213, 17–21. [Google Scholar] [CrossRef]
- Hart, R.J.; Hickey, M.; Maouris, P.; Buckett, W. Excisional surgery versus ablative surgery for ovarian endometriomata. Cochrane Database Syst. Rev. 2008, CD004992. [Google Scholar] [CrossRef]
- Donnez, J.; Wyns, C.; Nisolle, M. Does ovarian surgery for endometriomas impair the ovarian response to gonadotropin? Fertil. Steril. 2001, 76, 662–665. [Google Scholar] [CrossRef]
- Dahiya, A.; Sebastian, A.; Thomas, A.; George, R.; Thomas, V.; Peedicayil, A. Endometriosis and malignancy: The intriguing relationship. Int. J. Gynecol. Obstet. 2021, 155, 72–78. [Google Scholar] [CrossRef]
- Vercellini, P.; Somigliana, E.; Viganò, P.; Abbiati, A.; Barbara, G.; Crosignani, P.G. Surgery for endometriosis-associated infertility: A pragmatic approach. Hum. Reprod. 2009, 24, 254–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mereu, L.; Ruffo, G.; Landi, S.; Barbieri, F.; Zaccoletti, R.; Fiaccavento, A.; Stepniewska, A.; Pontrelli, G.; Minelli, L. Laparoscopic treatment of deep endometriosis with segmental colorectal resection: Short-term morbidity. J. Minim. Invasive Gynecol. 2007, 14, 463–469. [Google Scholar] [CrossRef] [PubMed]
- Daraï, E.; Cohen, J.; Ballester, M. Colorectal endometriosis and fertility. Eur. J. Obstet. Gynecol. Reprod. Biol. 2017, 209, 86–94. [Google Scholar] [CrossRef] [Green Version]
- Meuleman, C.; Tomassetti, C.; D’Hoore, A.; Van Cleynenbreugel, B.; Penninckx, F.; Vergote, I.; D’Hooghe, T. Surgical treatment of deeply infiltrating endometriosis with colorectal involvement. Hum. Reprod. Updat. 2011, 17, 311–326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Somigliana, E.; Garcia-Velasco, J.A. Treatment of infertility associated with deep endometriosis: Definition of therapeutic balances. Fertil. Steril. 2015, 104, 764–770. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vercellini, P.; Barbara, G.; Buggio, L.; Frattaruolo, M.P.; Somigliana, E.; Fedele, L. Effect of patient selection on estimate of reproductive success after surgery for rectovaginal endometriosis: Literature review. Reprod. Biomed. Online 2012, 24, 389–395. [Google Scholar] [CrossRef] [Green Version]
- Setúbal, A.; Sidiropoulou, Z.; Torgal, M.; Casal, E.; Lourenço, C.; Koninckx, P. Bowel complications of deep endometriosis during pregnancy or in vitro fertilization. Fertil. Steril. 2014, 101, 442–446. [Google Scholar] [CrossRef]
- Lebastchi, A.H.; Prieto, P.A.; Chen, C.; Lui, F.Y. Appendiceal endometriosis in a pregnant woman presenting with acute perforated appendicitis. J. Surg. Case Rep. 2013, 2013, rjt104. [Google Scholar] [CrossRef] [Green Version]
- Costa, A.; Sartini, A.; Garibaldi, S.; Cencini, M. Deep endometriosis induced spontaneous colon rectal perforation in pregnancy: Laparoscopy is advanced tool to confirm diagnosis. Case Rep. Obstet. Gynecol. 2014, 2014, 907150. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.-D.; Min, K.-O.; Moon, S.-W. Thoracoscopic treatment of recurrent pneumothorax in a pregnant woman: A case of ectopic deciduosis. Thorac. Cardiovasc. Surg. 2010, 58, 429–430. [Google Scholar] [CrossRef]
- Brosens, I.A.; Fusi, L.; Brosens, J. Endometriosis is a risk factor for spontaneous hemoperitoneum during pregnancy. Fertil. Steril. 2009, 92, 1243–1245. [Google Scholar] [CrossRef] [PubMed]
- Pisanu, A.; Deplano, D.; Angioni, S.; Ambu, R.; Uccheddu, A. Rectal perforation from endometriosis in pregnancy: Case report and literature review. World J. Gastroenterol. 2010, 16, 648–651. [Google Scholar] [CrossRef] [PubMed]
- Coccia, M.E.; Rizzello, F.; Palagiano, A.; Scarselli, G. The effect of the hormonal milieu of pregnancy on deep infiltrating endometriosis: Serial ultrasound assessment of changes in size and pattern of deep endometriotic lesions. Eur. J. Obstet. Gynecol. Reprod. Biol. 2012, 160, 35–39. [Google Scholar] [CrossRef]
- Barnhart, K.; Dunsmoor-Su, R.; Coutifaris, C. Effect of endometriosis on in vitro fertilization. Fertil. Steril. 2002, 77, 1148–1155. [Google Scholar] [CrossRef]
- Harb, H.; Gallos, I.; Chu, J.; Coomarasamy, A. The effect of endometriosis on in vitro fertilisation outcome: A systematic review and meta-analysis. BJOG Int. J. Obstet. Gynaecol. 2013, 120, 1308–1320. [Google Scholar] [CrossRef]
- Hamdan, M.; Dunselman, G.; Li, T.C.; Cheong, Y. The impact of endometrioma on IVF/ICSI outcomes: A systematic review and meta-analysis. Hum. Reprod. Updat. 2015, 21, 809–825. [Google Scholar] [CrossRef] [Green Version]
- Ho, H.-Y.; Lee, R.K.-K.; Hwu, Y.-M.; Lin, M.-H.; Su, J.-T.; Tsai, Y.-C. Poor response of ovaries with endometrioma previously treated with cystectomy to controlled ovarian hyperstimulation. J. Assist. Reprod. Genet. 2002, 19, 507–511. [Google Scholar] [CrossRef]
- Muzii, L.; Bellati, F.; Bianchi, A.; Palaia, I.; Manci, N.; Zullo, M.A.; Angioli, R.; Panici, P.B. Laparoscopic stripping of endometriomas: A randomized trial on different surgical techniques. Part II: Pathological results. Hum. Reprod. 2005, 20, 1987–1992. [Google Scholar] [CrossRef] [Green Version]
- Practice Committee of the American Society for Reproductive Medicine. Endometriosis and infertility. Fertil. Steril. 2006, 86, S156–S160. [Google Scholar] [CrossRef] [Green Version]
- Navarro, J.; Garrido, N.; Remohí, J.; Pellicer, A. How does endometriosis affect infertility? Obstet. Gynecol. Clin. N. Am. 2003, 30, 181–192. [Google Scholar] [CrossRef]
- Soliman, N.F.; Hillard, T.C. Hormone replacement therapy in women with past history of endometriosis. Climacteric J. Int. Menopause Soc. 2006, 9, 325–335. [Google Scholar] [CrossRef] [PubMed]
- Parazzini, F.; Bertulessi, C.; Pasini, A.; Rosati, M.; Di Stefano, F.; Shonauer, S.; Vicino, M.; Aguzzoli, L.; Trossarelli, G.F.; Massobrio, M.; et al. Determinants of short term recurrence rate of endometriosis. Eur. J. Obstet. Gynecol. Reprod. Biol. 2005, 121, 216–219. [Google Scholar] [CrossRef] [PubMed]
- Cheong, Y.; Tay, P.; Luk, F.; Gan, H.C.; Li, T.C.; Cooke, I. Laparoscopic surgery for endometriosis: How often do we need to re-operate? J. Obstet. Gynaecol. 2008, 28, 82–85. [Google Scholar] [CrossRef] [PubMed]
- Coccia, M.E.; Rizzello, F.; Gianfranco, S. Does controlled ovarian hyperstimulation in women with a history of endometriosis influence recurrence rate? J. Womens Health 2010, 19, 2063–2069. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Hondt, A.; Meuleman, C.; Tomassetti, C.; Peeraer, K.; D’Hooghe, T.M. Endometriosis and assisted reproduction: The role for reproductive surgery? Curr. Opin. Obstet. Gynecol. 2006, 18, 374–379. [Google Scholar] [CrossRef] [PubMed]
- Benaglia, L.; Somigliana, E.; Vighi, V.; Ragni, G.; Vercellini, P.; Fedele, L. Rate of severe ovarian damage following surgery for endometriomas. Hum. Reprod. 2010, 25, 678–682. [Google Scholar] [CrossRef] [Green Version]
- Tummon, I.S.; Asher, L.J.; Martin, J.S.; Tulandi, T. Randomized controlled trial of superovulation and insemination for infertility associated with minimal or mild endometriosis. Fertil. Steril. 1997, 68, 8–12. [Google Scholar] [CrossRef]
- Nulsen, J.C.; Walsh, S.; Dumez, S.; Metzger, D.A. A randomized and longitudinal study of human menopausal gonadotro-pin with intrauterine insemination in the treatment of infertility. Obstet. Gynecol. 1993, 82, 780–786. [Google Scholar]
- Werbrouck, E.; Spiessens, C.; Meuleman, C.; D’Hooghe, T. No difference in cycle pregnancy rate and in cumulative live-birth rate between women with surgically treated minimal to mild endometriosis and women with unexplained infertility after controlled ovarian hyperstimulation and intrauterine insemination. Fertil. Steril. 2006, 86, 566–571. [Google Scholar] [CrossRef] [Green Version]
- Van Der Houwen, L.E.E.; Schreurs, A.M.F.; Schats, R.; Heymans, M.W.; Lambalk, C.B.; Hompes, P.G.A.; Mijatovic, V. Efficacy and safety of intrauterine insemination in patients with moderate-to-severe endometriosis. Reprod. Biomed. Online 2014, 28, 590–598. [Google Scholar] [CrossRef] [Green Version]
- Sallam, H.N.; Garcia-Velasco, J.A.; Dias, S.; Arici, A. Long-term pituitary down-regulation before in vitro fertilization (IVF) for women with endometriosis. Cochrane Database Syst. Rev. 2006, 2006, CD004635, PMCID:PMC8195082. [Google Scholar] [CrossRef] [PubMed]
- Shi, Y.; Sun, Y.; Hao, C.; Zhang, H.; Wei, D.; Zhang, Y.; Zhu, Y.; Deng, X.; Qi, X.; Liu, H.; et al. Transfer of fresh versus frozen embryos in ovulatory women. N. Engl. J. Med. 2018, 378, 126–136. [Google Scholar] [CrossRef]
- Vuong, L.N.; Dang, V.Q.; Ho, T.M.; Huynh, B.G.; Ha, D.T.; Pham, T.D.; Nguyen, L.K.; Norman, R.; Mol, B.W. IVF Transfer of fresh or frozen embryos in women without polycystic ovaries. N. Engl. J. Med. 2018, 378, 137–147. [Google Scholar] [CrossRef] [PubMed]
- Donnez, J.; Chantraine, F.; Nisolle, M. The efficacy of medical and surgical treatment of endometriosis-associated infertility: Arguments in favour of a medico-surgical aproach. Hum. Reprod. Updat. 2002, 8, 89–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benaglia, L.; Somigliana, E.; Iemmello, R.; Colpi, E.; Nicolosi, A.E.; Ragni, G. Endometrioma and oocyte retrieval–induced pelvic abscess: A clinical concern or an exceptional complication? Fertil. Steril. 2008, 89, 1263–1266. [Google Scholar] [CrossRef]
- Barnett, R.; Banks, N.; DeCherney, A.H. Endometriosis and fertility preservation. Clin. Obstet. Gynecol. 2017, 60, 517–523. [Google Scholar] [CrossRef]
- Cobo, A.; Giles, J.; Paolelli, S.; Pellicer, A.; Remohí, J.; García-Velasco, J.A. Oocyte vitrification for fertility preservation in women with endometriosis: An observational study. Fertil. Steril. 2020, 113, 836–844. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.J.; Kim, S.K.; Lee, J.R.; Suh, C.S.; Kim, S.H. Oocyte cryopreservation for fertility preservation in women with ovarian endometriosis. Reprod. Biomed. Online 2020, 40, 827–834. [Google Scholar] [CrossRef] [PubMed]
- Horikawa, T.; Nakagawa, K.; Ohgi, S.; Kojima, R.; Nakashima, A.; Ito, M.; Takahashi, Y.; Saito, H. The frequency of ovulation from the affected ovary decreases following laparoscopic cystectomy in infertile women with unilateral endometrioma during a natural cycle. J. Assist. Reprod. Genet. 2008, 25, 239–244. [Google Scholar] [CrossRef] [Green Version]
- Sunkara, S.K.; Rittenberg, V.; Raine-Fenning, N.; Bhattacharya, S.; Zamora, J.; Coomarasamy, A. Association between the number of eggs and live birth in IVF treatment: An analysis of 400 135 treatment cycles. Hum. Reprod. 2011, 26, 1768–1774. [Google Scholar] [CrossRef] [Green Version]
- Doyle, J.O.; Richter, K.S.; Lim, J.; Stillman, R.J.; Graham, J.R.; Tucker, M.J. Successful elective and medically indicated oocyte vitrification and warming for autologous in vitro fertilization, with predicted birth probabilities for fertility preservation according to number of cryopreserved oocytes and age at retrieval. Fertil. Steril. 2016, 105, 459–466.e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shim, Y.J.; Hong, Y.H.; Kim, S.K.; Jee, B.C. Optimal numbers of mature oocytes to produce at least one or multiple top-quality day-3 embryos in normal responders. Clin. Exp. Reprod. Med. 2020, 47, 221–226. [Google Scholar] [CrossRef] [PubMed]
- Sanchez, A.M.; Vanni, V.S.; Bartiromo, L.; Papaleo, E.; Zilberberg, E.; Candiani, M.; Orvieto, R.; Viganò, P. Is the oocyte quality affected by endometriosis? A review of the literature. J. Ovarian Res. 2017, 10, 43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Juneau, C.; Kraus, E.; Werner, M.; Franasiak, J.; Morin, S.; Patounakis, G.; Molinaro, T.; de Ziegler, D.; Scott, R.T. Patients with endometriosis have aneuploidy rates equivalent to their age-matched peers in the in vitro fertilization population. Fertil. Steril. 2017, 108, 284–288. [Google Scholar] [CrossRef] [Green Version]
- National Institute for Health and Care Excellence. Endometriosis: Diagnosis and Management; NICE Guidelines [NG73]; National Institute for Health and Care Excellence: London, UK, 2017. [Google Scholar]
- Collinet, P.; Fritel, X.; Revel-Delhom, C.; Ballester, M.; Bolze, P.; Borghese, B.; Bornsztein, N.; Boujenah, J.; Brillac, T.; Chabbert-Buffet, N.; et al. Management of endometriosis: CNGOF/HAS clinical practice guidelines—Short version. J. Gynecol. Obstet. Hum. Reprod. 2018, 47, 265–274. [Google Scholar] [CrossRef]
- The Federation of Obstetric and Gynaecological Societies of India. FOGSI FOCUS Endometriosis; The Health Sciences Publisher: New Delhi, India, 2018. [Google Scholar]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Coccia, M.E.; Nardone, L.; Rizzello, F. Endometriosis and Infertility: A Long-Life Approach to Preserve Reproductive Integrity. Int. J. Environ. Res. Public Health 2022, 19, 6162. https://doi.org/10.3390/ijerph19106162
Coccia ME, Nardone L, Rizzello F. Endometriosis and Infertility: A Long-Life Approach to Preserve Reproductive Integrity. International Journal of Environmental Research and Public Health. 2022; 19(10):6162. https://doi.org/10.3390/ijerph19106162
Chicago/Turabian StyleCoccia, Maria Elisabetta, Luca Nardone, and Francesca Rizzello. 2022. "Endometriosis and Infertility: A Long-Life Approach to Preserve Reproductive Integrity" International Journal of Environmental Research and Public Health 19, no. 10: 6162. https://doi.org/10.3390/ijerph19106162
APA StyleCoccia, M. E., Nardone, L., & Rizzello, F. (2022). Endometriosis and Infertility: A Long-Life Approach to Preserve Reproductive Integrity. International Journal of Environmental Research and Public Health, 19(10), 6162. https://doi.org/10.3390/ijerph19106162