
Clinical (BMI and MRI) and Biochemical (Adiponectin, Leptin, TNF-α, and IL-6) Effects of High-Intensity Aerobic Training with High-Protein Diet in Children with Obesity Following COVID-19 Infection

 ,
,  , , , , and
, , , , and
Abstract
:1. Introduction
2. Methods
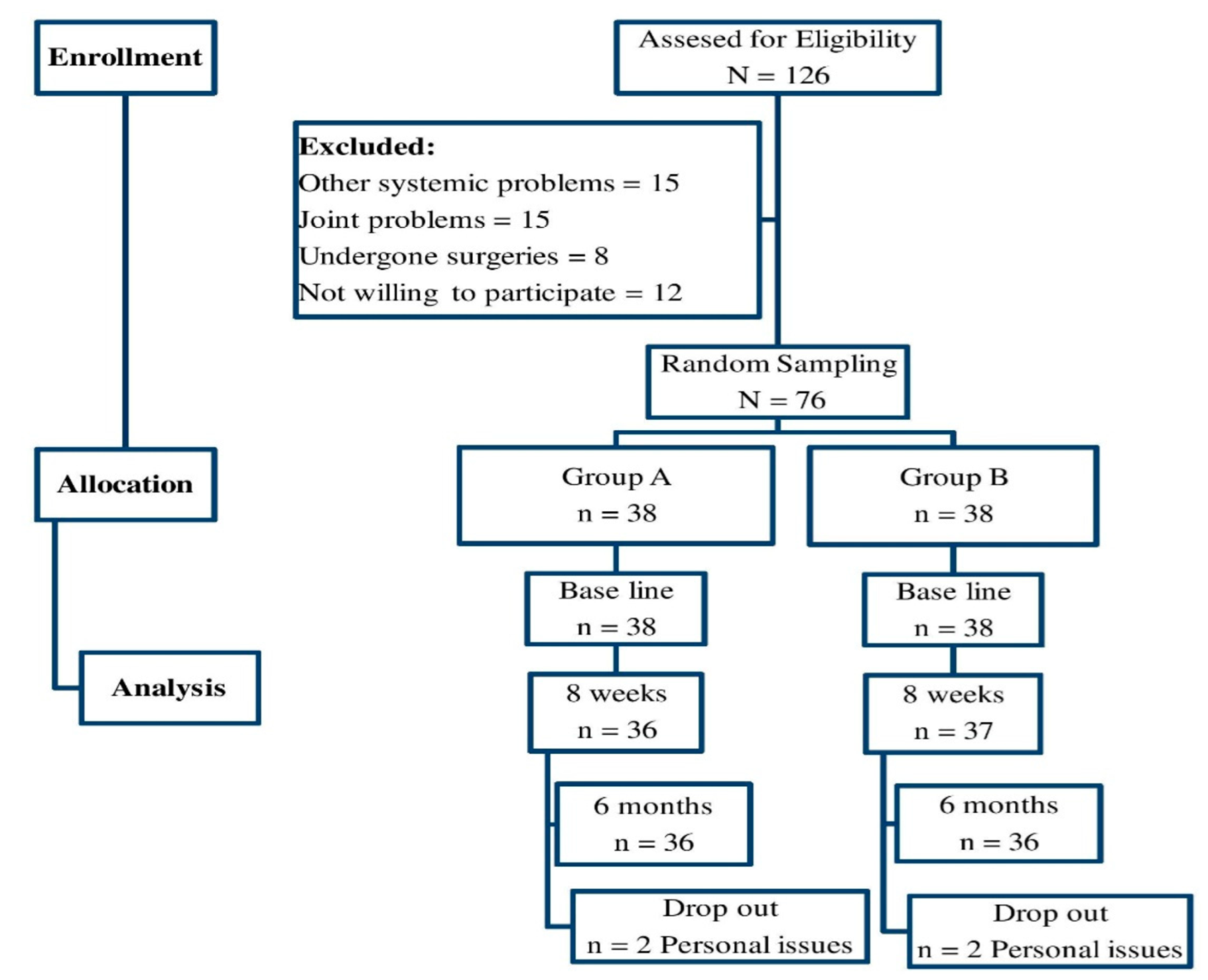
2.1. Study Design
2.2. Participants
2.3. Intervention
2.4. Outcome Measures
2.4.1. Body Mass Index (BMI)
2.4.2. Muscle
2.4.3. Biochemical Analysis
2.5. Sample Size
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nogueira-de-Almeida, C.A.; Ciampo, L.A.; Ferraz, I.S.; Del Ciampo, I.R.; Contini, A.A. COVID-19 and obesity in childhood and adolescence: A clinical review. J. Pediatr. 2020, 96, 546–558. [Google Scholar] [CrossRef]
- Kai, H.; Kai, M. Interactions of coronaviruses with ACE2, angiotensin II, and RAS inhibitors-lessons from available evidence and insights into COVID-19. Hypertens. Res. 2020, 43, 648–654. [Google Scholar] [CrossRef]
- Shekerdemian, L.S.; Mahmood, N.R.; Wolfe, K.K.; Riggs, B.J.; Ross, C.E.; McKiernan, C.A.; Heidemann, S.M.; Kleinman, L.C.; Sen, A.I.; Hall, M.W.; et al. Characteristics and outcomes of children with coronavirus disease 2019 (COVID-19) infection admitted to US and Canadian pediatric intensive care units. JAMA Pediatr. 2020, 174, 868. [Google Scholar] [CrossRef]
- Yumuk, V.; Tsigos, C.; Fried, M.; Schindler, K.; Busetto, L.; Micic, D.; Toplak, H. European guidelines for obesity management in adults. Obes. Facts 2015, 8, 402–424. [Google Scholar] [CrossRef]
- National Institutes of Health. Complementary, Alternative, or Integrative Health: What’s in a Name? National Center for Complementary and Integrative Health: Bethesda, MD, USA, 2020.
- Hussain, A.; Mahawar, K.; Xia, Z.; Yang, W.; El-Hasani, S. Obesity and mortality of COVID-19: Meta-analysis. Obes. Res. Clin. Pract. 2020, 14, 295–300. [Google Scholar] [CrossRef]
- Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N.; Margono, C.; Mullany, E.C.; Biryukov, S.; Abbafati, C.; Abera, S.F.; et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: A systematic analysis for the global burden of disease study 2013. Lancet 2014, 384, 766–781. [Google Scholar] [CrossRef]
- Frühbeck, G.; Baker, J.L.; Busetto, L.; Dicker, D.; Goossens, G.H.; Halford, J.C.G.; Handjieva-Darlenska, T.; Hassapidou, M.; Holm, J.-C.; Lehtinen-Jacks, S.; et al. European association for the study of obesity position statement on the global COVID-19 pandemic. Obes. Facts 2020, 13, 292–296. [Google Scholar] [CrossRef]
- Vamanu, E.; Rai, S. The Link between Obesity, Microbiota Dysbiosis, and Neurodegenerative Pathogenesis. Diseases 2021, 9, 45. [Google Scholar] [CrossRef]
- Cuschieri, S. COVID-19 panic, solidarity and equity—The Malta exemplary experience. J. Public Health 2020, 30, 459–464. [Google Scholar] [CrossRef]
- Kumar, S.; Kelly, A.S. Review of Childhood Obesity: From Epidemiology, Etiology, and Comorbidities to Clinical Assessment and Treatment. Mayo Clinc Proc. 2017, 92, 251–265. [Google Scholar] [CrossRef]
- Armoon, B.; Karimy, M. Epidemiology of childhood overweight, obesity and their related factors in a sample of preschool children from Central Iran. BMC Pediatr. 2019, 19, 159. [Google Scholar] [CrossRef]
- Kyrou, I.; Randeva, H.S.; Tsigos, C.; Kaltsas, G.; Weickert, M.O. Clinical Problems Caused by Obesity. In Endotext; Feingold, K.R., Anawalt, B., Boyce, A., Eds.; MDText.com, Inc.: South Dartmouth, MA, USA, 2000. [Google Scholar]
- Güngör, N.K. Overweight and obesity in children and adolescents. J. Clin. Res. Pediatr. Endocrinol. 2014, 6, 129–143. [Google Scholar] [CrossRef]
- Sheahan, T.P.; Sims, A.C.; Zhou, S.; Graham, R.L.; Pruijssers, A.J.; Agostini, M.L.; Leist, S.; Schafer, A.; Dinnon, K.H.; Stevens, L.J. An orally bioavailable broad-spectrum antiviral inhibits SARS-CoV-2 in human airway epithelial cell cultures and multiple coronaviruses in mice. Sci. Transl. Med. 2020; Epub ahead of print. [Google Scholar] [CrossRef]
- Bülbül, S. Exercise in the treatment of childhood obesity. Türk Pediatri Arşivi 2020, 55, 2–10. [Google Scholar]
- Kim, J.; Lim, H. Nutritional Management in Childhood Obesity. J. Obes. Metab. Syndr. 2019, 28, 225–235. [Google Scholar] [CrossRef]
- Shehadeh, M.B.; Suaifan, G.A.; Abu-Odeh, A.M.; Darwish, R.M. Complementary and alternative medicine use for weight management among females in Jordan: A community-based survey. East. Mediterr. Health J. 2020, 26, 443–452. [Google Scholar] [CrossRef]
- Upchurch, D.M.; Liang, L.; Sirois, F.M. A dual continuum model of the reasons for use of complementary health approaches among overweight and obese adults: Findings from the 2012 NHIS. BMC Complement. Altern. Med. 2018, 18, 339. [Google Scholar] [CrossRef]
- Ee, C.; Cave, A.E.; Naidoo, D.; Boyages, J. Prevalence of and attitudes towards complementary therapy use for weight after breast cancer in Australia: A national survey. BMC Complement. Altern. Med. 2019, 19, 332. [Google Scholar] [CrossRef]
- Styne, D.M.; Arslanian, S.A.; Connor, E.L.; Farooqi, I.S.; Murad, H.S.; Silverstein, J.H.; Yanovski, J.A. Pediatric Obesity-Assessment, Treatment, and Prevention: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol Metab. 2017, 102, 709–757. [Google Scholar] [CrossRef]
- Boutelle, K.N.; Rhee, K.E.; Liang, J.; Braden, A.; Douglas, J.; Strong, D.; Rock, C.L.; Wilfley, D.E.; Epstein, L.H.; Crow, S.J. Effect of Attendance of the Child on Body Weight, Energy Intake, and Physical Activity in Childhood Obesity Treatment: A Randomized Clinical Trial. JAMA Pediatr. 2017, 171, 622–628. [Google Scholar] [CrossRef]
- Shen, W.; Liu, H.; Punyanitya, M.; Chen, J.; Heymsfield, S.B. Pediatric obesity phenotyping by magnetic resonance methods. Curr. Opin. Clin. Nutr. Metab. Care 2005, 8, 595–601. [Google Scholar]
- Sirico, F.; Bianco, A.; D’Alicandro, G.; Castaldo, C.; Montagnani, S.; Spera, R.; Di Meglio, F.; Nurzynska, D. Effects of Physical Exercise on Adiponectin, Leptin, and Inflammatory Markers in Childhood Obesity: Systematic Review and Meta-Analysis. Child. Obes. 2018, 14, 207–217. [Google Scholar] [CrossRef]
- Guan, H.; Okely, A.D.; Aguilar-Farias, N.; Del Pozo Cruz, B.; Draper, C.E.; El Hamdouchi, A.; Florindo, A.A.; Jáuregui, A.; Katzmarzyk, P.T.; Kontsevaya, A.; et al. Promoting healthy movement behaviours among children during the COVID-19 pandemic. Lancet Child Adolesc. Health 2020, 4, 416–418. [Google Scholar] [CrossRef]
- Atlantis, E.; Barnes, E.H.; Singh, M.A.F. Efficacy of exercise for treating overweight in children and adolescents: A systematic review. Int. J. Obes. 2006, 30, 1027–1040. [Google Scholar] [CrossRef]
- Caspersen, C.J.; Powell, K.E.; Christenson, G. Physical activity, exercise and physical fitness: Definitions and distinctions for health-related research. Public Health Rep. 1985, 100, 126–131. [Google Scholar]
- Paes, S.T.; Marins, J.C.; Andreazzi, A.E. Efeitos metabólicos do exercício físico na obesidade infantil: Uma visão atual [Metabolic effects of exercise on childhood obesity: A current view]. Rev. Paul. Pediatr. 2015, 33, 122–129. [Google Scholar] [CrossRef]
- Goldthorpe, J.; Ali, N.; Calam, R. Providing healthy diets for young children: The experience of parents in a UK inner city. Int. J. Qual. Stud. Health Well-Being 2018, 13, 1490623. [Google Scholar] [CrossRef]
- Tripathi, M.; Mishra, S.K. Screen time and adiposity among children and adolescents: A systematic review. J. Public Health 2019, 28, 227–244. [Google Scholar] [CrossRef]
- Beals, J.W.; Burd, N.A.; Moore, D.; van Vliet, S. Obesity Alters the Muscle Protein Synthetic Response to Nutrition and Exercise. Front. Nutr. 2019, 6, 87. [Google Scholar] [CrossRef]
- Dideriksen, K.; Reitelseder, S.; Holm, L. Influence of amino acids, dietary protein, and physical activity on muscle mass development in humans. Nutrients 2013, 5, 852–876. [Google Scholar] [CrossRef]
- Koopman, R.; Walrand, S.; Beelen, M.; Gijsen, A.P.; Kies, A.K.; Boirie, Y.; Saris, W.H.M.; Van Loon, L.J.C. Dietary protein digestion and absorption rates and the subsequent postprandial muscle protein synthetic response do not differ between young and elderly men. J. Nutr. 2009, 139, 1707–1713. [Google Scholar] [CrossRef]
- Roth, S.; Ivey, F.M.; Martel, G.F.; Lemmer, J.T.; Ms, D.E.H.; Siegel, E.L.; Metter, E.J.; Fleg, J.L.; Fozard, J.L.; Ms, M.C.K.; et al. muscle size responses to strength training in young and older men and women. J. Am. Geriatr. Soc. 2001, 49, 1428–1433. [Google Scholar] [CrossRef]
- Yanai, H.; Yoshida, H. Beneficial Effects of Adiponectin on Glucose and Lipid Metabolism and Atherosclerotic Progression: Mechanisms and Perspectives. Int. J. Mol. Sci. 2019, 20, 1190. [Google Scholar] [CrossRef]
- Wu, S.; Bhat, Z.F.; Gounder, R.S.; Ahmed, I.A.M.; Al-Juhaimi, F.Y.; Ding, Y.; Bekhit, A.E. Effect of Dietary Protein and Processing on Gut Microbiota—A Systematic Review. Nutrients 2022, 14, 453. [Google Scholar] [CrossRef]
- Kondo, T.; Kobayashi, I.; Murakami, M. Effect of exercise on circulating adipokine levels in obese young women. Endocr. J. 2006, 53, 189–195. [Google Scholar] [CrossRef]
- Blüher, M.; Bullen, J.W.; Lee, J.H.; Kralisch, S.; Fasshauer, M.; Klöting, N.; Niebauer, J.; Schön, M.R.; Williams, C.J.; Mantzoros, C.S. Circulating adiponectin and expression of adiponectin receptors in human skeletal muscle: Associations with metabolic parameters and insulin resistance and regulation by physical training. J. Clin. Endocrinol. Metab. 2006, 91, 2310–2316. [Google Scholar] [CrossRef]
- Nassis, G.P.; Papantakou, K.; Skenderi, K.; Triandafillopoulou, M.; Kavouras, S.; Yannakoulia, M.; Chrousos, G.P.; Sidossis, L.S. Aerobic exercise training improves insulin sensitivity without changes in body weight, body fat, adiponectin, and inflammatory markers in overweight and obese girls. Metabolism 2005, 54, 1472–1479. [Google Scholar] [CrossRef]
- Esposito, K.; Pontillo, A.; Di Palo, C.; Giugliano, G.; Masella, M.; Marfella, R.; Giugliano, D. Effect of weight loss and lifestyle changes on vascular inflammatory markers in obese women: A randomized trial. JAMA 2003, 289, 1799–1804. [Google Scholar] [CrossRef]
- Kim, E.S.; Im, J.-A.; Kim, K.C.; Park, J.H.; Suh, S.-H.; Kang, E.S.; Kim, S.H.; Jekal, Y.; Lee, C.W.; Yoon, Y.-J.; et al. Improved insulin sensitivity and adiponectin level after exercise training in obese Korean youth. Obesity 2007, 15, 3023–3030. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Sr. No | Variable | Group A | Group B | p-Value |
|---|---|---|---|---|
| 1 | Age (y) | 10.12 ± 1.2 | 10.56 ± 1.4 | 0.145 |
| 2 | Height (m) | 1.28 ± 0.12 | 1.30 ± 0.10 | 0.432 |
| 3 | Weight (kg) | 43.8 ± 4.3 | 44.2 ± 4.8 | 0.703 |
| 4 | VO2peak (mL/kg/min) | 40.3 ± 3.9 | 39.2 ± 3.6 | 0.205 |
| 5 | HR (beats/min) | 76.8 ± 5.5 | 78.2 ± 4.9 | 0.245 |
| Sr. No | Variable | Duration | Group A | Group B | p-Value |
|---|---|---|---|---|---|
| 1 | Body mass index % (Percentile) | Base line | 98.8 ± 3.5 | 99.1 ± 3.7 | 0.717 |
| 8 weeks | 96.5 ± 3.4 | 99.3 ± 3.7 | 0.001 * | ||
| 6 months | 93.2 ± 3.1 | 99.5 ± 3.8 | 0.001 * | ||
| p-value | 0.001 * | 0.896 | |||
| 2 | Muscle quantity—CSA (MRI—Mid-arm: cm2) | Base line | 59.8 ± 5.1 | 58.9 ± 5.3 | 0.453 |
| 8 weeks | 48.2 ± 4.7 | 59.0 ± 5.3 | 0.001 | ||
| 6 months | 42.2 ± 4.5 | 59.2 ± 5.5 | 0.119 | ||
| p-value | 0.001 * | 0.969 | |||
| 3 | Muscle quantity—CSA (MRI—Mid-thigh: cm2) | Base line | 67.2 ± 5.5 | 67.1 ± 5.6 | 0.937 |
| 8 weeks | 61.2 ± 5.3 | 68.9 ± 5.5 | 0.001 * | ||
| 6 months | 56.5 ± 5.2 | 69.6 ± 5.7 | 0.001 * | ||
| p-value | 0.001 * | 0.138 | |||
| 4 | Muscle quantity—CSA (MRI—Mid-calf: cm2) | Base line | 59.5 ± 4.6 | 58.9 ± 4.5 | 0.567 |
| 8 weeks | 52.5 ± 4.1 | 59.5 ± 4.8 | 0.001 * | ||
| 6 months | 48.3 ± 3.9 | 59.6 ± 4.8 | 0.001 * | ||
| p-value | 0.001 * | 0.782 | |||
| 5 | Adiponectin (μg/mL) | Base line | 7.52 ± 0.4 | 7.45 ± 0.5 | 0.502 |
| 8 weeks | 8.74 ± 0.5 | 7.41 ± 0.5 | 0.001 * | ||
| 6 months | 9.28 ± 0.6 | 7.38 ± 0.4 | 0.001 * | ||
| p-value | 0.001 * | 0.808 | |||
| 6 | Leptin (ng/mL) | Base line | 12.25 ± 0.2 | 12.15 ± 0.3 | 0.091 |
| 8 weeks | 9.33 ± 0.2 | 12.34 ± 0.3 | 0.001 * | ||
| 6 months | 7.25 ± 0.1 | 12.18 ± 0.4 | 0.001 * | ||
| p-value | 0.001 * | 0.833 | |||
| 7 | TNF-α (pg/mL) | Base line | 1.7 ± 0.1 | 1.7 ± 0.2 | 1.000 |
| 8 weeks | 1.5 ± 0.1 | 1.7 ± 0.2 | 0.001 * | ||
| 6 months | 1.3 ± 0.1 | 1.8 ± 0.2 | 0.001 * | ||
| p-value | 0.001 * | 0.046 | |||
| 8 | IL-6 (pg/mL) | Base line | 0.56 ± 0.04 | 0.57 ± 0.05 | 0.338 |
| 8 weeks | 0.49 ± 0.04 | 0.58 ± 0.06 | 0.001 * | ||
| 6 months | 0.38 ± 0.03 | 0.59 ± 0.06 | 0.001 * | ||
| p-value | 0.001 * | 0.312 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nambi, G.; Alghadier, M.; Elnegamy, T.E.; Basuodan, R.M.; Alwhaibi, R.M.; Vellaiyan, A.; Nwihadh, N.A.; Aldhafian, O.R.; Verma, A.; Pakkir Mohamed, S.H.; et al. Clinical (BMI and MRI) and Biochemical (Adiponectin, Leptin, TNF-α, and IL-6) Effects of High-Intensity Aerobic Training with High-Protein Diet in Children with Obesity Following COVID-19 Infection. Int. J. Environ. Res. Public Health 2022, 19, 7194. https://doi.org/10.3390/ijerph19127194
Nambi G, Alghadier M, Elnegamy TE, Basuodan RM, Alwhaibi RM, Vellaiyan A, Nwihadh NA, Aldhafian OR, Verma A, Pakkir Mohamed SH, et al. Clinical (BMI and MRI) and Biochemical (Adiponectin, Leptin, TNF-α, and IL-6) Effects of High-Intensity Aerobic Training with High-Protein Diet in Children with Obesity Following COVID-19 Infection. International Journal of Environmental Research and Public Health. 2022; 19(12):7194. https://doi.org/10.3390/ijerph19127194
Chicago/Turabian StyleNambi, Gopal, Mshari Alghadier, Tamer E. Elnegamy, Reem M. Basuodan, Reem M. Alwhaibi, Arul Vellaiyan, Naif A. Nwihadh, Osama R. Aldhafian, Anju Verma, Shahul Hameed Pakkir Mohamed, and et al. 2022. "Clinical (BMI and MRI) and Biochemical (Adiponectin, Leptin, TNF-α, and IL-6) Effects of High-Intensity Aerobic Training with High-Protein Diet in Children with Obesity Following COVID-19 Infection" International Journal of Environmental Research and Public Health 19, no. 12: 7194. https://doi.org/10.3390/ijerph19127194
APA StyleNambi, G., Alghadier, M., Elnegamy, T. E., Basuodan, R. M., Alwhaibi, R. M., Vellaiyan, A., Nwihadh, N. A., Aldhafian, O. R., Verma, A., Pakkir Mohamed, S. H., Chevidikunnan, M. F., & Khan, F. (2022). Clinical (BMI and MRI) and Biochemical (Adiponectin, Leptin, TNF-α, and IL-6) Effects of High-Intensity Aerobic Training with High-Protein Diet in Children with Obesity Following COVID-19 Infection. International Journal of Environmental Research and Public Health, 19(12), 7194. https://doi.org/10.3390/ijerph19127194