
The Role of Physical Activity Status in the Relationship between Obesity and Carotid Intima-Media Thickness (CIMT) in Urban South African Teachers: The SABPA Study

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
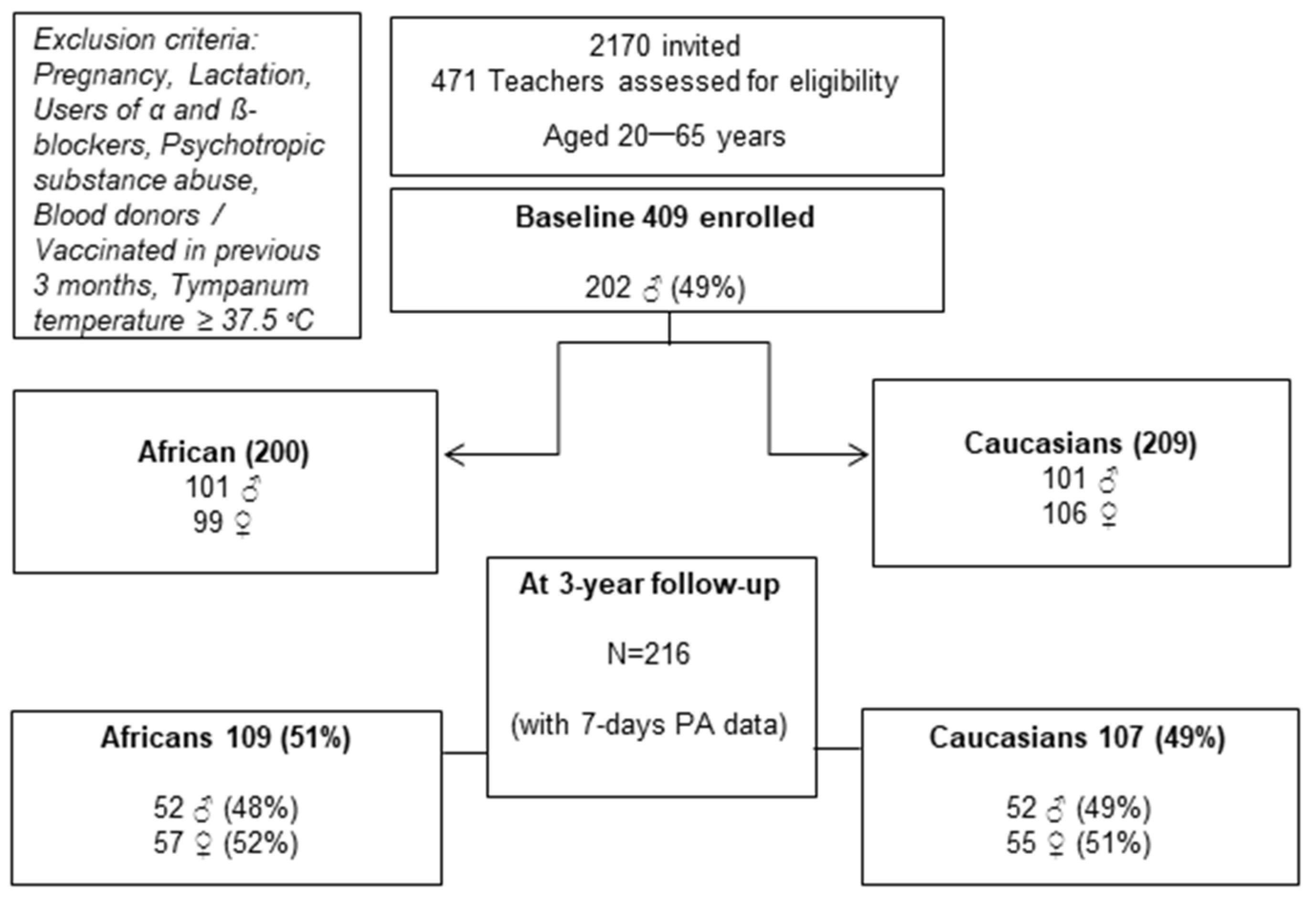
2.2. Study Population and Sample
2.3. Anthropometric Measures
2.4. Objectively Measured Physical Activity
2.5. Subclinical Atherosclerosis
2.5.1. Blood Pressure
2.5.2. Biochemical Analysis
2.6. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Blair, S.N. Physical inactivity: The biggest public health problem of the 21st century. Br. J. Sports Med. 2009, 43, 1–2. [Google Scholar] [PubMed]
- WHO (World Health Organization). Prevalence of Insufficient Physical Activity among Adults. 2018. Available online: http://apps.who.int/gho/data/view.main.2463?lang=en (accessed on 16 July 2019).
- Guthold, R.; Stevens, G.A.; Riley, L.M.; Bull, F.C. Worldwide trends in insufficient physical activity from 2001 to 2016: A pooled analysis of 358 population-based surveys. Lancet Glob. Health 2018, 6, 1077–1086. [Google Scholar] [CrossRef] [Green Version]
- WHO (World Health Organisation). Global Recommendations on Physical Activity for Health. 2010. Available online: https://apps.who.int/iris/bitstream/handle/10665/44399/9789241599979_eng.pdf;jsessionid=04C423D4CAE804D52D889A6E370BA2ED?sequence=1 (accessed on 16 July 2019).
- Ainsworth, B.E.; Haskell, W.L.; Herrman, S.D.; Meckes, N.; Bassett, D.R.; Tudor-Locke, C.; Greer, J.L.; Vezina, J.; Whitt-Glover, M.C.; Leon, A.S. Compendium of physical activities: A second update of codes and MET values. Med. Sci. Sports Exerc. 2011, 43, 1575–1581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bastien, M.; Poirier, P.; Lemieux, I.; Després, J.-P. Overview of Epidemiology and Contribution of Obesity to Cardiovascular Disease. Prog. Cardiovasc. Dis. 2014, 56, 369–381. [Google Scholar] [CrossRef] [PubMed]
- WHO (World Health Organization). Global Health Observatory Data Repository: Prevalence of Overweight among Adults, BMI ≥ 25. (2017a). Available online: http://apps.who.int/gho/data/view.main.BMI25Cv?lang=en (accessed on 17 September 2019).
- WHO (World Health Organization). Global Health Observatory Data Repository: Prevalence of Obesity among Adults, BMI ≥ 30. (2017b). Available online: http://apps.who.int/gho/data/view.main.BMI30Cv?lang=en (accessed on 17 September 2019).
- Laurence, E.C.; Volmink, J.; Esterhuizen, T.M.; Dalal, S.; Holmes, M.D. Risk of cardiovascular disease among teachers in Cape Town: Findings of the South African PaCT pilot study. S. Afr. Med. J. 2016, 106, 996–1001. [Google Scholar] [CrossRef] [Green Version]
- Jin, Y.; Kim, D.; Cho, J.; Lee, I.; Choi, K.; Kang, H. Association between obesity and carotid intima-media thickness in Korean office workers: The mediating effect of physical activity. Biomed. Res. Int. 2018, 2018, 4285038. [Google Scholar] [CrossRef] [Green Version]
- Touboul, P.-J.; Hennerici, M.G.; Meairs, S.; Adams, H.; Amarenco, P.; Bornstein, N.; Csiba, L.; Desvarieux, M.; Ebrahim, S.; Fatar, M.; et al. Mannheim carotid intima-media thickness consensus (2004–2006). Cerebrovasc. Dis. 2007, 23, 75–80. [Google Scholar] [CrossRef]
- Hamer, M.; Von Känel, R.; Reimann, M.; Malan, N.T.; Schutte, A.E.; Huisman, H.W.; Malan, L. Progression of cardiovascular risk factors in Black Africans: 3 year follow up of the SABPA cohort study. Atherosclerosis 2015, 238, 52–54. [Google Scholar] [CrossRef] [Green Version]
- Lakka, T.A.; Lakka, H.M.; Salonen, R.; Kaplan, G.A.; Salonen, J.T. Abdominal obesity is associated with accelerated progression of carotid atherosclerosis in men. Atherosclerosis 2001, 154, 497–504. [Google Scholar] [CrossRef]
- Tankó, L.B.; Bagger, Y.Z.; Qin, G.; Alexandersen, P.; Larsen, P.J.; Christiansen, C. Enlarged waist combined with elevated triglycerides is a strong predictor of accelerated atherogenesis and related cardiovascular mortality in postmenopausal women. Circulation 2005, 111, 1883–1890. [Google Scholar] [CrossRef] [Green Version]
- Lo, J.; Dolan, S.E.; Kanter, J.R.; Hemphill, L.C.; Connelly, J.M.; Lees, R.S.; Grinspoon, S.K. Effects of obesity, body composition, and adiponectin on carotid intima-media thickness in healthy women. J. Clin. Endocrinol. Metab. 2006, 91, 1677–1682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kotsis, V.T.; Stabouli, S.V.; Papamichael, C.M.; Zakopoulos, N.A. Impact of obesity in intima-media thickness of carotid arteries. Obesity 2006, 14, 1708–1715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sturm, W.; Sandhofer, A.; Engl, J.; Laimer, M.; Molnar, C.; Kaser, S.; Weiss, H.; Tilg, H.; Ebenbichler, C.F.; Patsch, J.R. Influence of visceral obesity and liver fat on vascular structure and function in obese subjects. Obesity 2009, 17, 1783–1788. [Google Scholar] [CrossRef] [PubMed]
- Ortega-Loubon, C.; Fernández-Molina, M.; Singh, G.; Correa, R. Obesity and its cardiovascular effects. Diabetes/Metab. Res. Rev. 2019, 35, e3135. [Google Scholar] [CrossRef] [PubMed]
- Arnold, M.; Linden, A.; Clarke, R.; Guo, Y.; Du, H.; Bian, Z.; Wan, E.; Yang, M.; Wang, L.; Chen, Y.; et al. Carotid intima-media thickness but not carotid artery plaque in healthy individuals is linked to lean body mass. J. Am. Heart Assoc. 2019, 8, e011919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kadoglou, N.P.E.; Iliadis, F.; Liapis, C.D. Exercise and Carotid Atherosclerosis. Eur. J. Vasc. Endovasc. Surg. 2008, 35, 264–272. [Google Scholar] [CrossRef] [Green Version]
- Byrkjeland, R.; Stensaeth, K.-H.; Anderssen, S.; Njerve, I.U.; Arnesen, H.; Seljeflot, I.; Solheim, S. Effects of exercise training on carotid intima-media thickness in patients with type 2 diabetes and coronary artery disease. Cardiovasc. Diabetol. 2016, 15, 13. [Google Scholar] [CrossRef]
- Parsons, T.J.; Sartini, C.; Ellins, E.A.; Halcox, J.P.J.; Smith, K.E.; Ash, S.; Lennon, L.T.; Wannamethee, S.G.; Lee, I.-M.; Whincup, P.H.; et al. Objectively measured physical activity, sedentary time and subclinical vascular disease: A cross-sectional study in older British men. Prev. Med. 2016, 89, 194–199. [Google Scholar] [CrossRef] [Green Version]
- Malan, L.; Hamer, M.; Frasure-Smith, N.; Steyn, H.S.; Malan, N.T. Cohort profile: Sympathetic activity and ambulatory blood pressure in Africans (SABPA) prospective cohort study. Int. J. Epidemiol. 2015, 44, 1814–1822. [Google Scholar] [CrossRef] [Green Version]
- O’Rourke, M. Arterial stiffness, systolic blood pressure, and logical treatment of arterial hypertension. Hypertension 1990, 15, 339–347. [Google Scholar] [CrossRef] [Green Version]
- Countouris, M.E.; Schwarz, E.B.; Rossiter, B.C.; Althouse, A.D.; Berlacher, K.L.; Jeyabalan, A.; Catov, J.M. Effects of lactation on postpartum blood pressure among women with gestational hypertension and preeclampsia. Am. J. Obstet. Gynecol. 2016, 215, e1–e8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stewart, A.; Marfell-Jones, M.; Olds, T.; De Ridder, J.H. International Standard for Anthropometric Assessment, 3rd ed.; ISAK: Lower Hutt, New Zealand, 2011. [Google Scholar]
- Botha, J.; De Ridder, J.H.; Potgieter, J.C.; Steyn, H.S.; Malan, L. Structural vascular disease in Africans: Performance of ethnic-specific waist circumference cut points using logistic regression and neural network analyses: The SABPA study. Exp. Clin. Endocrinol. Diabetes 2013, 121, 515–520. [Google Scholar] [CrossRef] [PubMed]
- Alberti, K.G.M.M.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.-C.; James, W.P.T.; Loria, C.M.; Smith, S.C. Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ashwell, M.; Hsieh, S.D. Six reasons why the waist-to-height ratio is a rapid and effective global indicator for health risks of obesity and how its use could simplify the international public health message on obesity. Int. J. Food Sci. Nutr. 2005, 56, 303–307. [Google Scholar] [CrossRef]
- Riebe, D.; Ehrman, J.K.; Liguori, G.; Magal, M. (Eds.) ACSM’s Guidelines for Exercise Testing and Prescription, 10th ed.; Wolhuters Kluwer: Philadelphia, PA, USA, 2018. [Google Scholar]
- Hamer, M.; Bruwer, E.J.; De Ridder, J.H.; Swanepoel, M.; Kengne, A.P.; Cockeran, M.; Malan, L. The association between seven-day objectively measured habitual physical activity and 24 h ambulatory blood pressure: The SABPA study. J. Hum. Hypertens. 2017, 31, 409–414. [Google Scholar] [CrossRef]
- Brage, S.; Brage, N.; Franks, P.W.; Ekelund, U.; Wong, M.Y.; Andersen, L.B.; Froberg, K.; Wareham, N.J. Branched equation modeling of simultaneous accelerometry and heart rate monitoring improves estimate of directly measured physical activity energy expenditure. J. Appl. Physiol. 2004, 96, 343–351. [Google Scholar] [CrossRef] [Green Version]
- Westerterp, K.R. Control of energy expenditure in humans. Eur. J. Clin. Nutr. 2017, 71, 340–344. [Google Scholar] [CrossRef]
- Wendelhag, I.; Liang, Q.; Gustavsson, T.; Wikstrand, J. A new automated computerized analyzing system simplifies readings and reduces the variability in ultrasound measurement of intima-media thickness. Stroke 1997, 28, 2195–2200. [Google Scholar] [CrossRef]
- Liang, Q.; Wendelhag, I.; Wikstrand, J.; Gustavsson, T. A multiscale dynamic programming procedure for boundary detection in ultrasonic artery images. IEEE Trans. Med. Imaging 2000, 19, 127–142. [Google Scholar] [CrossRef]
- Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.L.; Cooney, M.-T.; Corrà, U.; Cosyns, B.; Deaton, C.; et al. European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice. Eur. J. Prev. Cardiol. 2016, 23, NP1–NP96. [Google Scholar] [CrossRef] [Green Version]
- Ridker, P.M. Cardiology Patient Page. C-reactive protein: A simple test to help predict risk of heart attack and stroke. Circulation 2003, 108, e81–e85. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.W. Statistical Power Analysis for Behavioural Sciences, 2nd ed.; Lawrence Erlbaum Associates: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Ingelsson, E.; Sullivan, L.M.; Fox, C.S.; Murabito, J.M.; Benjamin, E.J.; Polak, J.F.; Meigs, J.B.; Keyes, M.J.; O’donnell, C.J.; Wang, T.J.; et al. Burden and prognostic importance of subclinical cardiovascular disease in overweight and obese individuals. Circulation 2007, 116, 375–384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leite, A.; Santos, A.; Monteiro, M.; Gomes, L.; Veloso, M.; Costa, M. Impact of overweight and obesity in carotid intima-media thickness of Portuguese adolescents. Acta Paediatr. 2012, 101, e115–e121. [Google Scholar] [CrossRef] [PubMed]
- Ryder, J.R.; Northrop, E.; Rudser, K.D.; Kelly, A.S.; Gao, Z.; Khoury, P.R.; Kimball, T.R.; Dolan, L.M.; Urbina, E.M. Accelerated early vascular aging among adolescents with obesity and/or type 2 diabetes mellitus. J. Am. Heart Assoc. 2020, 9, e014891. [Google Scholar] [CrossRef] [PubMed]
- Muluvhu, T.C.; Monyeki, M.A.; Strydom, G.L.; Toriola, A.L. Cardiovascular topics—Relationship between obesity and blood pressure among employees in the Vhembe district municipality of Limpopo Province, South Africa. Cardiovasc. J. Afr. 2019, 30, 361–368. [Google Scholar] [CrossRef]
- WHO (World Health Organization). Overweight and Obesity. Geneva. (2017c). Available online: https://www.who.int/gho/ncd/risk_factors/overweight/en/ (accessed on 22 August 2019).
- Yusuf, S.; Hawken, S.; Ôunpuu, S.; Bautista, L.; Franzosi, M.G.; Commerford, P.; Lang, C.C.; Rumboldt, Z.; Onen, C.L.; Lisheng, L.; et al. Obesity and the risk of myocardial infarction in 27 000 participants from 52 countries: A case-control study. Lancet 2005, 366, 1640–1649. [Google Scholar] [CrossRef]
- Balkau, B.; Deanfield, J.E.; Després, J.P.; Bassand, J.P.; Fox, K.A.A.; Smith, S.C.; Barter, P.; Tan, C.E.; Van Gaal, L.; Wittchen, H.U.; et al. International day for the evaluation of abdominal obesity (IDEA): A study of waist circumference, cardiovascular disease, and diabetes mellitus in 168 000 primary care patients in 63 countries. Circulation 2007, 116, 1942–1951. [Google Scholar] [CrossRef] [Green Version]
- Casanueva, F.F.; Moreno, B.; Rodríguez-Azeredo, R.; Massien, C.; Conthe, P.; Formiguera, X.; Barrios, V.; Balkau, B. Relationship of abdominal obesity with cardiovascular disease, diabetes and hyperlipidaemia in Spain. Clin. Endocrinol. 2010, 73, 35–40. [Google Scholar] [CrossRef]
- Flegal, K.M.; Ioannidis, J.; Doehner, W. Flawed methods and inappropriate conclusions for health policy on overweight and obesity: The Global BMI Mortality Collaboration meta-analysis. J. Cachexia Sarcopenia Muscle 2019, 10, 9–13. [Google Scholar] [CrossRef]
- Ahmadi-Abhari, S.; Luben, R.N.; Wareham, N.J.; Khaw, K.T. Seventeen year risk of all-cause and cause-specific mortality associated with C-reactive protein, fibrinogen and leukocyte count in men and women: The EPIC-Norfolk study. Eur. J. Epidemiol. 2013, 28, 541–550. [Google Scholar] [CrossRef]
- Arroba, A.I.; Campos-Caro, A.; Aguilar-Diosdado, M.; Valverde, Á.M. IGF-1, Inflammation and Retinal Degeneration: A Close Network. Front. Aging Neurosci. 2018, 10, 203. [Google Scholar] [CrossRef] [PubMed]
- Hoebel, S.; Malan, L.; Botha, J.; Swanepoel, M. Optimizing Waist Circumference Cut-points for the Metabolic Syndrome and its Components in a South African Cohort at 3-year Follow-up: The SABPA Prospective Cohort. Endocrine 2014, 67, 959–961. [Google Scholar] [CrossRef] [PubMed]
- Malan, L.; Hamer, M.; Von Kaenel, R.; Van Wyk, R.D.; Nilsson, P.M.; Sumner, A.E.; Steyn, H.S.; Badenhorst, C.; Malan, N.T. A Stress syndrome prototype reflects type 3 diabetes and ischemic stroke risk: The SABPA study. Biology 2021, 10, 162. [Google Scholar] [CrossRef] [PubMed]
- Saeed, S.; Waje-Andreassen, U.; Nilsson, P.M. The Association of the Metabolic Syndrome with Target Organ Damage: Focus on the Heart, Brain, and Central Arteries. Expert Rev. Cardiovasc. Ther. 2020, 18, 601–614. [Google Scholar] [CrossRef]
- Malan, L.; Hamer, M.; Von Känel, R.; Van Wyk, R.D.; Wentzel, A.; Steyn, H.S.; Van Vuuren, P.; Malan, N.T. Retinal-glia ischemia and inflammation induced by chronic stress: The SABPA study. Brain Behav. Immun.—Health 2020, 2, 100027. [Google Scholar] [CrossRef]
- Łoboz-Rudnicka, M.; Jaroch, J.; Bociąga, Z.; Rzyczkowska, B.; Uchmanowicz, I.; Polański, J.; Dudek, K.; Szuba, A.; Łoboz-Grudzień, K. Impact of cardiovascular risk factors on carotid intima-media thickness: Sex differences. Clin. Interv. Aging 2016, 11, 721–731. [Google Scholar] [CrossRef] [Green Version]
- van Mil, S.R.; Biter, L.U.; van de Geijn, G.J.M.; Birnie, E.; Dunkelgrun, M.; Ijzermans, J.N.M.; van der Meulen, N.; Mannaerts, G.H.H.; Cabezas, M.C. The effect of sex and menopause on carotid intima-media thickness and pulse wave velocity in morbid obesity. Eur. J. Clin. Investig. 2019, 49, e13118. [Google Scholar] [CrossRef]
- Rychter, A.M.; Naskręt, D.; Zawada, A.; Ratajczak, A.E.; Dobrowolska, A.; Krela-Kaźmierczak, I. What Can We Change in Diet and Behaviour in Order to Decrease Carotid Intima-Media Thickness in Patients with Obesity? J. Pers. Med. 2021, 11, 505. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total Group (n = 216) | Males (n = 104) | Females (n = 112) | |
|---|---|---|---|
| Age (years) | 49.67 ± 8.44 | 49.79 ± 8.48 | 49.55 ± 8.43 |
| Height (cm) | 169.12 ± 10.18 | 176.6 ±7.90 * | 162.14 ± 6.37 * |
| Weight (kg) | 83.65 ± 19.62 | 90.75 ± 16.51 * | 77.06 ± 20.04 * |
| BMI (kg/m2) | 29.3 ±6.49 | 29.06 ± 4.77 | 29.64 ± 7.76 |
| WC (cm) | 96.40 ± 15.92 | 102.12 ± 12.79 * | 91.08 ± 16.74 * |
| WHtR | 0.57 ± 0.09 | 0.58 ± 0.07 | 0.56 ± 0.11 |
| SBP (mmHg) | 129.11 ± 18.29 | 134.57 ± 16.56 * | 124.04 ± 18.42 * |
| DBP (mmHg) | 86.22 ± 11.33 | 90.87 ± 10.42 * | 81.91 ± 10.44 * |
| CIMT (mm) | 0.70 ± 0.15 | 0.75 ± 0.16 * | 0.66 ± 0.12 * |
| Hypertension medication, n (%) | 67 (31) | 39 (38) | 28 (25) |
| Metabolic syndrome, n (%) | 63 (29) | 48 (46) * | 15 (13) |
| Physical activity | |||
| Sedentary, n (%) | 71 (33) | 46 (44) | 25 (22) * |
| Light PA, n (%) | 145 (67) | 58 (56) | 87 (78) |
| CRP ≥ 3 mg/L, n (%) | 88 (41) | 36 (35) | 52 (47) |
| Moderate atherosclerosis risk (CIMT ≥ 0.75 mm) | 74 (34) | 49 (47) * | 25 (22) * |
| No atherosclerosis risk (CIMT < 0.75 mm) | 141 (66) | 55 (53) | 86 (78) |
| WC Classification | Sedentary | Light PA | |||
|---|---|---|---|---|---|
| n | Mean ± SD | n | Mean ± SD | ||
| Age (years) | Overweight | 48 | 49.60 ± 9.08 | 105 | 50.85 ± 8.17 |
| Normal WC | 23 | 46.91 ± 9.76 | 40 | 48.23 ± 7.14 | |
| Height (cm) | Overweight | 48 | 172.82 ± 9.60 * | 105 | 169.98 ± 10.40 * |
| Normal WC | 23 | 164.24 ± 9.49 | 40 | 165.25 ± 8.55 | |
| Weight (kg) | Overweight | 48 | 96.96 ± 17.06 * | 105 | 88.78 ± 16.68 * |
| Normal WC | 23 | 63.00 ± 9.70 | 40 | 66.09 ± 10.93 | |
| BMI (kg/m2) | Overweight | 48 | 32.55 ± 6.14 * | 105 | 31.14 ± 5.98 * |
| Normal WC | 23 | 23.38 ± 3.36 | 40 | 24.32 ± 4.10 | |
| WC (cm) | Overweight | 48 | 108.71 ± 13.21 * | 105 | 101.34 ± 11.27 * |
| Normal WC | 23 | 79.72 ± 7.28 | 40 | 78.23 ± 7.99 | |
| WHtR | Overweight | 48 | 0.63 ± 0.09 * | 105 | 0.60 ± 0.07 * |
| Normal WC | 23 | 0.49 ± 0.05 | 40 | 0.47 ± 0.05 | |
| CIMT (mm) | Overweight | 47 | 0.72 ± 0.17 | 105 | 0.73 ± 0.15 * |
| Normal WC | 23 | 0.65 ± 0.15 | 40 | 0.66 ± 0.10 | |
| AEE (kcal/wk) | Overweight | 48 | 704.09 ± 636.28 | 105 | 1526.54 ± 1179.74 |
| Normal WC | 23 | 990.43 ± 858.24 | 40 | 1346.84 ± 965.68 | |
| TEE (kcal/wk) | Overweight | 48 | 2807.59 ± 701.14 | 105 | 3571.55 ± 1431.79 |
| Normal WC | 23 | 2830.08 ± 1100.43 | 40 | 3247.30 ± 1589.70 | |
| PAL | Overweight | 48 | 1.48 ± 0.15 | 105 | 2.37 ± 0.66 |
| Normal WC | 23 | 1.51 ± 0.13 | 40 | 2.26 ± 0.50 | |
| WHtR Category | Sedentary | Light PA | |||
|---|---|---|---|---|---|
| n | Mean ± SD | n | Mean ± SD | ||
| Age (years) | <0.5 | 44 | 47.32 ± 10.21 | 95 | 49.96 ± 7.56 |
| ≥0.5 | 27 | 51.04 ± 7.27 | 49 | 50.67 ± 8.68 | |
| Height (cm) | <0.5 | 44 | 170.17 ± 11.33 | 95 | 169.79 ± 10.16 |
| ≥0.5 | 27 | 169.83 ± 8.64 | 49 | 166.60 ± 9.88 | |
| Weight (kg) | <0.5 | 44 | 75.27 ± 17.77 * | 95 | 75.64 ± 13.17 * |
| ≥0.5 | 27 | 103.37 ± 16.29 * | 49 | 96.36 ± 19.23 * | |
| BMI (kg/m2) | <0.5 | 44 | 25.67 ± 3.77 * | 95 | 26.24 ± 3.49 * |
| ≥0.5 | 27 | 35.96 ± 6.01 * | 49 | 35.26 ± 6.28 * | |
| WC (cm) | <0.5 | 44 | 89.08 ± 12.08 * | 95 | 87.80 ± 10.39 * |
| ≥0.5 | 27 | 116.02 ± 12.42 * | 49 | 109.49 ± 10.07 * | |
| WHtR | <0.5 | 44 | 0.52 ± 0.05 * | 95 | 0.52 ± 0.05 * |
| ≥0.5 | 27 | 0.68 ± 0.08 * | 49 | 0.66 ± 0.06 * | |
| SBP (mmHg) | <0.5 | 44 | 127 ± 18 * | 95 | 123 ± 15 * |
| ≥0.5 | 27 | 144 ± 19 * | 49 | 136 ± 18 * | |
| DBP (mmHg) | <0.5 | 44 | 87 ± 12 * | 95 | 82 ± 10 * |
| ≥0.5 | 27 | 93 ± 11 * | 49 | 90 ± 11 * | |
| CIMT (mm) | <0.5 | 44 | 0.70 ± 0.17 | 95 | 0.71 ± 0.14 |
| ≥0.5 | 27 | 0.69 ± 0.16 | 49 | 0.71 ± 0.16 | |
| AEE (kcal/wk) | <0.5 | 12 | 819.09 ± 970.19 | 28 | 1238.22 ± 153.10 |
| ≥0.5 | 59 | 792.33 ± 671.42 | 116 | 1485.69 ± 98.92 | |
| TEE (kcal/wk) | <0.5 | 12 | 2578.99 ± 1292.64 | 28 | 3085.28 ± 304.02 |
| ≥0.5 | 59 | 2862.85 ± 725.99 | 116 | 3520.39 ± 121.17 | |
| PAL (kcal/wk) | <0.5 | 12 | 1.42 ± 0.11 * | 28 | 2.12 ± 0.45 * |
| ≥0.5 | 59 | 1.50 ± 0.14 * | 116 | 2.36 ± 0.59 * | |
| Sedentary | Light PA | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age (years) | Height (cm) | Weight (kg) | BMI (kg/m2) | CIMT (mm) | WC (cm) | AEE (kcal/wk) | Age (years) | Height (cm) | Weight (kg) | BMI (kg/m2) | CIMT (mm) | WC (cm) | AEE (kcal/wk) | ||
| Age (years) | r | – | 0.06 | 0.07 | 0.03 | 0.33 ** | 0.14 | −0.13 | – | 0.02 | 0.03 | −0.01 | 0.31 ** | 0.13 | 0.01 |
| p | 0.60 | 0.59 | 0.79 | 0.01 | 0.25 | 0.29 | 0.81 | 0.68 | 0.90 | <0.01 | 0.11 | 0.90 | |||
| Height (cm) | r | 0.06 | – | 0.54 ** | 0.12 | 0.39 ** | 0.37 ** | −0.23 | 0.02 | – | 0.42 ** | −0.16 | 0.22 ** | 0.24 ** | 0.28 ** |
| p | 0.60 | <0.01 | 0.31 | <0.01 | <0.01 | 0.06 | 0.81 | <0.01 | 0.06 | 0.01 | <0.01 | <0.01 | |||
| Weight (kg) | r | 0.07 | 0.54 ** | – | 0.88 ** | 0.14 | 0.92 ** | −0.09 | 0.03 | 0.42 ** | – | 0.77 ** | 0.22 ** | 0.86 ** | 0.21 * |
| p | 0.59 | <0.01 | <0.01 | 0.25 | <0.01 | 0.44 | 0.68 | <0.01 | <0.01 | 0.01 | <0.01 | 0.01 | |||
| BMI (kg/ m2) | r | 0.03 | 0.12 | 0.88 ** | – | −0.05 | 0.90 ** | 0.02 | −0.01 | −0.16 | 0.77 ** | – | 0.09 | 0.81 ** | −0.01 |
| p | 0.79 | 0.31 | <0.01 | . | 0.66 | <0.01 | 0.86 | 0.90 | 0.06 | <0.01 | 0.27 | <0.01 | 0.88 | ||
| CIMT (mm) | r | 0.33 ** | 0.39 ** | 0.14 | −0.05 | – | 0.14 | −0.17 | 0.31 ** | 0.22 ** | 0.22 ** | 0.09 | – | 0.19 * | 0.11 |
| p | 0.01 | <0.01 | 0.25 | 0.66 | 0.25 | 0.15 | <0.01 | 0.01 | 0.01 | 0.27 | 0.02 | 0.20 | |||
| WC (cm) | r | 0.14 | 0.37 ** | 0.92 ** | 0.90 ** | 0.14 | – | −0.02 | 0.13 | 0.24 ** | 0.86 ** | 0.81 ** | 0.19 * | – | 0.10 |
| p | 0.25 | <0.01 | <0.01 | <0.01 | 0.25 | 0.86 | 0.11 | <0.01 | <0.01 | <0.01 | 0.02 | 0.234 | |||
| AEE (kcal/wk) | r | −0.13 | −0.23 | −0.09 | 0.02 | −0.17 | −0.02 | – | 0.01 | 0.28 ** | 0.21 * | −0.01 | 0.11 | 0.10 | - |
| p | 0.29 | 0.06 | 0.44 | 0.86 | 0.15 | 0.86 | 0.90 | <0.01 | 0.01 | 0.88 | 0.20 | 0.24 | |||
| CIMT ≥ 0.75 mm | ||||||||
|---|---|---|---|---|---|---|---|---|
| β | S.E. | Wald | df | Sig. | Exp(B) | 95% C.I. for EXP(B) | ||
| Lower | Upper | |||||||
| Age (years) | −0.051 | 0.020 | 6.396 | 1 | 0.011 | 0.950 | 0.913 | 0.989 |
| Sex | 0.853 | 0.350 | 5.946 | 1 | 0.015 | 2.346 | 1.182 | 4.656 |
| GGT (U/L) | −0.002 | 0.003 | 0.303 | 1 | 0.582 | 0.998 | 0.993 | 1.004 |
| SBP (mmHg) | −0.008 | 0.010 | 0.719 | 1 | 0.397 | 0.992 | 0.974 | 1.011 |
| Log CRP | 0.036 | 0.034 | 1.086 | 1 | 0.297 | 1.036 | 0.969 | 1.109 |
| WC cut point | 0.966 | 0.412 | 5.500 | 1 | 0.019 | 2.628 | 1.172 | 5.892 |
| PAL | −0.034 | 0.240 | 0.020 | 1 | 0.888 | 0.967 | 0.604 | 1.548 |
| Constant | 2.663 | 1.743 | 2.335 | 1 | 0.126 | 14.346 | ||
| B | S.E. | Wald | df | Sig. | Exp(B) | 95% C.I. for EXP(B) | ||
|---|---|---|---|---|---|---|---|---|
| Lower | Upper | |||||||
| Male | ||||||||
| Age (years) | −0.04 | 0.03 | 2.85 | 1 | 0.09 | 0.96 | 0.91 | 1.01 |
| SBP (mmHg) | −0.00 | 0.01 | 0.07 | 1 | 0.80 | 0.99 | 0.97 | 1.02 |
| Log Hs-CRP (mg/L) | −0.52 | 0.70 | 0.55 | 1 | 0.46 | 0.59 | 0.15 | 2.36 |
| Ethnic specific WC | 0.54 | 0.57 | 0.89 | 1 | 0.35 | 1.72 | 0.56 | 5.27 |
| Log GGT | −0.04 | 0.67 | 0.00 | 1 | 0.96 | 0.97 | 0.26 | 3.55 |
| Log PAL | 0.12 | 1.51 | 0.01 | 1 | 0.94 | 1.12 | 0.06 | 21.47 |
| Log CRP | 0.09 | 0.08 | 1.29 | 1 | 0.26 | 1.10 | 0.94 | 1.28 |
| Constant | 1.99 | 2.41 | 0.68 | 1 | 0.41 | 7.33 | ||
| Female | ||||||||
| Age (years) | −0.06 | 0.03 | 3.40 | 1 | 0.07 | 0.94 | 0.88 | 1.00 |
| SBP (mmHg) | −0.01 | 0.25 | 0.83 | 1 | 0.36 | 0.99 | 0.96 | 1.02 |
| Log Hs-CRP (mg/L) | 0.50 | 0.81 | 0.37 | 1 | 0.54 | 1.64 | 0.33 | 8.07 |
| Ethnic specific WC | 1.44 | 0.69 | 4.41 | 1 | 0.04 | 4.23 | 1.10 | 16.25 |
| Log GGT | 0.41 | 0.99 | 0.17 | 1 | 0.68 | 1.50 | 0.22 | 10.37 |
| Log PAL | 0.44 | 2.45 | 0.03 | 1 | 0.86 | 1.55 | 0.01 | 189.73 |
| Log CRP | −0.03 | 0.09 | 0.13 | 1 | 0.72 | 0.97 | 0.82 | 1.15 |
| Constant | 3.53 | 3.18 | 1.24 | 1 | 0.27 | 34.24 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Veldsman, T.; Swanepoel, M.; Monyeki, M.A.; Brits, J.S.; Malan, L. The Role of Physical Activity Status in the Relationship between Obesity and Carotid Intima-Media Thickness (CIMT) in Urban South African Teachers: The SABPA Study. Int. J. Environ. Res. Public Health 2022, 19, 6348. https://doi.org/10.3390/ijerph19106348
Veldsman T, Swanepoel M, Monyeki MA, Brits JS, Malan L. The Role of Physical Activity Status in the Relationship between Obesity and Carotid Intima-Media Thickness (CIMT) in Urban South African Teachers: The SABPA Study. International Journal of Environmental Research and Public Health. 2022; 19(10):6348. https://doi.org/10.3390/ijerph19106348
Chicago/Turabian StyleVeldsman, Tamrin, Mariette Swanepoel, Makama Andries Monyeki, Johanna Susanna Brits, and Leoné Malan. 2022. "The Role of Physical Activity Status in the Relationship between Obesity and Carotid Intima-Media Thickness (CIMT) in Urban South African Teachers: The SABPA Study" International Journal of Environmental Research and Public Health 19, no. 10: 6348. https://doi.org/10.3390/ijerph19106348
APA StyleVeldsman, T., Swanepoel, M., Monyeki, M. A., Brits, J. S., & Malan, L. (2022). The Role of Physical Activity Status in the Relationship between Obesity and Carotid Intima-Media Thickness (CIMT) in Urban South African Teachers: The SABPA Study. International Journal of Environmental Research and Public Health, 19(10), 6348. https://doi.org/10.3390/ijerph19106348