
SARS-CoV-2 Transmission in the Military during the Early Phase of the Pandemic—A Systematic Analysis


Abstract
:1. Introduction
2. Materials and Methods
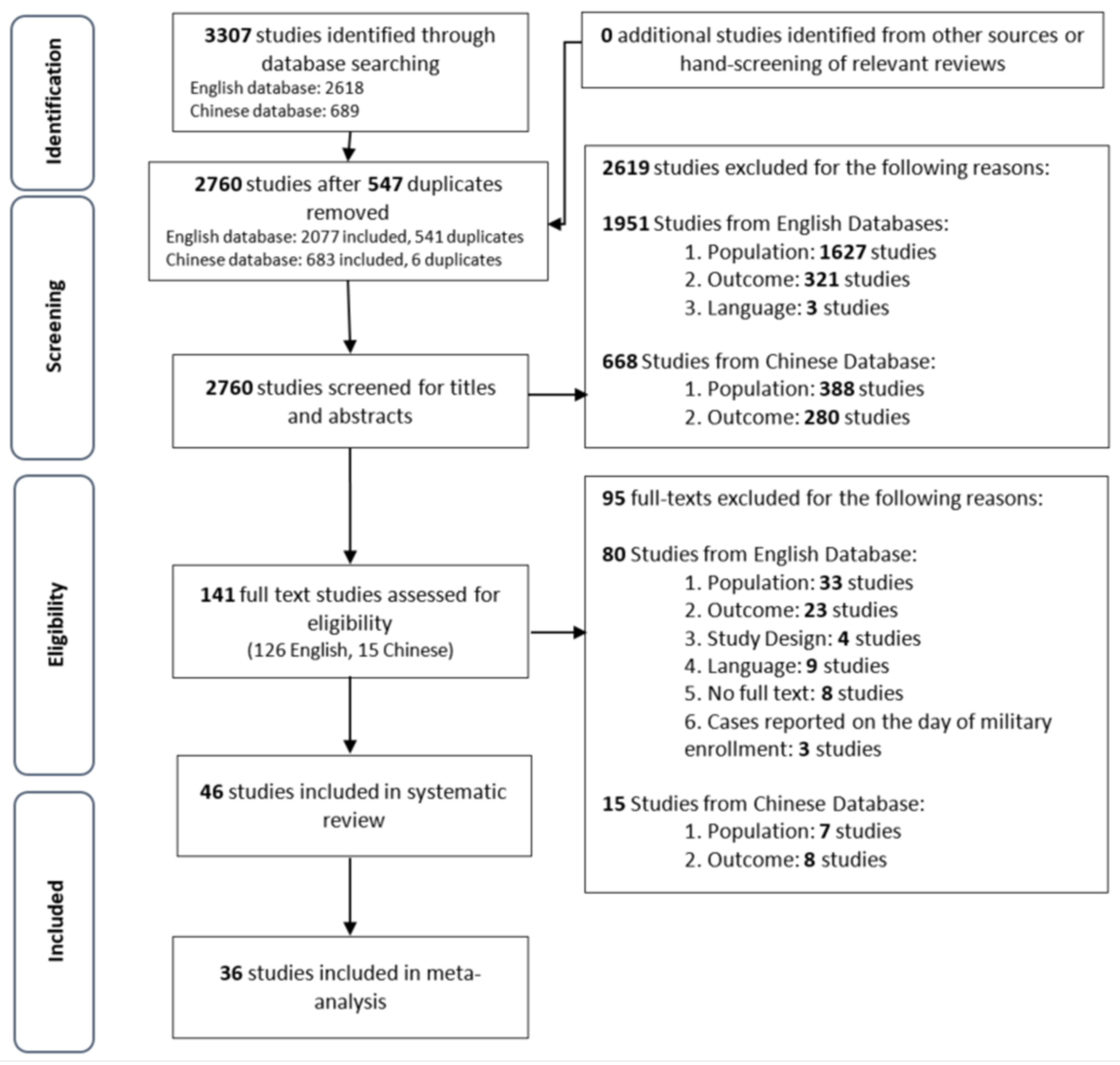
2.1. Search Strategy and Screening
- (1)
- Population: Official government-linked armed forces consisting of active serving personnel in the Army, Navy, Air Force, and other relevant units;
- (2)
- Outcome: Confirmed COVID-19 cases or SARS-CoV-2 infections in the military;
- (3)
- Intervention: All settings that involve military personnel—local and overseas deployment on military vehicles, hospitals, communities, or within military schools or training centers;
- (4)
- Study Design: All reliable sources regardless of article type;
- (5)
- Comparator: Not applicable.
2.2. Data Extraction
2.3. Data Analysis
3. Results
3.1. Published Literature
3.1.1. Study Characteristics

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study α | Publication | Study Type | Country | Study Period & | Population @ | Cases Only | Male (%) ^ | Age %,^ | Setting |
|---|---|---|---|---|---|---|---|---|---|
| Pirnay, J.P. (2020) [51] | Research Article | Retrospective cohort | Belgium | May 2020 | Belgian soldiers of “Mobile Education and Training Team” that trained special intervention company of Nigerian soldiers, undergoing arrival testing | N | 70 (100%) | Arrival testing upon return from deployment | |
| Escalera-Antezana, J.P. (2020) [33] | Research Letter | Letter | Bolivia | Unknown; 2 months | Military personnel of Bolivia; surveillance testing | N | |||
| Pasqualotto, A.C. (2021) [50] | Research Article | Cross-sectional | Brazil | 23–25 July 2020 | Military police in ten cities of Rio Grande do Sul—Porto Alegre, Caxias do Sul, Canoas, Pelotas, Santa Maria, Passo Fundo, Uruguaiana, Santa Cruz do Sul, Ijui, and Lajeado—who had no previous confirmed COVID-19 | N | 1292 (81.2%) | 34 (8) e | |
| Halladay, J. (2020) [35] | Fast Facts | Information sheet | Canada | April–7 July 2020 | Canadian Armed Forces deployed to long-term care facilities | N | Deployment to long-term care facilities | ||
| Elhakim, M. (2020) * [31] | Research Article | Pandemic response | Djibouti | Foreign military contingent deployed to Djibouti | Y | 1 (100%) | Arrival testing | ||
| Paleiron, N. (2021) [49] | Research Article | Cross-sectional | France | April 2020 | Charles de Gaulle sailors under outbreak investigation | N | 1466 (87%) | 28 (23–35) | Aircraft carrier |
| Chassery, L. (2021) [17] | Research Article | Retrospective outbreak analysis | France | April 2020 | French Navy sailors on Charles de Gaulle | Y | Aircraft carrier | ||
| Joshi, R.K. (2020) [37] | Research Letter | Prospective cohort | India | 30 May–12 July 2020 | Indian security forces personnel placed in 14-day quarantine after return from leave | N | Quarantine facility | ||
| Sasongko, S. (2021) # [52] | Research Article | Cross-sectional | Indonesia | 15 August–15 November 2020 | Inpatients of military/police occupation at Dustira Army Hospital with suspected COVID-19. Only those who had an RT-PCR swab and complete patient data included | N | Dustira Army Hospital | ||
| Nitecki, M. (2021) [47] | Research Article | Retrospective cohort | Israel | 26 March–2 August 2020 | Israel soldiers deemed eligible for COVID-19 testing by the ICC, including those voluntarily calling to report symptoms or a suspected exposure or those actively addressed following an epidemiological investigation. | N | 14398 (59.1%) | 20.5 (19.6–22.4) | |
| Segal, D. (2020) [22] | Research Article | Pandemic response | Israel | 26 February–19 April 2020 | Israel Defense Force Northern Command | N | 81.34% | 21.29 (4.06) c | |
| Talmy, T. (2021) [58] | Letter to the Editor | Case series | Israel | 20 March–5 May 2020 | Israel Defense Force (IDF) soldiers with positive SARS-CoV-2 test admitted to rehabilitation center by IDF Medical Corps | Y | 84 (70.6%) | 21 (19–25) | Rehabilitation center |
| Segal, D. (2021) [21] | Research Article | Pandemic response; vaccination | Israel | 1 March 2020–18 February 2021 | Individuals who served in 70 military units that have been allocated to three vaccination stations (for vaccination) | N | 13290 (71.1%) | 22.77 (1.35) f | |
| Tsur, A. (2021) [24] | Research Article | Screening policy/Pandemic response | Israel | 1 April–14 May 2020 | Israel Defense Forces soldiers from 13 units | N | 769 (78%) | 18–52 d | |
| Di Nunno, D. (2020) [30] | Research Article | Prospective case series | Italy | 16 March–4 May 2020 | Italian servicemen infected by SARS-CoV-2 during overseas deployment/military operations hospitalized in non-intensive wards | Y | 75 (92.6%) | 45.1 (10.4) | Celio Military Hospital |
| Borud, E.K. (2021) [28] | Research Article | Prospective cohort | Norway | 6 weeks from 19–27 April 2020 | Norwegian conscripts who just enrolled into military training and followed for 6 weeks | N | Army Base | ||
| Velasco, J.M. (2020) [60] | Research Article | Prospective cohort | Philippines | 14 April–15 August 2020 | Philippines military personnel under investigation for COVID-19, patients seeking clinical care and showing signs of COVID-19-like illness, or asymptomatic patients as part of contact tracing procedures. | N | V Luna Medical Center (tertiary care, teaching hospital under the Armed Forces of the Philippines Health Service Command), other military hospitals in Metro Manila | ||
| Oh, H.S. (2020) $ [48] | Commentary | Pandemic response | South Korea | January–End June 2020 | Confirmed cases in military population of South Korea | N | 54 (93.1%) | 27 g | |
| Wijesekara, N. (2021) [61] | Letter to the Editor | Modelling | Sri Lanka | 22 April 2020 | Navy sailor attached to Sri Lanka Naval Base at Welisara | Y | |||
| Baettig, S. J. (2020) [26] | Research Article | Case series | Switzerland | 12–27 March 2020 | Swiss Armed Forces; symptomatic recruit presenting at military medical center of Monte Ceneri and subsequent outbreak monitoring | N | Recruit school in Monte Ceneri | ||
| Bielecki, M. (2021) [27] | Research Article | Prospective cohort/Cross-sectional | Switzerland | 25 March–3 May 2020 | Swiss Armed Forces; symptomatic soldiers presenting at military medical center and asymptomatic soldiers who were sampled cross-sectionally | N | 526 (90%) | 20.6 (18–54) a | Army base in Airolo |
| Crameri, G.A.G. (2020) [18] | Rapid Communication | Retrospective cohort | Switzerland | Swiss Armed Forces; recruits of two heavily affected companies with available information on SARS-CoV-2 status | N | 174 (87%) | 20.7 (19.9 to 21.8) | Army base in Airolo | |
| Handrick, S. (2020) [36] | Short Report | Case series | Tunisia | 21 March 2020 | Tunisian soldier; arrival testing at Tunis-Carthage Airport | Y | 1 (100%) | 31 | Arrival testing upon return from deployment |
| Stachow, E. (2021) [56] | Research Letter | Retrospective cohort | United Kingdom | Symptomatic military personnel presenting to Royal Navy medical team | N | ||||
| Taylor, H. (2021) [59] | Research Article | Prospective outbreak investigation | United Kingdom | 5 weeks from 30 March 2021 | All adult Army personnel working in the Army barracks | N | Army barracks | ||
| Clifton, G.T. (2021) [29] | CDC MMWR | Cross-sectional | United States | 28–30 April 2020 | United States Army active duty soldiers deployed to field hospital to provide care to COVID-19 patients | N | 201 (59.8%) | 32 (25.3–40.0) | Deployment to Javits New York Medical Station |
| Elliott, B.P. (2021) [32] | Research Article | Retrospective cohort study | United States | 1 June–13 November 2020 | Active duty servicemen with laboratory-confirmed severe or life-threatening COVID-19 in a military treatment facility, confirmed positive by SARS-CoV-2 reverse transcription polymerase chain reaction (RT-PCR) | Y | Wright-Patterson Medical Center | ||
| Kasper, M.R. (2020) [38] | Research Article | Case series | United States | 23 March–18 May 2020 | USS Theodore Roosevelt sailors under emergency public health outbreak investigation | N | 3733 (78.1%) | 27.2 (18–59) b | Aircraft carrier |
| Kim, S.Y. (2021) $ [39] | Research Article | Pandemic response | United States | January–December 2020 | United States Forces Korea service members and affiliates | Y | United States Forces Korea Bases | ||
| Kline, J.D. (2020) [40] | Research Article | Case report | United States | 26 March 2020 | United States National Guard mobilized for national guard annual training, presented to emergency department | Y | 1 (100%) | 36 | Winn Army Community Hospital, Fort Stewart, Georgia |
| Kwon, P.O. (2020) [41] | News Article-Case Series | Case report | United States | 9 October 2020 | United States Army Officer under quarantine as close contact of case | Y | 1 (100%) | 34 | Quarantine Facility |
| Lalani, T. (2021) [42] | Research Article | Cross-sectional | United States | 8–16 May 2020 | United States Navy personnel and other military health care workers deployed on hospital ship | N | 217 (50.2%) | 18–29 (209/432, 48.4%) 30–39 (120/432, 27.8%) 40+ (103/432, 23.8%) | Deployment on USNS COMFORT |
| Letizia, A.G. (2020) [44] | Research Article | Cohort | United States | 2 weeks from 12 May–15 July 2020 | United States Marine Corps recruits under 14-day supervised quarantine before being allowed to enter Parris Island, part of CHARM study | N | Quarantine Facility (hotel/closed college campus) on Marine Corps Recruit Depot, Parris Island | ||
| Marcus, J.E. (2020) [45] | CDC MMWR | Cohort | United States | 1 March–18 April 2020 | United States Air Force trainees under quarantine before basic military training | N | Arrival Quarantine at Air Force Base Joint Base San Antonio-Lackland (JBSA) | ||
| Marcus, J.E. (2021) [46] | Research Article | Cohort | United States | 11 May–24 August 2020 | United States Air Force trainees under quarantine before basic military training | N | Arrival Quarantine at Air Force Base Joint Base San Antonio-Lackland (JBSA) | ||
| Servies, T. (2020) [53] | News Article | United States | 12 March–17 April 2020 | COVID-19 cases in United States active component military personnel in Europe, monitored by U.S. Army Public Health Command Europe (PHCE) on Army Disease Reporting System internet (ADRSi) for Army facilities | Y | 66 (83.5%) | 20–56 d | ||
| Smith, L. (2020) [55] | Research Article | Case Report | United States | 25 March 2020 | United States military personnel, active duty male who reported sick | Y | 1 (100%) | 21 | Military sick call clinic |
| Stanila, V. (2020) [57] | News Article | United States | 11 March–30 September 2020 | United States active duty service members air evacuated in CENTCOM and EUCOM for COVID-19 | Y | 204 (90.7%) | <20 (2/225, 0.9%) 20–24 (37/225, 16.4%) 25–29 (55/225, 24.4%) 30–39 (95/225, 42.2%) 40+ (36/225, 16.0%) | Air Evacuation from CENTCOM and EUCOM countries | |
| Ghoddusi, F. (2021) [34] | Research Article | Case report | United States | November 2020 | United States Army reservist on active duty orders presenting to outpatient clinic in Kuwait | Y | 1 (100%) | 28 | Outpatient in a role 1 facility (in deployed environment) |
| Letizia, A.G. (2021) [43] | Research Article | Prospective cohort | United States | 11 May–2 November 2020 | United States Marine Corps recruits followed up for 6 weeks during training at Marine Corps Recruit Depot-Parris Island (MCRDPI), part of CHARM study | N | 2622 (92.0%) | 19.1 (1.9) | Marine Corps Recruit Depot Parris Island (MCRDPI) |
| Sikorski, C.S. (2021) [54] | Research Article | Case report and pandemic response | United States | 26 February–27 April 2020 | US military population in Italy diagnosed at an Italian military hospital | N | Military hospital in Italy | ||
| Alvarado, G.R. (2020) [16] | Research Letter | Case series | United States | 31 March–15 April 2020 | USS Theodore Roosevelt sailors who disembarked at Naval Base Guam | N | Aircraft carrier | ||
| Kebisek, J. (2020) [19] | News Article | Special report | United States | 11 February–6 April 2020 | Confirmed cases among United States Army active component service members reported to the DRSi with symptom onset dates from 17 February 2020 through 2 April 2020 from any military treatment facility (MTF) | Y | 175 (79.9%) | <25 (34/219, 15.5%) 25–34 (76/219, 34.7%) 35–44 (67/219, 30.6%) 45+ (42/219, 19.2%) | Military treatment facilities |
| Payne, D.C. (2020) [20] | CDC MMWR | Cross-sectional | United States | 20–24 April 2020 | USS Theodore Roosevelt sailors under outbreak investigation, convenience sample of 382 service members serving aboard the aircraft carrier | N | 289 (75.7%) | 30 (24–35) | Aircraft carrier |
| Stidham, R.A. (2020) [23] | News Article | United States | 1 January–30 September 2020 | United States active duty service members, recruits, reserve/guard, cadets; confirmed or probable cases in Disease Reporting System Internet (DRSi) | Y | Active duty (23,987/39,703, 60.4%) Recruits (5491/39,703, 13.8%) Reserve/Guard (1880/39,703, 4.7%) Cadets (326/39,703, 0.8%) | Active duty/Recruits/Reserve or Guard/Cadets 15–19 (2517/39,703, 6.3%)/(4004/39,703, 10.1%)/(332/39,703, 0.8%)/(221/39,703, 0.6%) 20–24 (11,033/39,703, 27.8%)/(2008/39,703, 5.1%)/(537/39,703, 1.4%)/(205/39,703, 0.5%) 25–29 (6944/39,703, 17.5%)/(571/39,703, 1.4%)/(432/39,703, 1.1%)/(2/39,703, 0.005%) 30–34 (3952/39,703, 10.0%)/(176/39,703, 0.4%)/(377/39,703, 0.9%)/0 35–39 (2777/39,703, 7.0%)/(41/39,703, 0.1%)/(275/39,703, 0.7%)/0 40–44 (1403/39,703, 3.5%)/(7/39,703, 0.02%)/(193/39,703, 0.5%)/0 45–49 (760/39,703, 1.9%)/0/(152/39,703, 0.4%)/0 50–54 (363/39,703, 0.9%)/0/(136/39,703, 0.3%)/0 55–59 (147/39,703, 0.4%)/0/(55/39,703, 0.1%)/0 60–64 (54/39,703, 0.1%)/0/(8/39,703, 0.02%)/0 65+ (20/39,703, 0.05%)/0/(1/39,703, 0.003%)/0 | ||
| Vick, D.J. (2021) [25] | Research Letter | Letter | United States | Through 2 November 2020 | COVID-19 cases in United States military members reported by Department of Defense | Y |
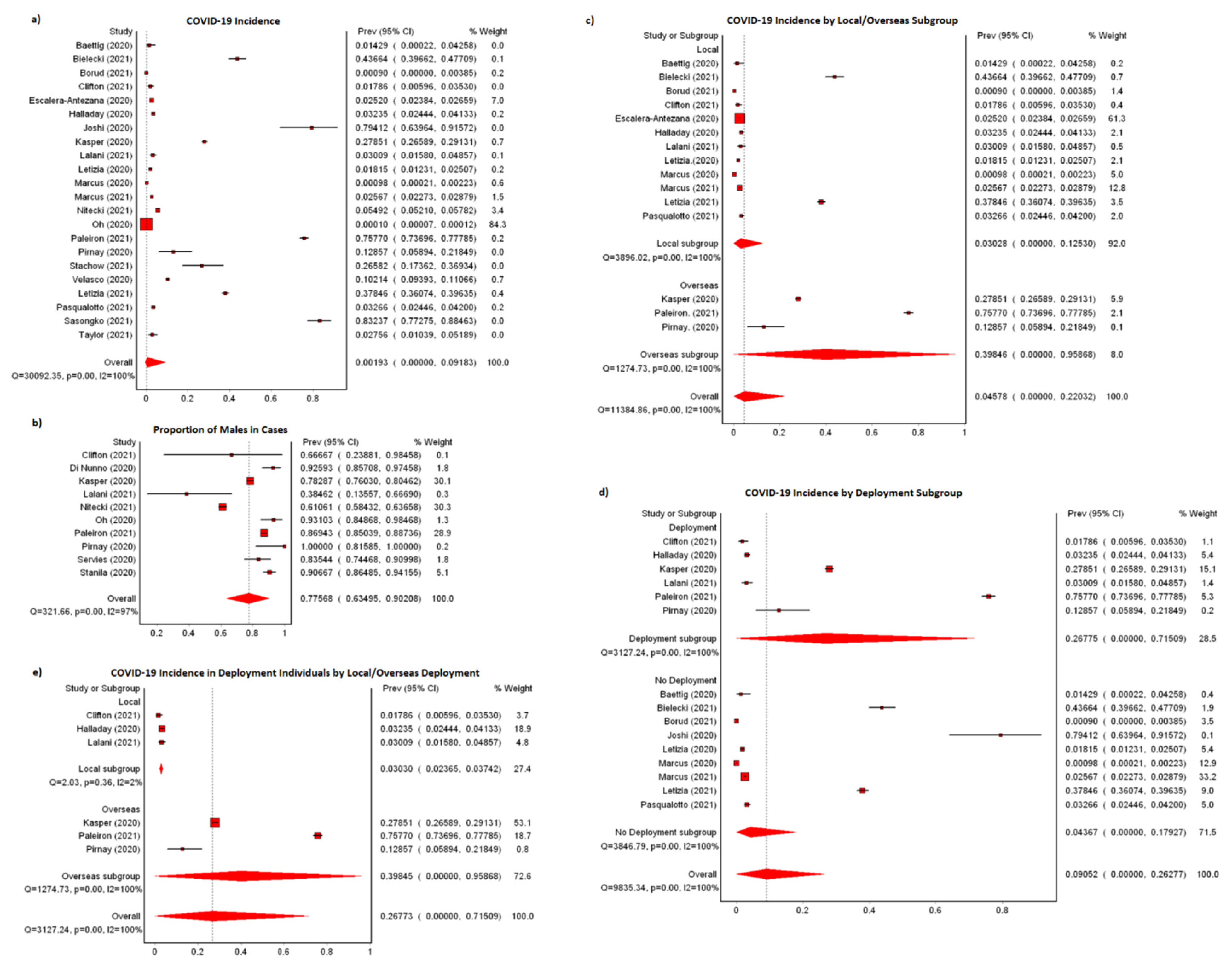
3.1.2. COVID-19 Incidence and Demographic of Cases
| Study | Outcomes (Not Included in Original Study’s Analysis) | Outcomes (Included in Original Study’s Analysis) | Clinical Characteristics | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No. of Cases | Total Personnel | Infected (%) | No. of Cases | Total Personnel # | Infected (%) | Testing Coverage % | Testing Mode | RT-PCR | Serology | Symptomatic (%) | Asymptomatic (%) | Hospitalization | Mortality | |
| Pirnay, J.P. (2020) [51] | 9 | 70 | 12.86% | 70 | RT-PCR, Serology, and Sequencing | 4/9 | 9/9 | 5 (55.6%) | 4 (44.4%) | 0 | 0 | |||
| Escalera-Antezana, J.P. (2020) [33] | 1261 | 50,040 | 2.52% | 24 | ||||||||||
| Pasqualotto, A.C. (2021) [50] | 52 h | 1592 | 3.27% | 1592 | RT-PCR, Serology | 4/50 | 52/1592 | |||||||
| Halladay, J. (2020) [35] | 1834 | 55 | 1700 | 3.24% | 0 | |||||||||
| Elhakim, M. (2020) [31] | 1 | |||||||||||||
| Paleiron, N. (2021) [49] | 1279 | 1688 | 75.77% | 1688 | RT-PCR | 1038/1688 | 1107 (86.6%) | 172 (13.4%) | 107 | 0 | ||||
| Chassery, L. (2021) [17] | 1148 | ≥50 | 2 | 0 | ||||||||||
| Joshi, R.K. (2020) [37] | 27 | 34 | 79.41% | 34 | RT-PCR | 27/34 | 0 | 27 (100%) | ||||||
| Sasongko, S. (2021) [52] | 144 | 173 | 83.24% | 173 | RT-PCR | 144/173 | 144 (100%) | 0 | 144 | |||||
| Nitecki, M. (2021) [47] | 1477 | 31,005 | 4.76% | 1338 | 24,362 | 5.49% | 24,362 | RT-PCR | 1338/24,362 | 1338 (100%) | 0 | |||
| Segal, D. (2020) [22] | 6 | rRT-PCR | 6 | |||||||||||
| Talmy, T. (2021) [58] | 219 | 119 | RT-PCR | 119 | 119 (100%) | 0 | 0 | |||||||
| Segal, D. (2021) [21] | 726 | 18,719 | 3.88% | RT-PCR | ||||||||||
| Tsur, A. (2021) [24] | 237 | 3j | 986 | 0.30% | RT-PCR, Serology | 3 (100%) | 0 | |||||||
| Di Nunno, D. (2020) [30] | 81 | 81 (100%) | 0 | 81 | ||||||||||
| Borud, E.K. (2021) [28] | 1 | 1114 b | 0.09% | 1114 | RT-PCR and Serology | 0/1114 | 1/1114 | 0 | 1 (100%) | |||||
| Velasco, J.M. (2020) [60] | 515 | 5042 | 10.21% | 5046 | rRT-PCR | 515/5046 | ||||||||
| Oh, H.S. (2020) $ [48] | 58 | 599,000 | 0.01% | 58 (100%) | 0 | 0 | ||||||||
| Wijesekara, N. (2021) [61] | 28 | 1 | ||||||||||||
| Baettig, S.J. (2020) [26] | 3 | 2 | 140 a | 1.43% | 55 | RT-PCR and Serology | 2/7 | 2/55 | 2 (100%) | 0 | 0 | 0 | ||
| Bielecki, M. (2021) [27] | 255 | 584 | 43.66% | RT-PCR and Serology | 107 (42.0%) | 148 (58.0%) | 1 | 0 | ||||||
| Crameri, G.A.G. (2020) [18] | 145 | 199 | 72.86% | 199 | RT-qPCR, Serology | 68 (46.9%) | 77 (53.1%) | |||||||
| Handrick, S. (2020) [36] | 1 | RT-qPCR, Sequencing | 1 | 0 | 1 (100%) | |||||||||
| Stachow, E. (2021) [56] | 21 | 79 | 26.58% | 79 | RT-PCR | 21/79 | 21 (100%) | 0 | ||||||
| Taylor, H. (2021) [59] | 7 i | 254 | 2.76% | 254 | RT-PCR, Serology, Sequencing | 7 (100%) | 0 | |||||||
| Clifton, G.T. (2021) [29] | 8 | 591 | 1.35% | 6 | 336 | 1.79% | 336 | RT-PCR and Serology | 2/336 | 5/336 | 4 (66.7%) | 2 (33.3%) | ||
| Elliott, B.P. (2021) [32] | 1 c | RT-PCR | 1 | 1 (100%) | 0 | 1 | ||||||||
| Kasper, M.R. (2020) [38] | 1331 | 4779 | 27.85% | 4779 | rRT-PCR | 1271/4779 | 759 (57.0%) | 572 (43.0%) | 23 | 1 | ||||
| Kim, S.Y. (2021) $ [39] | 479 | |||||||||||||
| Kline, J.D. (2020) [40] | 1 | RT-PCR | 1 | 1 (100%) | 0 | 1 | 0 | |||||||
| Kwon, P.O. (2020) [41] | 1 | RT-PCR | 1 | 1 (100%) | 0 | 0 | 0 | |||||||
| Lalani, T. (2021) [42] | 18 | >1200 | 1.50% | 13 | 432 | 3.01% | 432 | RT-PCR and Serology | 8/432 | 12/432 | 5 (38.5%) | 8 (61.5%) | ||
| Letizia, A. G.(2020) [44] | 57 | 3362 | 1.70% | 31d | 1708d | 1.81% | RT-PCR and Sequencing | |||||||
| Marcus, J.E. (2020) [45] | 4 | 4073 | 0.10% | 85 | RT-PCR | 4/85 | 4 (100%) | 0 | 0 | 0 | ||||
| Marcus, J.E. (2021) [46] | 273 | 10617 | 2.57% | 269 e | 10,479e | 2.57% | 10479 | RT-PCR | 269/10479 | 0 | ||||
| Servies, T. (2020) [53] | 84 | 79 | RT-PCR | 79 | 68 (100%) | 0 | 3 | 0 | ||||||
| Smith, L. (2020) [55] | 1 | RT-PCR | 1 | 1 (100%) | 0 | 0 | 0 | |||||||
| Stanila, V. (2020) [57] | 72,671 as of 10 December 2020 * | 225 | 45 (80.4%) | 11 (19.6%) | ||||||||||
| Ghoddusi, F. (2021) [34] | 1 | RT-PCR | 1 | 1 (100%) | 0 | 1 | 0 | |||||||
| Letizia, A.G. (2021) [43] | 1079 g | 2851 g | 37.85% | 2319 | RT-PCR, Serology | 1079/2319 | 347 (32.2%) | 732 (67.8%) | 0 | 0 | ||||
| Sikorski, C.S. (2021) [54] | 6 | RT-PCR | 6 | |||||||||||
| Alvarado, G.R. (2020) [16] | 736 | 4085 | 18.02% | 4085 | RT-PCR | 736/4085 | 590 (80.2%) | 146 (19.8%) | 6 | 1 | ||||
| Kebisek, J. (2020) [19] | 328 | 219 | 487,100 | 0.04% | RT-PCR | 219 (100%) | 0 | 12 | ||||||
| Payne, D.C. (2020) [20] | 235 | 238 | 382 | 62.30% | 382 | RT-PCR, Serology | 98/267 | 228/382 | 194 (81.5%) | 44 (18.5%) | 2 | |||
| Stidham, R.A. (2020) [23] | 39,703 f | 586 | 8 | |||||||||||
| Vick, D.J. (2021) [25] | 58,081 | |||||||||||||
3.1.3. Deployment and Possible Exposures
| Study | Local/Overseas | Deployment | Country of Deployment | Duration of Deployment | Recreational Activity | Close Contact (Secondary Transmission) | Healthcare | Other Exposure |
|---|---|---|---|---|---|---|---|---|
| Pirnay, J.P. (2020) [51] | Overseas | Y | Niger | 12 December 2019/1 February 2020–13/19 May 2020 | Provision of military education and training overseas (9/9, 100%) ^ | |||
| Escalera-Antezana, J.P. (2020) [33] | Local | Capital department, La Paz, highest concentration of forces, highest proportion of infected personnel (53.8%) | ||||||
| Pasqualotto, A C. (2021) [50] | Local | N | Close contact with COVID-19 cases (438/1592, 27.5%) @ | |||||
| Halladay, J. (2020) [35] | Local | Y | 3 months | Worked closely with LTC facility staff to carry out day-to-day operations and support infection control and prevention | ||||
| Elhakim, M. (2020) [31] | Overseas | Y | Djibouti | 1 day | ||||
| Paleiron, N. (2021) [49] | Overseas | Y | 22 January–13 April 2020 | |||||
| Chassery, L. (2021) [17] | Overseas | Y | Brest (13–16 March 2020) | 21 January–8 April 2020; supposedly until 23 April 2020, disease started on 5 April 2020 | Stopover in Brest for technical needs and change of crew | |||
| Joshi, R.K. (2020) [37] | N | Return from leave (27/27, 100%) & | Secondary transmission from asymptomatic cases in cohort (≥7/27) | |||||
| Segal, D. (2020) [22] | Local | N | ||||||
| Di Nunno, D. (2020) [30] | Overseas | Y | ||||||
| Borud, E.K. (2021) [28] | Local | N | ||||||
| Oh, H.S. (2020) [48] | Close contact with military member (28/58, 48.3%); Close contact with local community (27/58, 46.6%) | Healthcare associated (2/58, 3.4%) | Unknown (1/58, 1.7%) | |||||
| Wijesekara, N. (2021) [61] | On leave (1/1, 100%) | |||||||
| Baettig, S.J. (2020) [26] | Local | N | Vacation trip (1/2, 50%) | Second case might be secondary transmission (1/2, 50%) | ||||
| Bielecki, M. (2021) [27] | Local | N | ||||||
| Crameri, G.A.G. (2020) [18] | Local | N | ||||||
| Handrick, S. (2020) [36] | Overseas | Y | Morocco | |||||
| Clifton, G.T. (2021) [29] | Local | Y | 24 March–30 April 2020 | Travel within 2 weeks before arrival (0/6, 0%) | Direct care for COVID-19 patients (2/6, 33.3%) Break in PPE (1/6, 16.7%) Aerosol generating procedure (0/6, 0%) | Median direct patient care hours: 264 (228–300) | ||
| Kasper, M.R. (2020) [38] | Overseas | Y | 13 days | 1. Crew working in tighter spaces (e.g., reactor (1.73 (1.29–2.36)), engineering (1.85 (1.29–2.67)), supply (2.41 (1.78–3.26)), and weapons (2.70 (1.92–3.8)) departments) appeared more likely to have confirmed or suspected COVID-19 than those working in a combination of open-air and confined conditions (e.g., air and deck crew). 2. Members of the medical department, who wore personal protective equipment when evaluating crew members, had a somewhat lower attack rate (16.7% 8 cases among 48 personnel) than the overall crew despite being at highest risk as a result of exposure to patients with COVID-19 in a small space. | ||||
| Kim, S.Y. (2021) [39] | Overseas | Y | South Korea | |||||
| Kline, J.D. (2020) [40] | Local | N | Resident of an area that reported a cluster of COVID-19 cases, mobilization for national guard training, and recently traveled to Fort Stewart, Bartow County, Georgia | |||||
| Kwon, P.O. (2020) [41] | Overseas | Y | Close contact of confirmed case (1/1, 100%) | |||||
| Lalani, T. (2021) [42] | Local | Y | 28 March–30 April 2020 | Direct interaction with COVID-19 patients/individuals 2 weeks before deployment: No (1/13, 7.7%); Do not know (3/13, 23.1%); Yes (9/13, 69.2%). Anyone in workspace/berthing/social circle placed in isolation/quarantine: No (1/13, 7.7%); Do not know (3/13, 23.1%); Yes (9/13, 69.2%). | Primary workspace during deployment being ICU/Ward (12/13, 92.3%) Direct care of COVID-19 patients during deployment (12/13, 92.3%) Spent 2/3 or more of time in direct patient care during deployment (11/13, 84.6%) Aerosol generating procedure (5/13, 38.4%) | Berthing during deployment: Enlisted berthing (0/13, 0%); Non-government organization berthing (1/13, 7.7%); Officer berthing (1/13, 7.7%); Private hotel room (11/13, 84.6%). Place where meals were consumed: Galley (2/13, 15.4%); Hotel room (8/13, 61.5%); Other (1/13, 7.7%); Workspace (2/13, 15.4%). | ||
| Letizia, A.G. (2020) [44] | Local | N | Had an infected roommate (24/77, 31.2%) $ | |||||
| Marcus, J.E. (2020) [45] | Local | N | Contact of patient A during training (3/4, 75%) | First case speculated to have been infected during transit because he arrived from a state not reporting community spread of COVID-19 (1/4, 25%) | ||||
| Marcus, J.E. (2021) [46] | Local | N | ||||||
| Servies, T. (2020) [53] | Overseas | Y | Europe | |||||
| Smith, L. (2020) [55] | Local | N | Recent recreational activities (clubs, beach) (1/1, 100%) | Work in busy environment (1/1, 100%) | ||||
| Stanila, V. (2020) [57] | Overseas | Y | Kuwait, Saudi Arabia, Afghanistan, Iraq, Poland, Jordan, Kosovo % | |||||
| Ghoddusi, F. (2021) [34] | Overseas | Y | Kuwait | |||||
| Letizia, A.G. (2021) [43] | Local | N | ||||||
| Sikorski, C.S. (2021) [54] | Overseas | Y | Italy | |||||
| Alvarado, G.R. (2020) [16] | Overseas | Y | ||||||
| Payne, D.C. (2020) [20] | Overseas | Y | Western Pacific | Mid-January–End March | Reported contact with known COVID-19 case (64.2%) compared with those who did not (41.7%) (OR = 2.5; 95% CI = 1.1–5.8) Sharing the same sleeping berth with a crewmember who had positive test results (65.6%) compared with those who did not (36.4%) (OR = 3.3; 95% CI = 1.8–6.1) | Reported prevention behaviors: Increased hand washing (218/238, 91.6%) OR: 0.90 (0.42–1.94); Hand sanitizer use (219/238, 92.0%) OR: 0.59 (0.24–1.44); Avoiding common areas (78/238, 32.8%) OR: 0.56 (0.37–0.86) §; Face covering use (158/238, 66.4%) OR: 0.30 (0.17–0.52) §; Increased workspace cleaning (195/238, 81.9%) OR: 1.30 (0.78–2.16); Increased berthing cleaning (156/238, 65.5%) OR: 0.95 (0.61–1.47); Increased distance from others (105/238, 44.1%) OR: 0.52 (0.34–0.79)§ |
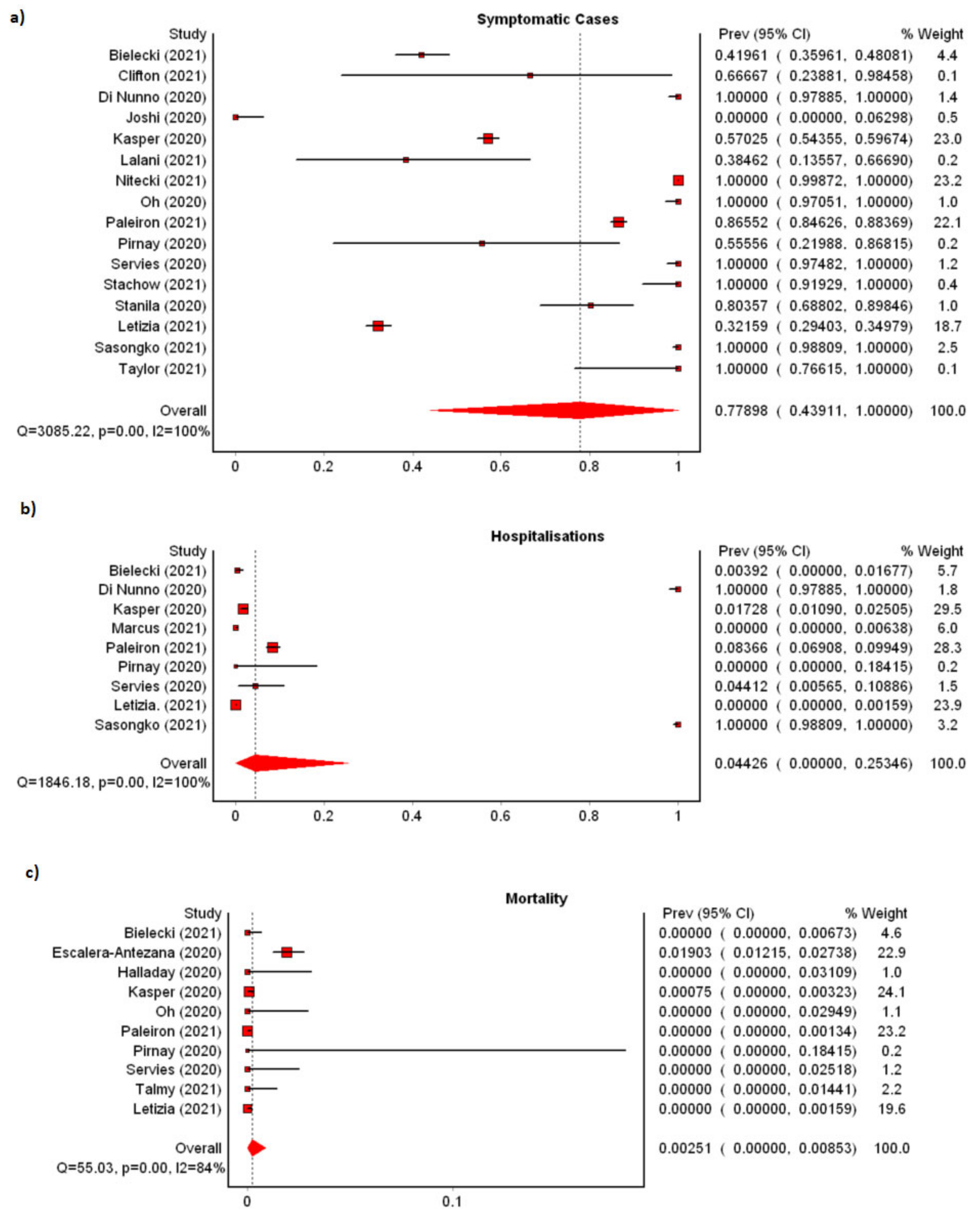
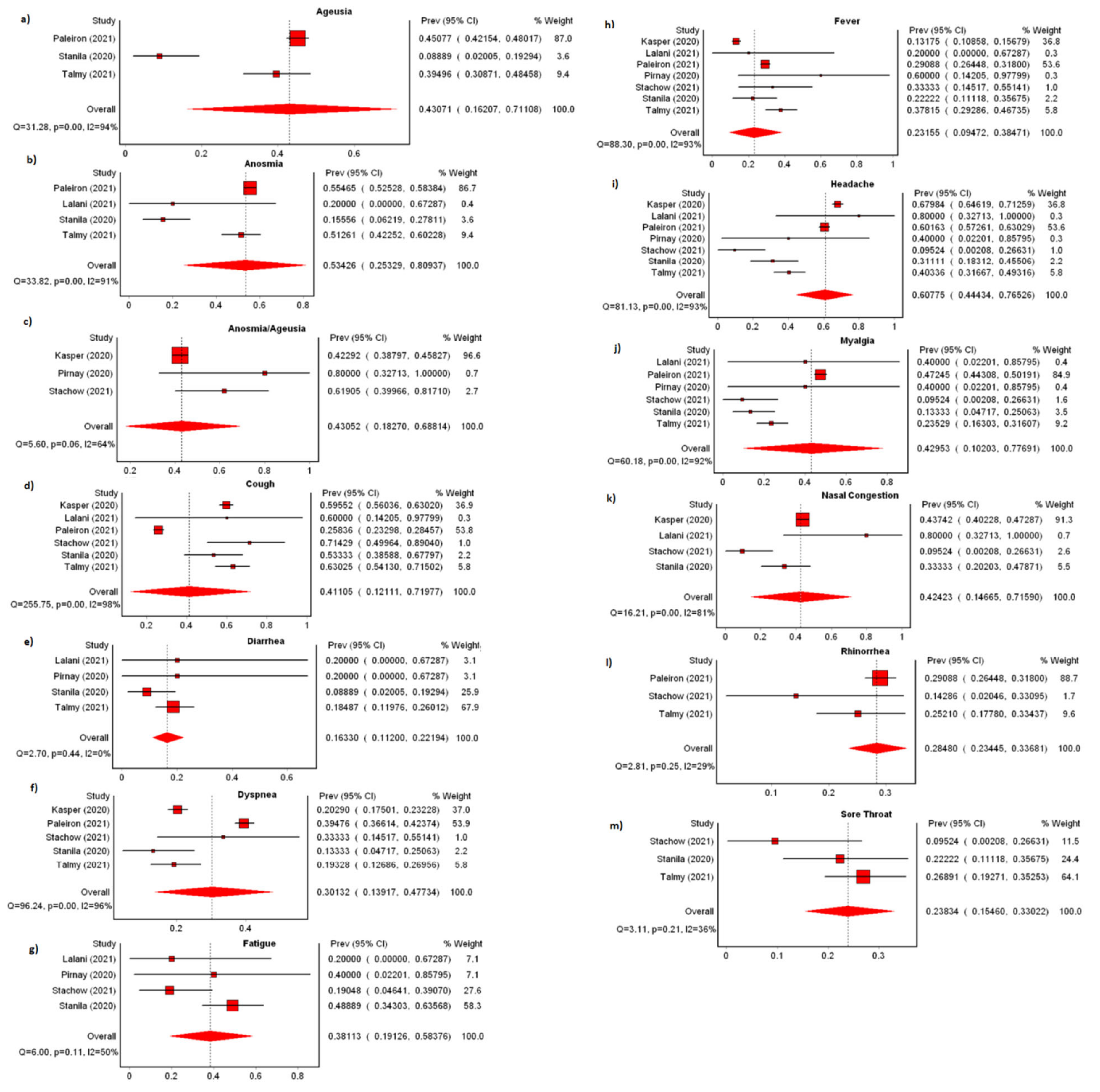
3.1.4. Clinical Characteristics
4. Discussion
4.1. Preventive Measures
4.2. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19. 11 March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 25 June 2021).
- Molina Hazan, V.; Balicer, R.D.; Groto, I.; Zarka, S.; Ankol, O.E.; Bar-Zeev, Y.; Levine, H.; Ash, N. The military role in a flu pandemic. Harefuah 2010, 149, 9–13, 64. [Google Scholar] [PubMed]
- Graham, E. The Armed Forces and COVID-19. Available online: https://www.iiss.org/blogs/analysis/2020/04/easia-armed-forces-and-covid-19 (accessed on 25 June 2021).
- Gibson-Fall, F. Military responses to COVID-19, emerging trends in global civil-military engagements. Rev. Int. Stud. 2021, 47, 155–170. [Google Scholar] [CrossRef]
- Brewster, M. Military Mission to COVID-Hit Long Term Care Homes Cost Taxpayers about $53 Million. Available online: https://www.cbc.ca/news/politics/covid-pandemic-coronavirus-canadian-armed-forces-1.5804063 (accessed on 25 June 2021).
- Declerq, K. Military Report Details ‘Horrifying’ Conditions at Two Toronto Long-Term Care Homes. Available online: https://www.cp24.com/news/military-report-details-horrifying-conditions-at-two-toronto-long-term-care-homes-1.5422069?cache=hyebvgxafjbyb (accessed on 25 June 2021).
- U.N. Command. Active-Duty Support to COVID-19 Response. Available online: https://www.northcom.mil/COVID19/ (accessed on 4 May 2021).
- Ng, V. How Singapore’s Military Is Fighting COVID-19. Available online: https://thediplomat.com/2020/03/how-singapores-military-is-fighting-covid-19/ (accessed on 25 June 2021).
- Yang, S.; Liu, X.Z. Xi Approves Chinese Military Medical Teams to Leave Hubei as Mission Completed. Available online: https://www.globaltimes.cn/content/1185830.shtml (accessed on 25 June 2021).
- Sajid, I. Pakistan Brings in Army to Battle COVID-19. Available online: https://www.aa.com.tr/en/asia-pacific/pakistan-brings-in-army-to-battle-covid-19/2218569 (accessed on 25 June 2021).
- Ho, Z.J.M.; Hwang, Y.F.J.; Lee, J.M.V. Emerging and re-emerging infectious diseases: Challenges and opportunities for militaries. Mil. Med. Res. 2014, 1, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [Green Version]
- MetXL Version 5.3. Available online: https://www.epigear.com/index_files/metaxl.html (accessed on 25 June 2021).
- Doi, S.A.; Barendregt, J.J.; Khan, S.; Thalib, L.; Williams, G. Advances in the meta-analysis of heterogeneous clinical trials I: The inverse variance heterogeneity model. Contemp. Clin. Trials 2015, 45, 130–138. [Google Scholar] [CrossRef] [Green Version]
- Abu-Zidan, F.M.; Abbas, A.K.; Hefny, A.F. Clinical “case series”: A concept analysis. Afr. Health Sci. 2012, 12, 557–562. [Google Scholar] [CrossRef] [Green Version]
- Alvarado, G.R.; Pierson, B.C.; Teemer, E.S.; Gama, H.J.; Cole, R.D.; Jang, S.S. Symptom Characterization and Outcomes of Sailors in Isolation After a COVID-19 Outbreak on a US Aircraft Carrier. JAMA Netw. Open 2020, 3, e2020981. [Google Scholar] [CrossRef]
- Chassery, L.; Texier, G.; De Santi, V.P.; Chaudet, H.; Bonnardel, N.; Pellegrin, L. A COVID-19 outbreak on board ship: Analysis of the sociotechnical system of epidemiological management in the French Navy. Saf. Sci. 2021, 140, 105296. [Google Scholar] [CrossRef]
- Crameri, G.A.G.; Bielecki, M.; Züst, R.; Buehrer, T.W.; Stanga, Z.; Deuel, J.W. Reduced maximal aerobic capacity after COVID-19 in young adult recruits, Switzerland, May 2020. Eurosurveillance 2020, 25, 2001542. [Google Scholar] [CrossRef]
- Kebisek, J.; Forrest, L.J.; Maule, A.L.; Steelman, R.A.; Ambrose, J.F. Special report: Prevalence of selected underlying health conditions among active component Army service members with coronavirus disease 2019, 11 February–6 April 2020. MSMR 2020, 27, 50–54. [Google Scholar]
- Payne, D.C.; Smith-Jeffcoat, S.E.; Nowak, G.; Chukwuma, U.; Geibe, J.R.; Hawkins, R.J.; Johnson, J.A.; Thornburg, N.J.; Schiffer, J.; Weiner, Z.; et al. SARS-CoV-2 Infections and Serologic Responses from a Sample of U.S. Navy Service Members—USS Theodore Roosevelt, April 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 714–721. [Google Scholar] [CrossRef]
- Segal, D.; Arzi, Y.I.; Bez, M.; Cohen, M.; Rotschield, J.; Fink, N.; Karp, E. Promoting Compliance to COVID-19 Vaccination in Military Units. Mil. Med. 2021, usab183. [Google Scholar] [CrossRef]
- Segal, D.; Rotschield, J.; Ankory, R.; Kutikov, S.; Moaddi, B.; Verhovsky, G.; Benov, A.; Twig, G.; Glassberg, E.; Fink, N.; et al. Measures to Limit COVID-19 Outbreak Effects among Military Personnel: Preliminary Data. Mil. Med. 2020, 185, e1624–e1631. [Google Scholar] [CrossRef]
- Stidham, R.A.; Stahlman, S.; Salzar, T.L. Cases of Coronavirus Disease 2019 and Comorbidities among Military Health System Beneficiaries, 1 January 2020 through 30 September 2020. MSMR 2020, 27, 2–8. [Google Scholar]
- Tsur, A.; Furer, A.; Avramovich, E.; Karp, E.; Twig, G.; Bader, T.; Almakias, M.; Fink, N. SARS-CoV-2 Epidemic in the Israeli Defense Force-Lessons Learned from Our rt-PCR Screening Policy. Mil. Med. 2021, usab215. [Google Scholar] [CrossRef]
- Vick, D.J. Evaluation of glucose-6-phosphate dehydrogenase (G6PD) status in US military and VA patients with COVID-19 infection. BMJ Mil. Health 2021, 167, 144. [Google Scholar] [CrossRef]
- Baettig, S.J.; Parini, A.; Cardona, I.; Morand, G.B. Case series of coronavirus (SARS-CoV-2) in a military recruit school: Clinical, sanitary and logistical implications. BMJ Mil. Health 2020, 167, 251–254. [Google Scholar] [CrossRef] [Green Version]
- Bielecki, M.; Züst, R.; Siegrist, D.; Meyerhofer, D.; Crameri, G.A.G.; Stanga, Z.; Stettbacher, A.; Buehrer, T.W.; Deuel, J.W. Social Distancing Alters the Clinical Course of COVID-19 in Young Adults: A Comparative Cohort Study. Clin. Infect. Dis. 2021, 72, 598–603. [Google Scholar] [CrossRef]
- Borud, E.K.; Nakstad, E.R.; Håberg, S.E.; Lind, A.; Fadum, E.A.; Taxt, A.M.; Steens, A.; Gjein, G.E.; Sunde, M.W.; Iversen, P.; et al. Severe acute respiratory syndrome coronavirus 2 prevalence in 1170 asymptomatic Norwegian conscripts. Health Sci. Rep. 2021, 4, e233. [Google Scholar] [CrossRef]
- Clifton, G.T.; Pati, R.; Krammer, F.; Laing, E.D.; Broder, C.C.; Mendu, D.R.; Simons, M.P.; Chen, H.W.; Sugiharto, V.A.; Kang, A.D.; et al. SARS-CoV-2 Infection Risk among Active Duty Military Members Deployed to a Field Hospital—New York City, April 2020. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 308–311. [Google Scholar] [CrossRef]
- Di Nunno, D.; Laghi, A.; Troiani, G.; Marseglia, B.; Anelli, L.; Farina, E.; Tarricone, F.; Mammana, G.; Catalano, C.; Bonito, A.; et al. Cutaneous manifestations in an Italian military COVID hub. G. Ital. Dermatol. Venereol. 2020, 155, 632–635. [Google Scholar] [CrossRef] [PubMed]
- Elhakim, M.; Tourab, S.B.; Zouiten, A. COVID-19 pandemic in Djibouti: Epidemiology and the response strategy followed to contain the virus during the first two months, 17 March to 16 May 2020. PLoS ONE 2020, 15, e0243698. [Google Scholar] [CrossRef] [PubMed]
- Elliott, B.P.; Buchek, G.M.; Koroscil, M.T. Characteristics, Treatment, and Outcomes of Patients With Severe or Life-threatening COVID-19 at a Military Treatment Facility—A Descriptive Cohort Study. Mil. Med. 2021, usab055. [Google Scholar] [CrossRef] [PubMed]
- Escalera-Antezana, J.P.; Mariaca-Cerball, C.A.; Alvarado-Arnez, L.E.; Balderrama-Saavedra, M.A.; Bonilla-Aldana, D.K.; Rodriguez-Morales, A.J. Incidence of SARS-CoV-2/COVID-19 in military personnel of Bolivia. BMJ Mil. Health 2020, 167, 215–216. [Google Scholar] [CrossRef] [PubMed]
- Ghoddusi, F.; Garcia, D.; Harroun, T. Post-COVID Multisystem Inflammatory Syndrome in the Deployed Environment. Mil. Med. 2021, usab159. [Google Scholar] [CrossRef]
- Halladay, J.; Bélanger, S.A.H. Fast facts on COVID-19 and the Canadian Armed Forces. J. Mil. Veteran Fam. Health 2020, 6, 7–8. [Google Scholar] [CrossRef]
- Handrick, S.; Bestehorn-Willmann, M.; Eckstein, S.; Walter, M.C.; Antwerpen, M.H.; Naija, H.; Stoecker, K.; Wölfel, R.; Ben Moussa, M. Whole genome sequencing and phylogenetic classification of Tunisian SARS-CoV-2 strains from patients of the Military Hospital in Tunis. Virus Genes 2020, 56, 767–771. [Google Scholar] [CrossRef]
- Joshi, R.K.; Ray, R.K.; Adhya, S.; Chauhan, V.P.S.; Pani, S. Spread of COVID-19 by asymptomatic cases: Evidence from military quarantine facilities. BMJ Mil. Health 2021, 167, 217–218. [Google Scholar] [CrossRef]
- Kasper, M.R.; Geibe, J.R.; Sears, C.L.; Riegodedios, A.J.; Luse, T.; Von Thun, A.M.; McGinnis, M.B.; Olson, N.; Houskamp, D.; Fenequito, R.; et al. An Outbreak of Covid-19 on an Aircraft Carrier. N. Engl. J. Med. 2020, 383, 2417–2426. [Google Scholar] [CrossRef]
- Kim, S.Y.; Lee, K.; Tussey, J.B.; Dougherty, E.J.; Williams, S.C.; Abrams, R.B.; Murray, C.K. Responding to COVID-19 among U.S. Military Units in South Korea: The U.S. Forces Korea’s Operation Kill the Virus. Mil. Med. 2021, 187, e138–e146. [Google Scholar] [CrossRef]
- Kline, J.D.; Donovan, A.E. Sentinel Case of COVID-19 at Fort Stewart, GA in a National Guard Soldier Participating in Annual Training: A Case Report. Mil. Med. 2020, 185, e2158–e2161. [Google Scholar] [CrossRef]
- Kwon, P.O.; Fisher, N.A.; Mancuso, J.D. SARS-CoV-2 and influenza coinfection in a deployed military setting—Two case reports. Med. Surveill. Mon. Rep. 2020, 27, 18–23. [Google Scholar]
- Lalani, T.; Lee, T.K.; Laing, E.D.; Ritter, A.; Cooper, E.; Lee, M.; Baker, M.; Baldino, T.; McAdoo, T.; Phogat, S.; et al. SARS-CoV-2 Infections and Serologic Responses among Military Personnel Deployed on the USNS COMFORT to New York City During the COVID-19 Pandemic. Open Forum Infect. Dis. 2021, 8, ofaa654. [Google Scholar] [CrossRef]
- Letizia, A.G.; Ge, Y.; Vangeti, S.; Goforth, C.; Weir, D.L.; Kuzmina, N.A.; Balinsky, C.A.; Chen, H.W.; Ewing, D.; Soares-Schanoski, A.; et al. SARS-CoV-2 seropositivity and subsequent infection risk in healthy young adults: A prospective cohort study. Lancet Respir. Med. 2021, 9, 712–720. [Google Scholar] [CrossRef]
- Letizia, A.G.; Ramos, I.; Obla, A.; Goforth, C.; Weir, D.L.; Ge, Y.; Bamman, M.M.; Dutta, J.; Ellis, E.; Estrella, L.; et al. SARS-CoV-2 Transmission among Marine Recruits during Quarantine. N. Engl. J. Med. 2020, 383, 2407–2416. [Google Scholar] [CrossRef]
- Marcus, J.E.; Frankel, D.N.; Pawlak, M.T.; Casey, T.M.; Blackwell, R.S.; Tran, F.V.; Dolan, M.J.; Yun, H.C. COVID-19 Monitoring and Response among U.S. Air Force Basic Military Trainees—Texas, March-April 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 685–688. [Google Scholar] [CrossRef]
- Marcus, J.E.; Frankel, D.N.; Pawlak, M.T.; Casey, T.M.; Cybulski, R.J., Jr.; Enriquez, E.; Okulicz, J.F.; Yun, H.C. Risk Factors Associated With COVID-19 Transmission among US Air Force Trainees in a Congregant Setting. JAMA Netw. Open 2021, 4, e210202. [Google Scholar] [CrossRef]
- Nitecki, M.; Taran, B.; Ketko, I.; Geva, G.; Yosef, R.; Toledo, I.; Twig, G.; Avramovitch, E.; Gordon, B.; Derazne, E.; et al. Self-reported symptoms in healthy young adults to predict potential coronavirus disease 2019. Clin. Microbiol. Infect. 2021, 27, 618–623. [Google Scholar] [CrossRef]
- Oh, H.S.; Woong, S. Strict Containment Strategy and Rigid Social Distancing Successfully Contained COVID-19 in the Military in South Korea. Mil. Med. 2020, 185, 476–479. [Google Scholar] [CrossRef]
- Paleiron, N.; Mayet, A.; Marbac, V.; Perisse, A.; Barazzutti, H.; Brocq, F.X.; Janvier, F.; Bertrand, D.; Bylicki, O. Impact of Tobacco Smoking on the risk of COVID-19. A large scale retrospective cohort study. Nicotine Tob. Res. 2021, 23, 1398–1404. [Google Scholar] [CrossRef]
- Pasqualotto, A.C.; de Castro Pereira, P.; Dalla Lana, D.F.; Schwarzbold, A.V.; Ribeiro, M.S.; Riche, C.V.W.; Castro, C.P.P.; Korsack, P.L.; Ferreira, P.E.B.; de Domingues, G.C.; et al. COVID-19 seroprevalence in military police force, Southern Brazil. PLoS ONE 2021, 16, e0249672. [Google Scholar] [CrossRef]
- Pirnay, J.P.; Selhorst, P.; Cochez, C.; Petrillo, M.; Claes, V.; Van der Beken, Y.; Verbeken, G.; Degueldre, J.; T’Sas, F.; Van den Eede, G.; et al. Study of a SARS-CoV-2 Outbreak in a Belgian Military Education and Training Center in Maradi, Niger. Viruses 2020, 12, 949. [Google Scholar] [CrossRef]
- Sasongko, S.; Nurrokhmawati, Y.; Rahayu, D.F. Characteristics of inpatients suspected COVID-19 based on swab results rt-pcr in dustira army hospital (Period on August, 15th–November, 15th 2020). Ann. Rom. Soc. Cell Biol. 2021, 25, 7710–7720. [Google Scholar]
- Servies, T. Characteristics of U.S. Army Beneficiary Cases of COVID-19 in Europe, 12 March 2020–17 April 2020. MSMR 2020, 27, 9–13. [Google Scholar]
- Sikorski, C.S.; Scheel, M.D.; Harris, S.M.; Nefczyk, J.A. COVID-19 Contact Tracing in an Overseas U.S. Military Population. Mil. Med. 2021, usab166. [Google Scholar] [CrossRef]
- Smith, L.; Hodges, C.; Pratt, M.; Porter, I.M. Case Report: COVID-19 Patient With Chief Complaint of Anosmia and Ageusia; a Unique Perspective on Atypical Symptomatology and Management in the Military. Mil. Med. 2020, 185, e2176–e2179. [Google Scholar] [CrossRef]
- Stachow, E.; Warden, S.; Cockcroft, K.; Schofield, S. Symptomatology of COVID-19, rhinovirus and undifferentiated viral infections in a static military population. BMJ Mil. Health 2021, 167, 290–291. [Google Scholar] [CrossRef]
- Stanila, V.; Wells, N.; Ziadeh, C.; Stahlman, S. Air Evacuation of Service Members for COVID-19 in U.S. Central Command and U.S. European Command from 11 March 2020 through 30 September 2020. MSMR 2020, 27, 14–17. [Google Scholar]
- Talmy, T.; Tsur, A.; Shabtay, O. Duration of SARS-CoV-2 detection in Israel Defense Forces soldiers with mild COVID-19. J. Med. Virol. 2021, 93, 608–610. [Google Scholar] [CrossRef]
- Taylor, H.; Wall, W.; Ross, D.; Janarthanan, R.; Wang, L.; Aiano, F.; Ellis, J.; Gopal, R.; Andrews, N.; Patel, M.; et al. Cross sectional investigation of a COVID-19 outbreak at a London Army barracks: Neutralising antibodies and virus isolation. Lancet Reg. Health Eur. 2021, 2, 100015. [Google Scholar] [CrossRef] [PubMed]
- Velasco, J.M.; Navarro, F.C.; Diones, P.C.; Villa, V.; Valderama, M.T.; Tabinas, H.; Chua, D.; Rosa, R.D.; Turao-Agoncillo, M.M.; Timbol, J.C.; et al. SARS-CoV-2 among Military and Civilian Patients, Metro Manila, Philippines. Mil. Med. 2021, 186, e760–e766. [Google Scholar] [CrossRef] [PubMed]
- Wijesekara, N.; Herath, N.; Kodituwakku, K.; Herath, H.D.B.; Ginige, S.; Ruwanpathirana, T.; Kariyawasam, M.; Samaraweera, S.; Herath, A.; Jayawardena, S.; et al. Predictive modelling for COVID-19 outbreak control: Lessons from the navy cluster in Sri Lanka. Mil. Med. Res. 2021, 8, 31. [Google Scholar] [CrossRef] [PubMed]
- Ng, O.T.; Marimuthu, K.; Koh, V.; Pang, J.; Linn, K.Z.; Sun, J.; De Wang, L.; Chia, W.N.; Tiu, C.; Chan, M.; et al. SARS-CoV-2 seroprevalence and transmission risk factors among high-risk close contacts: A retrospective cohort study. Lancet Infect. Dis. 2021, 21, 333–343. [Google Scholar] [CrossRef]
- Weissman, D.N.; de Perio, M.A.; Radonovich, L.J., Jr. COVID-19 and Risks Posed to Personnel During Endotracheal Intubation. JAMA 2020, 323, 2027–2028. [Google Scholar] [CrossRef]
- Tran, K.; Cimon, K.; Severn, M.; Pessoa-Silva, C.L.; Conly, J. Aerosol generating procedures and risk of transmission of acute respiratory infections to healthcare workers: A systematic review. PLoS ONE 2012, 7, e35797. [Google Scholar] [CrossRef] [Green Version]
- El-Boghdadly, K.; Wong, D.J.N.; Owen, R.; Neuman, M.D.; Pocock, S.; Carlisle, J.B.; Johnstone, C.; Andruszkiewicz, P.; Baker, P.A.; Biccard, B.M.; et al. Risks to healthcare workers following tracheal intubation of patients with COVID-19: A prospective international multicentre cohort study. Anaesthesia 2020, 75, 1437–1447. [Google Scholar] [CrossRef]
- Xie, J. China Claims Zero Infections in Its Militar. Available online: https://www.voanews.com/science-health/coronavirus-outbreak/china-claims-zero-infections-its-military (accessed on 25 June 2021).
- Magnezi, R.; Dankner, R.; Shani, M.; Levy, Y.; Ashkenazi, I.; Reuveni, H. Comparison of Health Care Services for Career Soldiers throughout the World. Mil. Med. 2005, 170, 995–998. [Google Scholar] [CrossRef] [Green Version]
- Morris, M.J.; Zacher, L.L.; Jackson, D.A. Investigating the Respiratory Health of Deployed Military Personnel. Mil. Med. 2011, 176, 1157–1161. [Google Scholar] [CrossRef] [Green Version]
- Murray, C.K.; Horvath, L.L.; Ericsson, C.D.; Hatz, C. An Approach to Prevention of Infectious Diseases during Military Deployments. Clin. Infect. Dis. 2007, 44, 424–430. [Google Scholar] [CrossRef] [Green Version]
- Murray, C.K.; Yun, H.C.; Markelz, A.E.; Okulicz, J.F.; Vento, T.J.; Burgess, T.H.; Cardile, A.P.; Miller, R.S. Operation United Assistance: Infectious disease threats to deployed military personnel. Mil. Med. 2015, 180, 626–651. [Google Scholar] [CrossRef] [Green Version]
- Zemke, J.N.; Sanchez, J.L.; Pang, J.; Gray, G.C. The Double-Edged Sword of Military Response to Societal Disruptions: A Systematic Review of the Evidence for Military Personnel as Pathogen Transmitters. J. Infect. Dis. 2019, 220, 1873–1884. [Google Scholar] [CrossRef]
- Johns, M.C.; Burke, R.L.; Vest, K.G.; Fukuda, M.; Pavlin, J.A.; Shrestha, S.K.; Schnabel, D.C.; Tobias, S.; Tjaden, J.A.; Montgomery, J.M.; et al. A growing global network’s role in outbreak response: AFHSC-GEIS 2008–2009. BMC Public Health 2011, 11, S3. [Google Scholar] [CrossRef] [Green Version]
- Piarroux, R.; Barrais, R.; Faucher, B.; Haus, R.; Piarroux, M.; Gaudart, J.; Magloire, R.; Raoult, D. Understanding the cholera epidemic, Haiti. Emerg. Infect. Dis. 2011, 17, 1161–1168. [Google Scholar] [CrossRef]
- Centre for Infectious Disease Epidemiology & Research. Military Infectious Disease Surveillance. Available online: https://blog.nus.edu.sg/nuscider/ (accessed on 23 July 2021).
- Oran, D.P.; Topol, E.J. Prevalence of Asymptomatic SARS-CoV-2 Infection. Ann. Intern. Med. 2020, 173, 362–367. [Google Scholar] [CrossRef]
- Syangtan, G.; Bista, S.; Dawadi, P.; Rayamajhee, B.; Shrestha, L.B.; Tuladhar, R.; Joshi, D.R. Asymptomatic SARS-CoV-2 Carriers: A Systematic Review and Meta-Analysis. Front. Public Health 2021, 8, 587374. [Google Scholar] [CrossRef]
- Grant, M.C.; Geoghegan, L.; Arbyn, M.; Mohammed, Z.; McGuinness, L.; Clarke, E.L.; Wade, R.G. The prevalence of symptoms in 24,410 adults infected by the novel coronavirus (SARS-CoV-2; COVID-19): A systematic review and meta-analysis of 148 studies from 9 countries. PLoS ONE 2020, 15, e0234765. [Google Scholar] [CrossRef]
- Mansourian, M.; Ghandi, Y.; Habibi, D.; Mehrabi, S. COVID-19 infection in children: A systematic review and meta-analysis of clinical features and laboratory findings. Arch. Pédiatr. 2021, 28, 242–248. [Google Scholar] [CrossRef]
- Caronna, E.; Ballvé, A.; Llauradó, A.; Gallardo, V.J.; Ariton, D.M.; Lallana, S.; López Maza, S.; Olivé Gadea, M.; Quibus, L.; Restrepo, J.L.; et al. Headache: A striking prodromal and persistent symptom, predictive of COVID-19 clinical evolution. Cephalalgia 2020, 40, 1410–1421. [Google Scholar] [CrossRef]
- Sampaio Rocha-Filho, P.A.; Magalhães, J.E. Headache associated with COVID-19: Frequency, characteristics and association with anosmia and ageusia. Cephalalgia 2020, 40, 1443–1451. [Google Scholar] [CrossRef]
- Graham, M.S.; Sudre, C.H.; May, A.; Antonelli, M.; Murray, B.; Varsavsky, T.; Kläser, K.; Canas, L.S.; Molteni, E.; Modat, M.; et al. Changes in symptomatology, reinfection, and transmissibility associated with the SARS-CoV-2 variant B.1.1.7: An ecological study. Lancet Public Health 2021, 6, e335–e345. [Google Scholar] [CrossRef]
- Curran, J.; Dol, J.; Boulos, L.; Somerville, M.; McCulloch, H. Public Health and Health Systems Impacts of SARS-CoV-2 Variants of Concern: A Rapid Scoping Review. medRxiv 2021. [Google Scholar] [CrossRef]
- Danner, C.; Rosa-Aquino, P. What We Know about the Dangerous Delta Variant. Available online: https://nymag.com/intelligencer/article/covid-b-1-617-2-delta-variant-what-we-know.html (accessed on 19 August 2021).
- Lee, V.J.; Tan, C.H.; Yap, J.; Cook, A.R.; Ting, P.-J.; Loh, J.-P.; Gao, Q.; Chen, M.I.; Kang, W.L.; Tan, B.H.; et al. Effectiveness of Pandemic H1N1-2009 Vaccination in Reducing Laboratory Confirmed Influenza Infections among Military Recruits in Tropical Singapore. PLoS ONE 2011, 6, e26572. [Google Scholar] [CrossRef] [PubMed]
- Haas, E.J.; Angulo, F.J.; McLaughlin, J.M.; Anis, E.; Singer, S.R.; Khan, F.; Brooks, N.; Smaja, M.; Mircus, G.; Pan, K.; et al. Impact and effectiveness of mRNA BNT162b2 vaccine against SARS-CoV-2 infections and COVID-19 cases, hospitalisations, and deaths following a nationwide vaccination campaign in Israel: An observational study using national surveillance data. Lancet 2021, 397, 1819–1829. [Google Scholar] [CrossRef]
- Tan, C. Study of 29,000 People Quarantined in S’pore Shows COVID-19 Vaccines Can Prevent Infection and Severe Illness. Available online: https://www.straitstimes.com/singapore/study-of-29000-people-on-quarantine-in-spore-shows-vaccines-can-prevent-infection-and (accessed on 28 July 2021).
- Department of Defense Strategy for COVID-19 Testing and Surveillance. Available online: https://www.militaryonesource.mil/family-relationships/family-life/covid-19-resources/covid-19-testing-and-surveillance/ (accessed on 28 July 2021).
- Mahmud, A.H. SAF Could Use Rapid COVID-19 Tests during Large-Scale Events Like Graduation Parades. Available online: https://www.channelnewsasia.com/news/singapore/saf-covid-19-rapid-tests-large-scale-events-graduation-parade-13383710 (accessed on 28 July 2021).
- MINDEF Singapore. Fact Sheet: The SAF Stands Ready Amidst COVID-19. Available online: https://www.mindef.gov.sg/web/portal/mindef/news-and-events/latest-releases/article-detail/2021/June/30jun21_fs3 (accessed on 28 July 2021).
- Oyewole, A.O.; Barrass, L.; Robertson, E.G.; Woltmann, J.; O’Keefe, H.; Sarpal, H.; Dangova, K.; Richmond, C.; Craig, D. COVID-19 Impact on Diagnostic Innovations: Emerging Trends and Implications. Diagnostics 2021, 11, 182. [Google Scholar] [CrossRef] [PubMed]
- Schneider, C.R.; Dryhurst, S.; Kerr, J.; Freeman, A.L.J.; Recchia, G.; Spiegelhalter, D.; van der Linden, S. COVID-19 risk perception: A longitudinal analysis of its predictors and associations with health protective behaviours in the United Kingdom. J. Risk Res. 2021, 24, 294–313. [Google Scholar] [CrossRef]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gwee, S.X.W.; Chua, P.E.Y.; Pang, J. SARS-CoV-2 Transmission in the Military during the Early Phase of the Pandemic—A Systematic Analysis. Int. J. Environ. Res. Public Health 2022, 19, 7418. https://doi.org/10.3390/ijerph19127418
Gwee SXW, Chua PEY, Pang J. SARS-CoV-2 Transmission in the Military during the Early Phase of the Pandemic—A Systematic Analysis. International Journal of Environmental Research and Public Health. 2022; 19(12):7418. https://doi.org/10.3390/ijerph19127418
Chicago/Turabian StyleGwee, Sylvia Xiao Wei, Pearleen Ee Yong Chua, and Junxiong Pang. 2022. "SARS-CoV-2 Transmission in the Military during the Early Phase of the Pandemic—A Systematic Analysis" International Journal of Environmental Research and Public Health 19, no. 12: 7418. https://doi.org/10.3390/ijerph19127418
APA StyleGwee, S. X. W., Chua, P. E. Y., & Pang, J. (2022). SARS-CoV-2 Transmission in the Military during the Early Phase of the Pandemic—A Systematic Analysis. International Journal of Environmental Research and Public Health, 19(12), 7418. https://doi.org/10.3390/ijerph19127418