
Access to Services from Persons with Disabilities in Afghanistan: Is Community Based Rehabilitation Making a Difference?


Abstract
:1. Introduction
2. Materials and Methods
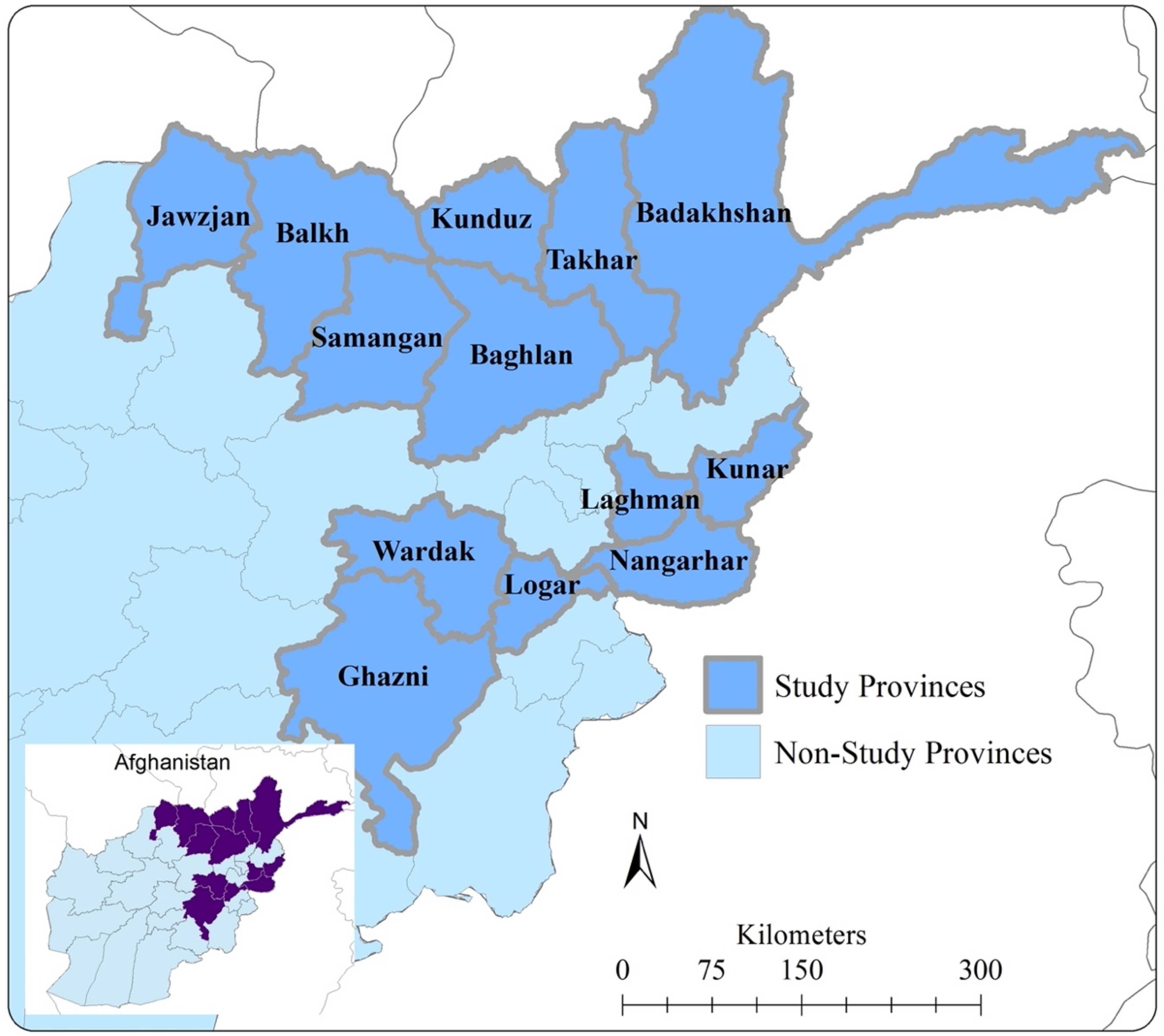
2.1. Study Location and Population
2.2. Study Design
2.3. Data Collection
2.4. Study Variables
2.4.1. Outcomes
- Physical Therapy
- Mobility and assistive devices
- Employment and livelihood support
- Education support
- Advocacy and community mobilization
2.4.2. Exposure Variables
2.4.3. Potential Confounders
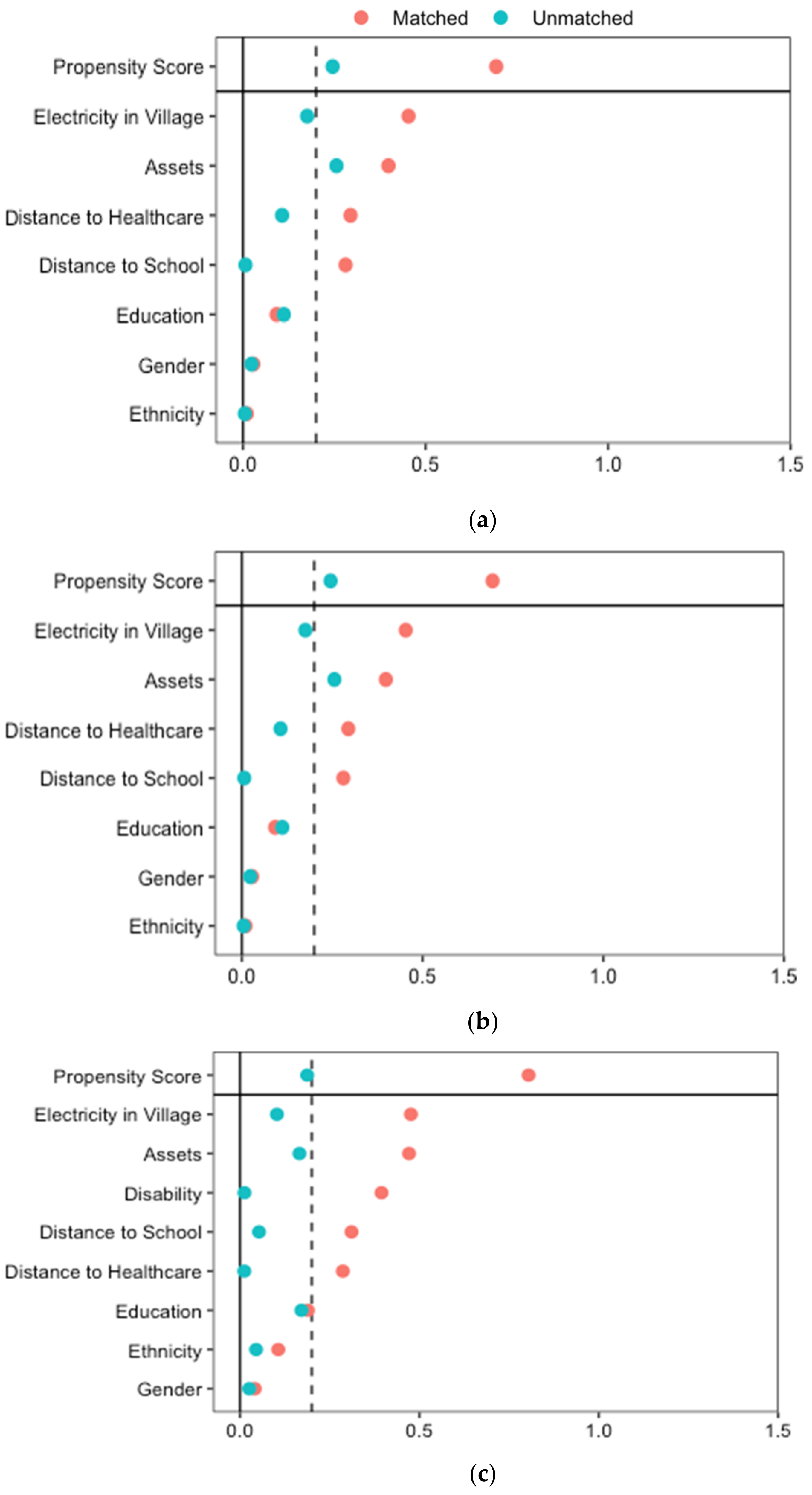
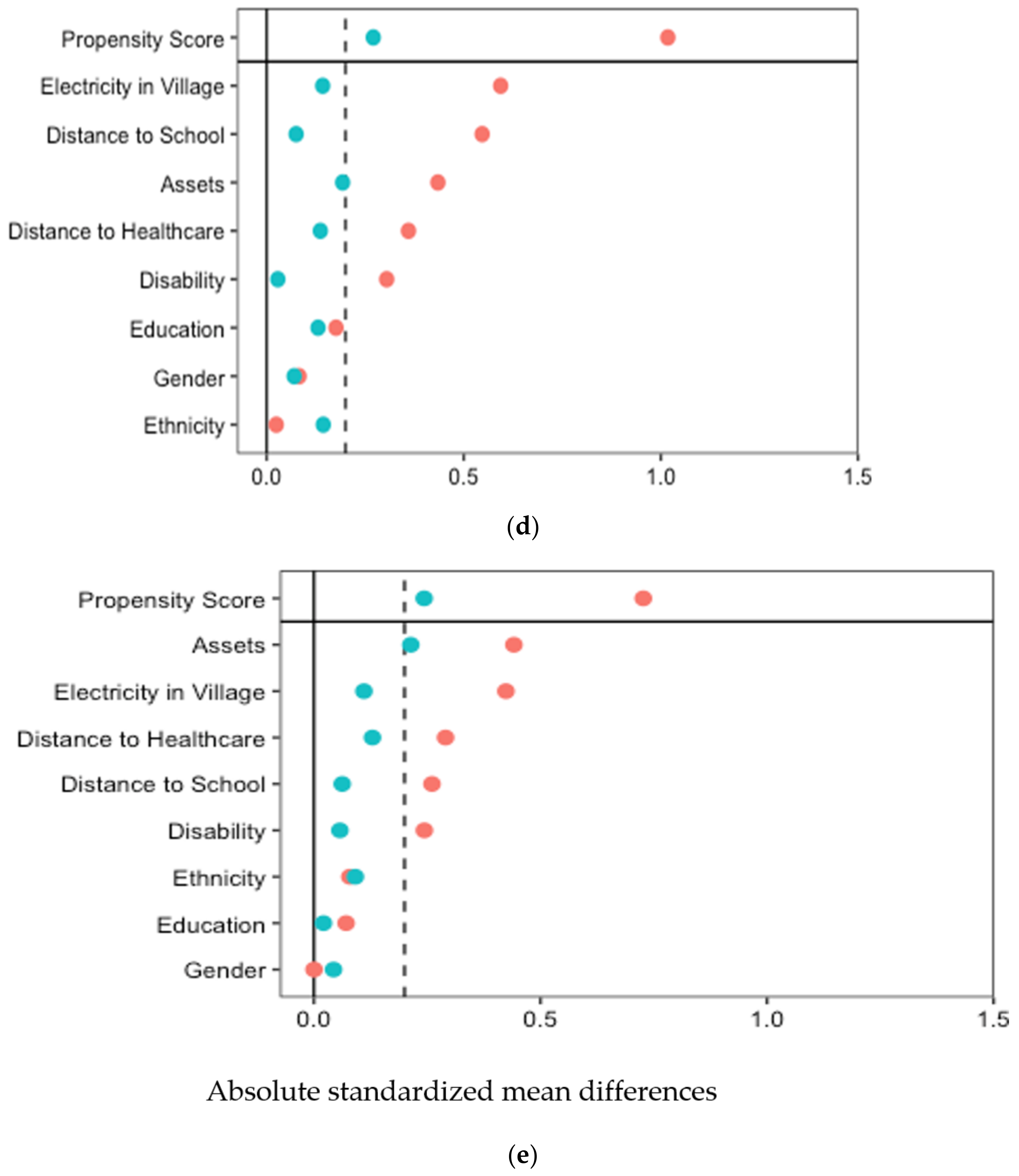
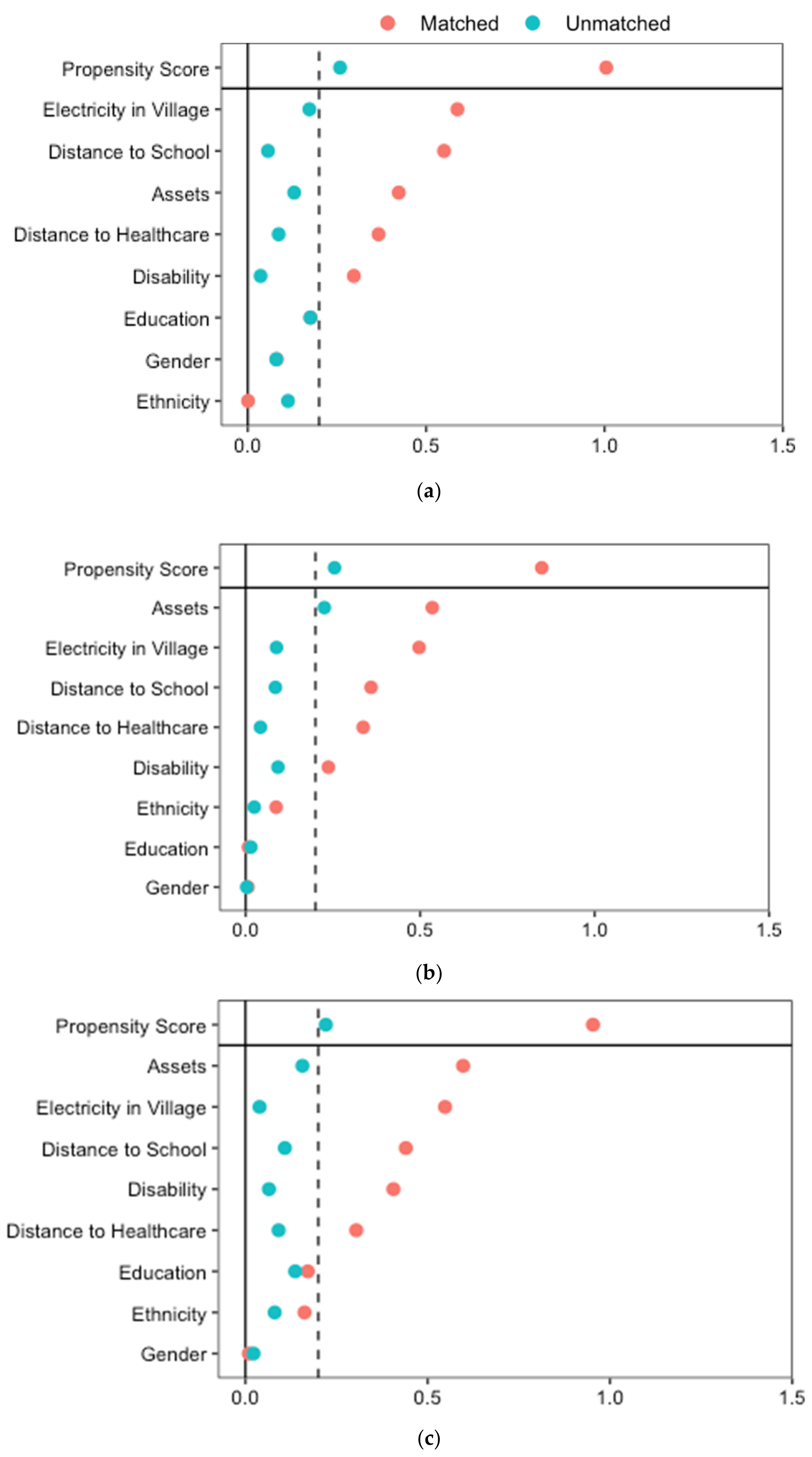
2.5. Statistical Analysis
3. Results
3.1. Baseline Descriptive Statistics
3.2. Endline Bivariate Analysis
3.3. Effect of the CBR Program on Access to Services
3.4. Unmet Needs by the CBR Program
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- United Nations Department of Economic and Social Affairs. UN Flagship Report on Disability and Development 2018; United Nations Department of Economic and Social Affairs: New York, NY, USA, 2018; p. 390. [Google Scholar]
- Mitra, S. The Human Development Model of Disability, Health and Wellbeing. In Disability, Health and Human Development; Springer: Berlin/Heidelberg, Germany, 2018; pp. 9–32. [Google Scholar]
- Palmer, M. Disability and Poverty: A Conceptual Review. J. Disabil. Policy Stud. 2011, 21, 210–218. [Google Scholar] [CrossRef]
- Hume-Nixon, M.; Kuper, H. The association between malnutrition and childhood disability in low- and middle- income countries: Systematic review and meta-analysis of observational studies. Trop. Med. Int. Health 2018, 23, 1158–1175. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, N.; Buliung, R.; Wilson, K. Disability and food access and insecurity: A scoping review of the literature. Health Place 2019, 57, 107–121. [Google Scholar] [CrossRef] [PubMed]
- Prynn, J.E.; Kuper, H. Perspectives on disability and non-communicable diseases in low-and middle-income countries, with a focus on stroke and dementia. Int. J. Environ. Res. Public Health 2019, 16, 3488. [Google Scholar] [CrossRef] [Green Version]
- Trani, J.F.; Kumar, P.; Ballard, E.; Chandola, T. Assessment of progress towards universal health coverage for people with disabilities in Afghanistan: A multilevel analysis of repeated cross-sectional surveys. Lancet Glob. Health 2017, 5, e828–e837. [Google Scholar] [CrossRef] [Green Version]
- Mutwali, R.; Ross, E. Disparities in physical access and healthcare utilization among adults with and without disabilities in South Africa. Disabil. Health J. 2019, 12, 35–42. [Google Scholar] [CrossRef]
- Mactaggart, I.; Baker, S.; Bambery, L.; Iakavai, J.; Kim, M.J.; Morrison, C.; Poilapa, R.; Shem, J.; Sheppard, P.; Tanguay, J.; et al. Water, women and disability: Using mixed-methods to support inclusive wash programme design in Vanuatu. Lancet Reg. Health-West. Pac. 2021, 8, 100109. [Google Scholar] [CrossRef]
- Trani, J.-F.; Fowler, P.; Bakhshi, P.; Kumar, P. Assessment of progress in education for children and youth with disabilities in Afghanistan: A multilevel analysis of repeated cross-sectional surveys. PLoS ONE 2019, 14, e0217677. [Google Scholar] [CrossRef]
- Bakhshi, P.; Babulal, G.M.; Trani, J.F. Disability, Poverty and Schooling in Post-Civil War in Sierra Leone. Eur. J. Dev. Res. Forthcom. 2021, 33, 482–501. [Google Scholar] [CrossRef]
- Lamichhane, K. Disability and barriers to education: Evidence from Nepal. Scand. J. Disabil. Res. 2013, 15, 311–324. [Google Scholar] [CrossRef]
- Mizunoya, S.; Mitra, S.; Yamasaki, I. Disability and school attendance in 15 low- and middle-income countries. World Dev. 2018, 104, 388–403. [Google Scholar] [CrossRef]
- Tripney, J.; Roulstone, A.; Vigurs, C.; Hogrebe, N.; Schmidt, E.; Stewart, R. Interventions to Improve the Labour Market Situation of Adults with Physical and/or Sensory Disabilities in Low- and Middle-Income Countries: A Systematic Review. Campbell Syst. Rev. 2015, 11, 1–127. [Google Scholar] [CrossRef]
- Morwane, R.E.; Dada, S.; Bornman, J. Barriers to and facilitators of employment of persons with disabilities in low-and middle-income countries: A scoping review. Afr. J. Disabil. 2021, 10, 833. [Google Scholar] [CrossRef]
- Trani, J.-F.; Bakhshi, P.; Brown, D.; Lopez, D.; Gall, F. Disability as deprivation of capabilities: Estimation using a large-scale survey in Morocco and Tunisia and an instrumental variable approach. Soc. Sci. Med. 2018, 211, 48–60. [Google Scholar] [CrossRef]
- Tobias, E.I.; Mukhopadhyay, S. Disability and social exclusion: Experiences of individuals with visual impairments in the Oshikoto and Oshana regions of Namibia. Psychol. Dev. Soc. 2017, 29, 22–43. [Google Scholar] [CrossRef]
- Tilly, L. Afraid to leave the house: Issues leading to social exclusion and loneliness for people with a learning disability. Tizard Learn. Disabil. Rev. 2019, 24, 168–175. [Google Scholar] [CrossRef]
- Trani, J.-F.; Bakhshi, P.; Tlapek, S.M.; Lopez, D.; Gall, F. Disability and Poverty in Morocco and Tunisia: A Multidimensional Approach. J. Hum. Dev. Capab. 2015, 16, 518–548. [Google Scholar] [CrossRef]
- United Nations. Convention on the Rights of Persons with Disabilities; United Nations: New York, NY, USA, 2006. [Google Scholar]
- World Health Organization. Community-Based Rehabilitation: CBR Guidelines; WHO: Geneva, Switzerland, 2010. [Google Scholar]
- ILO; UNESCO; WHO. Community Based Rehabilitation: A Strategy for Rehabilitation, Equalization of Opportunities, Poverty Reduction and Social Inclusion of People with Disabilities; Joint Position Paper; United Nations: Geneva, Switzerland, 2004. [Google Scholar]
- DFID. Disability, Poverty and Development; DFID: London, UK, 2000. [Google Scholar]
- Eldar, R. Integrated institution—community rehabilitation in developed countries: A proposal. Disabil. Rehabil. 2000, 22, 266–274. [Google Scholar] [CrossRef]
- Helander, E.; UNDP. Interregional Programme for Disabled. In Prejudice and Dignity: An Introduction to Community-Based Rehabilitation; United Nations Development Programme: New York, NY, USA, 1993. [Google Scholar]
- Mitchell, R. The research base of community-based rehabilitation. Disabil. Rehabil. 1999, 21, 459–4688. [Google Scholar] [CrossRef]
- Mauro, V.; Biggeri, M.; Grilli, L. Does Community-Based Rehabilitation Enhance the Multidimensional Well-Being of Deprived Persons With Disabilities? A Multilevel Impact Evaluation. World Dev. 2015, 76, 190–202. [Google Scholar] [CrossRef]
- Cornielje, H. The Role and Position of Disabled People’s Organisations in Community Based Rehabilitation: Balancing between Dividing Lines. Asia Pac. Disabil. Rehabil. J. 2009, 20, 3–14. [Google Scholar]
- Sharma, M. Community participation in community-based rehabilitation programmes. Asia Pac. Disabil. Rehabil. J. 2007, 18, 146–157. [Google Scholar]
- World Health Organization. International Consultation to Review Community-Based Rehabilitation; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Turmusani, M.; Vreede, A.; Wirz, S.L. Some ethical issues in community-based rehabilitation initiatives in developing countries. Disabil. Rehabil. 2002, 24, 558–564. [Google Scholar] [CrossRef] [PubMed]
- Chappell, P.; Johannsmeier, C. The impact of community based rehabilitation as implemented by community rehabilitation facilitators on people with disabilities, their families and communities within South Africa. Disabil. Rehabil. 2009, 31, 7–13. [Google Scholar] [CrossRef]
- Kuyini, A.B.; Alhassan, A.-R.K.; Mahama, F.K. The ghana community-based rehabilitation program for people with disabilities: What happened at the end of donor support? J. Soc. Work. Disabil. Rehabil. 2011, 10, 247–267. [Google Scholar] [CrossRef]
- Saran, A.; White, H.; Kuper, H. Evidence and gap map of studies assessing the effectiveness of interventions for people with disabilities in low-and middle-income countries. Campbell Syst. Rev. 2020, 16, e1070. [Google Scholar] [CrossRef] [Green Version]
- Iemmi, V.; Blanchet, K.; Gibson, L.J.; Kumar, K.S.; Rath, S.; Hartley, S.; Murthy, G.V.S.; Patel, V.; Weber, J.; Kuper, H. Community-based rehabilitation for people with physical and mental disabilities in low- and middle-income countries: A systematic review and meta-analysis. J. Dev. Eff. 2016, 8, 368–387. [Google Scholar] [CrossRef] [Green Version]
- Mauro, V.; Biggeri, M.; Deepak, S.; Trani, J.F. The effectiveness of community-based rehabilitation programmes: An impact evaluation of a quasi-randomised trial. J. Epidemiol. Community Health 2014, 68, 1102–1108. [Google Scholar] [CrossRef] [Green Version]
- Shore, S.; Juillerat, S. The impact of a low cost wheelchair on the quality of life of the disabled in the developing world. Med Sci. Monit. 2012, 18, CR533–CR542. [Google Scholar] [CrossRef] [Green Version]
- Serin, G.E.Ç.; Kisa, S.S.; Aydin, Ö. The effectiveness of nutrition and activity programmes for young adults with intellectual disabilities. Int. J. Caring Sci. 2014, 7, 449. [Google Scholar]
- Soji, F.; Kumar, J.; Varughese, S. Sustainability: Lessons from a community-based rehabilitation programme in Karnataka, India. Knowl. Manag. Dev. J. 2016, 12, 79–103. [Google Scholar]
- Zhang, G.F.; Tsui, C.M.; Lu, A.J.B.; Yu, L.B.; Tsang, H.W.H.; Li, D. Integrated Supported Employment for People With Schizophrenia in Mainland China: A Randomized Controlled Trial. Am. J. Occup. Ther. 2017, 71, 7106165020p1–7106165020p8. [Google Scholar] [CrossRef]
- Trani, J.-F.; Vasquez-Escallon, J.; Bakhshi, P. The impact of a community based rehabilitation program in Afghanistan: A longitudinal analysis using propensity score matching and difference in difference analysis. Confl. Health 2021, 15, 1–21. [Google Scholar] [CrossRef]
- Chatterjee, S.; Patel, V.; Chatterjee, A.; Weiss, H.A. Evaluation of a community-based rehabilitation model for chronic schizophrenia in rural India. Br. J. Psychiatry 2003, 182, 57–62. [Google Scholar] [CrossRef] [Green Version]
- Chatterjee, S.; Naik, S.; John, S.; Dabholkar, H.; Balaji, M.; Koschorke, M.; Varghese, M.; Thara, R.; Weiss, H.A.; Williams, P.; et al. Effectiveness of a community-based intervention for people with schizophrenia and their caregivers in India (COPSI): A randomised controlled trial. Lancet 2014, 383, 1385–1394. [Google Scholar] [CrossRef] [Green Version]
- Trani, J.-F.; Browne, J.; Kett, M.; Bah, O.; Morlai, T.; Bailey, N.; Groce, N. Access to health care, reproductive health and disability: A large scale survey in Sierra Leone. Soc. Sci. Med. 2011, 73, 1477–1489. [Google Scholar] [CrossRef]
- Trani, J.-F.; Bakhshi, P.; Noor, A.A.; Lopez, D.; Mashkoor, A. Poverty, vulnerability, and provision of healthcare in Afghanistan. Soc. Sci. Med. 2010, 70, 1745–1755. [Google Scholar] [CrossRef] [Green Version]
- Mulumba, M.; Nantaba, J.; Brolan, C.E.; Ruano, A.L.; Brooker, K.; Hammonds, R. Perceptions and experiences of access to public healthcare by people with disabilities and older people in Uganda. Int. J. Equity Health 2014, 13, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Munthali, A.C.; Swartz, L.; Mannan, H.; MacLachlan, M.; Chilimampunga, C.; Makupe, C. This one will delay us”: Barriers to accessing health care services among persons with disabilities in Malawi. Disabil. Rehabil. 2019, 41, 683–690. [Google Scholar] [CrossRef]
- Vergunst, R.; Swartz, L.; Hem, K.-G.; Eide, A.H.; Mannan, H.; MacLachlan, M.; Mji, G.; Braathen, S.H.; Schneider, M. Access to health care for persons with disabilities in rural South Africa. BMC Health Serv. Res. 2017, 17, 741. [Google Scholar] [CrossRef] [Green Version]
- Dassah, E.; Aldersey, H.M.; McColl, M.A.; Davison, C. When I don’t have money to buy the drugs, I just manage—Exploring the lived experience of persons with physical disabilities in accessing primary health care services in rural Ghana. Soc. Sci. Med. 2018, 214, 83–90. [Google Scholar] [CrossRef] [PubMed]
- Mactaggart, I.; Kuper, H.; Murthy, G.V.S.; Sagar, J.; Oye, J.; Polack, S. Assessing health and rehabilitation needs of people with disabilities in Cameroon and India. Disabil. Rehabil. 2015, 38, 1757–1764. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. Training in the Community for People with Disabilities: Guide for Local Supervisors; World Health Organization: Geneva, Switzerland, 1989; p. 70. [Google Scholar]
- Trani, J.-F.; Babulal, G.M.; Bakhshi, P. Development and Validation of the 34-Item Disability Screening Questionnaire (DSQ-34) for Use in Low and Middle Income Countries Epidemiological and Development Surveys. PLoS ONE 2015, 10, e0143610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeMaio, T.; Rothgeb, J. Cognitive interviewing techniques: In the lab and in the field. In Answering Questions. Methodology for Determining Cognitive and Communicative Processes in Survey Research; Schwarz, N., Sudman, S., Eds.; Jossey-Bass, Inc.: San Francsico, CA, USA, 1996; pp. 177–196. [Google Scholar]
- Donabedian, A. Aspects of Medical Care Administration: Specifying Requirements for Health Care; Harvard University Press: Cambridge, MA, USA, 1973. [Google Scholar]
- Andersen, R.M. Revisiting the behavioral model and access to medical care: Does it matter? J. Health Soc. Behav. 1995, 36, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Ameli, O.; Newbrander, W. Contracting for health services: Effects of utilization and quality on the costs of the Basic Package of Health Services in Afghanistan. Bull. World Health Organ. 2008, 86, 920–928. [Google Scholar]
- Kolenikov, S.; Angeles, G. Socioeconomic status measurement with discrete proxy variables: Is principal component analysis: A reliable answer? Rev. Income Wealth 2009, 55, 128–165. [Google Scholar] [CrossRef] [Green Version]
- Stuart, E.A.; Marcus, S.M.; Horvitz-Lennon, M.V.; Gibbons, R.D.; Normand, S.-L.T.; Brown, C.H. Using Non-Experimental Data to Estimate Treatment Effects. Psychiatr. Ann. 2009, 39, 719–728. [Google Scholar] [CrossRef] [Green Version]
- Rosenbaum, P.R.; Rubin, D.B. The central role of the propensity score in observational studies for causal effects. Biometrika 1983, 70, 41–55. [Google Scholar] [CrossRef]
- Austin, P.C. An Introduction to Propensity Score Methods for Reducing the Effects of Confounding in Observational Studies. Multivar. Behav. Res. 2011, 46, 399–424. [Google Scholar] [CrossRef] [Green Version]
- Blundell, R.; Costa-Dias, M. Alternative approaches to evaluation in empirical microeconomics. Port. Econ. J. 2002, 1, 91–115. [Google Scholar] [CrossRef]
- Austin, P.C. Statistical Criteria for Selecting the Optimal Number of Untreated Subjects Matched to Each Treated Subject When Using Many-to-One Matching on the Propensity Score. Am. J. Epidemiol. 2010, 172, 1092–1097. [Google Scholar] [CrossRef]
- Caliendo, M.; Kopeinig, S. Some Practical Guidance for the Implementation of Propensity Score Matching. J. Econ. Surv. 2008, 22, 31–72. [Google Scholar] [CrossRef] [Green Version]
- Rubin, D.B. Using Propensity Scores to Help Design Observational Studies: Application to the Tobacco Litigation. Health Serv. Outcomes Res. Methodol. 2001, 2, 169–188. [Google Scholar] [CrossRef]
- Rubin, D.B. Estimating causal effects of treatments in randomized and nonrandomized studies. J. Educ. Psychol. 1974, 66, 688–701. [Google Scholar] [CrossRef] [Green Version]
- Heckman, J.J.; Ichimura, H.; Todd, P.E. Matching As An Econometric Evaluation Estimator: Evidence from Evaluating a Job Training Programme. Rev. Econ. Stud. 1997, 64, 605–654. [Google Scholar] [CrossRef]
- Iemmi, V.; Kumar, K.S.; Blanchet, K.; Gibson, L.; Hartley, S.; Murthy, G.V.; Patel, V.; Weber, J.; Kuper, H. Community-based rehabilitation for people with physical and mental disabilities in low- and middle-income countries. Cochrane Database Syst. Rev. 2017, 2017, CD010617. [Google Scholar] [CrossRef]
- Trani, J.F.; Bakhshi, P. Profiling and understanding people with disabilities in Afghanistan. In Development Effort in Afghanistan: Is There a Will and a Way? The Case of Disability and Vulnerability; Trani, J.F., Ed.; L’Harmattan: Paris, France, 2011; pp. 73–102. [Google Scholar]
- Trani, J.-F.; Loeb, M. Poverty and disability: A vicious circle? Evidence from Afghanistan and Zambia. J. Int. Dev. 2010, 24, S19–S52. [Google Scholar] [CrossRef] [Green Version]
- Walsh, F.P.; Tickle, A.C. Working towards recovery: The role of employment in recovery from serious mental health problems: A qualitative meta-synthesis. Int. J. Psychosoc. Rehabil. 2013, 17, 35–49. [Google Scholar]
- World Health Organization; World Bank. World Report on Disability; World Health Organization: Geneva, Switzerland, 2011; p. 325. [Google Scholar]
- Parsons, J.A.; Bond, V.A.; Nixon, S.A. ‘Are We Not Human?’ Stories of Stigma, Disability and HIV from Lusaka, Zambia and Their Implications for Access to Health Services. PLoS ONE 2015, 10, e0127392. [Google Scholar] [CrossRef] [Green Version]
- Eide, A.H.; Mannan, H.; Khogali, M.; Van Rooy, G.; Swartz, L.; Munthali, A.; Hem, K.-G.; MacLachlan, M.; Dyrstad, K. Perceived Barriers for Accessing Health Services among Individuals with Disability in Four African Countries. PLoS ONE 2015, 10, e0125915. [Google Scholar] [CrossRef]
- Cerveau, T. Deconstructing myths; facing reality. Understanding social representations of disability in Afghanistan. In Development Efforts in Afghanistan: Is There a Will and a Way? The Case of Disability and Vulnerability; Trani, J.F., Ed.; L’Harmattan: Paris, France, 2011; pp. 103–122. [Google Scholar]
- Maulik, P.K.; Darmstadt, G.L. Childhood disability in low- and middle-income countries: Overview of screening, prevention, services, legislation, and epidemiology. Pediatrics 2007, 120 (Suppl. 1), S1–S55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cooney, G.; Jahoda, A.; Gumley, A.; Knott, F. Young people with intellectual disabilities attending mainstream and segregated schooling: Perceived stigma, social comparison and future aspirations. J. Intellect. Disabil. Res. 2006, 50, 432–444. [Google Scholar] [CrossRef] [PubMed]
- Karangwa, E.; Ghesquière, P.; Devlieger, P. The grassroots community in the vanguard of inclusion: The Rwandan perspective. Int. J. Incl. Educ. 2007, 11, 607–626. [Google Scholar] [CrossRef]
- Green, S.E. What do you mean ‘what’s wrong with her? Stigma and the lives of families of children with disabilities. Soc. Sci. Med. 2003, 57, 1361–1374. [Google Scholar] [CrossRef]
- Trani, J.F.; Ballard, E.; Pena, J. Stigma of persons with disabilities in Afghanistan: Examining the pathways from stereotyping to mental distress. Soc. Sci. Med. 2016, 153, 258–265. [Google Scholar] [CrossRef] [PubMed]
- Graham, L.; Moodley, J.; Selipsky, L. The disability-poverty nexus and the case for a capabilities approach: Evidence from Johannesburg, South Africa. Disabil. Soc. 2013, 28, 324–337. [Google Scholar] [CrossRef]
- Graham, L. Differences in employment and income poverty between people with and without disabilities in South Africa. Alter 2020, 14, 299–317. [Google Scholar] [CrossRef]
- Mont, D.; Cuong, N.V. Disability and poverty in Vietnam. World Bank Econ. Rev. 2011, 25, 323–359. [Google Scholar] [CrossRef]
- Mitra, S.; Posarac, A.; Vick, B. Disability and Poverty in Developing Countries: A Multidimensional Study. World Dev. 2013, 41, 1–18. [Google Scholar] [CrossRef]
- Banks, L.M.; Kuper, H.; Polack, S. Poverty and disability in low- and middle-income countries: A systematic review. PLoS ONE 2017, 12, e0189996. [Google Scholar] [CrossRef] [Green Version]
- Sen, A. The Idea of Justice; The Belknap Press of Harvard University Press: Cambridge, MA, USA, 2009. [Google Scholar]
- Sen, A.K. Development as Freedom; Oxford University Press: Oxford, UK, 1999. [Google Scholar]
- Sen, A.K. Equality of What? In Choice, Welfare and Measurement; Blackwell: Oxford, UK, 1982. [Google Scholar]
- Sen, A.K. Capability and Well-being. In The Quality of Life; Clarendon Press: Oxford, UK, 1993; pp. 30–53. [Google Scholar]
- Mitra, S.; Palmer, M.; Kim, H.; Mont, D.; Groce, N. Extra costs of living with a disability: A review and agenda for research. Disabil. Health J. 2017, 10, 475–484. [Google Scholar] [CrossRef]
- Trani, J.F.; Kuhlberg, J.; Cannings, T.; Chakkal, D. Multidimensional poverty in Afghanistan: Who are the poorest of the poor? Oxf. Dev. Stud. 2016, 44, 220–245. [Google Scholar] [CrossRef]
- Chronister, J.; Chou, C.-C.; Liao, H.-Y. The role of stigma coping and social support in mediating the effect of societal stigma on internalized stigma, mental health recovery, and quality of life among people with serious mental illness. J. Community Psychol. 2013, 41, 582–600. [Google Scholar] [CrossRef]
- Biggeri, M.; Deepak, S.; Mauro, V.; Trani, J.-F.; Kumar, J.; Ramasamy, P. Do community-based rehabilitation programmes promote the participation of persons with disabilities? A case control study from Mandya District, in India. Disabil. Rehabil. 2013, 36, 1508–1517. [Google Scholar] [CrossRef]
- Pinilla-Roncancio, M. The reality of disability: Multidimensional poverty of people with disability and their families in Latin America. Disabil. Health J. 2018, 11, 398–404. [Google Scholar] [CrossRef]
- Pinilla-Roncancio, M.; Mactaggart, I.; Kuper, H.; Dionicio, C.; Naber, J.; Murthy, G.V.S.; Polack, S. Multidimensional poverty and disability: A case control study in India, Cameroon, and Guatemala. SSM-Popul. Health 2020, 11, 100591. [Google Scholar] [CrossRef]
- Groce, N.; Kett, M.; Lang, R.; Trani, J.-F. Disability and Poverty: The need for a more nuanced understanding of implications for development policy and practice. Third World Q. 2011, 32, 1493–1513. [Google Scholar] [CrossRef]
- Dupree, N. The historical and cultural context of disability in Afghanistan. In Development Effort in Afghanistan: Is There a Will and a Way? The Case of Disability and Vulnerability; Trani, J.F., Ed.; L’Harmattan: Paris, France, 2011; p. 284. [Google Scholar]
- Mannell, J.; Grewal, G.; Ahmad, L.; Ahmad, A. A Qualitative Study of Women’s Lived Experiences of Conflict and Domestic Violence in Afghanistan. Violence against Women 2020, 27, 1862–1878. [Google Scholar] [CrossRef]
- Trani, J.F.; Bakhshi, P.; Rolland, C. Capabilities, Perception of Well-being and Development Effort: Some Evidence from Afghanistan. Oxf. Dev. Stud. 2011, 39, 403–426. [Google Scholar] [CrossRef] [Green Version]
- Trani, J.F.; Bakhshi, P. Vulnerability and mental health in afghanistan: Looking beyond war exposure. Transcult. Psychiatry 2013, 50, 108–139. [Google Scholar] [CrossRef]
- Swedish Committee for Afghanistan. People with Disabilities. 2022. Available online: https://swedishcommittee.org/our-work/people-disabilities (accessed on 28 April 2022).







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control (n = 1133) | Treatment (n = 1861) | Overall (n = 2994) | |
|---|---|---|---|
| Gender | |||
| Male | 701 (62%) | 1159 (62%) | 1860 (62%) |
| Female | 431 (38%) | 702 (38%) | 1133 (38%) |
| Age (years) | |||
| Mean (SD) | 31 (21) | 15 (15) | 21 (19) |
| Ethnicity | |||
| Pashtun | 339 (30%) | 669 (36%) | 1008 (34%) |
| Tajik | 345 (30%) | 749 (40%) | 1094 (37%) |
| Other | 274 (24%) | 429 (23%) | 703 (23%) |
| Disability | |||
| Physical | 567 (50%) | 1307 (70%) | 1874 (63%) |
| Sensory | 178 (16%) | 230 (12%) | 408 (14%) |
| Intellectual | 70 (6%) | 176 (9%) | 246 (8%) |
| Mental Illness | 45 (4%) | 7 (0%) | 52 (2%) |
| Multiple | 98 (9%) | 130 (7%) | 228 (8%) |
| Disability Cause | |||
| Birth | 338 (30%) | 1118 (60%) | 1456 (49%) |
| Accident | 164 (14%) | 242 (13%) | 406 (14%) |
| Disease | 296 (26%) | 336 (18%) | 632 (21%) |
| Conflict-related Injury | 117 (10%) | 94 (5%) | 211 (7%) |
| Other | 217 (19%) | 71 (4%) | 288 (10%) |
| Education | |||
| No formal education | 780 (69%) | 1547 (83%) | 2327 (78%) |
| Some formal education | 177 (16%) | 295 (16%) | 472 (16%) |
| Assets | |||
| 20% poorest | 341 (30%) | 231 (12%) | 572 (19%) |
| 20–80% | 532 (47%) | 1183 (64%) | 1715 (57%) |
| 20% richest | 139 (12%) | 433 (23%) | 572 (19%) |
| Electricity in Village | |||
| No | 264 (23%) | 184 (10%) | 448 (15%) |
| Yes | 868 (77%) | 1677 (90%) | 2545 (85%) |
| Time to Reach School (minutes) | |||
| Mean (SD) | 19 (12) | 17 (10) | 18 (11) |
| Time to Reach Healthcare (minutes) | |||
| Mean (SD) | 30 (24) | 25 (18) | 27 (21) |
| Control n (%) | Treatment n (%) | p Value | |
|---|---|---|---|
| Access to services | |||
| Physical Therapy | 100 (8.83) | 1514 (81.35) | 0 < 0.001 |
| Assistive Service | 102 (9.01) | 1001 (53.80) | 0 < 0.001 |
| Employment Service | 212 (41.57) | 253 (48.47) | 0.026 |
| Education Service | 22 (8.87) | 391 (6306) | 0 < 0.001 |
| Advocacy Service | 158 (13.96) | 1578 (84.79) | 0 < 0.001 |
| Unmet needs | |||
| Healthcare | 496 (56.56) | 444 (33.66) | 0 < 0.001 |
| Education (6–17) | 186 (75) | 459 (74.51) | 0.882 |
| Housing | 205 (23.38) | 209 (15.88) | 0 < 0.001 |
| Employment (15–61) | 298 (58.43) | 269 (51.53) | 0.026 |
| Pension (>17) | 492 (56.1) | 545 (41.44) | 0 < 0.001 |
| Income (>17) | 412 (68.9) | 331 (65.81) | 0.275 |
| Family respect | 160 (18.24) | 191 (14.48) | 0.018 |
| Community respect | 388 (44.24) | 419 (31.77) | 0 < 0.001 |
| Marriage | 209 (31.67) | 266 (43.89) | 0 < 0.001 |
| Physical Therapy | Assistive Technology | Employment | Education | Advocacy | |
|---|---|---|---|---|---|
| β | β | β | β | β | |
| Endline (ref.: Baseline) | 0.087 *** | 0.105 *** | 0.043 | 0.027 | 0.105 *** |
| (0.014) | (0.024) | (0.035) | (0.024) | (0.017) | |
| Treatment (ref.: Control) | 0.949 *** | 0.170 ** | 0.316 *** | 0.037 | 0.300 *** |
| (0.032) | (0.054) | (0.079) | (0.055) | (0.038) | |
| Female (ref.: Male) | 0.021 | −0.068 *** | 0.011 | −0.055 ** | 0.012 |
| (0.011) | (0.019) | (0.026) | (0.020) | (0.012) | |
| Tajik (ref.: Pashtun) | −0.022 | −0.012 | 0.002 | −0.046 * | −0.005 |
| (0.012) | (0.020) | (0.030) | (0.021) | (0.014) | |
| Other ethnicity (ref.: Pashtun) | −0.042 ** | 0.008 | −0.008 | −0.030 | 0.024 |
| (0.013) | (0.022) | (0.033) | (0.022) | (0.016) | |
| Age | −0.001 | 0.000 | −0.005 | −0.003 *** | −0.001 |
| (0.000) | (0.001) | (0.004) | (0.001) | (0.000) | |
| Accident (ref.: Birth) | 0.005 | −0.022 | −0.105 * | −0.062 * | −0.002 |
| (0.016) | (0.027) | (0.042) | (0.027) | (0.019) | |
| Disease (ref.: Birth) | 0.026 | −0.022 | −0.036 | −0.076 ** | −0.003 |
| (0.015) | (0.026) | (0.035) | (0.026) | (0.017) | |
| War related (ref.: Birth) | 0.037 | 0.087 ** | −0.196 * | 0.033 | 0.020 |
| (0.019) | (0.032) | (0.099) | (0.031) | (0.025) | |
| Other cause (ref.: Birth) | −0.013 | −0.108 * | −0.105 | −0.068 | −0.039 |
| (0.032) | (0.053) | (0.073) | (0.044) | (0.033) | |
| Education (ref.: No education) | 0.011 | 0.035 | 0.167 *** | 0.045 * | 0.029 |
| (0.013) | (0.022) | (0.030) | (0.022) | (0.016) | |
| Assets 20–80% (ref.: 20% poorest) | −0.001 | 0.002 | −0.036 | 0.028 | −0.003 |
| (0.013) | (0.022) | (0.033) | (0.023) | (0.015) | |
| Assets 20% richest (ref.: 20% poorest) | 0.028 | 0.076 ** | −0.019 | 0.001 | 0.023 |
| (0.016) | (0.027) | (0.042) | (0.029) | (0.019) | |
| Electricity in village (ref.: No electricity) | −0.004 | 0.063 ** | 0.033 | 0.059 * | −0.081 *** |
| (0.014) | (0.023) | (0.033) | (0.025) | (0.016) | |
| Time to reach to school | −0.002 *** | −0.001 | −0.000 | 0.003 *** | −0.003 *** |
| (0.000) | (0.001) | (0.001) | (0.001) | (0.001) | |
| Time to reach healthcare facility | 0.000 | −0.000 | −0.001 | 0.001 | −0.000 |
| (0.000) | (0.000) | (0.001) | (0.001) | (0.000) | |
| Wave time × Treatment | −0.052 * | 0.170 *** | 0.124 * | 0.184 *** | 0.203 *** |
| (0.020) | (0.034) | (0.050) | (0.035) | (0.024) | |
| N. obs. | 2164 | 2164 | 932 | 1656 | 3620 |
| R squared | 0.780 | 0.282 | 0.345 | 0.256 | 0.466 |
| F statistic | 448.707 | 49.633 | 28.295 | 33.114 | 185.046 |
| p value | 0.000 | 0.000 | 0.000 | 0.000 | 0.000 |
| Health | Education | Housing | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Variable | OR 1 | 95% CI 1 | p-Value | OR 1 | 95% CI 1 | p-Value | OR 1 | 95% CI 1 | p-Value |
| Group | |||||||||
| Control | Reference | Reference | Reference | ||||||
| Treatment | 0.51 | 0.40, 0.66 | <0.001 | 1.02 | 0.66, 1.58 | >0.9 | 0.69 | 0.51, 0.93 | 0.016 |
| Gender | |||||||||
| Male | |||||||||
| Female | 1.28 | 1.01, 1.62 | 0.045 | 0.75 | 0.48, 1.16 | 0.2 | 1.16 | 0.87, 1.54 | 0.3 |
| Ethnicity | |||||||||
| Pashtun | Reference | Reference | Reference | ||||||
| Tajik | 1.10 | 0.85, 1.43 | 0.5 | 0.70 | 0.42, 1.17 | 0.2 | 1.12 | 0.81, 1.54 | 0.5 |
| Other | 0.79 | 0.59, 1.07 | 0.13 | 0.57 | 0.33, 0.99 | 0.044 | 1.06 | 0.74, 1.50 | 0.8 |
| Age (years) | 1.00 | 0.99, 1.01 | 0.9 | 0.92 | 0.87, 0.97 | 0.004 | 1.00 | 0.99, 1.01 | 0.5 |
| Disability | |||||||||
| Physical | Reference | Reference | Reference | ||||||
| Sensory | 0.71 | 0.51, 0.98 | 0.037 | 1.41 | 0.81, 2.47 | 0.2 | 0.73 | 0.49, 1.09 | 0.13 |
| Intellectual | 1.20 | 0.80, 1.79 | 0.4 | 1.71 | 0.91, 3.28 | 0.10 | 0.79 | 0.46, 1.30 | 0.4 |
| Mental Illness | 1.81 | 0.87, 4.02 | 0.12 | 0.65 | 0.28–1.46 | 0.3 | 0.55 | 0.20, 1.31 | 0.2 |
| Associated | 1.43 | 0.94, 2.19 | 0.10 | 2.24 | 1.09, 4.92 | 0.035 | 0.75 | 0.43, 1.23 | 0.3 |
| Disability Cause | |||||||||
| Birth | Reference | Reference | Reference | ||||||
| Accident | 0.75 | 0.51, 1.10 | 0.14 | 1.00 | 0.49, 2.10 | >0.9 | 1.05 | 0.66, 1.65 | 0.8 |
| Disease | 0.90 | 0.65, 1.26 | 0.6 | 0.90 | 0.51, 1.64 | 0.7 | 1.37 | 0.92, 2.03 | 0.12 |
| War related | 0.61 | 0.38, 0.98 | 0.041 | 0.62 | 0.14, 2.69 | 0.5 | 1.51 | 0.88, 2.55 | 0.13 |
| Other | 1.05 | 0.54, 2.04 | 0.9 | 0.25 | 0.06, 0.86 | 0.034 | 2.08 | 1.03, 4.06 | 0.035 |
| Education | |||||||||
| No formal education | Reference | Reference | Reference | ||||||
| Formal Education | 0.54 | 0.39, 0.74 | <0.001 | 0.40 | 0.24, 0.65 | <0.001 | 1.21 | 0.84, 1.72 | 0.3 |
| Assets | |||||||||
| 20% Poorest | Reference | Reference | Reference | ||||||
| 20–40% | 0.75 | 0.53, 1.05 | 0.093 | 1.89 | 0.97, 3.72 | 0.061 | 0.72 | 0.49, 1.06 | 0.10 |
| 40–60% | 0.61 | 0.42, 0.86 | 0.005 | 0.99 | 0.51, 1.90 | >0.9 | 0.58 | 0.38, 0.88 | 0.010 |
| 60–80% | 0.44 | 0.30, 0.64 | <0.001 | 0.96 | 0.49, 1.89 | >0.9 | 0.55 | 0.35, 0.85 | 0.008 |
| 20% Richest | 0.57 | 0.40, 0.82 | 0.002 | 1.51 | 0.75, 3.04 | 0.2 | 0.48 | 0.31, 0.74 | 0.001 |
| Electricity in Village | |||||||||
| No Electricity | Reference | Reference | Reference | ||||||
| Electricity | 1.22 | 0.90, 1.65 | 0.2 | 0.73 | 0.42, 1.24 | 0.2 | 1.09 | 0.76, 1.58 | 0.7 |
| Time to School (minutes) | 1.01 | 1.00, 1.03 | 0.013 | 1.00 | 0.98, 1.02 | >0.9 | 1.00 | 0.99, 1.01 | 0.7 |
| Time to Healthcare (minutes) | 1.02 | 1.01, 1.02 | <0.001 | 1.00 | 0.99, 1.01 | 0.7 | 1.00 | 1.00, 1.01 | 0.2 |
| Employment | Income | Pension | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Variable | OR 1 | 95% CI 1 | p-Value | OR 1 | 95% CI 1 | p-Value | OR 1 | 95% CI 1 | p-Value |
| Treatment | |||||||||
| Control | — | — | — | — | — | — | |||
| Treatment | 0.74 | 0.54, 1.01 | 0.062 | 0.55 | 0.38, 0.80 | 0.002 | 0.62 | 0.44, 0.88 | 0.007 |
| Gender | |||||||||
| Male | — | — | — | — | — | — | |||
| Female | 0.82 | 0.59, 1.15 | 0.2 | 0.59 | 0.40, 0.86 | 0.006 | 0.74 | 0.51, 1.06 | 0.10 |
| Ethnicity | |||||||||
| Pashtun | — | — | — | — | — | — | |||
| Tajik | 1.67 | 1.17, 2.41 | 0.005 | 1.70 | 1.14, 2.55 | 0.009 | 0.68 | 0.46, 1.00 | 0.048 |
| Other | 1.10 | 0.75, 1.62 | 0.6 | 1.25 | 0.81, 1.93 | 0.3 | 0.36 | 0.23, 0.54 | <0.001 |
| Age (years) | 0.97 | 0.96, 0.98 | <0.001 | 0.97 | 0.96, 0.98 | <0.001 | 1.00 | 0.99, 1.01 | 0.6 |
| Disability | |||||||||
| Physical | — | — | — | — | — | — | |||
| Sensory | 1.06 | 0.66, 1.71 | 0.8 | 1.39 | 0.81, 2.44 | 0.2 | 1.09 | 0.65, 1.84 | 0.7 |
| Intellectual | 1.22 | 0.58, 2.66 | 0.6 | 1.23 | 0.44, 3.82 | 0.7 | 1.93 | 0.71, 5.87 | 0.2 |
| Mental Illness | 1.12 | 0.43, 3.04 | 0.8 | 0.68 | 0.25, 1.99 | 0.5 | 0.59 | 0.21, 1.60 | 0.3 |
| Multiple | 0.69 | 0.36, 1.33 | 0.3 | 0.58 | 0.27, 1.27 | 0.2 | 0.90 | 0.41, 2.00 | 0.8 |
| Disability Cause | |||||||||
| Birth | — | — | — | — | — | — | |||
| Accident | 1.02 | 0.64, 1.65 | >0.9 | 1.71 | 0.97, 3.03 | 0.062 | 1.35 | 0.78, 2.32 | 0.3 |
| Disease | 1.20 | 0.76, 1.89 | 0.4 | 1.25 | 0.74, 2.12 | 0.4 | 0.96 | 0.58, 1.60 | 0.9 |
| Conflict-related | 1.09 | 0.63, 1.89 | 0.8 | 1.00 | 0.55, 1.82 | >0.9 | 0.63 | 0.35, 1.11 | 0.11 |
| Other | 0.64 | 0.25, 1.61 | 0.3 | 1.21 | 0.49, 3.08 | 0.7 | 0.54 | 0.22, 1.29 | 0.2 |
| Education | |||||||||
| No formal education | — | — | — | — | — | — | |||
| Formal Education | 0.77 | 0.53, 1.12 | 0.2 | 0.96 | 0.62, 1.50 | 0.9 | 0.91 | 0.60, 1.38 | 0.7 |
| Assets | |||||||||
| 120% Poorest | — | — | — | — | — | — | |||
| 20–40% | 0.76 | 0.47, 1.24 | 0.3 | 0.76 | 0.42, 1.35 | 0.3 | 0.90 | 0.52, 1.55 | 0.7 |
| 40–60% | 1.18 | 0.71, 1.94 | 0.5 | 0.90 | 0.50, 1.63 | 0.7 | 1.27 | 0.73, 2.21 | 0.4 |
| 60–80% | 0.82 | 0.49, 1.37 | 0.5 | 1.00 | 0.54, 1.82 | >0.9 | 1.01 | 0.57, 1.76 | >0.9 |
| 20% Richest | 0.79 | 0.48, 1.29 | 0.3 | 0.56 | 0.31, 0.99 | 0.048 | 0.67 | 0.38, 1.16 | 0.2 |
| Electricity in Village | |||||||||
| No Electricity | — | — | — | — | — | — | |||
| Electricity | 0.71 | 0.44, 1.13 | 0.2 | 1.01 | 0.59, 1.70 | >0.9 | 1.20 | 0.72, 1.98 | 0.5 |
| Time to School (minutes) | 1.00 | 0.99, 1.02 | 0.7 | 1.01 | 0.99, 1.03 | 0.2 | 1.01 | 0.99, 1.03 | 0.4 |
| Time to Healthcare (minutes) | 1.01 | 1.00, 1.01 | 0.2 | 1.01 | 1.00, 1.02 | 0.2 | 1.01 | 1.00, 1.02 | 0.044 |
| Family Respect | Community Respect | Marriage | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Characteristics | OR 1 | 95% CI 1 | p-Value | OR 1 | 95% CI 1 | p-Value | OR 1 | 95% CI 1 | p-Value |
| Group | |||||||||
| Control | Reference | Reference | Reference | ||||||
| Treatment | 0.65 | 0.46, 0.90 | 0.011 | 0.44 | 0.34, 0.58 | <0.001 | 0.63 | 0.47, 0.83 | 0.001 |
| Gender | |||||||||
| Male | Reference | Reference | Reference | ||||||
| Female | 1.28 | 0.94, 1.75 | 0.12 | 1.02 | 0.80, 1.31 | 0.9 | 0.98 | 0.74, 1.28 | 0.9 |
| Ethnicity | |||||||||
| Pashtun | Reference | Reference | Reference | ||||||
| Tajik | 1.18 | 0.83, 1.67 | 0.4 | 1.46 | 1.11, 1.92 | 0.007 | 1.18 | 0.87, 1.59 | 0.3 |
| Other | 0.89 | 0.59, 1.33 | 0.6 | 1.27 | 0.94, 1.73 | 0.12 | 1.55 | 1.11, 2.15 | 0.009 |
| Age (years) | 0.98 | 0.97, 0.99 | 0.006 | 0.98 | 0.98, 0.99 | <0.001 | 0.98 | 0.97, 0.99 | <0.001 |
| Disability | |||||||||
| Physical | Reference | Reference | Reference | ||||||
| Sensory | 0.82 | 0.51, 1.28 | 0.4 | 1.03 | 0.73, 1.43 | 0.9 | 1.16 | 0.81, 1.66 | 0.4 |
| Intellectual | 2.08 | 1.30, 3.29 | 0.002 | 2.66 | 1.75, 4.07 | <0.001 | 1.11 | 0.71, 1.72 | 0.6 |
| Mental Illness | 1.97 | 0.82, 4.42 | 0.11 | 1.90 | 0.91, 3.99 | 0.087 | 1.29 | 0.54, 2.82 | 0.5 |
| Associated | 2.33 | 1.44, 3.70 | <0.001 | 2.05 | 1.35, 3.12 | <0.001 | 1.10 | 0.69, 1.72 | 0.7 |
| Disability Cause | |||||||||
| Birth | Reference | Reference | Reference | ||||||
| Accident | 0.51 | 0.28, 0.90 | 0.026 | 0.73 | 0.49, 1.09 | 0.13 | 0.70 | 0.45, 1.08 | 0.11 |
| Disease | 0.90 | 0.57, 1.39 | 0.6 | 0.66 | 0.46, 0.93 | 0.019 | 0.84 | 0.58, 1.22 | 0.4 |
| Conflict-related | 0.41 | 0.16, 0.91 | 0.041 | 0.46 | 0.26, 0.77 | 0.004 | 0.79 | 0.45, 1.35 | 0.4 |
| Other cause | 0.77 | 0.27, 1.88 | 0.6 | 1.00 | 0.49, 2.03 | >0.9 | 1.86 | 0.88, 3.86 | 0.10 |
| Education | |||||||||
| No formal education | Reference | Reference | Reference | ||||||
| Formal Education | 0.37 | 0.20, 0.63 | <0.001 | 0.31 | 0.22, 0.45 | <0.001 | 2.88 | 2.10, 3.95 | <0.001 |
| Assets | |||||||||
| 20% Poorest | Reference | Reference | Reference | ||||||
| 20–40% | 0.68 | 0.44, 1.05 | 0.082 | 0.88 | 0.62, 1.25 | 0.5 | 0.65 | 0.44, 0.96 | 0.032 |
| 40–60% | 0.51 | 0.31, 0.83 | 0.007 | 0.69 | 0.47, 1.00 | 0.049 | 0.96 | 0.64, 1.42 | 0.8 |
| 60–80% | 0.56 | 0.34, 0.92 | 0.023 | 0.65 | 0.44, 0.96 | 0.033 | 0.97 | 0.64, 1.46 | 0.9 |
| 20% Richest | 0.70 | 0.44, 1.11 | 0.13 | 0.91 | 0.62, 1.31 | 0.6 | 0.89 | 0.59, 1.33 | 0.6 |
| Electricity in Village | |||||||||
| No Electricity | Reference | Reference | Reference | ||||||
| Electricity | 0.90 | 0.61, 1.36 | 0.6 | 1.00 | 0.73, 1.37 | >0.9 | 0.77 | 0.55, 1.07 | 0.12 |
| Time to School (minutes) | 1.02 | 1.00, 1.03 | 0.027 | 1.00 | 0.99, 1.01 | 0.7 | 1.00 | 0.99, 1.01 | >0.9 |
| Time to Healthcare (minutes) | 1.00 | 0.99, 1.01 | 0.5 | 1.00 | 1.00, 1.01 | 0.5 | 1.00 | 0.99, 1.00 | 0.6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Trani, J.-F.; Pitzer, K.A.; Vasquez Escallon, J.; Bakhshi, P. Access to Services from Persons with Disabilities in Afghanistan: Is Community Based Rehabilitation Making a Difference? Int. J. Environ. Res. Public Health 2022, 19, 6341. https://doi.org/10.3390/ijerph19106341
Trani J-F, Pitzer KA, Vasquez Escallon J, Bakhshi P. Access to Services from Persons with Disabilities in Afghanistan: Is Community Based Rehabilitation Making a Difference? International Journal of Environmental Research and Public Health. 2022; 19(10):6341. https://doi.org/10.3390/ijerph19106341
Chicago/Turabian StyleTrani, Jean-Francois, Kyle A. Pitzer, Juanita Vasquez Escallon, and Parul Bakhshi. 2022. "Access to Services from Persons with Disabilities in Afghanistan: Is Community Based Rehabilitation Making a Difference?" International Journal of Environmental Research and Public Health 19, no. 10: 6341. https://doi.org/10.3390/ijerph19106341
APA StyleTrani, J. -F., Pitzer, K. A., Vasquez Escallon, J., & Bakhshi, P. (2022). Access to Services from Persons with Disabilities in Afghanistan: Is Community Based Rehabilitation Making a Difference? International Journal of Environmental Research and Public Health, 19(10), 6341. https://doi.org/10.3390/ijerph19106341