
A Scoping Review of Community-Based Adult Suicide Prevention Initiatives in Rural and Regional Australia

 , , , and
, , , and
Abstract
:1. Introduction
2. Method
2.1. Identifying the Research Question
2.2. Identifying Relevant Studies
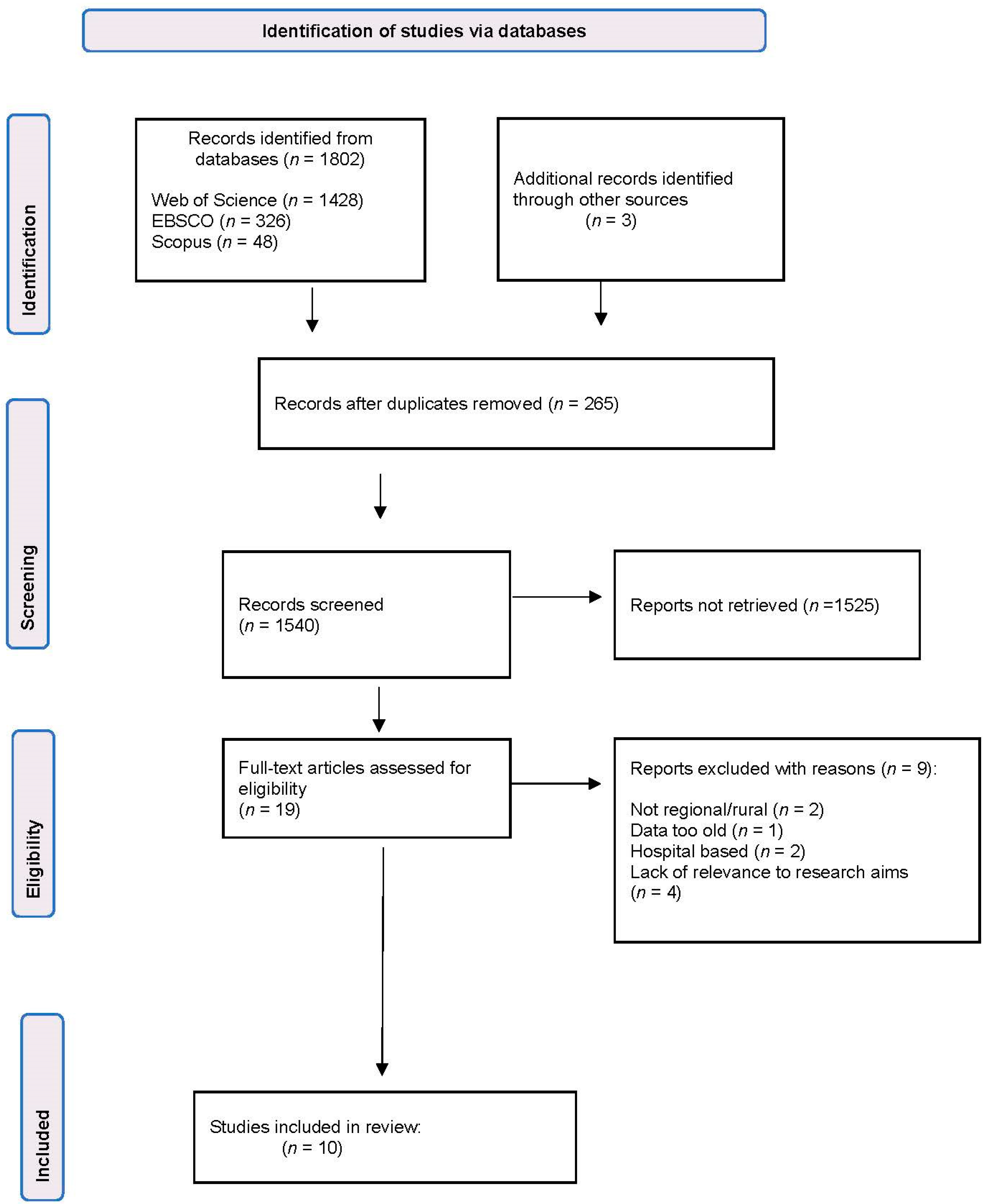
2.3. Study Selection
2.4. Charting the Data
2.5. Reporting the Results
3. Results
3.1. Article Characteristics

{kind=link}
| Author and Year | Study Aim(s) | Study Design | Population | Description of Suicide Prevention Initiative | Main Findings |
|---|---|---|---|---|---|
| Barnett et al. [22] 2019 | To gain an understanding of the experience of artists impacted by mental illness who participated in the Rural Art Roadshow. | Mixed methods | n = 23 artists (17.4% male) | The aim of the project was to help reduce stigma and promote a positive image of mental health in rural communities. | The three themes—Community Impact, Social Gains, and Personal Gains—demonstrated positive social and personal benefits for participating artists. The Rural Art Roadshow is a promising mental health promotion approach that could be replicated in other rural and remote areas of Australia. |
| Calabria et al. [17] 2020 | To examine the feasibility and acceptability of the Aboriginal-adapted Community Reinforcement Approach (CRA) delivered to Aboriginal and non-Aboriginal clients in a non-Aboriginal-focused rural, community-based drug and alcohol treatment service, and to assess pre–post-program changes for drug and alcohol use and wellbeing outcomes. | Quantitative pre- and post-intervention evaluation | Aboriginal and non-Aboriginal clients aged 18 years and over (n = 55, 58% males) | The CRA is an evidence-based cognitive behavioural therapy (CBT) intervention that targets harmful drug and alcohol use. Compared to the US version, the tailored CRA had reduced technical language, reduced number of treatment sessions, the option of a group delivery, and was deemed to be culturally acceptable. | The CRA was associated with statistically significant reductions in the use of alcohol, tobacco, cannabis, amphetamines, and over the counter medications, as well as levels of psychological distress. The CRA was also associated with an increase in levels of empowerment for both Aboriginal and non-Aboriginal clients. |
| Davies et al. [18] 2020 | To evaluate the We-Yarn suicide prevention gatekeeper training Workshop, and to examine whether participants reported being more able to address and respond to suicide in their communities. | Mixed methods | n = 106 attendees including a mixed group of community members, staff of other health and community service organisations, and staff from Aboriginal Community-Controlled Health Organisations (ACCHOs) | We-Yarn is a suicide prevention gatekeeper training workshop—the workshop encouraged discussion and sharing of experiences, cultural tailoring of the program to include the seven domains of connection, and the use of the SCARF action plan (Suspect, Connect, Ask, Refer, Follow-Up). | We-Yarn appeared to be well-suited and culturally appropriate for Aboriginal suicide prevention gatekeeper training. There were significant improvements in participants’ self-reported knowledge and capacity to support someone struggling with social and emotional wellbeing problems. The workshops were valuable in strengthening knowledge and providing opportunities to discuss various approaches for culturally appropriate suicide prevention strategies. |
| Handley et al. [16] 2021 | This paper describes the Good SPACE suicide prevention program and the lessons learned from delivering this program over a 14-year period (formerly known as the Farm-Link; see Perceval et al., 2020). | Commentary | Rural communities | Good SPACE is a suicide prevention program designed to prevent suicide through community and clinical education. The program educates rural community members to recognise the signs of suicide vulnerability and how to take action if they meet someone considering suicide. | A consistent finding was that approximately 80% of workshop attendees were females. The program was complemented by the development and co-design of variants to meet the needs of their intended audience. |
| Harris et al. [23] 2018 | To display a selection of artworks in four small communities to engage and promote positive discussions about mental health. | Mixed methods survey | Visitor evaluation (n = 56) | The Rural Art Roadshow was a travelling program of artwork that visited rural communities to help improve community understanding of mental health, reduce stigma, and promote art-based mental health initiatives. | Each opening feature provided an opportunity for artists to speak about their experience of mental ill-health and creating their artwork. The art exhibition was well attended (n = 600 visitors), but with a low response rate to the evaluation surveys. There was a strong agreement that the art exhibition should be repeated annually. |
| Hearn et al. [19] 2016 | To describe a community-developed Aboriginal model for early identification and referral of people with psychological distress and suicidal ideation. | Case study: descriptive | n = 12 support persons (No demographic data available) | The Jekkora model consists of recruitment and appointment of support persons, identifying people at risk, follow-up and referral by support persons, and expansion and sustainability. A series of training programs provided to support persons, such as: ASIST (Applied Suicide Intervention Skills Training), safeTALK, Living Hope Bereavement Support, and Support after Suicide. | The Jekkora model was developed by Aboriginal people for their community. It is a culturally acceptable, problem-specific, sustainable service for the early identification, treatment, and follow-up support for Aboriginal people in distress |
| Kennedy et al. [21] 2020 | To evaluate the effectiveness of an intervention tailored for the farming community, designed to reduce stigma among male farm workers with a lived experience of suicide. | Mixed methods analysis | The Ripple Effect website had 12,755 visitors during the research period. n = 710 participants consented. Of these participants, n = 169 were from the target group (30–64-year-old males) | The Ripple Effect digital intervention was divided into five chapters, and email reminders were sent at designated time points to encourage completion. It included personal stories, videos, education, and personal goal setting. | The intervention was far-reaching. There were no identified changes in perceived stigma using quantitative measures; however, behavioural/ attitude changes emerged in the qualitative data. This program was successful in reaching their targeted population, along with other groups in rural Australia. |
| Perceval et al. [24] 2020 | To evaluate a wellbeing and suicide prevention education workshop, SCARF (Suspect, Connect, Ask, Refer, Follow-Up), developed for Australian farming and rural communities. | Quantitative pre- and post-intervention evaluation | n = 255 (153 females, 102 males); mean age: 44.4 years | Wellbeing and suicide prevention education workshop—SCARF (Suspect, Connect, Ask, Refer, Follow-Up)—specifically developed for Australian farming and rural communities | There was a significant increase in suicide literacy and confidence immediately post-workshop, which remained at the 3-month follow-up. Mental wellbeing was also significantly improved at the 3-month follow-up. There were no changes to the overall score on the Stigma of Suicide Scale (SOSS). |
| Powell et al. [25] 2019 | To examine the implementation of a community-driven mental health and wellbeing initiative in northern New South Wales, which began in response to a geographic cluster of local suicides. | Mixed methods | Review of 65 project documents (Quantitative data) Semi-structured interviews with 99 local stakeholders | “Our Healthy Clarence” is described as a novel, low-cost, small, bottom-up, locally driven approach. It was developed in response to a geographic cluster of local suicides. A stakeholder group formed to develop and enact the community mental health and wellbeing plan. | Stakeholders reported increased community agency, collaboration, optimism, and willingness to discuss mental health, suicide, and help-seeking. This initiative could serve as a model for other communities to address suicide and self-harm, and improve wellbeing. |
| Snodgrass et al. [20] 2020 | To evaluate Deadly Thinking, which is a social and emotional wellbeing promotion program targeted at remote and rural Aboriginal and Torres Strait Islander communities. | Quantitative pre- and post-intervention evaluation | n = 413 participants across 40 locations in rural and remote Australia (n = 263 females, n = 114 males, n = 36 missing data) | Deadly Thinking aims to improve emotional health literacy, psychological wellbeing, and attitudes towards help-seeking associated with emotional ill-health. | Overall, there were low rates of marked distress in groups, and participants reported positive perceptions of community safety and wellbeing. Participants considered that that the workshop would help them to support others experiencing an emotional health crisis and improve their knowledge. |
| Author and Year | Frequency of Program | Targeted Audience | Types of Activities | Evaluation Plan/Measurement/Tool | Program Strategies | Lessons Learnt |
|---|---|---|---|---|---|---|
| Barnett et al. [22] 2019 | Art exhibition remained open for one week in each venue. Opening events were held in the evening and lasted 1–2 h. | Four small rural communities in Tasmania, Australia. | Art exhibition—22 pieces of art selected from the annual “Minds Do Matter” exhibition in Launceston. | Semi-structured interviews with the artists. Visitor survey of 6 statements on a Likert Scale and 3 open-ended questions. | The program promoted art as therapy and used the community event to foster social inclusion and have positive conversations about mental health. Entry to the exhibition was free. | Quality improvement suggestions included other mediums of disseminating the art, such as the use of social media or discussion boards. Future events should include a promotion and publicity plan tailored to each community. |
| Calabria et al. [17] 2020 | The Community Reinforcement Approach (CRA) was offered to clients individually (60 min sessions) or in groups (90 min sessions). Six weekly sessions were planned, with the option of additional individual sessions. | Aboriginal and non- Aboriginal clients aged 18 years and over who attended a non- Aboriginal-focused community-based drug and alcohol treatment service in rural New South Wales. | Cognitive behavioural therapy (CBT) within a group setting or on an individual basis. | Outcome measures were collected at baseline, 4 weeks, 3 months, and 6 months. Kessler-5, Growth Empowerment Measure (GEM), and Alcohol, Smoking, and Substance Involvement Screening Test (ASSIST) | Therapists were local people who are known and trusted by the community. Aboriginal health workers were involved in the delivery of CRA to Aboriginal clients. CRA was embedded into routine practice. | This CBT approach also included training in skills that are transferable to other areas of life, such as communication, and may have contributed to improvements in psychological wellbeing, signifying the importance of building individual capacity. |
| Davies et al. [18] 2020 | Six We-Yarn workshops that took approximately 6 h each over a period of 6 months. | Aboriginal people and those who work with Aboriginal communities and people in rural New South Wales. | Culturally safe suicide prevention skills training. | Self-rated responses on a 5-point Likert scale about their capacity and confidence to respond to a person at risk of suicide. Open-ended questions about the workshop. Focus groups. | Each workshop was facilitated by an experienced non-Aboriginal suicide prevention trainer and an experienced Aboriginal facilitator. Both facilitators had lived experience of suicide. | The sharing of the facilitators’ lived experiences was vital to instigating discussion and connecting with the workshop participants. Ongoing strategies should be community-led, and programs such as We-Yarn should be part of a multifaceted suicide prevention strategy. |
| Handley et al. [16] 2021 | Good SPACE is a 4-h program. | Farmers, Aboriginal people, and general rural community members. | Education/ workshops | Evaluations included surveys/interviews following workshops. | The Good SPACE program was supplemented by other specialist training for GPs and clinicians to strengthen the local response. | Evaluation did not consider how to address the bigger issues of how to improve target audience reach, local engagement, and connection to services. General promotional approaches tended to recruit participants who were already well-versed in mental health. |
| Harris et al. [23] 2018 | Art exhibition remained open for one week in each venue. Opening events were held in the evening and lasted 1–2 h. | Four small rural communities in Tasmania, Australia. | Art exhibition—22 pieces of art selected from the annual “Minds Do Matter” exhibition in Launceston. | Short survey of 6 statements on a Likert Scale and 3 open-ended questions. | The program promoted art as therapy and used the community event to foster social inclusion and have positive conversations about mental health. Entry to the exhibition was free. | Feedback indicated that the public wished to embed the exhibition in the local community, in partnership with local governments, businesses, schools, and health services. Suggestions from the public on how to improve future events included the need to have more interactive activities, the provision of further information on how to obtain mental health advice and services and increasing the reach of the roadshow. |
| Hearn et al. [19] 2016 | Training programs lasted between 2 and 4 h, and were delivered to 12 individuals. | Posters and flyers were used to recruit interested people from the local community in Echuca, Victoria. After training, 10 individuals were selected to form the first group of voluntary trained support persons (VTSPs). | The VTSPs made weekly telephone calls to a referred person for 3 months using 5 questions to guide casual conversation. An Aboriginal health worker was notified if the person demonstrated sign of distress. Referrals were made by a GP. | Program evaluation plan not specified. VTSPs documented key responses and attended a monthly debriefing session. | At the end of the 3 months, community members who were supported were encouraged to take up the role of support persons for others in the community, and to undergo training. | By including people with a lived experience after their experience with the program, this model fosters community empowerment. Helps to establish social connectedness, wellbeing, and community resilience within Aboriginal communities. |
| Kennedy et al. [21] 2020 | Online intervention estimated to take 2.5 to 4 h to complete; recommended to be completed in a few sessions over a couple of weeks. | The focus was on a male population (aged 30–64 years) in farming communities; however, participation in the intervention was expanded to include all adults (male and female). | Digital intervention consisting of five chapters. | Stigma of Suicide Scale; Literacy of Suicide Scale. Online feedback survey using both qualitative and quantitative questions. | Partners and stakeholders with links to the farming community were recruited to assist in sharing information about the Ripple Effect across rural networks, such as social media, local media, industry newsletters, community presentations, sporting clubs, and information flyers. A Community Champions Network was also developed to promote the project. | The previously identified evidence of association between increasing mental health literacy and decreasing mental health stigma may not apply to suicide literacy and suicide stigma. Support services should be easily accessible and should demonstrate an understanding of farming life and work when delivered within a rural context. |
| Perceval et al. [24] 2020 | 4-h workshop delivered free of charge. | Australian farming and rural communities in New South Wales. | Education. | Literacy of Suicide Scale, Stigma of Suicide Scale, Warwick–Edinburgh Mental Wellbeing Scale, confidence scale (developed for the study). | The program was delivered to frontline agricultural professionals, including agribusiness bankers, rural financial counsellors and accountants, those working with farming organisations—such as New South Wales (NSW) Farmers or Local Land Services—staff from employment, disability and care agencies, chaplains, and farming community groups. | Refresher training could be useful, as the mean scores for literacy and confidence dropped after 3 months despite a significant increase post-workshop. The SCARF program has since been updated to CARE (Connect, Ask, Refer, Encourage), signifying the importance of using contemporary evidence to inform suicide prevention programs. |
| Powell et al. [25] 2019 | In early 2016, a steering group was formed to implement Our Healthy Clarence. This initiative has operated for two years and has five key objectives to address community mental health and wellbeing. | Members of the Clarence Valley Local Government area in New South Wales (~51,750 residents). | Community workshops. New services: a headspace centre; pop-up information and referral hubs in community centres. 2000 people received training in mental health literacy and suicide prevention in the community and workplaces. Standalone community events and connection with other community events and partners. Strength-based messaging through media. Sharing of Mindframe guidelines to media outlets. | Formative evaluation— use of 65 project documents and 36 semi-structured interviews with local stakeholders. No evaluation of the impact of the initiative. | The initiative was based on the principles of public health and community development. Factors that contributed to its success included leadership support, clarity of purpose, a paid independent coordinator, community involvement, and transparent governance. | To be sustainable, initiatives must respond to the local context and build on local assets if they are to be relevant and sustainable. Governance and structure were important to the success of the initiative. The multidimensional nature of the program denotes challenges and various complexities in evaluating the initiative, as statistics such as suicide rates or hospital admissions do not reflect the objectives of the initiative. |
| Snodgrass et al. [20] 2020 | Two phases: group-based 1-day community workshop, or 2-day Train the Trainer (TTT) workshop | Aboriginal and Torres Strait Islander adults | Workshops | 5 items adapted from Shaw and d’Abb’s community health scale, Kessler-5, MINI Suicidal Scale, a modified version of the Alcohol, Smoking, and Substance Involvement Screening Test, help-seeking intentions, and workshop feedback survey. | Deadly Thinking includes the opportunity for participants to discuss common sources of stress, such as family, employment, racism, discrimination, anxiety, depression, stigma, and suicide. It was developed in conjunction with local Aboriginal communities through a previous project. | There were a lower number of males who participated in the program; thus, the authors were unable to determine the extent to which the program was acceptable to men. It is recommended that providing a workshop specifically designed for men can encourage increased male attendance, creating a safe environment to discuss sensitive topics. |
3.2. Key Characteristics of Suicide Prevention Initiatives
3.3. Program Evaluation
3.4. Program Strategies
3.5. Key Findings of Initiatives
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Australian Government. Suicide in Australia. 2021. Available online: https://www.health.gov.au/health-topics/mental-health-and-suicide-prevention/suicide-in-australia (accessed on 23 November 2021).
- Australian Institute of Health and Welfare. Australia’s Health 2018; AIHW: Canberra, Australia, 2018.
- World Health Organisation. Suicide. Available online: https://www.who.int/news-room/fact-sheets/detail/suicide (accessed on 23 November 2021).
- World Health Organisation. Suicide: One Person Dies Every 40 Seconds. Available online: https://www.who.int/news/item/09-09-2019-suicide-one-person-dies-every-40-seconds (accessed on 23 November 2021).
- State of Victoria. Royal Commission into Victoria’s Mental Health System. Available online: https://finalreport.rcvmhs.vic.gov.au/download-report/ (accessed on 21 December 2021).
- Australian Government. Australia’s Long Term National Health Plan. Available online: https://www.health.gov.au/sites/default/files/australia-s-long-term-national-health-plan_0.pdf (accessed on 30 December 2021).
- Reifels, L.; Ftanou, M.; Krysinska, K.; Machlin, A.; Robinson, J.; Pirkis, J. Research Priorities in Suicide Prevention. Available online: https://www.suicidepreventionaust.org/wp-content/uploads/2020/09/Research-Priorities-Report-FINAL-2017-11-03.pdf (accessed on 21 March 2022).
- Dabkowski, E.; Porter, J.E. An exploration into suicide prevention initiatives for mental health nurses: A systematic literature review. Int. J. Ment. Health Nurs. 2021, 30, 610–623. [Google Scholar] [CrossRef] [PubMed]
- Zalsman, G.; Hawton, K.; Wasserman, D.; van Heeringen, K.; Arensman, E.; Sarchiapone, M.; Carli, V.; Höschl, C.; Barzilay, R.; Balazs, J.; et al. Suicide prevention strategies revisited: 10-year systematic review. Lancet Psychiatry 2016, 3, 646–659. [Google Scholar] [CrossRef]
- De Cotta, T.; Knox, J.; Farmer, J.; White, C.; Davis, H. Community co-produced mental health initiatives in rural Australia: A scoping review. Aust. J. Rural. Health 2021, 29, 865–878. [Google Scholar] [CrossRef] [PubMed]
- Roy, P.; Tremblay, G.; Oliffe, J.L.; Jbilou, J.; Robertson, S. Male farmers with mental health disorders: A scoping review. Aust. J. Rural. Health 2013, 21, 3–7. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Popay, J.; Roberts, H.; Sowden, A.; Petticrew, M.; Arai, L.; Rodgers, M.; Duffy, S. Guidance on the Conduct of Narrative Synthesis in Systematic Reviews; A Product from the ESRC Methods Programme; Lancaster University: Lancaster, UK, 2006. [Google Scholar]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef]
- Handley, T.E.; Davies, K.; Booth, A.; Dalton, H.; Perkins, D. Lessons from the development and delivery of a rural suicide prevention program. Aust. J. Rural. Health 2021, 29, 994–999. [Google Scholar] [CrossRef]
- Calabria, B.; Shakeshaft, A.P.; Clifford, A.; Stone, C.; Clare, P.J.; Allan, J.; Bliss, D. Reducing drug and alcohol use and improving well-being for Indigenous and non-Indigenous Australians using the Community Reinforcement Approach: A feasibility and acceptability study. Int. J. Psychol. J. Int. Psychol. 2020, 55 (Suppl. 1), 88–95. [Google Scholar] [CrossRef]
- Davies, K.; Read, D.M.Y.; Booth, A.; Turner, N.; Gottschall, K.; Perkins, D. Connecting with social and emotional well-being in rural Australia: An evaluation of ‘We-Yarn’, an Aboriginal gatekeeper suicide prevention workshop. Aust. J. Rural. Health 2020, 28, 579–587. [Google Scholar] [CrossRef]
- Hearn, S.; Wanganeen, G.; Sutton, K.; Isaacs, A. The Jekkora group: An Aboriginal model of early identification, and support of persons with psychological distress and suicidal ideation in rural communities. Adv. Ment. Health 2016, 14, 96–105. [Google Scholar] [CrossRef]
- Snodgrass, W.J.; Rayner, V.; Rice, S.M.; Purcell, R.; Bowers, J. Evaluation of a culturally sensitive social and emotional well-being program for Aboriginal and Torres Strait Islanders. Aust. J. Rural. Health 2020, 28, 327–337. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, A.J.; Brumby, S.A.; Versace, V.L.; Brumby-Rendell, T. The ripple effect: A digital intervention to reduce suicide stigma among farming men. BMC Public Health 2020, 20, 813. [Google Scholar] [CrossRef] [PubMed]
- Barnett, T.; de Deuge, J.; Bridgman, H. Promoting mental health through a Rural Art Roadshow: Perspectives of participating artists. Int. J. Ment. Health Syst. 2019, 13, 44. [Google Scholar] [CrossRef] [Green Version]
- Harris, M.W.; Barnett, T.; Bridgman, H. Rural art roadshow: A travelling art exhibition to promote mental health in rural and remote communities. Arts Health 2018, 10, 57–64. [Google Scholar] [CrossRef]
- Perceval, M.; Reddy, P.; Ross, V.; Joiner, T.; Kolves, K. Evaluation of the SCARF well-being and suicide prevention program for rural Australian communities. J. Rural. Health 2020, 36, 247–254. [Google Scholar] [CrossRef]
- Powell, N.; Dalton, H.; Perkins, D.; Considine, R.; Hughes, S.; Osborne, S.; Buss, R. Our healthy Clarence: A community-driven wellbeing initiative. Int. J. Environ. Res. Public Health 2019, 16, 3691. [Google Scholar] [CrossRef] [Green Version]
- Perceval, M.; Ross, V.; Kõlves, K.; Reddy, P.; De Leo, D. Social factors and Australian farmer suicide: A qualitative study. BMC Public Health 2018, 18, 1367. [Google Scholar] [CrossRef] [Green Version]
- Jones, M.; Ferguson, M.; Walsh, S.; Martinez, L.; Marsh, M.; Cronin, K.; Procter, N. Perspectives of rural health and human service practitioners following suicide prevention training programme in Australia: A thematic analysis. Health Soc. Care Community 2018, 26, 356–363. [Google Scholar] [CrossRef]
- Australian Institute of Health and Welfare. Australia’s Health 2020 in Brief. Available online: https://www.aihw.gov.au/getmedia/2aa9f51b-dbd6-4d56-8dd4-06a10ba7cae8/aihw-aus-232.pdf.aspx?inline=true (accessed on 14 March 2022).
- Nasir, B.; Kisely, S.; Hides, L.; Ranmuthugala, G.; Brennan-Olsen, S.; Nicholson, G.C.; Gill, N.S.; Hayman, N.; Kondalsamy-Chennakesavan, S.; Toombs, M. An Australian Indigenous community-led suicide intervention skills training program: Community consultation findings. BMC Psychiatry 2017, 17, 219. [Google Scholar] [CrossRef] [Green Version]
- Bryant, L.; Garnham, B. Suicide and Its Prevention for Ageing Farmers; Department of Health and Ageing (SA): Adelaide, Australia, 22 March 2016.
- Thomas, A.; Lubarsky, S.; Durning, S.J.; Young, M.E. Knowledge syntheses in medical education: Demystifying scoping reviews. Acad. Med. 2017, 92, 161–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cooper, S.; Cant, R.; Kelly, M.; Levett-Jones, T.; McKenna, L.; Seaton, P.; Bogossian, F. An evidence-based checklist for improving scoping review quality. Clin. Nurs. Res. 2019, 30, 230–240. [Google Scholar] [CrossRef] [PubMed]

| Search Term | Variations |
|---|---|
| Suicid * | Suicide prevention Suicide reduction Suicide intervention Mental health Mental illness Mental disorder |
| Adult * | Older Middle aged Farm * |
| Initiative * | Program * Intervention * Strateg * |
| Regional | Rural Remote Community Country |
| NOT child * | Paediatric Pediatric Young Adolesc * Teenager |
| Inclusion Criteria | Exclusion Criteria |
| Peer-reviewed publications Studies published between 2012 and 2022 English language Full-text articles Studies conducted in Australia Adults aged ≥18 years Rural/regional areas only Community-based | Metropolitan areas Hospital-based suicide prevention initiatives (inpatient/outpatient) Adolescent or youth population (<18 years) Studies focused on psychometric or measurement tools |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dabkowski, E.; Porter, J.E.; Barbagallo, M.S.; Prokopiv, V.; Jackson, M.R. A Scoping Review of Community-Based Adult Suicide Prevention Initiatives in Rural and Regional Australia. Int. J. Environ. Res. Public Health 2022, 19, 7007. https://doi.org/10.3390/ijerph19127007
Dabkowski E, Porter JE, Barbagallo MS, Prokopiv V, Jackson MR. A Scoping Review of Community-Based Adult Suicide Prevention Initiatives in Rural and Regional Australia. International Journal of Environmental Research and Public Health. 2022; 19(12):7007. https://doi.org/10.3390/ijerph19127007
Chicago/Turabian StyleDabkowski, Elissa, Joanne E. Porter, Michael S. Barbagallo, Valerie Prokopiv, and Megan R. Jackson. 2022. "A Scoping Review of Community-Based Adult Suicide Prevention Initiatives in Rural and Regional Australia" International Journal of Environmental Research and Public Health 19, no. 12: 7007. https://doi.org/10.3390/ijerph19127007
APA StyleDabkowski, E., Porter, J. E., Barbagallo, M. S., Prokopiv, V., & Jackson, M. R. (2022). A Scoping Review of Community-Based Adult Suicide Prevention Initiatives in Rural and Regional Australia. International Journal of Environmental Research and Public Health, 19(12), 7007. https://doi.org/10.3390/ijerph19127007