
Increasing Seasonal Influenza Vaccination among University Students: A Systematic Review of Programs Using a Social Marketing Perspective




Abstract
:1. Introduction
1.1. Significance of Increasing University Students’ Uptake of Seasonal Influenza Vaccine
1.2. Literature Assessment Method: Social Marketing Benchmark Criteria
- Synthesize knowledge gained from previous seasonal influenza vaccination promotion programs or interventions that have effectively increased university students’ vaccination rates;
- Assess the extent to which social marketing principles were applied in identified studies;
- Inform healthcare policymakers and university management on the effective practices that can be applied to motivate university students to uptake annual seasonal influenza vaccines.
2. Methods
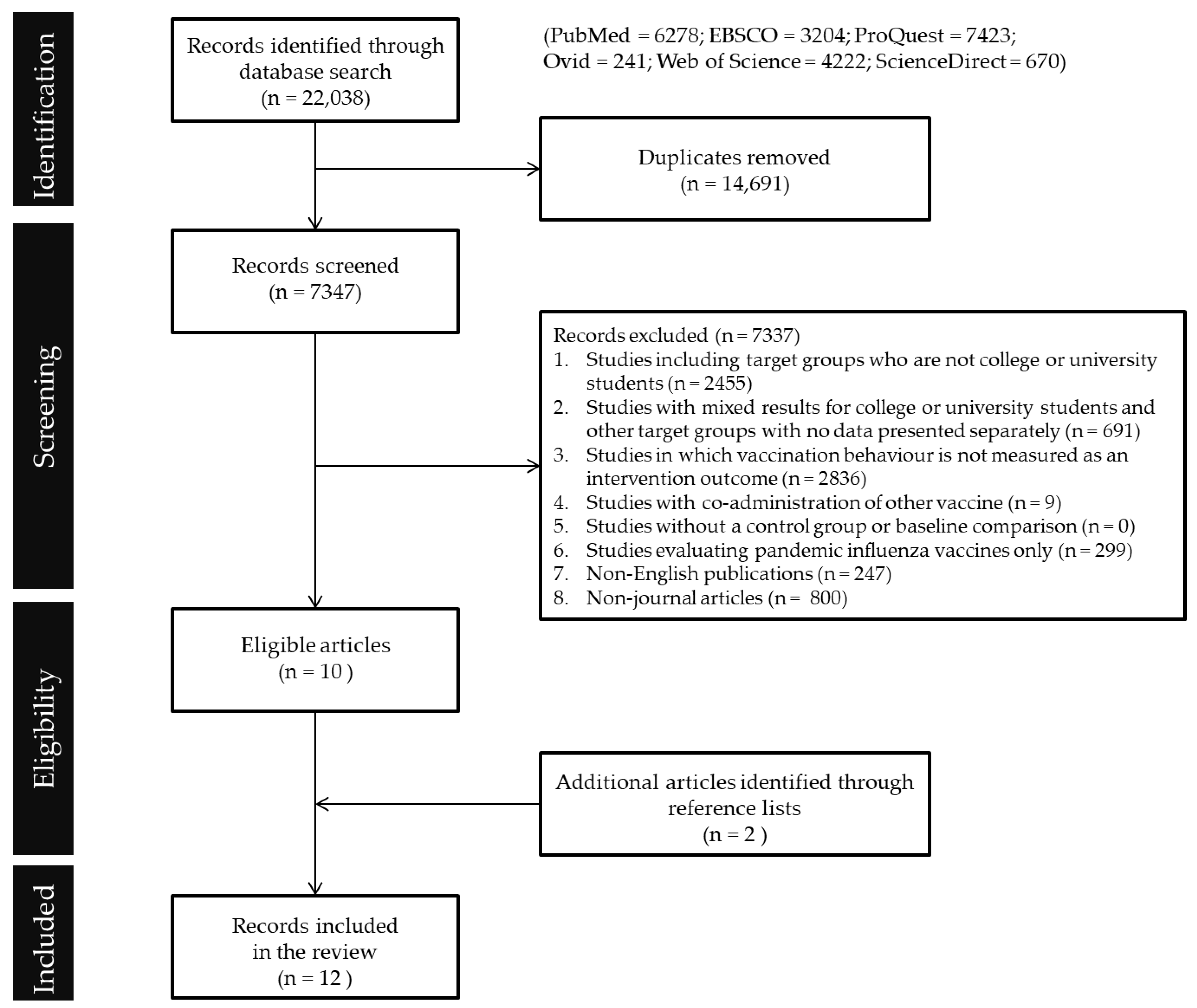
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction and Synthesis
3. Results
3.1. Study Characteristics
3.2. Vaccination Program Assessment against Social Marketing Components
3.2.1. Behavior Objectives and Outcomes
3.2.2. Audience Segmentation
3.2.3. Consumer Orientation
3.2.4. Competition
3.2.5. Theory
3.2.6. Insight
3.2.7. Exchange
3.2.8. Marketing Mix (4Ps)
4. Discussion
4.1. Lack of Studies on Vaccination Behavior in Countries beyond USA
4.2. Lack of Audience-Centric Approach in Program Design
4.3. Building Programs That Engage Students for Behavior Change
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Influenza (Seasonal). Available online: https://www.who.int/news-room/fact-sheets/detail/influenza-(seasonal) (accessed on 4 February 2020).
- Nichol, K.L.; D’Heilly, S.; Ehlinger, E.P. Influenza vaccination among college and university students: Impact on influenzalike illness, health care use, and impaired school performance. Arch. Pediatrics Adolesc. Med. 2008, 162, 1113–1118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delahoy, M.J.; Mortenson, L.; Bauman, L.; Marquez, J.; Bagdasarian, N.; Coyle, J.; Sumner, K.; Lewis, N.M.; Lauring, A.S.; Flannery, B. Influenza A (H3N2) outbreak on a university campus—Michigan, October–November 2021. Morb. Mortal. Wkly. Rep. 2021, 70, 1712. [Google Scholar] [CrossRef] [PubMed]
- Uchida, M.M.D.; Tsukahara, T.M.D.; Kaneko, M.M.D.; Washizuka, S.M.D.; Kawa, S.M.D. How the H1N1 influenza epidemic spread among university students in Japan: Experience from Shinshu University. Am. J. Infect. Control 2012, 40, 218–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, L.; Chu, C.; Yang, G.; Hao, R.; Li, Z.; Cao, Z.; Qiu, S.; Li, P.; Wu, Z.; Yuan, Z.; et al. Transmission Characteristics of Different Students during a School Outbreak of (H1N1) pdm09 Influenza in China, 2009. Sci. Rep. 2014, 4, 5982. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Vaccines against influenza WHO position paper—November 2012. Wkly. Epidemiol. Rec. 2012, 87, 461–476. [Google Scholar]
- Bhatt, H. Improving influenza vaccination rates during COVID-19 pandemic—the need of the hour. J. Glob. Health 2021, 11, 03042. [Google Scholar] [CrossRef] [PubMed]
- Plans-Rubió, P. The vaccination coverage required to establish herd immunity against influenza viruses. Prev. Med. 2012, 55, 72–77. [Google Scholar] [CrossRef]
- Larson, H.J.; Jarrett, C.; Eckersberger, E.; Smith, D.M.; Paterson, P. Understanding vaccine hesitancy around vaccines and vaccination from a global perspective: A systematic review of published literature, 2007–2012. Vaccine 2014, 32, 2150–2159. [Google Scholar] [CrossRef]
- Nowak, G.J.; Sheedy, K.; Bursey, K.; Smith, T.M.; Basket, M. Promoting influenza vaccination: Insights from a qualitative meta-analysis of 14 years of influenza-related communications research by US Centers for Disease Control and Prevention (CDC). Vaccine 2015, 33, 2741–2756. [Google Scholar] [CrossRef]
- Schmid, P.; Rauber, D.; Betsch, C.; Lidolt, G.; Denker, M.-L. Barriers of influenza vaccination intention and behavior–a systematic review of influenza vaccine hesitancy, 2005–2016. PLoS ONE 2017, 12, e0170550. [Google Scholar] [CrossRef]
- Fall, E.; Izaute, M.; Chakroun-Baggioni, N. How can the health belief model and self-determination theory predict both influenza vaccination and vaccination intention? A longitudinal study among university students. Psychol. Health 2018, 33, 746–764. [Google Scholar] [CrossRef] [PubMed]
- Shon, E.-J.; Choe, S.; Lee, L.; Ki, Y. Influenza vaccination among US college or university students: A systematic review. Am. J. Health Promot. 2021, 35, 708–719. [Google Scholar] [CrossRef] [PubMed]
- Bednarczyk, R.A.; Chu, S.L.; Sickler, H.; Shaw, J.; Nadeau, J.A.; McNutt, L.-A. Low uptake of influenza vaccine among university students: Evaluating predictors beyond cost and safety concerns. Vaccine 2015, 33, 1659–1663. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, Y.I.; Jin, Y.; Nowak, G. Motivating Influenza Vaccination Among Young Adults: The Effects of Public Service Advertising Message Framing and Text Versus Image Support. Soc. Mark. Q. 2018, 24, 89–103. [Google Scholar] [CrossRef]
- Bronchetti, E.T.; Huffman, D.B.; Magenheim, E. Attention, intentions, and follow-through in preventive health behavior: Field experimental evidence on flu vaccination. J. Econ. Behav. Organ. 2015, 116, 270–291. [Google Scholar] [CrossRef] [Green Version]
- Anskis, M. Swarthmore Economists Ask: What Convinces College Students to Get Flu Vaccines? Available online: https://www.swarthmore.edu/news-events/swarthmore-economists-ask-what-convinces-college-students-to-get-flu-vaccines (accessed on 1 April 2022).
- MacDonald, N.E. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- John, R.; Cheney, M.K. Resistance to Influenza Vaccination: Psychographics, Audience Segments, and Potential Promotions to Increase Vaccination. Soc. Mark. Q. 2008, 14, 67–90. [Google Scholar] [CrossRef]
- Nowak, G.J.; Gellin, B.G.; MacDonald, N.E.; Butler, R. Addressing vaccine hesitancy: The potential value of commercial and social marketing principles and practices. Vaccine 2015, 33, 4204–4211. [Google Scholar] [CrossRef] [Green Version]
- WHO. 2013 Guide to Tailoring Immunization Programmes. 2013. Available online: http://www.euro.who.int/en/health-topics/communicable-diseases/poliomyelitis/publications/2013/2013-guide-to-tailoring-immunization-programmes (accessed on 1 May 2021).
- Saunders, S.G.; Barrington, D.J.; Sridharan, S. Redefining social marketing: Beyond behavioural change. J. Soc. Mark. 2015, 5, 160–168. [Google Scholar] [CrossRef]
- Firestone, R.; Rowe, C.J.; Modi, S.N.; Sievers, D. The effectiveness of social marketing in global health: A systematic review. Health Policy Plan. 2016, 32, 110–124. [Google Scholar] [CrossRef] [Green Version]
- Craig Lefebvre, R.; Flora, J.A. Social marketing and public health intervention. Health Educ. Q. 1988, 15, 299–315. [Google Scholar] [CrossRef] [PubMed]
- Grier, S.; Bryant, C.A. Social marketing in public health. Annu. Rev. Public Health 2005, 26, 319–339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cates, J.R.; Diehl, S.J.; Crandell, J.L.; Coyne-Beasley, T. Intervention effects from a social marketing campaign to promote HPV vaccination in preteen boys. Vaccine 2014, 32, 4171–4178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hull, P.C.; Williams, E.A.; Khabele, D.; Dean, C.; Bond, B.; Sanderson, M. HPV vaccine use among African American girls: Qualitative formative research using a participatory social marketing approach. Gynecol. Oncol. 2014, 132, S13–S20. [Google Scholar] [CrossRef] [Green Version]
- Sundstrom, B.; Carr, L.A.; DeMaria, A.L.; Korte, J.E.; Modesitt, S.C.; Pierce, J.Y. Protecting the next generation: Elaborating the health belief model to increase HPV vaccination among college-age women. Soc. Mark. Q. 2015, 21, 173–188. [Google Scholar] [CrossRef]
- Evans, W.D.; French, J. Demand creation for COVID-19 vaccination: Overcoming vaccine hesitancy through social marketing. Vaccines 2021, 9, 319. [Google Scholar] [CrossRef]
- Wassler, P.; Del Chiappa, G.; Nguyen, T.H.H.; Fedeli, G.; Williams, N.L. Increasing vaccination intention in pandemic times: A social marketing perspective. Ital. J. Mark. 2022, 2022, 37–58. [Google Scholar] [CrossRef]
- Kunze, U.; Kunze, M. The Austrian vaccination paradox: Tick-borne encephalitis vaccination versus influenza vaccination. Cent. Eur. J. Public Health 2015, 23, 223. [Google Scholar] [CrossRef] [Green Version]
- Tetu-Mouradjian, L.M. Increasing annual influenza vaccinations among healthcare workers in Rhode Island: A social marketing approach. Rhode Isl. Med. J. 2010, 93, 271. [Google Scholar]
- Andreasen, A.R. Marketing Social Marketing in the Social Change Marketplace. J. Public Policy Mark. 2002, 21, 3–13. [Google Scholar] [CrossRef]
- National Social Marketing Centre. NSMC Benchmark Criteria. Available online: https://www.thensmc.com/content/nsmc-benchmark-criteria-0 (accessed on 7 December 2021).
- Slater, M.D. Theory and method in health audience segmentation. J. Health Commun. 1996, 1, 267–284. [Google Scholar] [CrossRef] [PubMed]
- Dietrich, T.; Rundle-Thiele, S.; Kubacki, K. Segmentation in Social Marketing: Process, Methods and Application; Springer: Singapore, 2017. [Google Scholar]
- Willmott, T.J.; Mathew, A.; Saleme, P.; Rundle-Thiele, S. Participatory design application in youth sexual violence and abuse prevention: A mixed-methods systematic review. Trauma Violence Abus. 2022, 15248380221078891. [Google Scholar] [CrossRef] [PubMed]
- Lahtinen, V.; Dietrich, T.; Rundle-Thiele, S. Long live the marketing mix. Testing the effectiveness of the commercial marketing mix in a social marketing context. J. Soc. Mark. 2020, 10, 357–375. [Google Scholar] [CrossRef]
- Carins, J.E.; Rundle-Thiele, S.R. Eating for the better: A social marketing review (2000–2012). Public Health Nutr. 2014, 17, 1628–1639. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2019. [Google Scholar]
- Koharchik, L.S.; Hardy, E.; Salman, K. Evidence-based initiative to improve influenza immunisation participation among undergraduate nursing students. J. Infect. Prev. 2012, 13, 186–191. [Google Scholar] [CrossRef]
- Shropshire, A.M.; Brent-Hotchkiss, R.; Andrews, U.K. Mass media campaign impacts influenza vaccine obtainment of university students. J. Am. Coll. Health 2013, 61, 435–443. [Google Scholar] [CrossRef] [PubMed]
- Roberto, A.J.; Mongeau, P.A.; Liu, Y.; Hashi, E.C. “Fear the Flu, Not the Flu Shot”: A Test of the Extended Parallel Process Model. J. Health Commun. 2019, 24, 829–836. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.-N.; Stück, D.; Konty, K.; Rivers, C.; Brown, C.R.; Zbikowski, S.M.; Foschini, L. Large-scale influenza vaccination promotion on a mobile app platform: A randomized controlled trial. Vaccine 2020, 38, 3508–3514. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.J.; Francesconi, M.; Cooper, M.H.; Covello, A.; Guo, M.; Gharib, S.D. Community health workers on a college campus: Effects on influenza vaccination. J. Am. Coll. Health 2018, 66, 317–323. [Google Scholar] [CrossRef]
- Hargrave, K. Interprofessional Collaboration Improves Uptake of Flu Vaccines on a College Campus. J. Christ. Nurs. 2020, 37, 221–227. [Google Scholar] [CrossRef] [PubMed]
- Hannings, A.N.; Darley, A.; Kearney, J.C.; Upchurch, B.L.; Groft, K. Marketing mobile influenza vaccine clinics on a college campus. J. Am. Pharm. Assoc. 2021, 62, 551–554. [Google Scholar] [CrossRef] [PubMed]
- Osborne, M.T.; Kenah, E.; Lancaster, K.; Tien, J. Catch the tweet to fight the flu: Using Twitter to promote flu shots on a college campus. J. Am. Coll. Health 2021, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Monn, J.L. An evidence-based project to improve influenza immunization uptake. J. Nurse Pract. 2016, 12, e159–e162. [Google Scholar] [CrossRef]
- Nyandoro, M.G.; Kelly, D.A.; Macey, D.J.; Mak, D.B. Student-centered interventions the key to student health care worker influenza vaccination. Infect. Dis. Health 2016, 21, 108–115. [Google Scholar] [CrossRef] [Green Version]
- Saro-Buendía, M.; Marrero-Sánchez, Á.; García-Ruiz de Morales, D.; Chiara-Graciani, G.; Coderch-Carretero, J.; Perez-Jacoiste Asin, M.A.; Silva, J.T.; Fernández-Ruiz, M.; Arrazola, P.; Aguado, J.M. Implementation of a program to improve influenza vaccination rates among medical students: A comparative study involving two university affiliated hospitals. Hum. Vaccines Immunother. 2021, 17, 3662–3669. [Google Scholar] [CrossRef] [PubMed]
- Borenstein, M.; Hedges, L.; Higgins, J.; Rothstein, H. Comprehensive Meta-Analysis Version 3; Biostat: Englewood, NJ, USA, 2013. [Google Scholar]
- Bryant, C.; Lindenberger, J.; Brown, C.; Kent, E.; Schreiber, J.M.; Bustillo, M.; Canright, M.W. A social marketing approach to increasing enrollment in a public health program: A case study of the Texas WIC program. Hum. Organ. 2001, 60, 234–246. [Google Scholar] [CrossRef]
- Lee, D.; Chong, G.C. Promoting Mobile Health Adoption to Hospital Patients Through Social Influencers: A Multi-Group Analysis Among Patients With High vs. Low Hospital Usage. Int. J. Healthc. Inf. Syst. Inform. 2021, 16, 1–15. [Google Scholar] [CrossRef]
- Rundle-Thiele, S.; Dietrich, T.; Carins, J. CBE: A framework to guide the application of marketing to behavior change. Soc. Mark. Q. 2021, 27, 175–194. [Google Scholar] [CrossRef]
- Xia, Y.; Deshpande, S.; Bonates, T. Effectiveness of Social Marketing Interventions to Promote Physical Activity Among Adults: A Systematic Review. J. Phys. Act. Health 2016, 13, 1263–1274. [Google Scholar] [CrossRef]
- Rundle-Thiele, S.; David, P.; Willmott, T.; Pang, B.; Eagle, L.; Hay, R. Social marketing theory development goals: An agenda to drive change. J. Mark. Manag. 2019, 35, 160–181. [Google Scholar] [CrossRef]
- White, S.; Park, Y.S.; Israel, T.; Cordero, E.D. Longitudinal evaluation of peer health education on a college campus: Impact on health behaviors. J. Am. Coll. Health 2009, 57, 497–506. [Google Scholar] [CrossRef] [PubMed]
- Rundle-Thiele, S.; Pang, B.; Knox, K.; David, P.; Parkinson, J.; Hussenoeder, F. Generating new directions for reducing dog and koala interactions: A social marketing formative research study. Australas. J. Environ. Manag. 2019, 26, 173–187. [Google Scholar] [CrossRef]
- Opel, D.J.; Diekema, D.S.; Lee, N.R.; Marcuse, E.K. Social marketing as a strategy to increase immunization rates. Arch. Pediatrics Adolesc. Med. 2009, 163, 432–437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cozza, V.; Alfonsi, V.; Rota, M.C.; Paolini, V.; Degli Atti, M.L.C. Promotion of influenza vaccination among health care workers: Findings from a tertiary care children’s hospital in Italy. BMC Public Health 2015, 15, 697. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, K.S.; Lam, T.P.; Kwok, K.W.; Lam, K.F.; Wu, D.; Ho, P.L. Seasonal influenza vaccine uptake among Chinese in Hong Kong: Barriers, enablers and vaccination rates. Hum. Vaccines Immunother. 2020, 1–10. [Google Scholar] [CrossRef]
- Jarrett, C.; Wilson, R.; O’Leary, M.; Eckersberger, E.; Larson, H.J. Strategies for addressing vaccine hesitancy—A systematic review. Vaccine 2015, 33, 4180–4190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, J.; While, A.E.; Norman, I.J. Knowledge and attitudes regarding influenza vaccination among nurses: A research review. Vaccine 2010, 28, 7207–7214. [Google Scholar] [CrossRef]
- Lee, D.; Rundle-Thiele, S.; Li, G. Motivating Seasonal Influenza Vaccination and Cross-Promoting COVID-19 Vaccination: An Audience Segmentation Study among University Students. Vaccines 2021, 9, 1397. [Google Scholar] [CrossRef]
- Kim, J.; Rundle-Thiele, S.; Knox, K. Systematic literature review of best practice in food waste reduction programs. J. Soc. Mark. 2019, 9, 447–466. [Google Scholar] [CrossRef]
- Benis, A.; Khodos, A.; Ran, S.; Levner, E.; Ashkenazi, S. Social media engagement and influenza vaccination during the COVID-19 pandemic: Cross-sectional survey study. J. Med. Internet Res. 2021, 23, e25977. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Study | Location | Duration of Vaccination Promotion Program | Target Audience |
|---|---|---|---|
| Koharchik et al. (2012) [42] | USA | 2011–12 flu season | Healthcare students |
| Nyandoro et al. (2016) [51] | Australia | 2014 flu season (March–June 2014) | |
| Saro-Buendía et al. (2021) [52] | Spain | 2018–19 flu season (October 2018–March 2019) | |
| Shropshire et al. (2013) [43] | USA | 2011–12 flu season (September 2011–February 2012) | University students |
| Bronchetti et al. (2015) [16] | USA | 2012–13 flu season (October–December 2012) | |
| Monn (2016) [50] | USA | 2014–15 flu season (September–December 2014) | |
| Huang et al. (2018) [46] | USA | Pilot program: 2013–14 flu season | |
| Enhanced program: 2014–15 and 2015–16 flu seasons | |||
| Roberto et al. (2019) [44] | USA | NA | |
| Hargrave (2020) [47] | USA | 2018–19 flu season (September 2018–February 2019) | |
| Osborne et al. (2021) [49] | USA | 2018–19 flu season (October 2018–May 2019) | |
| Hannings et al. (2021) [48] | USA | 2018–19 flu season | |
| Lee et al. (2020) [45] | USA | 2016–17 flu season (September–November 2016) | Young adults aged 18–27 |
| Behavior Outcomes (Vaccination Rate %) | |||||
|---|---|---|---|---|---|
| Study | Target Audience and Sample Size (n 1) | Study Design | Details of Seasonal Influenza Vaccination Promotion Program | Absolute | Difference vs. Baseline 2 and/or Control |
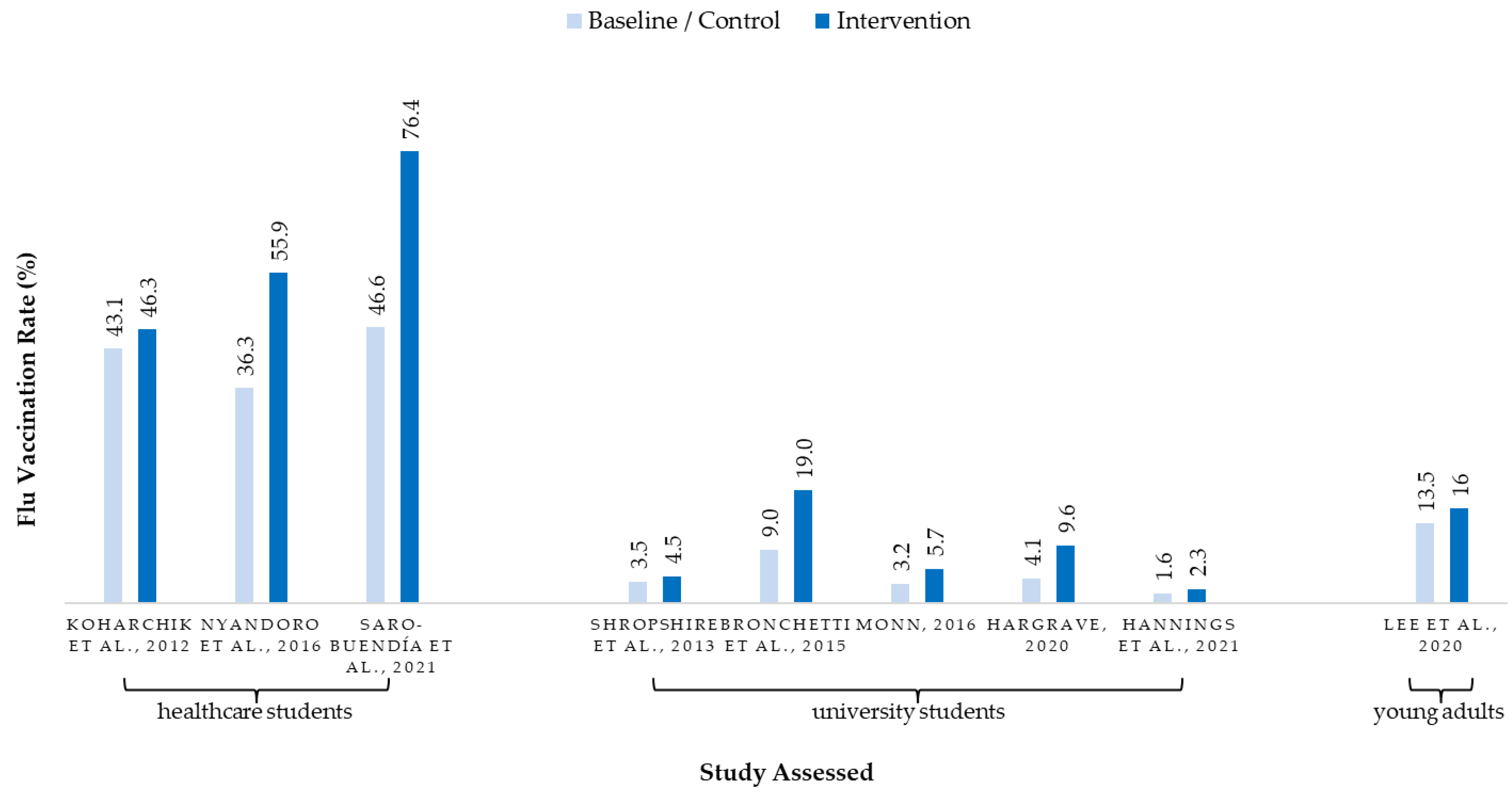
| Koharchik et al. [42] | Nursing students (n = unknown) | Pretest–posttest design | (1) Posters from the CDC urging immunization; (2) educational information shared in post-clinical conferences; (3) emails reminding dates and convenient locations of influenza clinics on campus; (4) a draw for gift cards to the university bookstore for vaccination | Intervention: 46.3% Previous year: 43.1% | +7% |
| Nyandoro et al. [51] | First-year medicine, nursing and midwifery, and physiotherapy students (n = 1620) | Pretest–posttest design | (1) Peer champions (who were trained with the evidence base behind the policy, efficacy and risks of influenza vaccination, information about convenient locations where students could get flu vaccination) delivered weekly reminders at lectures and through cohort specific social media outlets; (2) information pamphlet (printed and electronic) for peer champions and university staff to disseminate; (3) university staff, both on campus and at clinical placement sites, promote annual flu vaccination to the students. | Intervention: 55.9% Previous year: 36.3% | +54% |
| Saro-Buendía et al. [52] | Medical students of two universities (n = 1490) | Quasi experimental study | For both control and intervention groups: (1) educational materials (talks, posters, leaflets, and videos); (2) access to the vaccine (flexible hours, mobile teams, and free vaccination); (3) promotion of vaccination by HCWs; (4) rewards (badges and lanyards). Activities only for intervention group: (5) educational talks by senior years students; (6) flexible hours, mobile vaccine teams in teaching areas of the hospital; (7) reminder messages via Facebook and WhatsApp; (8) sticker on staff badge to identify those who have vaccinated. | Intervention: 76.4% Previous year: 46.6% Control: 55.3% Previous year: 42.7% | +27% |
| Shropshire et al. [43] | Undergraduate students (n = 720) | Pretest–posttest design | (1) Flyers, which had been implemented in previous year, were posted across campus (key locations such as dormitories, campus gym, and student union); (2) PowerPoint reminder slide (to be displayed by faculty members in class); (3) web banner on health center website, campus homepage, and campus Web portal and social media pages. | Intervention: 4.5% Previous year: 3.5% | +28% |
| Bronchetti et al. [16] | Students from six colleges (n = 9358) | Randomized controlled trial | Students were randomized into one of four conditions. Each group received the same number and timing of e-mails (one initial e-mail and two reminders) but the e-mail content was different. Group 1 (control)—on-campus vaccination information; Group 2 (incentive)—informing students that they could receive $30 cash if they get a flu vaccine at the campus health center by a specific date Group 3 (peer)—emails were sent from peer endorsers to recommend receiving flu vaccination Group 4 (coughing)—emails began with the text “Listen to this 3-s clip and imagine feeling like this during finals week!” with a link to an audio file of a sick person coughing. | Group 1 (control): 9% Group 2 (incentive): 19% Group 3 (peer): 8% Group 4 (coughing): 9% | No significant difference between group 3 (peer), group 4 (coughing), and the control. Group 2 (incentive): +119% * only +34% vs. control if cannibalization of off-campus vaccination is considered |
| Monn [50] | Post-graduate and undergraduate (n = 5248) | Pretest–posttest design | (1) Launched three vaccination clinics; (2) influenza information and reminders for immunization clinics were promoted on student health center Facebook page, college website, and campus-wide posters; (3) health center staff’s recommendation to students visiting the center. | Intervention: 5.7% Previous years: 3.2% | +78% |
| Huang et al. [46] | Students in 4 of the 6 dorms (n = unknown) | Quasi experimental study | Pilot: Health Peer Advisors and Liaisons (HealthPALs) greeted students at dining hall, informed them of the flu clinic, explained the benefits of vaccination, and answered students’ questions. | NA | +66% |
| Undergraduate students (n = 6635) | Intervention: In addition to (1) in-person outreach, HealthPALs conducted (2) a personalized social media campaign. (3) Dormitory-specific posters encouraging fellow residents to attend the nearest flu clinic. (4) HealthPALs distributed outreach materials through dormitory-wide email lists, social media websites, and printed postings in common spaces and hallways. (5) a new flu clinic. | NA | +85% * +58% if effect of newly added clinic is excluded | ||
| Roberto et al. [44] | College students n = 482 | Pretest–posttest design | Participants were randomly assigned to one of the four message exposure conditions: 2 (high threat/low threat) × 2 (high efficacy/low efficacy) Attitude and intentions towards flu shot were measured immediately after reading the message. Flu shot behavior was measured 30 days later. | HTHE: 20% HTLE: 17% LTHE: 23% LTLE: 16% | No effect for fear appeal messages (either efficacy or threat or their interaction effect) on behavior |
| Hargrave [47] | Undergraduate students (n = 1400) | Pretest–posttest design | (1) Implemented a one-day mobile flu shot clinic on campus; (2) partnered with local pharmacy that could bill students’ private health insurance (i.e., vaccination cost was reduced from USD20 to free of charge) | Intervention: 9.6% (no mobile clinic): 4.4% Historical average: 4.1% | +131% vs. 6-year average * +7% (if increase from mobile clinic is excluded) |
| Osborne et al. [49] | Undergraduate students (n = 702) | Randomized controlled trial | Control group—participants followed a control Twitter account that tweeted no content Intervention group—participants followed an intervention Twitter account that posted daily tweets promoting flu vaccination. Campaign engagement (e.g., retweet promotional tweets, construct own tweet containing a hashtag) was incentivized with prize raffle entries. | Vaccination rate of both intervention and control: ~45% | No significant difference between intervention and control groups |
| Hannings et al. [48] | 50,000 students and staff (n = unknown) | Pretest–posttest design | A campus-wide flu vaccination promotion campaign across: (1) e-mail; (2) digital or paper flyers; (3) onsite signage directing people to the mobile clinic locations; (4) university health center website and staff recommendations; (5) university publications; (6) local radio; (7) social media (Facebook, Instagram, Twitter); (8) student ambassador communication at campus events | Intervention: 2.3% Previous year: 1.6% | +44% |
| Lee et al. [45] | 50,286 individuals aged 18–65 in a local health plan. This table shows the rate of people aged 18–27 (n = unknown) | Randomized controlled trial | 3 batches of in-app message were sent to participants, with each batch sent every 2 weeks. Participants were randomized into three groups: Group 1: message encouraging flu vaccination with wellness points reward Group 2: message reminding uptake of flu vaccine without mentioning the reward Group 3: did not receive any in-app messages about flu vaccinations. Messages were arranged to send either (i) in a “timely” manner within two days of the expected prescription pickup by the person at pharmacy in which they may receive flu vaccine, or (ii) on a random delivery date | Intervention groups (messaged): 16% Control group (no message): 13.5% | +18.5% messaged group vs. control No significant difference between group 1 (message + incentive) vs. group 2 (reminder message only) |
| Study | Behavioral Change 1 | Audience Segmentation | Consumer Orientation 2 | Competition | Theory | Insight | Exchange | Marketing Mix |
|---|---|---|---|---|---|---|---|---|
| Koharchik et al. [42] 3 | √ (+7%) | ✕ | √ Lower level | ✕ | ✕ | ✕ | √ Raffles | √ All 4Ps |
| Nyandoro et al. [51] 3 | √ (+54%) | ✕ | √ Higher level | √ Off-campus vaccine at a fee | ✕ | √ | ✕ | √ All 4Ps |
| Saro-Buendía et al. [52] 3 | √ (+27%) | ✕ | √ Lower level | ✕ | ✕ | ✕ | √ ID badge sticker | √ All 4Ps |
| Shropshire et al. [43] | √ (+28%) | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | √ All 4Ps |
| Bronchetti et al. [16] | √ (+119%) | ✕ | ✕ | √ Off-campus substitution | √ Nudge theory | ✕ | √ Incentive | √ All 4Ps |
| Monn [50] | √ (+78%) | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | √ Price unknown |
| Huang et al. [46] | √ (+85%) | ✕ | √ Higher level | ✕ | √ Peer influence | √ | ✕ | √ All 4Ps |
| Roberto et al. [44] | ✕ | ✕ | ✕ | ✕ | √ Extended Parallel Process Model | ✕ | ✕ | √ No place or price |
| Hargrave [47] | √ (+131%) | ✕ | ✕ | √ Free off-campus vaccine (insurance) | √ Theory of planned behavior | ✕ | ✕ | √ Promotion not mentioned |
| Osborne et al. [49] | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | √ No place or price |
| Hannings et al. [48] | √ (+44%) | ✕ | ✕ | ✕ | ✕ | ✕ | ✕ | √ All 4Ps |
| Lee et al. [45] | √ (+18.5%) | ✕ | ✕ | ✕ | ✕ | ✕ | √ App points | √ All 4Ps |
| Study | Behavioral Change 1 | Place | Price | Marcom Channel | Message Appeal “Message” on Promotional Collaterals |
|---|---|---|---|---|---|
| Koharchik et al. [42] 2 | +7% | Convenient time and location of flu clinic | Free | Education talks, poster, email, raffles | Poster: an appeal to the moral responsibility that healthcare personnel have to their patients to increase immunization |
| Email: info on dates, convenient locations of influenza clinics, and raffles | |||||
| Nyandoro et al. [51] 2 | +54% | All hospital placement sites | Free | In-class peer promotion, cohort specific social media, posters | Tagline emphases on duty of care, professional responsibility and accountability: “Get a flu vaccination to protect you & your patients” |
| Saro-Buendía et al. [52] 2 | +27% | On-site vaccination in teaching areas | Free | Education talks, posters, leaflets, videos | “Let’s be more than 30% The sticker is for them. Less flu in 2019” |
| Shropshire et al. [43] | +28% | Flu clinic | Low-cost | In-class ppt slides, website banner ads, social media | Information on dates and price of influenza vaccination at campus health center |
| Bronchetti et al. [16] | +119% | Campus health center | Free (insurance plan or parents) | Emails | “Flu vaccine (get $30!)” |
| Monn [50] | +128% | Three vaccination clinics arranged | Free | Posters, Facebook post, College web portal, health center staff | Influenza information, recommendation to receive flu vaccine, time and locations of vaccination clinics |
| Huang et al. [46] | +85% | University flu clinic + a new clinic in dormitory | Free | Peer health advisors, posters, emails, social media | Tagline appealing to students’ community identity and sense of collective responsibility: “To protect not only themselves, but also others in their dormitory” |
| Roberto et al. [44] | No change | -- | -- | Ad exposure experiment | Feal appeal messages (threat vs. efficacy) |
| Hargrave [47] | +113% | Mobile “no-appointment necessary” clinic | Free (partnership with privacy pharmacy) | -- | -- |
| Osborne et al. [49] | No change | -- | -- | Social media (Twitter) | Tweets promoting flu vaccination |
| Hannings et al. [48] | +44% | Mobile clinic | Free (insurance plan) | e-mail, flyers, signage, website banner, university publications, local radio, social media, student ambassador | Encouraged the audience to get vaccinated using a “#FluGA” slogan as a university-wide campaign (but no benefits or cost info were featured) |
| Lee et al. [45] | +18.5% | Pharmacy in which participants pick up prescriptions | Free | In-app message (earn wellness points in app for flu vaccination) | App message: “Get a flu shot next time you visit a pharmacy” |
| App message that highlighted the incentive: “Flu shot = 200 points Get a flu shot next time you visit a pharmacy” |
| What worked | Studies |
| Free flu vaccine | [16,42,45,46,47,48,50,51,52] |
| Convenient flu shot locations | [42,45,46,47,48,50,51,52] |
| Multi-channel communications | [42,43,46,48,50,51,52] |
| Positive parental and peer influence | [43,46,52] |
| Incentive | [16,42] |
| Ads on university website | [43] |
| Vaccination reminder | [42] |
| What did not work | Studies |
| Social media | [43,49] |
| Education | [42] |
| Non-monetary nudges | [16] |
| Fear-appeal message | [44] |
| Repeated message | [45] |
| What else needs to be addressed | Studies |
| Lack of time | [42,52] |
| Intention not to get vaccinated | [16,42] |
| Lack of follow-through on intentions | [16] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, D.; Rundle-Thiele, S.; Wut, T.M.; Li, G. Increasing Seasonal Influenza Vaccination among University Students: A Systematic Review of Programs Using a Social Marketing Perspective. Int. J. Environ. Res. Public Health 2022, 19, 7138. https://doi.org/10.3390/ijerph19127138
Lee D, Rundle-Thiele S, Wut TM, Li G. Increasing Seasonal Influenza Vaccination among University Students: A Systematic Review of Programs Using a Social Marketing Perspective. International Journal of Environmental Research and Public Health. 2022; 19(12):7138. https://doi.org/10.3390/ijerph19127138
Chicago/Turabian StyleLee, Daisy, Sharyn Rundle-Thiele, Tai Ming Wut, and Gabriel Li. 2022. "Increasing Seasonal Influenza Vaccination among University Students: A Systematic Review of Programs Using a Social Marketing Perspective" International Journal of Environmental Research and Public Health 19, no. 12: 7138. https://doi.org/10.3390/ijerph19127138
APA StyleLee, D., Rundle-Thiele, S., Wut, T. M., & Li, G. (2022). Increasing Seasonal Influenza Vaccination among University Students: A Systematic Review of Programs Using a Social Marketing Perspective. International Journal of Environmental Research and Public Health, 19(12), 7138. https://doi.org/10.3390/ijerph19127138