
Collaborative Learning: A Qualitative Study Exploring Factors Contributing to a Successful Tobacco Cessation Train-the-Trainer Program as a Community of Practice

 , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
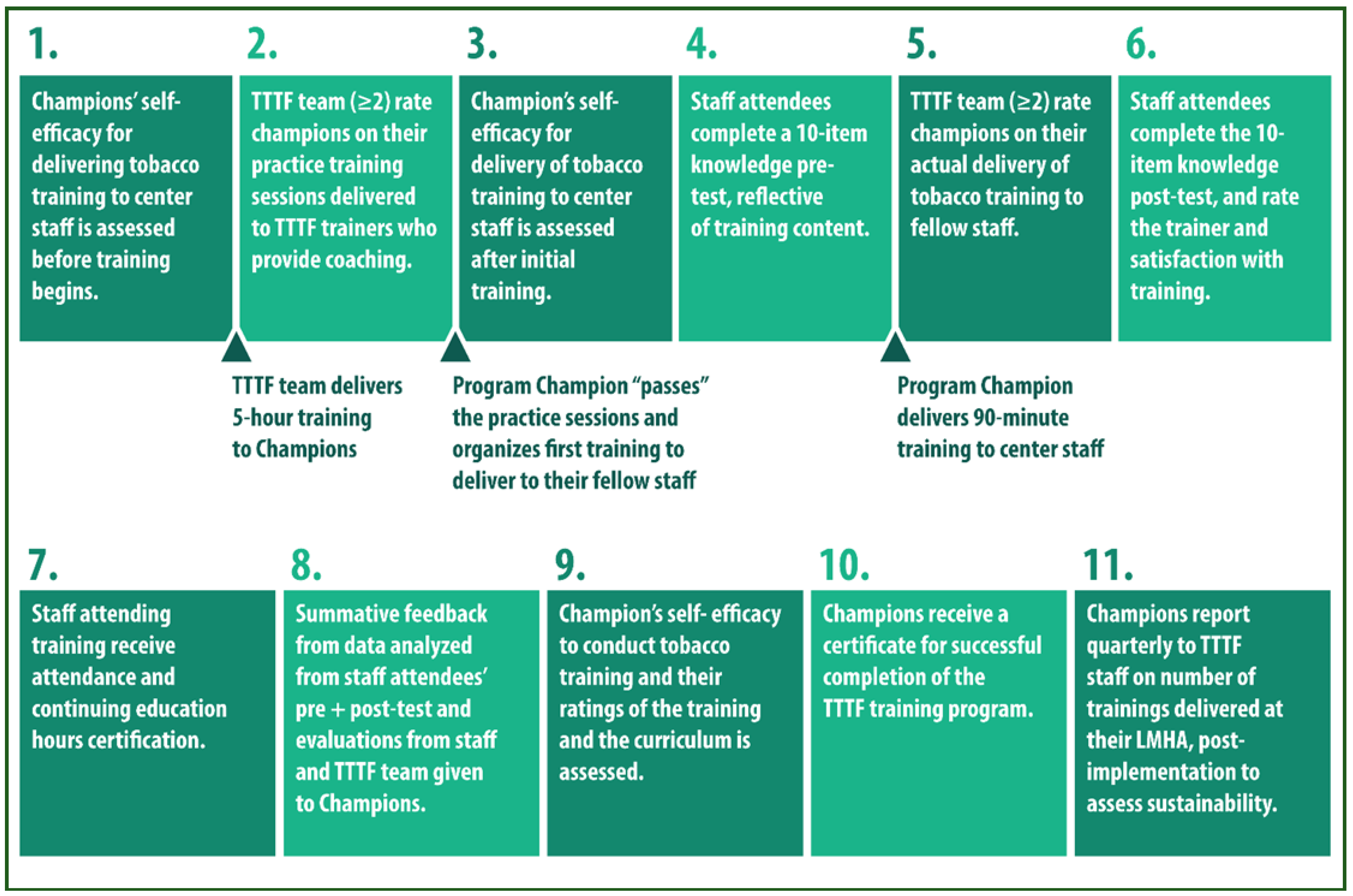
2.1. TTTF Train-the-Trainer
2.2. Ethical Approval
2.3. Study Design and Participants
2.4. Data Collection
2.5. Data Analysis
2.6. Theoretical Framework: Communities of Practice
3. Results
3.1. Collaborative Learning: Value of Peer Support, Feedback, and Practice
3.1.1. Value of Peer Support
I agree with Sheila, she’s pointed out several times that we all learned a lot from each other in sitting in on each other’s trainings as well. So really, we sat through maybe 10 trainings. We all fed off that, and we all gained bits and pieces of everybody else’s techniques as well as their points of interest that they pointed out maybe better than we did. So I think it was a huge benefit for us to sit in each other’s trainings.(Lisa, LMHA1)
3.1.2. Feedback
One of [my coworkers] came up to me and told me about this last [employee training], “My God, I was so impressed by the training”, and that helps me to get better. … It’s always good to get feedback from people. Especially people who work with you because they’re going to be honest.(Veronica, LMHA1)
3.1.3. Practice
It would’ve not been helpful at all if we had not had those practice sessions with each other and with you guys. If we had gone from you giving us the training straight into doing training for our staff, I don’t think it would’ve gone as well… especially where I think I’ve got holes I find myself less confident. So, I was really grateful to have those trainings that we did with each other.(Sheila, LMHA1)
3.2. Building Knowledge, Increased Champion Confidence, Program Ownership, and Innovation
3.2.1. Building Knowledge
You guys are so very knowledgeable, you were an excellent resource, and knew the material front to back. That helped us feel more confident because you guys were so at ease with the material, and I appreciate that…You were like—‘Hey, this is what works, this is what we’ve seen that doesn’t work’…I felt that you were there to support us from the beginning and being really approachable and just normal people, trying to help people learn about tobacco use. So I think that was a big part of our learning. We didn’t feel threatened or intimidated in any way to try to do it perfect. Because I think you guys said from the beginning, we’re all going to have different styles, we’re all going to have different parts of that presentation that we dobetter, and some places that we’re not as good presenting. And like S. [peer] said, I think we fed off of that we were able to see different things through being able to learn from everybody else’s presentation.(Lisa, LMHA1)
3.2.2. Increased Champion Confidence
You all were very patient and the guidance that you gave us was good. In the beginning, I was a little bit confused… but once you all started guiding me… you slowed it down, and I think giving it to us in pieces really worked and helped my self-confidence to be able to do the presentation.(Clara, LMHA2)
3.2.3. Program Ownership: Becoming a Tobacco Treatment Specialist
As I’m going, I think of stories I can say along the way. It reminds me of stuff I’ve experienced in the past with clients that I’m able to add little stories to for these different topics, to help people quit smoking. It was challenging, but then with the support and assistance and the help that you all gave me and the encouragement, I was able to open up, and I was able to make it a little bit of my own, and the more I did it the more excited I would get, and then I got inspired and so I was able to do the presentation with a flow and to make it more of my own.(Clara, LMHA2)
I think it was a very good training because—I was kind of nervous at the beginning because there was a lot of information and learning, but at the end, it was all worth it, I feel confident. … This program was fairly new to me, and if you would’ve asked me in the beginning, I probably would’ve said no, I’m not confident at all to do the training… But now I feel confident. I know that I’m probably going to keep learning, and I am probably going to run into something that I might not know, but that’s a process, that’s what goes with it. I’m just happy I went through it.(Veronica, LMHA2)
3.2.4. Innovation
The other thing that we haven’t really explored, that we want to, is the training together. Like, for example, I do half the class and then L. [peer] finishes it up, or vice-versa. So the audience gets a mixture of different opinions and people.(Sheila, LMHA1)
3.3. Informative Curriculum, Adaptable to Targeted Populations
3.3.1. Informative Curriculum
At first, it was kind of difficult… It was challenging, but with all the support, and all the important information was there—the dangers, what parts of the body it [smoking] affects, and the way it affects it, and it went into a nice flow into how to try to help people to quit smoking, and the different medications that they can use to stop. All this information is very helpful because when I am talking to people about tobacco, I’m able to explain to them better because I know a lot more now with this training… My co-workers said they enjoyed it, and they learned a lot. They said that everything was very informational and very educational for them. They learned stuff that they didn’t know about tobacco.(Clara, LMHA2)
I know that you were providing us with a lot of new information especially given to me when I had previous knowledge. I did learn a lot. That’s what I would say, there’s nothing to improve. I know there’s always going to be more information coming in but your whole presentation, all the training you gave us, those were perfect…I learned a lot of information that can benefit my patients, especially how they can obtain more services… like what I learned from peers besides all the information is mainly the benefits the patients can obtain from us.(Juan, LMHA2)
3.3.2. Curriculum Adaptable to Target Populations
I think everything about that training was good, I liked it. It’s very informative. It’s a lot of information, but it’s good. It focuses on a lot of topics, a lot of different populations…I had some coworkers that work with IDD, most of their patients smoke, and they liked that information so they can also explain it to them. So, there was nothing to be added. Everybody thought it was very educational and informational.(Clara, LMHA2)
I’d really like to look a little bit more at those marginalized cultures, looking at our homeless, LGBTQ+. Keeping us up-to-date on the new information that comes out, we’d love to have that… There’s just not enough of a focus [on special populations], so what we’d need if we were to specialize a 30-, 45-min training for a specific group, we might want to focus on the population that you work with most, and looking at a bit more data on that.(Sarah, LMHA3)
There were gaps [in information] with the IDD, I think we need to keep up with it and see what other information is available, for that and the homeless. But of course, that in general has very limited data. I just did the best I could to add more to [the training].(Veronica, LMHA2)
3.4. Staying Abreast of Changing Tobacco/Nicotine Research and Evidence-Based Practice: Clarification and Additional Resources
3.4.1. Staying Abreast of Changing Tobacco/Nicotine Research: Clarifications
I think when we first did our [TTTF] training, it [vaping] had just started, and a lot of people were thinking it would be a good alternative to cigarettes… I’m really excited to learn more about e-cigarettes. I was surprised this morning when I taught… a lot of them thought that vaping was a NRT [Nicotine Replacement Therapy], and they get that confused, that they think that e-cigarettes are an alternative… A safe alternative to smoking.(Sheila, LMHA1)
3.4.2. Additional Resources
You all had the different types of e-cigarettes, and like the different types of tobacco, and the chew tobacco, there’s all different types of tobacco. We try to keep up to date on all the different changing e-cigarettes because there’s always so many new ones coming out on the market all the time. Yes, because research, it changes all the time.There’s always new information out there. Of course, we’d like new research also about e-cigarettes, and SNUS—since we still don’t know a lot about that. We’re still learning since it’s new.(Clara, LMHA2)
Especially the part that I really enjoyed and learn the most from—even though there’s still a lot for us to find out—is the part about the electronic cigarettes, the e-cigarettes. I think it’s really fascinating. It’s interesting because that’s the most popular method now especially for teens and such. I knew pretty much nothing about the e-cigarettes, and so it was good just to learn the little bit that we, that the community does know now.(Michael, LMHA1)
3.4.3. Staying Abreast of Tobacco Cessation Evidence-Based Practices
I heard this morning [on a webinar] that they felt that ‘cessation’ wasn’t the adequate term any longer, that we needed to use the word ‘treatment’, or ‘smoking recovery’ instead of ‘cessation’, because they felt that was a much stronger word to be using to show that it is that type of addiction that’s going to require treatments for people to stop.(Sheila, LMHA1)
3.5. Facilitated Practice: Responsiveness and Practical Coaching/Assistance by TTTF Team
3.5.1. Responsiveness
And also, I want to say that B. [TTTF trainer] was very responsive to our questions, I sent him a lot of questions and I know that S. [peer] did also. But he was extremely responsive to them, and that put us more at ease too knowing that he was there if we were having a panic moment, or we were confused about something. And so, I really appreciate that.(Lisa, LMHA1)
3.5.2. Practical Coaching/Assistance
It was a good experience, this is very good for people to learn and be able to educate other people about the dangers of tobacco because tobacco has been out there for a long time, and it does so much damage to people… You all did excellent in guiding us, and with the support and the assistance, you encouraged us very well and the support was really good, and you all inspired us very well, like, you want to do something with it.(Clara, LMHA2)
3.5.3. Structure and Model
You guys have done a really great job with this training. I don’t know that there’s much more information that you could give somebody… I feel very confident in my ability to train this course… There was a lot of information to cover, and a lot of times, it seems like people try to fit a training into too short of amount of time, and then expect you to be able to regurgitate that whenever you are training somebody else. That doesn’t always work, so I loved how long our initial training was and then the fact that we had to train a couple more times in order to be certified… And not being the only one from our organization to go through this training, it was very nice for us to be able to do it as a team… In the two employee trainings that I did, I got really great feedback. People really appreciated that information. I had the opportunity to take in all that information and learn it really well… of all the train the trainer trainings that I’ve been through, this one was by far the best.(Jane, LMHA3)
4. Discussion
4.1. Collaborative Learning Builds Knowledge, Champion Confidence, and Professional Identity
4.2. Responding to Diverse Populations and Evolving Tobacco/Nicotine Landscape
4.3. Strengths, Limitations, and Future Research
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- United States Department of Health and Human Services. Smoking Cessation: A Report of the Surgeon General. CDC, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health. 2020. Available online: https://www.hhs.gov/sites/default/files/2020-cessation-sgr-full-report.pdf (accessed on 22 January 2022).
- Allen, A.M.; Muramoto, M.L.; Campbell, J.; Connolly, T.E.; McGuffin, B.A.; Bernstein, A.D. Multimethod Formative Research to Improve the Training and Delivery of Tobacco-cessation Interventions in Behavioral Health Settings. J. Addict. Med. 2019, 13, 470–475. Available online: https://pubmed.ncbi.nlm.nih.gov/30908345/ (accessed on 22 January 2022). [CrossRef] [PubMed]
- Prochaska, J.J.; Das, S.; Wolff, K.C.Y. Smoking, Mental Illness, and Public Health. Annu. Rev. Public Health 2017, 38, 165–185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prochaska, J.J.; Gates, E.F.; Davis, K.C.; Gutierrez, K.; Prutzman, Y.; Rodes, R. The 2016 Tips from Former Smokers Campaign: Associations with Quit Intentions and Quit Attempts Among Smokers with and without Mental Health Conditions. Nicotine Tob. Res. 2019, 21, 576–583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Annamalai, A.; Singh, N.; O’Malley, S.S. Smoking Use and Cessation Among People with Serious Mental Illness. Yale J. Biol. Med. 2015, 88, 271–277. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4553647/ (accessed on 22 January 2022).
- Callaghan, R.C.; Veldhuizen, S.; Jeysingh, T.; Orlan, C.; Graham, C.; Kakouris, G.; Remington, G.; Gately, J. Patterns of Tobacco-Related Mortality among Individuals Diagnosed with Schizophrenia, Bipolar Disorder, or Depression. J. Psych. Res. 2014, 48, 102–110. [Google Scholar] [CrossRef]
- Callaghan, R.C.; Gately, J.M.; Skyes, J.; Taylor, L. The Prominence of Smoking-Related Mortality Among Individuals with Alcohol- or Drug-Use Disorders. Drug Alcohol Rev. 2013, 37, 97–105. [Google Scholar] [CrossRef] [Green Version]
- Williams, J.M.; Steinberg, M.L.; Griffiths, K.G.; Cooperman, N. Smokers with Behavioral Health Comorbidity should be Designated a Tobacco Use Disparity Group. Am. J. Public Health 2013, 103, 1549–1555. [Google Scholar] [CrossRef]
- Gubner, N.R.; Pagano, A.; Tajima, B.; Guydish, J. A comparison of daily versus weekly electronic cigarette users in treatment for substance abuse. Nicotine Tob. Res. 2018, 20, 636–642. [Google Scholar] [CrossRef]
- Marynak, K.; VanFrank, B.; Tetlow, S.; Mahoney, M.; Phillips, E.; Jamal, A.; Schecter, A.; Tipperman, D.; Babb, S. Tobacco Cessation Interventions and Smoke-Free Policies in Mental Health and Substance Abuse Treatment Facilities—United States, 2016. Morb. Mortal. Wkly. Rep. 2018, 67, 519–523. [Google Scholar] [CrossRef]
- Fiore, M.C.; Jaen, C.R.; Baker, T.B.; Bailey, W.C.; Bennett, G.; Benowitz, N.L.; Christiansen, B.A.; Connell, M.; Curry, S.J.; Dorfman, S.F.; et al. A Clinical Practice Guideline for Treating Tobacco Use and Dependence: 2008 Update. A U.S. Public Health Service Report. Am. J. Prev. Med. 2008, 35, 158–176. [Google Scholar] [CrossRef] [Green Version]
- Center for Disease Control and Prevention. Best Practices for Comprehensive Tobacco Control Programs. Atlanta, GA. United States of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion. 2014. Available online: https://www.cdc.gov/tobacco/stateandcommunity/best_practices/pdfs/2014/comprehensive.pdf (accessed on 7 March 2022).
- Siu, A.L.; United States Preventive Services Task Force. Behavioral and Pharmacotherapy Interventions for Tobacco Smoking Cessation in Adults, Including Pregnant Women: US Preventive Services Task Force Recommendation Statement. Ann. Intern. Med. 2015, 163, 622–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kleber, H.D.; Weiss, R.D.; Anton, R.F., Jr.; George, T.P.; Greenfield, S.F.; Kosten, T.R.; O’Brien, C.P.; Rounsaville, B.J.; Strain, E.C.; Ziedonis, D.M.; et al. Practice Guideline for the Treatment of Patients with Substance Use Disorders—Second Edition. Am. J. Psychiatry 2006, 163, 1–81. Available online: https://psychiatryonline.org/pb/assets/raw/sitewide/practice_guidelines/guidelines/substanceuse.pdf (accessed on 22 January 2022).
- Grimshaw, J.M.; Thomas, R.E.; MacLennan, G.; Fraser, C.; Ramsay, C.R.; Vale, L.; Whitty, P.; Eccles, M.P.; Matowe, L.; Shirran, L.; et al. Effectiveness and Efficiency of Guideline Dissemination and Implementation Strategies. Health Technol. Assess. 2004, 8, 1–72. [Google Scholar] [CrossRef] [PubMed]
- Brown, C.H.; Medoff, D.; Dickerson, F.B.; Fang, L.J.; Lucksted, A.; Goldberg, R.W.; Kreyenbuhl, J.; Himelhoch, S.; Dixon, L.B. Factors Influencing Implementation of Smoking Cessation Treatment within Community Mental Health Centers. J. Dual Diagn. 2015, 11, 145–150. [Google Scholar] [CrossRef] [Green Version]
- Graydon, M.M.; Corno, C.M.; Schacht, R.L.; Knoblach, D.J.; Wiprovnick, A.E.; Thrash, S.T.; Petersen, A.A.; DiClemente, C.C. A Statewide Initiative to Train Behavioral Health Providers in Smoking Cessation. Transl. Behav. Med. 2018, 8, 855–866. [Google Scholar] [CrossRef] [Green Version]
- Nitturi, V.; Chen, T.A.; Leal, I.M.; Fernandez, V.C.; Drenner, K.; Kyburz, B.; Williams, T.; Obasi, E.M.; Britton, M.; Howard, M.; et al. Implementation and Outcomes of a Train-the-Trainer Program at Behavioral Health Treatment Centers as a Mechanism to Maintain Organizational Capacity to Address Tobacco Use Disorder. Int. J. Environ. Res. Public Health 2021, 18, 11635. [Google Scholar] [CrossRef]
- Koch, J.R.; Breland, A. Behavioral Healthcare Staff Attitudes and Practices Regarding Consumer Tobacco Cessation Services. J. Ment. Health Adm. 2017, 44, 399–413. [Google Scholar] [CrossRef]
- Siru, R.; Hulse, G.K.; Tait, R.J. Assessing Motivation to Quit Smoking in People with Mental Illness: A Review. Addiction 2009, 104, 719–733. [Google Scholar] [CrossRef]
- Lawn, S.; Campion, J. Achieving Smoke-Free Mental Health Services: Lessons from the Past Decade of Implementation Research. Int. J. Environ. Res. Public Health 2013, 10, 4224–4244. [Google Scholar] [CrossRef] [Green Version]
- Garey, L.; Neighbors, C.; Leal, I.M.; Lam, C.Y.; Wilson, W.T.; Kyburz, B.; Stacy, T.; Correa-Fernandez, V.; Williams, T.; Zvolensky, M.J.; et al. Organizational Moderators of Change in Behavioral Health Center Clinician and Staff Tobacco-Related Knowledge Following Brief Education during a Comprehensive Tobacco-Free Workplace Program Implementation. Patient Educ. Couns. 2019, 102, 1680–1686. [Google Scholar] [CrossRef]
- Sheals, K.; Tombor, I.; McNeill, A.; Shahab, L. A Mixed-Method Systematic Review and Meta-Analysis of Mental Health Professionals’ Attitudes Toward Smoking and Smoking-Cessation Among People with Mental Illnesses. Addiction 2016, 111, 1536–1553. [Google Scholar] [CrossRef] [PubMed]
- Himelhoch, S.; Riddle, J.; Goldman, H.H. Barriers to implementing Evidence-Based Smoking Cessation Practices in Nine Community Mental Health Sites. Psychiatr. Serv. 2014, 65, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Compton, W. The Need to Incorporate Smoking Cessation into Behavioral Health Treatment. Am. J. Addict. 2018, 27, 42–43. [Google Scholar] [CrossRef]
- Cavazos-Rehg, P.A.; Breslau, N.; Hatsukami, D.; Krauss, M.J.; Spitznagel, E.L.; Grucza, R.A.; Salyer, P.; Hartz, S.M.; Bierut, L.J. Smoking Cessation is Associated with Lower Rates of Mood/Anxiety and Alcohol Use Disorders. Psychol. Med. 2014, 44, 2523–2535. [Google Scholar] [CrossRef] [Green Version]
- Taylor, G.; McNeill, A.; Girling, A.; Farley, A.; Lindson-Hawley, N.; Aveyard, P. Change in mental health After Smoking Cessation: Systematic Review and Meta-analysis. BMJ 2014, 348, g1151. [Google Scholar] [CrossRef] [Green Version]
- Prochaska, J.J.; Delucchi, K.; Hall, S.M. A Meta-analysis of Smoking Cessation Interventions with Individuals in Substance Abuse Treatment or Recovery. J. Consult. Clin. Psychol. 2004, 72, 1144–1156. [Google Scholar] [CrossRef] [Green Version]
- McClure, E.A.; Acquavita, S.P.; Dunn, K.E.; Stroller, K.B.; Stitzer, M.L. Characterizing Smoking, Cessation Services, and Quit Interest across Outpatient Substance Abuse Treatment Modalities. J. Subst. Abus. Treat. 2014, 46, 194–201. [Google Scholar] [CrossRef] [Green Version]
- Gulliver, S.B.; Kamholz, B.W.; Helstrom, A.W. Smoking Cessation and Alcohol Abstinence: What Do the Data Tell Us? Alcohol Res. Health 2006, 29, 208–213. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6527036/pdf/208-212.pdf (accessed on 7 March 2022).
- Cookson, C.; Strang, J.; Ratschen, E.; Sutherland, G.; Finch, E.; McNeill, A. Smoking and its Treatment in Addiction Services: Clients’ and Staff Behaviour and Attitudes. BMC Health Serv. Res. 2014, 14, 304. [Google Scholar] [CrossRef] [Green Version]
- Williams, J.M.; Stroup, T.S.; Brunette, M.F.; Raney, L.E. Tobacco Use and Mental Illness: A Wake-up Call for Psychiatrists. Psychiatr. Serv. 2014, 65, 1406–1408. [Google Scholar] [CrossRef]
- Metse, A.P.; Wiggers, J.H.; Wye, P.M.; Wolfenden, L.; Prochaska, J.J.; Stockings, E.A.; Williams, J.M.; Ansell, K.; Fehily, C.; Bowman, J.A. Smoking and Mental Illness: A Bibliometric Analysis of Research Output Over Time. Nicotine Tob. Res. 2017, 19, 24–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Substance Abuse and Mental Health Services Administration. National Mental Health Services Survey (N-MHSS) Data Spotlight Report; About 1 in 4 Mental Health Treatment Facilities Offered Services to Quit Smoking. The National Services Survey (N-MHSS) Data Spotlight Report. 2014. Available online: http://www.samhsa.gov/data/sites/default/files/Spot148_NMHSS_Smoking_Cessation/NMHSS-Spot148-QuitSmoking-2014.pdf (accessed on 7 March 2022).
- Hall, S.M.; Prochaska, J.J. Treatment of Smokers with Co-occurring Disorders: Emphasis on Integration in Mental Health and Addiction Treatment Settings. Annu. Rev. Clin. Psychol. 2009, 5, 409–431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, J.M.; Misikimen, T.; Minsky, S.; Cooperman, N.A.; Miller, M.; Dooley Budsock, P.; Cruz, J.; Stinberg, M.L. Increasing Tobacco Dependence Treatment Through Continuing Education Training for Behavioral Health Professionals. Psychiatr. Serv. 2015, 66, 21–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Payne, T.J.; Gaughf, N.W.; Sutton, M.J.; Sheffer, C.E.; Elci, O.U.; Cropsey, K.L.; Taylor, S.; Netters, T.; Whitworth, C.; Deutsch, P.; et al. The Impact of Brief Tobacco Treatment Training on Practice Behaviours, Self-efficacy and Attitudes Among Healthcare Providers. Int. J. Clin. Pract. 2014, 68, 882–889. [Google Scholar] [CrossRef]
- Greenhalgh, T.; Robert, G.; MacFarlane, F.; Bate, P.; Kyriakidou, O. Diffusion of Innovation in Service Organization: Systematic Review Recommendations. Milbank Q. 2004, 82, 581–629. [Google Scholar] [CrossRef] [Green Version]
- Proctor, E.K.; Landsverk, J.; Aarons, G.; Chambers, D.; Glisson, C.; Mittman, B. Implementation Research in Mental Health Services: An Emerging Science with Conceptual, Methodological, and Training Challenges. Adm. Policy Ment. Health 2009, 36, 24–34. [Google Scholar] [CrossRef]
- Institute of Medicine (US) Committee on Quality of Health Care in America. Crossing the Quality Chasm: A New Health System for the 21st Century; National Academies Press: Washington, DC, USA, 2001. [Google Scholar]
- National Advisory Mental Health Council. Blueprint for Change: Research on Child and Adolescent Mental Health Intervention Development and Deployment; National Institute of Mental Health: Bethesda, MD, USA, 2001. [Google Scholar]
- National Advisory Mental Health Council. The Road Ahead: Research Partnerships to Transform Services. A Report by the National Advisory Mental Health Council’s Workgroup on Services and Clinical Epidemiology Research; National Institute of Mental Health: Bethesda, MD, USA, 2006. [Google Scholar]
- Bertram, R.M.; Blasé, K.A.; Fixsen, D.L. Improving Programs and Outcomes: Implementing Frameworks and Organization Change. Res. Soc. Work Pract. 2015, 25, 477–487. [Google Scholar] [CrossRef]
- Ziedonis, D.M.; Guydish, J.; Williams, J.; Steinberg, M.; Foulds, J. Barriers and Solutions to Addressing Tobacco Dependence in Addiction Treatment Programs. Alcohol Res. Health 2006, 29, 228–235. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6527042/ (accessed on 8 March 2022).
- Johnson, S.E.; Mitrou, F.; Lawrence, D.; Zubrixk, S.R.; Wolstencroft, K.; Ennals, P.; Hall, C.; McNaught, E. Feasibility of a Consumer Centered Tobacco Management Intervention in Community Mental Health Services in Australia. Comm. Ment. Health J. 2020, 56, 1354–1365. [Google Scholar] [CrossRef]
- Borrelli, B.; Lee, C.; Novak, S. Is Provider Training Effective? Changes in Attitudes Towards Smoking Cessation and Counseling Behaviors of Home Health Care Nurses. Prev. Med. 2008, 46, 358–363. [Google Scholar] [CrossRef] [Green Version]
- Correa-Fernández, V.; Wilson, W.T.; Kyburz, B.; O’Connor, D.P.; Stacey, T.; Williams, T.; Lam, C.Y.; Reitzel, L.R. Evaluation of the Taking Texas Tobacco Free Workplace Program within Behavioral Health Centers. Transl. Behav. Med. 2018, 9, 319–327. [Google Scholar] [CrossRef] [PubMed]
- Beidas, R.S.; Kendall, P.C. Training Therapists in Evidence-based Practice: A Critical Review of Studies from a Systems-contextual Perspective. Clin. Psych. Sci. Pract. 2010, 17, 1–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, L.C.; Grimshaw, J.M.; Nielsen, C.; Judd, M.; Coyte, P.C.; Graham, I.D. Evolution of Wenger’s Concept of Community of Practice. Implement. Sci. 2009, 4, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lave, J.; Wenger, E. Situated Learning: Legitimate Peripheral Participation; Cambridge University Press: Cambridge, UK, 1991. [Google Scholar] [CrossRef]
- Wenger, E. Communities of Practice: A Brief Introduction; National Science Foundation: Alexandria, VA, USA, 2011; Available online: https://scholarsbank.uoregon.edu/xmlui/bitstream/handle/1794/11736/A%20brief%20introduction%20to%20CoP.pdf (accessed on 10 March 2022).
- Ranmuthugala, G.; Plumb, J.J.; Cunningham, F.C.; Georgiou, A.; Westbrook, J.J.; Braithwaite, J. How and Why are Communities of Practice Established in the Healthcare Sector? A Systematic Review of the Literature. BMC Health Serv. Res. 2011, 11, 273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nitturi, V.; Chen, T.A.; Kyburz, B.; Leal, I.M.; Fernández, V.C.; O’Connor, D.; Williams, T.; Garey, L.; Stacey, T.; Wilson, W.T.; et al. Organizational Characteristics and Readiness for Tobacco-Free Workplace Program Implementation Moderates Changes in Clinician’s Delivery of Smoking Interventions within Behavioral Health Treatment Clinics. Nicotine Tob. Res. 2021, 23, 310–319. [Google Scholar] [CrossRef] [PubMed]
- Samaha, H.L.; Correa-Fernández, V.; Lam, C.; Wilson, W.T.; Kyburz, B.; Stacey, T.; Williams, T.; Reitzel, L.R. Addressing Tobacco Use Among Consumers and Staff at Behavioral Health Treatment Facilities Through Comprehensive Workplace Programming. Health Promot. Pract. 2017, 18, 561–570. [Google Scholar] [CrossRef] [PubMed]
- Le, K.; Fernández, V.C.; Leal, I.M.; Kyburz, B.; Chen, T.A.; Barrientos, D.; Saenz, E.; Williams, T.; O’Connor, D.P.; Obasi, E.M.; et al. Tobacco-free Workplace Program at a Substance Use Treatment Center. Am. J. Health Behav. 2020, 44, 652–665. [Google Scholar] [CrossRef]
- Correa-Fernández, V.; Wilson, W.T.; Shedrick, D.A.; Kyburz, B.; Stacey, T.; Williams, T.; Lam, C.Y.; Reitzel, L.R. Implementation of a Tobacco-free Workplace Program at a Local Mental Health Authority. Transl. Behav. Med. 2017, 7, 204–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leal, I.M.; Chen, T.A.; Fernández, V.C.; Le, K.; O’Connor, D.P.; Kyburz, B.; Wilson, W.T.; Williams, T.; Reitzel, L.R. Adapting and Evaluating Implementation of Tobacco-Free Workplace Program in Behavioral Health Centers. Am. J. Health Behav. 2020, 44, 820–839. [Google Scholar] [CrossRef]
- Le, K.; Chen, T.A.; Leal, I.M.; Fernández, V.C.; Obasi, E.M.; Kyburz, B.; Williams, T.; Casey, K.; Taing, M.; O’Connor, D.P.; et al. Organizational factors moderating changes in tobacco use dependence care delivery following a comprehensive tobacco-free workplace intervention in non-profit substance use treatment centers. International journal of environmental research and public health. Int. J. Environ. Res. Public Health 2021, 18, 10485. [Google Scholar] [CrossRef]
- Texas Health and Human Services, 2022 Local Mental Health Authorities (LMHAs). 2022. Available online: https://www.hhs.texas.gov/providers/behavioral-health-services-providers/local-mental-health-authorities (accessed on 9 March 2022).
- Eby, L.T.; Burk, H.; Maher, C.P. How Serious of a Problem is Staff Turnover in Substance Abuse Treatment? A Longitudinal Study of Actual Turnover. J. Subst. Abus. Treat. 2010, 39, 264–271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hyde, P.S. Report to Congress on the Nation’s Substance Abuse and Mental Health Workforce Issues. United States Department for Health and Human Services, Subst. Abuse and Mental Health Services. 2013. Available online: http://www.cimh.org/sites/main/files/file-attachments/samhsa_bhwork_0.pdf (accessed on 9 March 2022).
- Patton, M.Q. Qualitative Research and Evaluation Methods: Integrating Theory and Practice, 4th ed.; SAGE Publications: Thousand Oaks, CA, USA, 2014. [Google Scholar]
- Rai, N.; Thapa, B. A Study on Purposive Sampling Method in Research; Kathmandu School of Law: Anantalingeshwar, Nepal, 2015. [Google Scholar]
- Mayan, M.J. Essentials of Qualitative Inquiry, 1st ed.; Left Coast Press: Walnut Creek, CA, USA, 2009. [Google Scholar]
- Archibald, M.M.; Ambagsheer, R.C.; Casey, M.G.; Lawless, M. Using Zoom for Qualitative Data Collection: Perceptions and Experiences of Researchers and Participants. Int. J. Qual. Methods 2019, 18, 1609406919874596. [Google Scholar] [CrossRef] [Green Version]
- Norwell, L.S.; Norris, J.M.; White, D.E.; Moules, N.J. Thematic Analysis: Striving to Meet the Trustworthiness Criteria. Int. J. Qual. Methods 2017, 16, 1609406917733847. [Google Scholar] [CrossRef]
- Ando, H.; Cousins, R.; Young, C. Achieving Saturation in Thematic Analysis: Development and Refinement of a Codebook. Compr. Psychol. 2014, 3, 2165–2228. [Google Scholar] [CrossRef] [Green Version]
- Braithwaite, J.; Westbrook, J.I.; Ranmuthugala, G.; Cunningham, F.; Plumb, J.; Wiley, J.; Ball, D.; Huckson, S.; Hughes, C.; Johnston, B.; et al. The Development, Design, Testing, Refinement, Simulation and Application of an Evaluation Framework for Communities of Practice and Social-Professional Networks. BMC Health Serv. Res. 2009, 9, 162. [Google Scholar] [CrossRef] [Green Version]
- Brown, J.S.; Duguid, P. Organizational Learning and Communities-of-Practice: Toward a Unified View of Working, Learning, and Innovation. Org. Sci. 1991, 2, 40–57. Available online: https://www.jstor.org/stable/2634938 (accessed on 11 March 2022). [CrossRef]
- Pyrko, I.; Dörfler, V.; Eden, C. Thinking together: What makes communities of practice work? Hum. Relat. 2017, 70, 389–409. [Google Scholar] [CrossRef] [Green Version]
- Tintorer, D.L.; Domínguez, J.M.; Rivera, E.P.; Beneyto, S.F.; Tuduri, X.M.; Rubió, S. Keys to success of a community of clinical practice in primary care: A qualitative evaluation of the ECOPIH project. BMC Fam. Pract. 2018, 19, 56. [Google Scholar] [CrossRef]
- Moore, J.L.; Bjørkli, C.; Havdahl, R.T.; Lømo, L.L.; Midthaug, M.; Skjuve, M.; Klokkerud, M.; Nordvik, J.E. A qualitative study exploring contributors to the success of a community of practice in rehabilitation. BMC Med. Educ. 2021, 21, 282. [Google Scholar] [CrossRef]
- Thompson, G.N.; Estabrooks, C.A.; Degner, L.F. Clarifying the concepts in knowledge transfer: A literature review. J. Adv. Nurs. 2006, 53, 691–701. [Google Scholar] [CrossRef]
- Flodgren, G.; Parmelli, E.; Doumit, G.; Gattellari, M.; O’Brien, M.A.; Grimshaw, J.; Eccles, M.P. Local Opinion Leaders: Effects on Professional Practice and Health Care Outcomes. Cochrane Database Syst. Rev. 2007, 10, CD000125. [Google Scholar] [CrossRef]
- Saigí-Rubió, F.; González-González, I. Cooperative learning environments: Virtual communities of practice in the healthcare sector. eLearn Res. Pap. Ser. 2014, 9, 15–25. [Google Scholar]
- Russell, J.; Greenhalgh, T.; Boynton, P.; Rigby, M. Soft networks for bridging the gap between research and practice: Illuminative evaluation of Chain. BMJ 2004, 328, 1174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- West, E.; Barron, D.; Dowsett, J.; Newton, J. Hierarchies and cliques in the social networks of health care professionals: Implications for the design of dissemination strategies. Soc. Sci. Med. 1999, 48, 633–646. [Google Scholar] [CrossRef]
- Dopson, S.; FitzGerald, L.; Ferlie, E.; Gabbay, J.; Locock, L. No magic targets! Changing clinical practice to become more evidence based. Health Care Manag. Rev. 2002, 1, 35–47. [Google Scholar] [CrossRef]
- Cunningham, F.C.; Ranmuthugala, G.; Plumb, J.; Georgiou, A.; Westbrook, J.I.; Braithwaite, J. Health professional networks as a vector for improving healthcare quality and safety: A systematic review. BMJ Qual. Saf. 2012, 21, 239–249. [Google Scholar] [CrossRef] [Green Version]
- Polanyi, M. The logic of tacit inference. Philosophy. 1966, 41, 1–18. Available online: https://www.jstor.org/stable/3749034 (accessed on 29 April 2022). [CrossRef]
- Barwick, M.A.; Peters, J.; Boydell, K. Getting to uptake: Do Communities of Practice Support the Implementation of Evidence-Based Practice? J. Can. Acad. Child Adolesc. Psychiatry 2009, 18, 16–29. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2651208/ (accessed on 29 April 2022).
- Soubhi, H.; Bayliss, E.A.; Fortin, M.; Hudon, C.; van den Akker, M.; Thivierge, R.; Posel, N.; Fleiszer, D. Learning and caring in communities of practice: Using relationships and collective learning to improve primary care for patients with multimorbidity. Ann. Fam. Med. 2010, 8, 170–177. [Google Scholar] [CrossRef] [Green Version]
- Nicolini, D. Practice as the site of knowing: Insights from the field of telemedicine. Organ. Sci. 2011, 22, 602–620. [Google Scholar] [CrossRef]
- Lees, A.; Meyer, E. Theoretically speaking: Use of a communities of practice framework to describe and evaluate interprofessional education. J. Interprof. Care 2011, 25, 84–90. [Google Scholar] [CrossRef] [PubMed]
- About the Program. Available online: https://www.takingtexastobaccofree.com/trainthetrainer (accessed on 3 May 2022).
- National Academies of Sciences, Engineering, and Medicine. Public Health Consequences of E-Cigarettes; The National Academies Press: Washington, DC, USA, 2018. [Google Scholar] [CrossRef]
- Ebbert, J.O.; Agunwamba, A.A.; Rutten, L.J. Counseling patients on the use of e-cigarettes. Mayo Clin. Proc. 2015, 90, 128–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Center | Number of Individual Clinics | Number of Full-Time Employees | Number of Full-Time Providers | Total Annual Clients Served | Total Annual Unique Client Contacts | Counties Served (%Rural) |
|---|---|---|---|---|---|---|
| LMHA1 | 42 | 247 | 150 | 92,498 | 5420 | 23 (100%) |
| LMHA2 | 20 | 323 | 254 | 229,482 | 9808 | 4 (50%) |
| LMHA3 | 31 | 419 | 286 | 239,672 | 11,243 | 6 (88.3%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martinez Leal, I.; Martinez, J.; Britton, M.; Chen, T.A.; Correa-Fernández, V.; Kyburz, B.; Nitturi, V.; Obasi, E.M.; Drenner, K.; Williams, T.; et al. Collaborative Learning: A Qualitative Study Exploring Factors Contributing to a Successful Tobacco Cessation Train-the-Trainer Program as a Community of Practice. Int. J. Environ. Res. Public Health 2022, 19, 7664. https://doi.org/10.3390/ijerph19137664
Martinez Leal I, Martinez J, Britton M, Chen TA, Correa-Fernández V, Kyburz B, Nitturi V, Obasi EM, Drenner K, Williams T, et al. Collaborative Learning: A Qualitative Study Exploring Factors Contributing to a Successful Tobacco Cessation Train-the-Trainer Program as a Community of Practice. International Journal of Environmental Research and Public Health. 2022; 19(13):7664. https://doi.org/10.3390/ijerph19137664
Chicago/Turabian StyleMartinez Leal, Isabel, Jayda Martinez, Maggie Britton, Tzuan A. Chen, Virmarie Correa-Fernández, Bryce Kyburz, Vijay Nitturi, Ezemenari M. Obasi, Kelli Drenner, Teresa Williams, and et al. 2022. "Collaborative Learning: A Qualitative Study Exploring Factors Contributing to a Successful Tobacco Cessation Train-the-Trainer Program as a Community of Practice" International Journal of Environmental Research and Public Health 19, no. 13: 7664. https://doi.org/10.3390/ijerph19137664
APA StyleMartinez Leal, I., Martinez, J., Britton, M., Chen, T. A., Correa-Fernández, V., Kyburz, B., Nitturi, V., Obasi, E. M., Drenner, K., Williams, T., Casey, K., Carter, B. J., & Reitzel, L. R. (2022). Collaborative Learning: A Qualitative Study Exploring Factors Contributing to a Successful Tobacco Cessation Train-the-Trainer Program as a Community of Practice. International Journal of Environmental Research and Public Health, 19(13), 7664. https://doi.org/10.3390/ijerph19137664