
Oral Hygiene in Adolescence: A Questionnaire-Based Study





Abstract
:1. Introduction
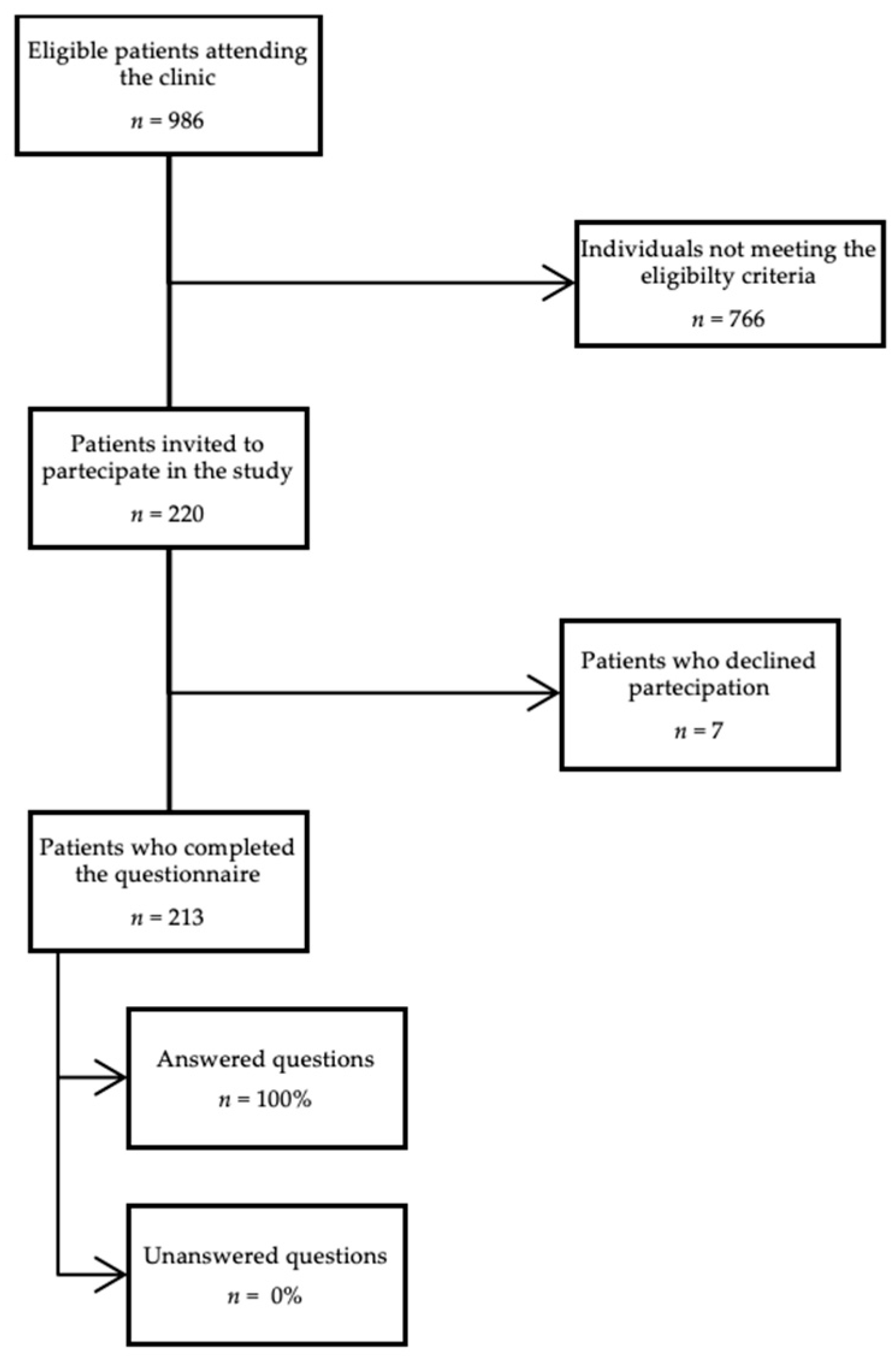
2. Materials and Methods
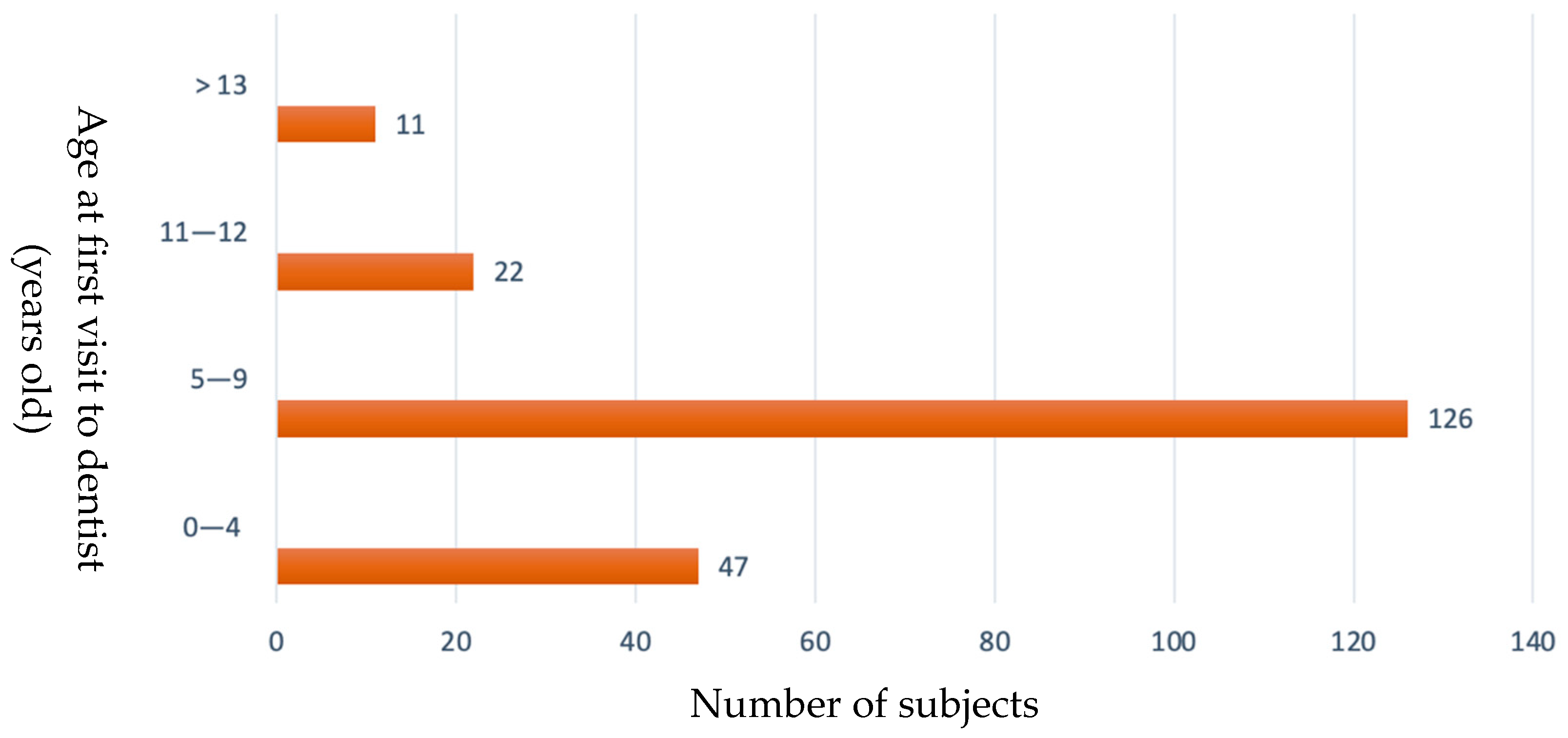
3. Results
3.1. Oral Hygiene at Home
3.2. Professional Oral Hygiene
3.3. Education on Oral Hygiene at Home
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sawyer, S.M.; Azzopardi, P.S.; Wickremarathne, D.; Patton, G.C. The Age of Adolescence. Lancet Child Adolesc. Health 2018, 2, 223–228. [Google Scholar] [CrossRef]
- Vijayakumar, N.; op de Macks, Z.; Shirtcliff, E.A.; Pfeifer, J.H. Puberty and the Human Brain: Insights into Adolescent Development. Neurosci. Biobehav. Rev. 2018, 92, 417–436. [Google Scholar] [CrossRef]
- Mascarenhas, P.; Gapski, R.; Al-Shammari, K.; Wang, H.L. Influence of Sex Hormones on the Periodontium. J. Clin. Periodontol. 2003, 30, 671–681. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, S.; Fujii, H.; Machida, Y.; Okuda, K. A Longitudinal Study from Prepuberty to Puberty of Gingivitis: Correlation between the Occurrence of Prevotella Intermedia and Sex Hormones. J. Clin. Periodontol. 1994, 21, 658–665. [Google Scholar] [CrossRef]
- Wojcicki, C.J.; Harper, D.S.; Robinson, P.J. Differences in Periodontal Disease-Associated Microorganisms of Subgingival Plaque in Prepubertal, Pubertal and Postpubertal Children. J. Periodontol. 1987, 58, 219–223. [Google Scholar] [CrossRef] [PubMed]
- Van Loveren, C. Sugar Restriction for Caries Prevention: Amount and Frequency. Which Is More Important? Caries Res. 2019, 53, 168–175. [Google Scholar] [CrossRef]
- Guideline: Sugars Intake for Adults and Children. Available online: https://www.who.int/publications/i/item/9789241549028 (accessed on 31 May 2022).
- Thomas, D.M.; Mirowski, G.W. Nutrition and Oral Mucosal Diseases. Clin. Dermatol. 2010, 28, 426–431. [Google Scholar] [CrossRef]
- Gigena, P.C.; Cornejo, L.S.; Lescano-de-Ferrer, A. Oral Health in Drug Addict Adolescents and Non Psychoactive Substance Users. Acta Odontol. Latinoam. AOL 2015, 28, 48–57. [Google Scholar] [CrossRef]
- Jansson, L. Association between Alcohol Consumption and Dental Health. J. Clin. Periodontol. 2008, 35, 379–384. [Google Scholar] [CrossRef]
- Seneviratne, C.J.; Zhang, C.F.; Samaranayake, L.P. Dental plaque biofilm in oral health and disease. Chin. J. Dent. Res. 2011, 14, 87–94. [Google Scholar]
- Alhaija, E.S.A.; Al-Saif, E.M.; Taani, D.Q. Periodontal Health Knowledge and Awareness among Subjects with Fixed Orthodontic Appliance. Dent. Press J. Orthod. 2018, 23, e1–e40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cozzani, M.; Ragazzini, G.; Delucchi, A.; Mutinelli, S.; Barreca, C.; Rinchuse, D.J.; Servetto, R.; Piras, V. Oral Hygiene Compliance in Orthodontic Patients: A Randomized Controlled Study on the Effects of a Post-Treatment Communication. Prog. Orthod. 2016, 17, 41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qu, X.; Houser, S.H.; Tian, M.; Zhang, Q.; Pan, J.; Zhang, W. Effects of Early Preventive Dental Visits and Its Associations with Dental Caries Experience: A Cross-Sectional Study. BMC Oral Health 2022, 22, 150. [Google Scholar] [CrossRef]
- Ericsson, J.S.; Östberg, A.L.; Wennström, J.L.; Abrahamsson, K.H. Oral Health-Related Perceptions, Attitudes, and Behavior in Relation to Oral Hygiene Conditions in an Adolescent Population. Eur. J. Oral Sci. 2012, 120, 335–341. [Google Scholar] [CrossRef] [PubMed]
- Graça, S.R.; Albuquerque, T.S.; Luis, H.S.; Assunção, V.A.; Malmqvist, S.; Cuculescu, M.; Slusanschi, O.; Johannsen, G.; Galuscan, A.; Podariu, A.C.; et al. Oral Health Knowledge, Perceptions, and Habits of Adolescents from Portugal, Romania, and Sweden: A Comparative Study. J. Int. Soc. Prev. Community Dent. 2019, 9, 470–480. [Google Scholar] [CrossRef] [PubMed]
- Nasir, E.F.; Vu, J. Oral Hygiene Practice among 18-Year-Old Norwegian Adolescents Using Health Belief Model: A Cross-Sectional Study. Eur. J. Dent. 2022, 16, 56–63. [Google Scholar] [CrossRef]
- Veiga, N.J.; Pereira, C.M.; Ferreira, P.C.; Correia, I.J. Oral Health Behaviors in a Sample of Portuguese Adolescents: An Educational Issue. Health Promot Perspect 2014, 4, 35–45. [Google Scholar] [CrossRef] [Green Version]
- Inquimbert, C.; Clement, C.; Couatarmanach, A.; Tramini, P.; Bourgeois, D.; Carrouel, F. Oral Hygiene Practices and Knowledge among Adolescents Aged between 15 and 17 Years Old during Fixed Orthodontic Treatment: Multicentre Study Conducted in France. Int. J. Environ. Res. Public Health 2022, 19, 2316. [Google Scholar] [CrossRef]
- Alshahrani, N.F.; Alshahrani, A.N.A.; Alahmari, M.A.; Almanie, A.M.; Alosbi, A.M.; Togoo, R.A. First Dental Visit: Age, Reason, and Experiences of Saudi Children. Eur. J. Dent. 2018, 12, 579–584. [Google Scholar] [CrossRef]
- Mika, A.; Mitus-Kenig, M.; Zeglen, A.; Drapella-Gasior, D.; Rutkowska, K.; Josko-Ochojska, J. The Child’s First Dental Visit. Age, Reasons, Oral Health Status and Dental Treatment Needs among Children in Southern Poland. Eur. J. Paediatr. Dent. 2018, 19, 265–370. [Google Scholar] [CrossRef]
- Mileva, S.P.; Kondeva, V.K. Age at and Reasons for the First Dental Visit. Folia Med. 2010, 52, 56–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Savage, M.F.; Lee, J.Y.; Kotch, J.B.; Vann, W.F. Early Preventive Dental Visits: Effects on Subsequent Utilization and Costs. Pediatrics 2004, 114, e418–e423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sälzer, S.; Slot, D.E.; van der Weijden, F.A.; Dörfer, C.E. Efficacy of Inter-Dental Mechanical Plaque Control in Managing Gingivitis—A Meta-Review. J. Clin. Periodontol. 2015, 42, S92–S105. [Google Scholar] [CrossRef] [Green Version]
- Mattos-Silveira, J.; Matos-Lima, B.B.; Oliveira, T.A.; Jarroug, K.; Rego, R.V.; Reyes, A.; Ferreira, F.R.; Imparato, J.C.; Braga, M.M. Why Do Children and Adolescents Neglect Dental Flossing? Eur. Arch. Paediatr. Dent. 2017, 18, 45–50. [Google Scholar] [CrossRef]
- Matsui, M.; Chosa, N.; Shimoyama, Y.; Minami, K.; Kimura, S.; Kishi, M. Effects of Tongue Cleaning on Bacterial Flora in Tongue Coating and Dental Plaque: A Crossover Study. BMC Oral Health 2014, 14, 4. [Google Scholar] [CrossRef] [Green Version]
- Furuta, M.; Ekuni, D.; Irie, K.; Azuma, T.; Tomofuji, T.; Ogura, T.; Morita, M. Sex Differences in Gingivitis Relate to Interaction of Oral Health Behaviors in Young People. J. Periodontol. 2011, 82, 558–565. [Google Scholar] [CrossRef]
- Östberg, A.L.; Halling, A.; Lindblad, U. Gender Differences in Knowledge, Attitude, Behavior and Perceived Oral Health among Adolescents. Acta Odontol. Scand. 1999, 57, 231–236. [Google Scholar] [CrossRef]
- Al-Ansari, J.M.; Honkala, S. Gender Differences in Oral Health Knowledge and Behavior of the Health Science College Students in Kuwait. J. Allied Health 2007, 36, 41–46. [Google Scholar]
- Migliorati, M.; Isaia, L.; Cassaro, A.; Rivetti, A.; Silvestrini-Biavati, F.; Gastaldo, L.; Piccardo, I.; Dalessandri, D.; Silvestrini-Biavati, A. Efficacy of Professional Hygiene and Prophylaxis on Preventing Plaque Increase in Orthodontic Patients with Multibracket Appliances: A Systematic Review. Eur. J. Orthod. 2015, 37, 297–307. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Questionnaire | ||
|---|---|---|
| General information | Sex |
|
| Have you ever visited a dentist? |
| |
| If so, when was the first time you did it? (years old) |
| |
| Oral hygiene at home | How many times a day do you brush your teeth? |
|
| What type of toothbrush do you use? (It is possible to choose more than one answer) |
| |
| Have you ever used dental floss? |
| |
| Do you use any other tools for your oral hygiene at home? |
| |
| If so, which ones? | …............... | |
| Do you also clean your tongue after tooth brushing? |
| |
| Professional Oral Hygiene | Do you know what professional oral hygiene is? |
|
| Have you ever undergone professional oral hygiene? |
| |
| If so, how many times a year? |
| |
| Do you wear braces? |
| |
| Have you ever worn it? |
| |
| During the orthodontic treatment, has your dentist ever recommended that you undergo professional oral hygiene? |
| |
| Oral hygiene instructions | Who provided you with training on oral hygiene? (It is possible to choose more than one option) |
|
| Have you ever attended meetings on oral hygiene held by a dentist or dental hygiene at school or anywhere else? |
| |
| Would you like to receive more information about oral health? |
| |
| Total | Males | Females | Orthodontics | No Orthodontics | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Type of toothbrush | ||||||||||
| Electric | 29 | (13.6%) | 13 | (18.8%) | 16 | (11.1%) | 5 | (10.9%) | 24 | (14.4%) |
| Manual | 161 | (75.6%) | 56 | (81.2%) | 105 | (72.9%) | 34 | (73.9%) | 127 | (76.0%) |
| Sonic | 0 | (0.0%) | 0 | (0.0%) | 0 | (0.0%) | 0 | (0.0%) | 0 | (0.0%) |
| Electric and manual | 23 | (10.8%) | 0 | (0.0%) | 23 | (16.0%) | 7 | (15.2%) | 0 | (0.0%) |
| Teeth brushing | ||||||||||
| Never | 2 | (0.9%) | 2 | (2.9%) | 0 | (0.0%) | 0 | (0.0%) | 2 | (1.2%) |
| Once a day (morning) | 24 | (11.3%) | 7 | (10.1%) | 17 | (11.8%) | 3 | (6.5%) | 21 | (12.6%) |
| Once a day (evening) | 10 | (4.7%) | 5 | (7.2%) | 5 | (3.5%) | 3 | (6.5%) | 7 | (4.2%) |
| Twice a day | 128 | (60.1%) | 46 | (66.7%) | 82 | (56.9%) | 28 | (60.9%) | 100 | (59.9%) |
| Three times a day | 46 | (21.6%) | 9 | (13.0%) | 37 | (25.7%) | 11 | (23.9%) | 35 | (21.0%) |
| More than 3 times a day | 3 | (1.4%) | 0 | (0.0%) | 3 | (2.1%) | 1 | (2.2%) | 2 | (1.2%) |
| Flossing | ||||||||||
| Never tried it | 64 | (30.0%) | 24 | (34.8%) | 40 | (27.8%) | 12 | (26.1%) | 52 | (31.1%) |
| No, I tried but did not like it | 75 | (35.2%) | 27 | (39.1%) | 48 | (33.3%) | 13 | (28.3%) | 62 | (37.1%) |
| Once a week | 27 | (12.7%) | 9 | (13.0%) | 18 | (12.5%) | 7 | (15.2%) | 20 | (12.0%) |
| More than once a week | 20 | (9.4%) | 4 | (5.8%) | 16 | (11.1%) | 7 | (15.2%) | 13 | (7.8%) |
| Once a day | 15 | (7.0%) | 3 | (4.3%) | 12 | (8.3%) | 5 | (10.9%) | 10 | (6.0%) |
| Other | 12 | (5.6%) | 2 | (2.9%) | 10 | (6.9%) | 5 | (10.9%) | 7 | (4.2%) |
| Tongue cleaning | ||||||||||
| Yes | 104 | (48.8%) | 29 | (42.0%) | 75 | (52.1%) | 26 | (56.5%) | 78 | (46.7%) |
| No | 109 | (51.2%) | 40 | (58.0%) | 69 | (47.9%) | 20 | (43.5%) | 89 | (53.3%) |
| Professional Oral Hygiene | ||||||
|---|---|---|---|---|---|---|
| Total | Orthodontics | No orthodontics | ||||
| 213 Subjects | 46 Subjects | 167 Subjects | ||||
| Awareness of professional oral hygiene | 176 | 83% | 35 | 76% | 131 | 78% |
| Use of professional oral hygiene | 143 | 67% | 34 | 74% | 109 | 65% |
| Frequency of use of professional oral hygiene | ||||||
| Once | 52 | 36% | 9 | 20% | 43 | 26% |
| Less than once a year | 16 | 8% | 5 | 11% | 11 | 7% |
| Once a year | 37 | 17% | 9 | 20% | 28 | 17% |
| Twice a year | 32 | 15% | 6 | 13% | 26 | 16% |
| More than twice a year | 6 | 3% | 5 | 11% | 1 | 1% |
| Training on Oral Hygiene | ||
|---|---|---|
| Total | ||
| 213 Subjects | ||
| Who provides training on oral hygiene | ||
| Parents | 128 | 60.1% |
| Dentist or dental hygienist | 18 | 8.5% |
| Parents and dentist or dental hygienist | 49 | 23.0% |
| Parents, dentist or dental hygienist, and internet | 1 | 0.5% |
| No training, internet | 1 | 0.5% |
| No training | 13 | 6.1% |
| Attendance at meetings on oral hygiene | ||
| Yes | 26 | 12.2% |
| No | 187 | 87.8% |
| Interest in obtaining more information about oral hygiene | ||
| Yes | 175 | 82.2% |
| No | 38 | 17.8% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sbricoli, L.; Bernardi, L.; Ezeddine, F.; Bacci, C.; Di Fiore, A. Oral Hygiene in Adolescence: A Questionnaire-Based Study. Int. J. Environ. Res. Public Health 2022, 19, 7381. https://doi.org/10.3390/ijerph19127381
Sbricoli L, Bernardi L, Ezeddine F, Bacci C, Di Fiore A. Oral Hygiene in Adolescence: A Questionnaire-Based Study. International Journal of Environmental Research and Public Health. 2022; 19(12):7381. https://doi.org/10.3390/ijerph19127381
Chicago/Turabian StyleSbricoli, Luca, Lia Bernardi, Fatima Ezeddine, Christian Bacci, and Adolfo Di Fiore. 2022. "Oral Hygiene in Adolescence: A Questionnaire-Based Study" International Journal of Environmental Research and Public Health 19, no. 12: 7381. https://doi.org/10.3390/ijerph19127381
APA StyleSbricoli, L., Bernardi, L., Ezeddine, F., Bacci, C., & Di Fiore, A. (2022). Oral Hygiene in Adolescence: A Questionnaire-Based Study. International Journal of Environmental Research and Public Health, 19(12), 7381. https://doi.org/10.3390/ijerph19127381